
Loeys-Dietz syndrome
Loeys-Dietz syndrome a human genetic disorder of connective tissue that causes aortic aneurysms, widely spaced eyes (hypertelorism), cleft palate and/or split uvula (the little piece of flesh that hangs down in the back of the mouth) and twisting or spiraled arteries (arterial tortuosity) 1. Other findings include craniosynostosis, extropia (eyes that turn outward), micrognathia, structural brain abnormalities, intellectual deficit, and congenital heart disease. Connective tissue provides strength and flexibility to structures such as bones, ligaments, muscles, and blood vessels. Loeys-Dietz syndrome signs and symptoms vary among individuals. There are six types of Loeys-Dietz syndrome, labelled types 1 through 6, which are distinguished by their genetic cause. Loeys-Dietz syndrome types 1 and 2 appear to be the most common forms. This condition is called Loeys-Dietz syndrome type 1 when affected individuals have cleft palate, craniosynostosis, and/or hypertelorism. Individuals without these features are said to have Loeys-Dietz syndrome type 2. The disease is caused by mutations in the TGFBR1, the TGFBR2, the SMAD3 or the TGFB2 genes 1. Regardless of the type, signs and symptoms of Loeys-Dietz syndrome can become apparent anytime from childhood through adulthood, and the severity is variable.
The prevalence of Loeys-Dietz syndrome is unknown.
Loeys-Dietz syndrome is inherited in an autosomal dominant manner with variable clinical expression 1. It is important to have an early and adequate treatment for the heart problems because the chance for aortic dissection and other vascular problems may be high in some patients. Aortic dissection has been observed in early childhood (age ≥6 months) and/or at aortic dimensions that do not confer risk in other connective tissue disorders such as Marfan syndrome 1. Many specialists may be involved for the best management of the patient.
In Loeys-Dietz syndrome the aorta can weaken and stretch, causing a bulge in the blood vessel wall (an aneurysm). Stretching of the aorta may also lead to a sudden tearing of the layers in the aorta wall (aortic dissection). People with Loeys-Dietz syndrome can also have aneurysms or dissections in arteries throughout the body and have arteries with abnormal twists and turns (arterial tortuosity).
Individuals with Loeys-Dietz syndrome often have skeletal problems including premature fusion of the skull bones (craniosynostosis), an abnormal side-to-side curvature of the spine (scoliosis), either a sunken chest (pectus excavatum) or a protruding chest (pectus carinatum), an inward- and upward-turning foot (clubfoot), flat feet (pes planus), or elongated limbs with joint deformities called contractures that restrict the movement of certain joints. A membrane called the dura, which surrounds the brain and spinal cord, can be abnormally enlarged (dural ectasia). In individuals with Loeys-Dietz syndrome, dural ectasia typically does not cause health problems. Malformation or instability of the spinal bones (vertebrae) in the neck is a common feature of Loeys-Dietz syndrome and can lead to injuries to the spinal cord. Some affected individuals have joint inflammation (osteoarthritis) that commonly affects the knees and the joints of the hands, wrists, and spine.
People with Loeys-Dietz syndrome may bruise easily and develop abnormal scars after wound healing. The skin is frequently described as translucent, often with stretch marks (striae) and visible underlying veins. Some individuals with Loeys-Dietz syndrome develop an abnormal accumulation of air in the chest cavity that can result in the collapse of a lung (spontaneous pneumothorax) or a protrusion of organs through gaps in muscles (hernias). Other characteristic features include widely spaced eyes (hypertelorism), eyes that do not point in the same direction (strabismus), a split in the soft flap of tissue that hangs from the back of the mouth (bifid uvula), and an opening in the roof of the mouth (cleft palate).
Individuals with Loeys-Dietz syndrome frequently develop immune system-related problems such as food allergies, asthma, or inflammatory disorders such as eczema or inflammatory bowel disease.
Loeys-Dietz syndrome type 1
Loeys-Dietz syndrome 1 caused by mutations in the TGFBR1 gene
Loeys-Dietz syndrome type 2
Loeys-Dietz syndrome 2 caused by mutations in the TGFBR2 gene
Loeys-Dietz syndrome type 3
Loeys-Dietz syndrome 3 caused by mutations in the SMAD3 gene
Loeys-Dietz syndrome type 4
Loeys-Dietz syndrome 4 caused by mutations in the TGFB2 gene
Loeys-Dietz syndrome type 5
Loeys-Dietz syndrome 5 caused by mutations in the TGFB3 gene
Loeys-Dietz syndrome type 6
Loeys-Dietz syndrome 6 caused by mutations in the SMAD2 gene
Loeys-Dietz syndrome causes
The five types of Loeys-Dietz syndrome are distinguished by their genetic cause: TGFBR1 gene mutations cause type 1, TGFBR2 gene mutations cause type 2, SMAD3 gene mutations cause type 3, TGFB2 gene mutations cause type 4, and TGFB3 gene mutations cause type 5. These five genes play roles in a cell signaling pathway called the transforming growth factor beta (TGF-β) pathway, which directs the functions of the body’s cells during growth and development. This pathway also regulates the formation of the extracellular matrix, an intricate lattice of proteins and other molecules that forms in the spaces between cells and is important for tissue strength and repair.
Mutations in the TGFBR1, TGFBR2, SMAD3, TGFB2, or TGFB3 gene result in the production of a protein with reduced function. Even though the protein is less active, signaling within the TGF-β pathway occurs at an even greater intensity than normal in tissues throughout the body. Researchers speculate that the activity of other proteins in this signaling pathway is increased to compensate for the protein whose function is reduced; however, the exact mechanism responsible for the increase in signaling is unclear. The overactive TGF-β pathway disrupts the development of the extracellular matrix and various body systems, leading to the signs and symptoms of Loeys-Dietz syndrome.
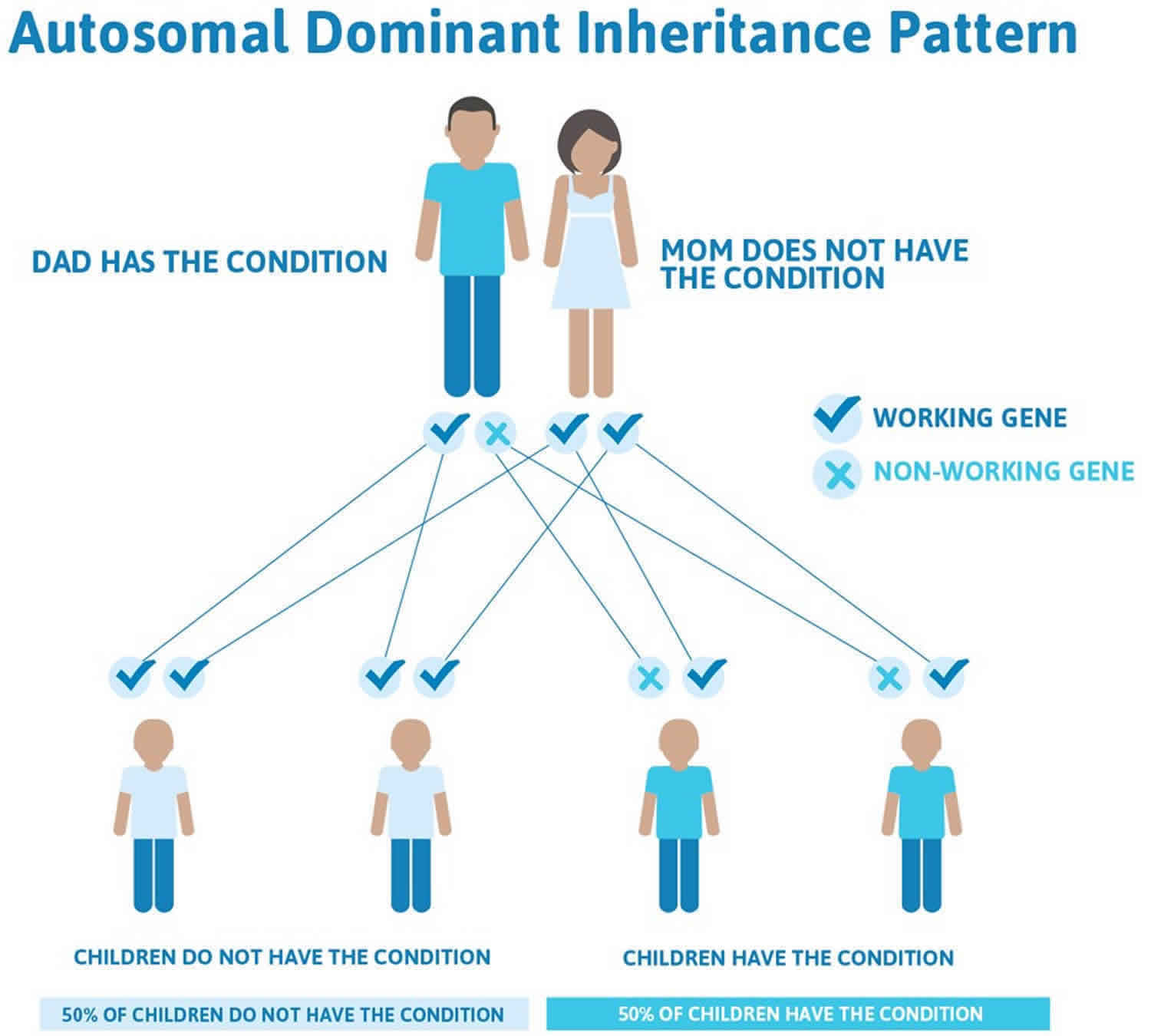
Loeys-Dietz syndrome inheritance pattern
Loeys-Dietz syndrome has an autosomal dominant pattern of inheritance, which means one copy of the altered gene in each cell is sufficient to cause the disorder.
In cases where the autosomal dominant condition does run in the family, the chance for an affected person to have a child with the same condition is 50% regardless of whether it is a boy or a girl. These possible outcomes occur randomly. The chance remains the same in every pregnancy and is the same for boys and girls.
- When one parent has the abnormal gene, they will pass on either their normal gene or their abnormal gene to their child. Each of their children therefore has a 50% (1 in 2) chance of inheriting the changed gene and being affected by the condition.
- There is also a 50% (1 in 2) chance that a child will inherit the normal copy of the gene. If this happens the child will not be affected by the disorder and cannot pass it on to any of his or her children.
In about 75 percent of cases, Loeys-Dietz syndrome results from a new gene mutation and occurs in people with no history of the disorder in their family. This is called a de novo mutation. In 25 percent of cases, an affected person inherits the mutation from one affected parent.
Figure 1. Loeys-Dietz syndrome autosomal dominant inheritance pattern
People with specific questions about genetic risks or genetic testing for themselves or family members should speak with a genetics professional.
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://www.findageneticcounselor.com/) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://www.abgc.net/about-genetic-counseling/find-a-certified-counselor/) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counselors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (http://www.acmg.net/ACMG/Genetic_Services_Directory_Search.aspx) has a searchable database of medical genetics clinic services in the United States.
Loeys-Dietz syndrome signs and symptoms
Loeys-Dietz syndrome should be suspected in individuals with the following vascular, skeletal, craniofacial, cutaneous, allergic/inflammatory, and ocular findings 2. Four main characteristics suggest the diagnosis of Loeys-Dietz syndrome. These features are not usually seen all together in other connective tissue disorders as major characteristics.
These symptoms include:
- Aneurysms (widening or dilation of arteries), which can be observed by imaging techniques. These are most often observed in the aortic root (base of the artery leading from the heart) but can be seen in other arteries throughout the body
- Arterial tortuosity (twisting or spiraled arteries), most often occurring in the vessels of the neck and observed on imaging techniques
- Hypertelorism (widely spaced eyes)
- Bifid (split) or broad uvula (the little piece of flesh that hangs down in the back of the mouth)
It is important to note, however, that these findings are not observed in all patients and do not concretely lead to a diagnosis of Loeys-Dietz syndrome.
Categorized by system, below is a more detailed list of symptoms recorded in individuals diagnosed with Loeys-Dietz syndrome:
Vascular
- Dilatation or dissection of the aorta and other arteries. Aortic root dilatation is seen in more than 95% of probands; the aortic root is the most common site for a dissection to occur. In rare circumstances, aneurysms or dissections can be seen in other arteries in the head, chest, abdomen, or extremities in the absence of aortic involvement.
- Other arterial aneurysms and tortuosity
- Evaluation is best done with magnetic resonance angiography (MRA) or CT angiogram (CTA) with 3D reconstruction from head to pelvis to identify arterial aneurysms or dissections and arterial tortuosity throughout the arterial tree.
- Tortuosity is often most prominent in head and neck vessels.
- Approximately 50% of individuals with Loeys-Dietz syndrome studied had an aneurysm distant from the aortic root that would not have been detected by echocardiography.
Craniofacial (head and face)
- Malar hypoplasia (flat cheek bones)
- Slight downward slant to the eyes
- Craniosynostosis (early fusion of the skull bones)
- Cleft palate (hole in the roof of the mouth)
- Blue sclerae (blue tinge to the whites of the eyes)
- Micrognathia (small chin) and/or retrognathia (receding chin)
Skeletal (bones)
- Long fingers and toes
- Contractures of the fingers
- Clubfoot or skewfoot deformity
- Scoliosis (s-like curvature of the spine)
- Cervical-spine instability (instability in the vertebrae directly below the skull)
- Joint laxity
- Pectus excavatum (chest wall deformity that causes the sternum and breast bone to grow inward) / Pectus carinatum (chest wall deformity that pushes the sternum and breast bone out)
- Osteoarthritis
- Typically normal stature
Skin
- Translucent skin
- Soft or velvety skin
- Easy bruising
- Abnormal or wide scarring
- Soft skin texture
- Hernias
- Milia, prominently on the face
Cardiac
- Congenital (existing at birth) heart defects, which can include patent ductus arteriosus (PDA), atrial or ventricular septal defect (ASD/VSD) and bicuspid aortic valve.
Ocular
- Myopia (nearsighted)
- Eye muscle disorders
- Blue or dusky sclerae
- Retinal detachment: The retina is the light-sensitive layer of tissue that lines the inside of the eye and sends visual messages through the optic nerve to the brain. When the retina detaches, it is lifted or pulled from its normal position. If not promptly treated, retinal detachment can cause permanent vision loss.
Other
- Food, seasonal or environmental allergies
- Asthma / chronic sinusitis
- Eczema
- Eosinophilic esophagitis/gastritis
- Inflammatory bowel disease such as Crohn’s disease or ulcerative colitis
- Hollow organs such as intestine, uterus and spleen prone to rupture
Emergency situations
Following is information regarding potential emergency situations that can arise in someone with Loeys-Dietz Syndrome.
Cardiovascular
Aortic or arterial dissection is a potentially life threatening complication related to aortic aneurysm. Symptoms of aortic dissection include sudden severe chest pain, migrating to the chest, neck, back, abdomen and/or an extremity. Some individuals with aortic dissection have reported nausea, vomiting, shortness of breath, and collapse. Symptoms of aortic dissection warrant calling your local emergency services number and transport to the nearest hospital for aortic imaging (CTA, MRA, echocardiography) to confirm or exclude dissection, for stabilization, and appropriate treatment. Stroke symptoms may present with neck artery dissections.
Pulmonary
Spontaneous pneumothorax results from rupture of pulmonary blebs. Blebs form due to increased air spaces in the lung. Symptoms of spontaneous pneumothorax include chest, neck or back pain exacerbated by deep breathing, or difficult breathing due to pain. HEMOPTYSIS of unknown etiology has also been seen in Loeys-Dietz syndrome.
Hollow organ rupture
Hollow organ rupture or tear of the spleen or uterus has been reported rarely. Bowel rupture may be a very rare complication.
Ocular
Retinal detachment is associated with sudden visual field loss. Although retinal detachment is not life threatening, unrecognized/untreated detachment can result in blindness. Therefore, sudden visual disturbance warrants emergency evaluation.
Loeys-Dietz syndrome complications
Several major complications have been noted in early patient studies.
The majority of individuals with Loeys-Dietz syndrome are diagnosed with aneurysms (commonly called enlargements or dilations) of the aortic root. Aneurysms can also be seen throughout the arterial tree (all of the arteries). Although monitoring of aneurysms, surgical intervention and medication use will hopefully help to decrease the amount of cardiovascular complications associated with Loeys-Dietz syndrome, there is a risk for death due to aortic dissection (aneurysm rupture or tear).
Individuals diagnosed with Loeys-Dietz syndrome should go to the emergency room if they have episodes of intense and/or prolonged pain in the body. As many emergency room professionals may not be familiar with the diagnosis of Loeys-Dietz syndrome, it is important that they know of the predisposition to arterial rupture and that prompt imaging should be performed. Rarely, hollow organ (uterus, spleen, intestine) rupture occurs. Individuals impacted by Loeys-Dietz syndrome should work with their physician to develop an emergency letter that should be placed in their medical records and shared with schools, workplaces, etc.
Another complication observed in individuals with Loeys-Dietz syndrome is cervical-spine instability (instability in the vertebrae directly below the skull). This can potentially cause serious risks and should be evaluated with x-rays in the flexion and extension positions.
An orthopedics physician may need to be consulted and may recommend further imaging such as MRI or CT of the neck. These images should be performed prior to any surgeries requiring intubation, as this will impact anesthesia management. A small proportion of individuals with Loeys-Dietz syndrome require surgical intervention to fuse the bones of the skull to prevent dangerous slippage of the bones around the spinal cord.
A complication specific to women is the high incidence of difficulties during pregnancy. There is a high risk of aortic dissection or uterine rupture during pregnancy or directly after childbirth. Many women with Loeys-Dietz syndrome have had numerous successful pregnancies. It is challenging that there are no predictors of which women may experience complications and which may not. If you have a diagnosis of Loeys-Dietz syndrome, you should consult your physicians prior to a pregnancy to discuss risks and to determine a plan for pregnancy management. As some individuals with Loeys-Dietz syndrome are on blood pressure medications in the angiotensin receptor blocker class, it is important to note that this medication is teratogenic (causing medical concerns, birth defects and/or death) to the fetus and a plan for titrating off this medication should be put in place prior to pursuing pregnancy.
Loeys-Dietz syndrome diagnosis
There are several clinical evaluations that are currently pursued together to determine a diagnosis of Loeys-Dietz syndrome.
If there is suspicion of Loeys-Dietz syndrome, it is recommended that individuals be evaluated by a geneticist who is familiar with connective tissue disorders. During the initial visit, a detailed family and medical history will be taken and a comprehensive physical examination will be conducted to evaluate the skeletal, craniofacial and skin-related features that are typically present in individuals with Loeys-Dietz syndrome.
If there is continued suspicion of Loeys-Dietz syndrome, an echocardiogram (ultrasound imaging of the heart) should be performed to assess if there is aortic enlargement and/or other structural heart defects that are consistent with the diagnosis. A consultation with a cardiologist will be necessary to help interpret the cardiac findings.
A physician may also suggest further imaging of the arteries throughout the body. This is done by obtaining a CTA (CT angiogram or computed tomography angiogram) or MRA (MR angiogram or magnetic resonance angiogram) of the entire arterial tree (head, neck, chest, pelvis and abdomen). These imaging studies will detect aneurysms in other arteries.
Three-dimensional reconstruction (3D) of CTA or MRA imaging is recommended to check for arterial tortuosity, a common finding in individuals with Loeys-Dietz syndrome, particularly in the neck. This finding in itself does not typically cause medical concern but can suggest more evidence to support the diagnosis of Loeys-Dietz syndrome.
Genetic testing for mutations (gene changes) within the TGFBR1, TGFBR2, SMAD3, TGFB2 and TGFB3 genes is clinically available if there is high suspicion of the diagnosis. This test should be ordered by a geneticist, who will be able to accurately interpret and convey the results of the testing. A geneticist will also be able to interpret the family history and determine if genetic testing for other family members is appropriate. If a gene mutation is found in a child, it is typically recommended to test the parents for the same mutation to give accurate recurrence risk information. Testing of offspring of an adult diagnosed with Loeys-Dietz syndrome is always recommended.
Loeys-Dietz syndrome treatment
Loeys-Dietz syndrome manifests itself in a number of ways; therefore, no two persons with Loeys-Dietz syndrome will have identical medical characteristics. It is recommended that you consult your physician or a local geneticist if you have questions about individual health concerns. It is always important to consult your doctor to determine an effective and personalized course of action.
Medications
Pressure on the aorta (the largest artery leaving the heart) and other arteries can be controlled by the administration of medications that work to lessen the strain on the body’s major arteries by reducing heart rate and blood pressure. In mouse models of Loeys-Dietz syndrome the specific class of blood-pressure lowering medications known as angiotensin receptor blockers, has shown great benefit in reducing aneurysm growth. In people impacted by Loeys-Dietz syndrome, if this type of medication is used, it should be used at optimal titration. Angiotensin receptor blockers include medications by the name of Losartan, Irbesartan or Candesartan. Many people are also maintained on beta-blockers (Atenolol, Metoprolol). It is recommended that individuals with Loeys-Dietz syndrome remain on these medications even after surgical repair of aneurysms.
Imaging
Continued monitoring of the aorta through annual echocardiograms is necessary. A baseline CTA or MRA of the head, neck, chest, abdomen and pelvis should also be performed to detect and monitor aneurysm formation and/or dissections (tears). The frequency of these scans depends on aneurysm size and rate of growth, so it is recommended that individuals consult their doctor on the appropriate intervals for imaging. Individuals should try not to go more than two years without head-to-pelvis imaging. If a person is using MRA imaging for surveillance, every few imaging cycles a CTA of the head and neck should be considered, as this imaging has better clarity of small arteries in the head and neck.
Cervical Spine Imaging: X-rays of the cervical spine in the flexion and extension positions are recommended to assess for vertebral anomalies and/or instability. If there are any anomalies detected, consultation with an orthopedist is recommended. Rarely, surgery for cervical spine fusion is required. It is important to assess for cervical spine instability prior to undergoing any surgery, as this may impact intubation procedures.
Vascular Surgery
Vascular surgery is a widely recommended treatment option as a preventative surgery for individuals with a rapidly enlarging aorta or artery or a pronounced family history of arterial dissection. Aortic root replacement is the most common vascular surgery occurring in individuals with Loeys-Dietz syndrome, and it is highly successful. There are many examples of successful arterial repairs for aneurysms throughout the body through a variety of surgical interventions as vascular tissue is not typically weak or fragile in individuals with Loeys-Dietz syndrome.
Exercise Restrictions
Exercise restrictions are typically put in place to assist in slowing the rate of aortic and arterial aneurysm growth. It is advised that individuals with Loeys-Dietz syndrome avoid competitive sports, especially contact sports, and other exercises or muscle straining activities performed to the point of exhaustion. Individuals can and should remain active with aerobic types of activities that are performed in moderation. Exercises where you have to strain your muscles, such as push-ups, chin-ups, sit-ups, are to be avoided. Activities such as hiking, biking, jogging and swimming that help to naturally lower the heart rate and blood pressure should be a part of an individual’s cardiovascular activity. A good recommendation for cardiovascular activities is to exercise only to a level where you can hold a conversation while performing the activity.
Orthopedics
Individuals with Loeys-Dietz syndrome may need orthopedic surgery or other interventions such as bracing for scoliosis, orthotics/surgeries for foot deformities or contractures or harnesses for congenital hip dislocation. Typically, surgery for pectus anomalies is pursued for cosmetic purposes and not out of medical necessity.
Allergies
Environmental and food allergies are increased in individuals with Loeys-Dietz syndrome and may require a consultation with an allergist or gastroenterologist. Allergic reactions may present as rhinitis or sinusitis, eczema, or hives. Gastrointestinal complaints can include the feeling of food getting stuck in your throat, diarrhea, abdominal pain or difficulty gaining weight. Some individuals have severe inflammatory disease of the esophagus or intestines that may need stricter intervention such as medications or feeding tubes to help with caloric intake.
Loeys-Dietz syndrome life expectancy
The major sources of morbidity and early mortality in Loeys-Dietz syndrome are dilatation of the aorta at the level of the sinuses of Valsalva, a predisposition for aortic dissection and rupture, mitral valve prolapse with or without regurgitation, and enlargement of the proximal pulmonary artery 1.
Individuals with Loeys-Dietz syndrome have a more aggressive vascular course (with routine involvement of vascular segments distant from the aortic root) than that observed in Marfan syndrome. Mean age at death is 26 years 3. Attias et al 4 reported that the proportion of individuals with aortic dilatation, the age at dissection, and the need for surgery were similar in those with a heterozygous TGFBR2 pathogenic variant and those with a heterozygous FBN1 pathogenic variant causative of Marfan syndrome; however, the rate of death was greater in families with a heterozygous TGFBR2 pathogenic variant. Similarly, a study of 228 families with a heterozygous pathogenic variant in either TGFBR1 or TGFBR2 demonstrated similar aortic risk (dissection or aortic surgery) in both groups 5.
References- Loeys BL, Dietz HC. Loeys-Dietz Syndrome. 2008 Feb 28 [Updated 2018 Mar 1]. In: Adam MP, Ardinger HH, Pagon RA, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2019. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1133
- Loeys BL, Chen J, Neptune ER, Judge DP, Podowski M, Holm T, Meyers J, Leitch CC, Katsanis N, Sharifi N, Xu FL, Myers LA, Spevak PJ, Cameron DE, De Backer J, Hellemans J, Chen Y, Davis EC, Webb CL, Kress W, Coucke P, Rifkin DB, De Paepe AM, Dietz HC. A syndrome of altered cardiovascular, craniofacial, neurocognitive and skeletal development caused by mutations in TGFBR1 or TGFBR2. Nat Genet. 2005;37:275–81
- Loeys BL, Schwarze U, Holm T, Callewaert BL, Thomas GH, Pannu H, De Backer JF, Oswald GL, Symoens S, Manouvrier S, Roberts AE, Faravelli F, Greco MA, Pyeritz RE, Milewicz DM, Coucke PJ, Cameron DE, Braverman AC, Byers PH, De Paepe AM, Dietz HC. Aneurysm syndromes caused by mutations in the TGF-beta receptor. N Engl J Med. 2006;355:788–98
- Attias D, Stheneur C, Roy C, Collod-Béroud G, Detaint D, Faivre L, Delrue MA, Cohen L, Francannet C, Béroud C, Claustres M, Iserin F, Khau Van Kien P, Lacombe D, Le Merrer M, Lyonnet S, Odent S, Plauchu H, Rio M, Rossi A, Sidi D, Steg PG, Ravaud P, Boileau C, Jondeau G. Comparison of clinical presentations and outcomes between patients with TGFBR2 and FBN1 mutations in Marfan syndrome and related disorders. Circulation. 2009;120:2541–9
- Jondeau G, Ropers J, Regalado E, Braverman A, Evangelista A, Teixedo G, De Backer J, Muiño-Mosquera L, Naudion S, Zordan C, Morisaki T, Morisaki H, Von Kodolitsch Y, Dupuis-Girod S, Morris SA, Jeremy R, Odent S, Adès LC, Bakshi M, Holman K, LeMaire S, Milleron O, Langeois M, Spentchian M, Aubart M, Boileau C, Pyeritz R, Milewicz DM., Montalcino Aortic Consortium. International registry of patients carrying TGFBR1 or TGFBR2 mutations: results of the MAC (Montalcino Aortic Consortium). Circ Cardiovasc Genet. 2016;9:548–58





{kind=link}