Mees lines
Mees lines also called “true leukonychia”, leukonychia striata or transverse leukonychia, are a change that occurs in the color of the nail with no palpable ridges, typically described as transverse non-blanching white bands that may extend the complete width of the nail plate, running parallel to the lunula across the entire nail bed of the individual that frequently affect multiple nails, although they also may on a single digit 1. Mees lines migrate toward the distal end of the nail plate over time because the abnormality is in the nail plate and not the nail bed. Mees lines are classically associated with arsenic poisoning 2. If arsenic poisoning is suspected, hair or tissue samples should be obtained for verification; the timing of the poisoning can be estimated based on the rate of nail plate growth 1. However, Mees’ lines also may be associated with multiple other conditions such as thallium or other heavy metal poisoning 3, Hodgkin lymphoma or Hodgkin’s disease, congestive heart failure, renal failure, carcinoid tumors, chemotherapy (i.e., cyclophosphamide, vincristine and doxorubicin), leprosy, malaria, carbon monoxide poisoning and other systemic insults 1.
Mees lines may be confused with Muehrcke lines also called “apparent leukonychia”, which are paired white lines caused by vascular congestion in the nail bed (see Figures 1 and 2 below) 4. Muehrcke lines are easily distinguished from Mees lines because Muehrcke lines fade with digital compression (blood is squeezed from the vessels beneath the nail) and do not migrate with the growth of the nail 5. Muehrcke lines occur in patients with liver disease, nephrotic syndrome, malnutrition and severe hypoalbuminemia (i.e., albumin level less than 2 g per dL or less than 20 g/L) and disappear when the protein level normalizes 6.
In patients with Mees’ lines, the nail bed is normal, but the nail itself is microscopically fragmented, probably because of the disruption of normal growth at the nail matrix during the insult. The width of the lines varies and, because the defect is in the nail itself, the line moves distally with time. Thus, the timing of the insult can be determined by measuring the distance of the lines from the cuticle.
Figure 1. Mees lines
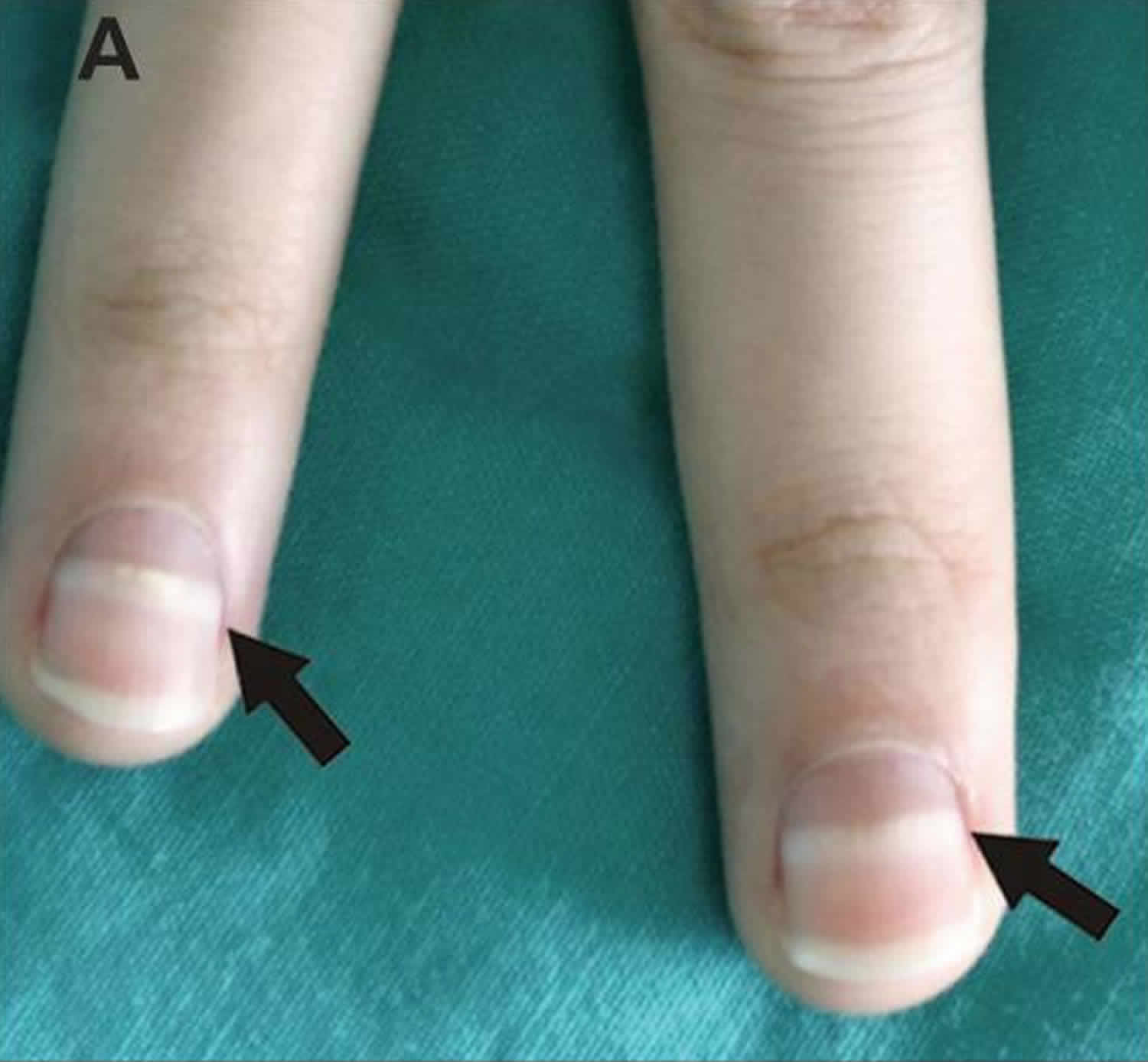
Footnote: Mees lines (arrows) in the fingernails of a 27-year-old woman.
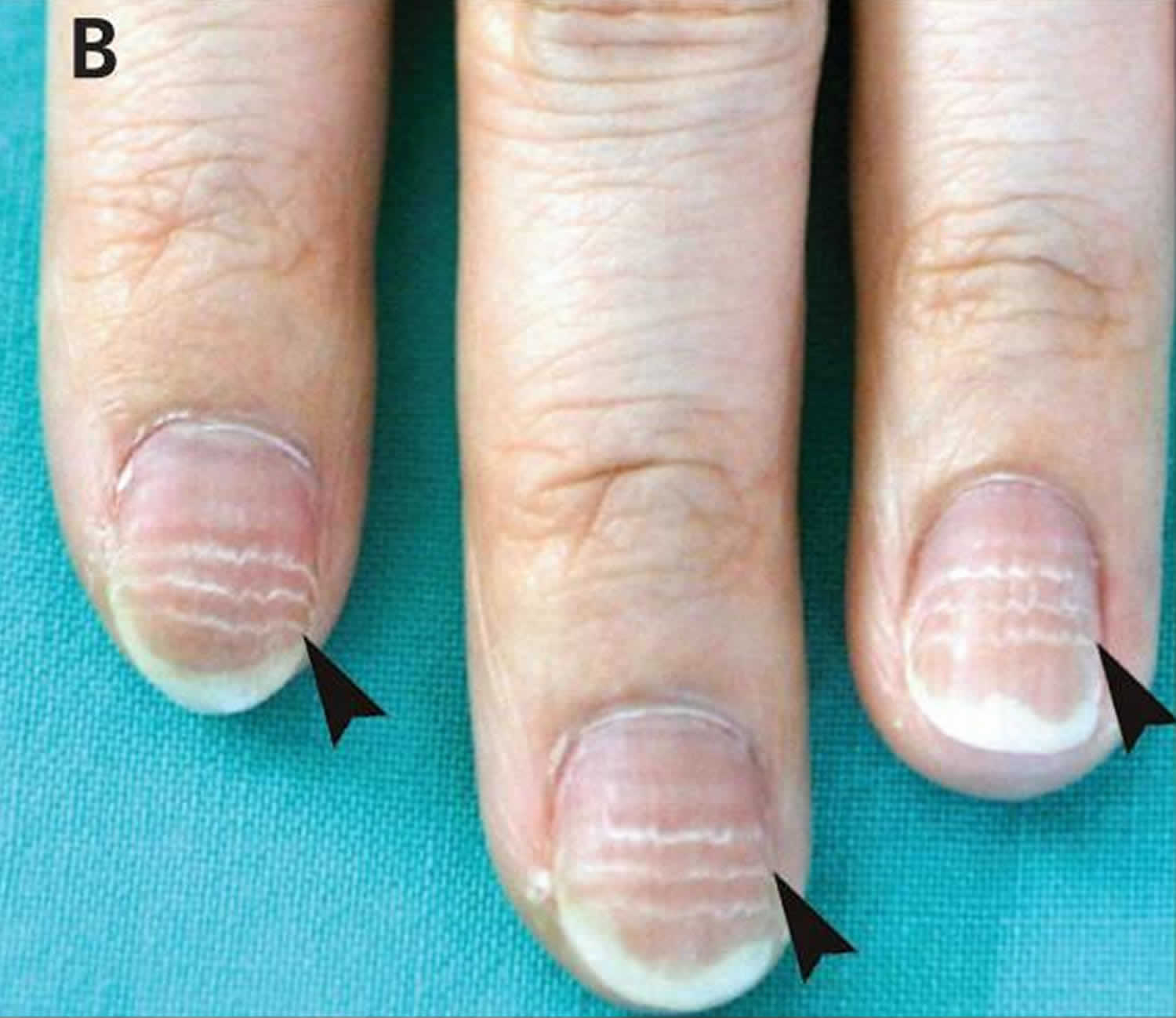
[Source 7 ]Figure 2. Muehrcke lines

Footnote: Fingernails of a 45-year-old man with chronic hypoalbuminemia related to cirrhosis, showing multiple narrow, parallel, white transverse bands that disappeared on blanching. The bands were nonpalpable and separated by normal pink nail, suggestive of Muehrcke lines. Nail clubbing is also visible.
[Source 8 ]Figure 3. Beau lines
Footnote: Beau lines (arrowheads) in the fingernails of a 41-year-old woman.
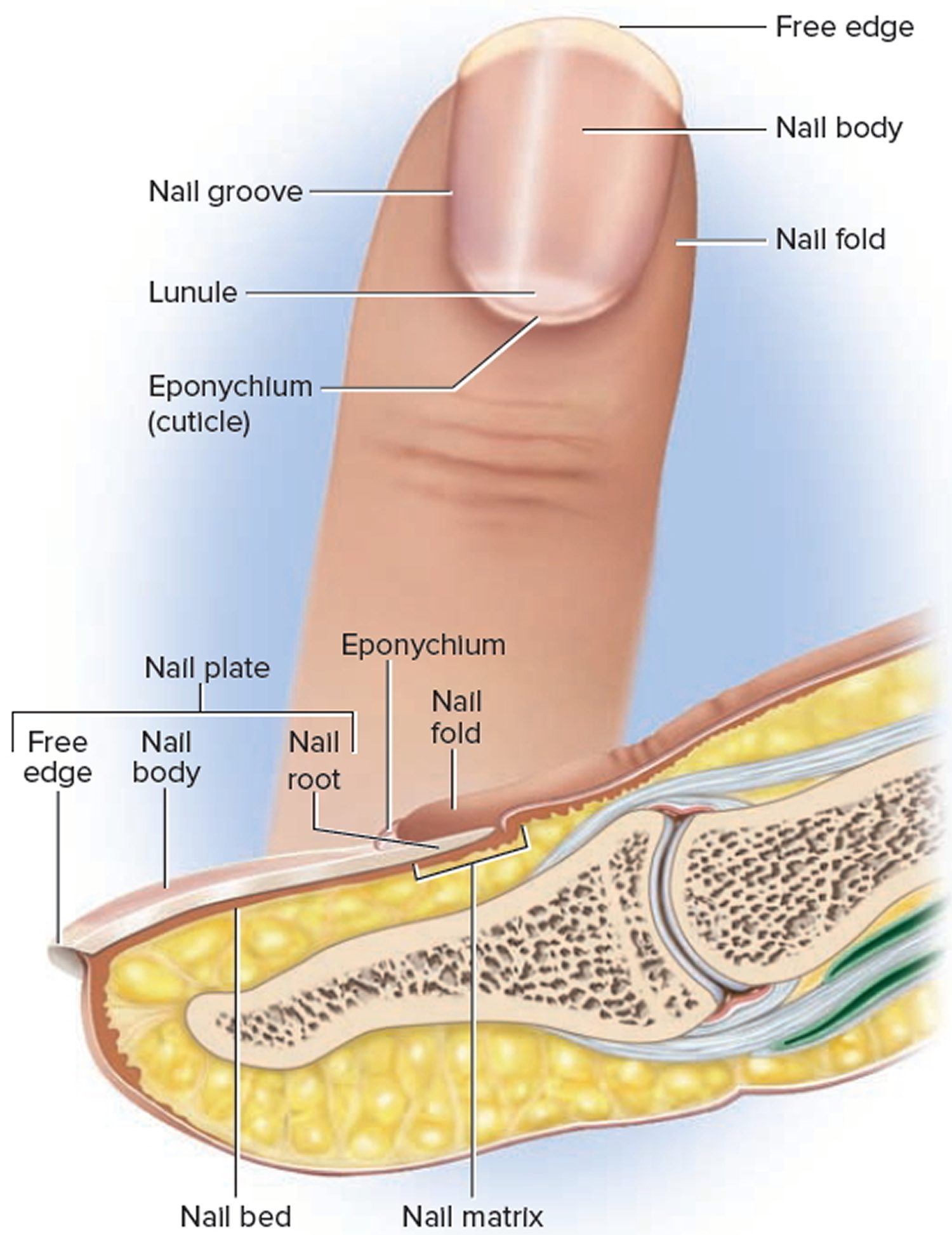
[Source 7 ]Fingernails anatomy
Nails are protective coverings on the ends of the fingers and toes. Fingernails and toenails are clear, hard derivatives of the stratum corneum. They are composed of very thin, dead, scaly cells, densely packed together and filled with parallel fibers of hard keratin. Each nail consists of a nail plate, which includes the free edge overhanging the tip of the finger or toe; that overlies a surface of skin called the nail bed. Specialized epithelial cells continuous with the epithelium of the skin produce the nail bed. The nail body, which is the visible attached part of the nail; and the nail root, which extends proximally under the overlying skin. The surrounding skin rises a bit above the nail as a nail fold, separated from the margin of the nail plate by a nail groove. The groove and the space under the free edge accumulate dirt and bacteria and require special attention when scrubbing for duty in an operating room or nursery.
The skin underlying the nail plate is the nail bed; its epidermis is called the hyponychium. At the proximal end of the nail, the stratum basale thickens into a growth zone called the nail matrix. Mitosis in the matrix accounts for the growth of the nail—about 1 mm per week in the fingernails and slightly slower in the toenails. The thickness of the matrix obscures the underlying dermal blood vessels and is the reason why an opaque white crescent, the lunule (lunula), often appears at the proximal end of a nail. A narrow zone of dead skin, the cuticle or eponychium, commonly overhangs this end of the nail.
The appearance of the fingertips and nails can be valuable in medical diagnosis. The fingertips become swollen or clubbed in response to long-term hypoxemia—a deficiency of oxygen in the blood stemming from conditions such as congenital heart defects and emphysema. Dietary deficiencies may be reflected in the appearance of the nails. An iron deficiency, for example, may cause them to become flat or concave (spoonlike) rather than convex. Contrary to popular belief, adding gelatin to the diet has no effect on the growth or hardness of the nails.
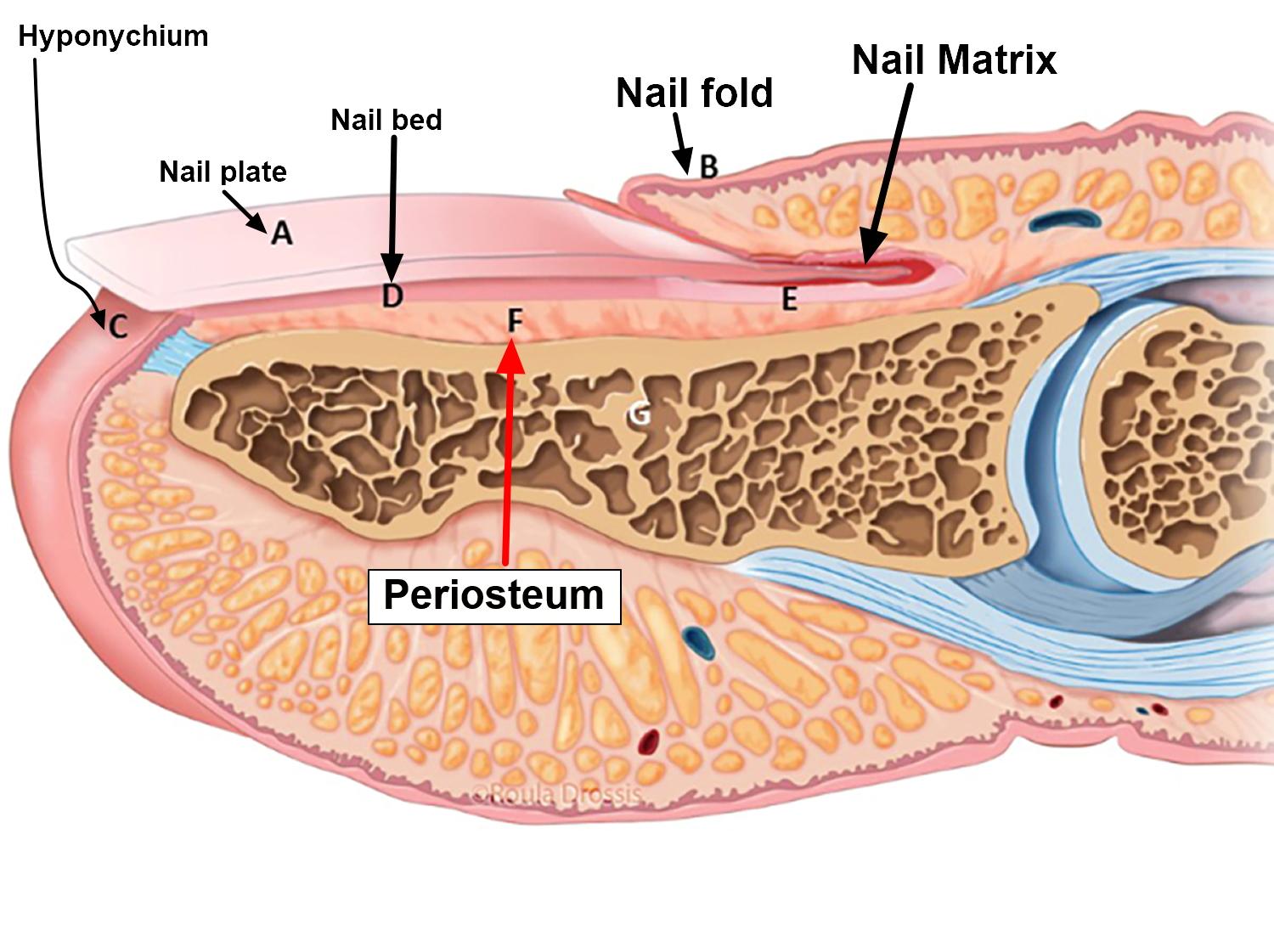
Figure 4. Fingernail
Mees lines causes
Mees lines are classically associated with arsenic poisoning 2. If arsenic poisoning is suspected, hair or tissue samples should be obtained for verification; the timing of the arsenic poisoning can be estimated based on the rate of nail plate growth 1. However, Mees’ lines also may be associated with multiple other conditions such as thallium or other heavy metal poisoning 3, Hodgkin lymphoma or Hodgkin’s disease, congestive heart failure, renal failure, carcinoid tumors, chemotherapy (i.e., cyclophosphamide, vincristine and doxorubicin), leprosy, malaria, carbon monoxide poisoning and other systemic insults 1.
In Mees lines (true leukonychia) the transverse, non-blanching white bands appear that run parallel to the lunula across the entire nail bed are caused by an insult to the distal nail matrix that does not lead to cessation in growth of the matrix, but instead causes parakeratosis of the ventral nail plate 4.
Mees lines treatment
Mees lines treatment involves diagnosing and treating the underlying cause.
References- Nail Abnormalities: Clues to Systemic Disease. Am Fam Physician. 2004 Mar 15;69(6):1417-1424. https://www.aafp.org/afp/2004/0315/p1417.html
- Sharma S, Gupta A, Deshmukh A, Puri V. Arsenic poisoning and Mees’ lines. QJM. 2016;109(8):565–566. doi:10.1093/qjmed/hcw068 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4986432
- Chauhan S, D’Cruz S, Singh R, Sachdev A. Mees’ lines. Lancet. 2008;372(9647):1410.
- Hinds G, Thomas VD. Malignancy and cancer treatment-related hair and nail change. Dermatol Clin. 2008;26:59–68.
- Piraccini BM, Iorizzo M. Drug reactions affecting the nail unit: diagnosis and management. Dermatol Clin. 2007;25:215–21.
- D’Alessandro A, Muzi G, Monaco A, Filiberto S, Barboni A, Abbritti G. Yellow nail syndrome: does protein leakage play a role?. Eur Respir J. 2001;17:149–52.
- Huang TC, Chao TY. Mees lines and Beau lines after chemotherapy. CMAJ. 2010;182(3):E149. doi:10.1503/cmaj.090501 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2826482
- Sharma V, Kumar V. Muehrcke lines. CMAJ. 2013;185(5):E239. doi:10.1503/cmaj.120269 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3602273





{kind=link}