
Nager syndrome
Nager syndrome also called Nager acrofacial dysostosis syndrome or preaxial mandibulofacial dysostosis, is a rare inherited disorder that mainly affects the development of the face, hands, and arms. The severity of Nager syndrome varies among affected individuals. Children with Nager syndrome are born with underdeveloped cheek bones (malar hypoplasia) and incomplete development of the lower jaw (mandibular hypoplasia), causing the jaw to appear abnormally small (micrognathia). They often have an opening in the roof of the mouth called a cleft palate. These abnormalities frequently cause feeding problems in infants with Nager syndrome. The airway is usually partially blocked due to the micrognathia, which can lead to life-threatening breathing problems.
People with Nager syndrome often have eyes that slant downward (downslanting palpebral fissures), no eyelashes, and a notch in the lower eyelids called an eyelid coloboma. Many affected individuals have (microtia) and/or malformed (dysplastic) external ears, often with a blind ending or absent external ear canals, resulting in hearing impairment (conductive hearing loss). About 60 percent have hearing loss caused by defects in the middle ear (conductive hearing loss). Nager syndrome does not affect a person’s intelligence, although speech development may be delayed due to hearing impairment.
Nager syndrome is distinguished from other forms of acrofacial dysostosis by the limb abnormalities, which are primarily on the thumb (radial) side of the hand and forearm including underdevelopment, malformed or absence of the thumbs and the radius bone in the forearm, and abnormal fusion of bones in the forearms (radioulnar synostosis). Their forearms may be shortened due to the partial or complete absence of a bone called the radius. Affected individuals may also have fingers that are unusually curved (clinodactyly) or fused together (syndactyly). People with Nager syndrome sometimes have difficulty fully extending their elbows. Nager syndrome can also cause bone abnormalities in the legs and feet.
Nager syndrome is a rare condition. Its prevalence is unknown. Many cases go misdiagnosed or undiagnosed, making it difficult to determine the true frequency in the general population. More than 100 cases have been reported in the medical literature 1. Nager syndrome is typically inherited in an autosomal dominant pattern and is caused by changes (mutations) in the SF3B4 gene. Although an individual with Nager syndrome can transmit the condition to his/her children, many cases occur randomly (sporadic) as a new gene change (de novo mutation) in the family.
Nager syndrome causes
More than half of cases of Nager syndrome are caused by mutations in the SF3B4 gene which is located on chromosome 1q12-q21 2. The cause of the remainder of cases is unknown; other genes are thought to be involved in the condition.
The SF3B4 gene provides instructions for making the SAP49 protein, which is one piece of a complex called a spliceosome. Spliceosomes help process messenger RNA (mRNA), which is a chemical cousin of DNA that serves as a genetic blueprint for making proteins. The spliceosomes recognize and then remove regions from mRNA molecules that are not used in the blueprint (which are called introns).
The SAP49 protein may also be involved in a chemical signaling pathway known as the bone morphogenic protein (BMP) pathway. This signaling pathway regulates various cellular processes and is involved in the growth of cells. The SAP49 protein is particularly important for the maturation of cells that build bones and cartilage (osteoblasts and chondrocytes).
SF3B4 gene mutations that cause Nager syndrome prevent the production of functional SAP49 protein. Although the effect of this protein shortage is unknown, researchers suspect that it disrupts spliceosome formation, which may impair mRNA processing and alter the activity of genes involved in the development of several parts of the body. A loss of SAP49 may also impair BMP pathway signaling, leading to abnormal development of bones in the face, hands, and arms.
Nager syndrome inheritance pattern
When caused by mutations in the SF3B4 gene, Nager syndrome follows an autosomal dominant inheritance pattern, which means one copy of the altered gene in each cell is sufficient to cause the disorder. Most cases occur as a new (sporadic or de novo) mutation at the time of the formation of the egg or sperm for that child only, and no other family members are affected. An individual who is the first one in the family to have Nager syndrome does, however, still have a 50% risk to transmit it to his or her children. Autosomal dominant Nager syndrome may also be caused by mutations in other genes. Previous reports of siblings with Nager syndrome born to apparently unaffected parents could represent a different recessive form of Nager syndrome, but are more likely due to failure to recognize the condition in a mildly affected parent or to a parent having a gene change only in the ovary or testis (gonadal mosaicism) 3.
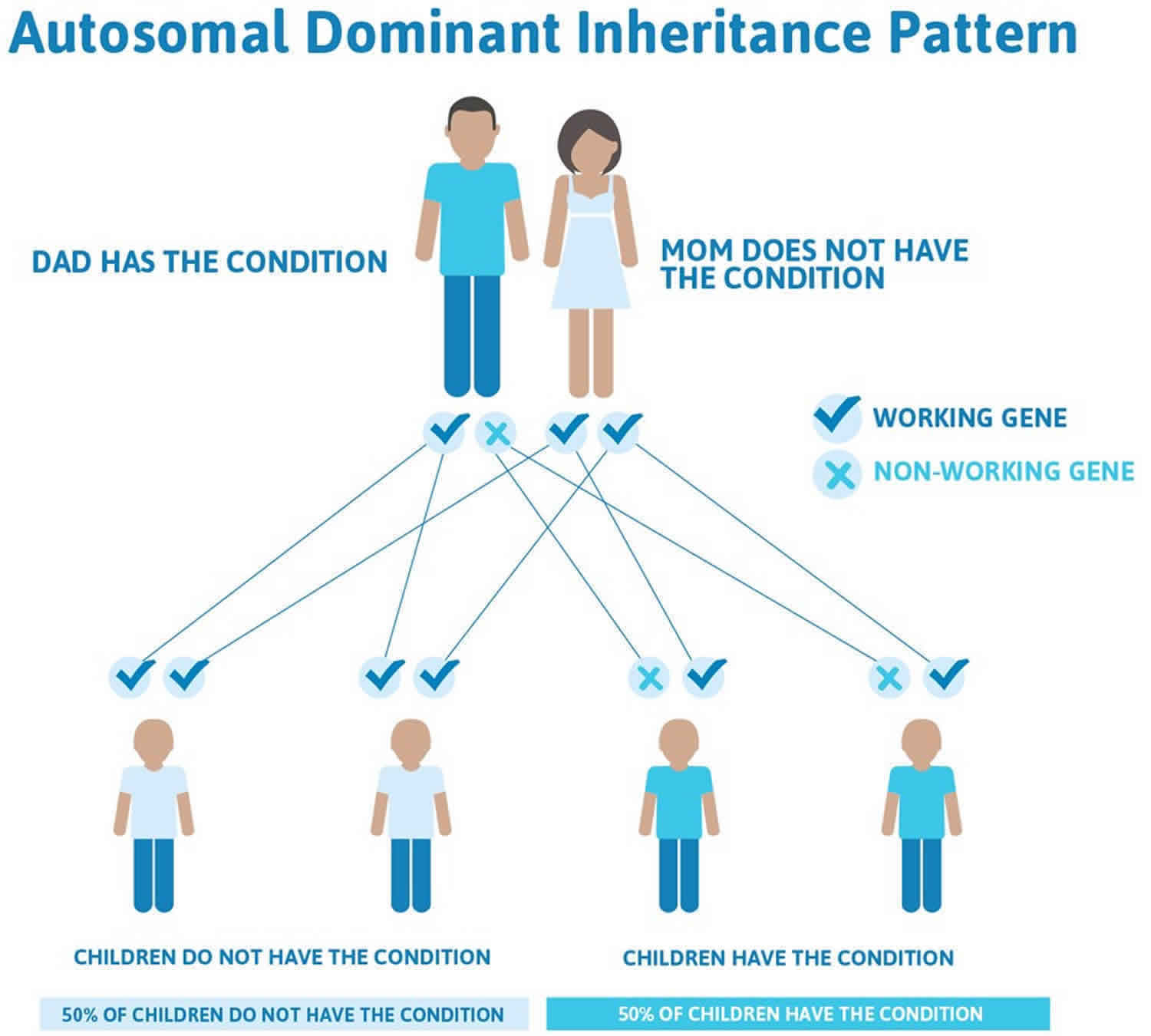
Often autosomal dominant conditions can be seen in multiple generations within the family. If one looks back through their family history they notice their mother, grandfather, aunt/uncle, etc., all had the same condition. In cases where the autosomal dominant condition does run in the family, the chance for an affected person to have a child with the same condition is 50% regardless of whether it is a boy or a girl. These possible outcomes occur randomly. The chance remains the same in every pregnancy and is the same for boys and girls.
- When one parent has the abnormal gene, they will pass on either their normal gene or their abnormal gene to their child. Each of their children therefore has a 50% (1 in 2) chance of inheriting the changed gene and being affected by the condition.
- There is also a 50% (1 in 2) chance that a child will inherit the normal copy of the gene. If this happens the child will not be affected by the disorder and cannot pass it on to any of his or her children.
Figure 1. Nager syndrome autosomal dominant inheritance pattern
Nager syndrome can also be inherited in an autosomal recessive pattern, which means both copies of a gene in each cell have mutations 1. The parents of an individual with an autosomal recessive condition each carry one copy of a mutated gene, but they typically do not show signs and symptoms of the condition. Nager syndrome is suspected to have an autosomal recessive inheritance pattern when unaffected parents have more than one affected child. The genetic cause in these families is unknown.
It is rare to see any history of autosomal recessive conditions within a family because if someone is a carrier for one of these conditions, they would have to have a child with someone who is also a carrier for the same condition. Autosomal recessive conditions are individually pretty rare, so the chance that you and your partner are carriers for the same recessive genetic condition are likely low. Even if both partners are a carrier for the same condition, there is only a 25% chance that they will both pass down the non-working copy of the gene to the baby, thus causing a genetic condition. This chance is the same with each pregnancy, no matter how many children they have with or without the condition.
- If both partners are carriers of the same abnormal gene, they may pass on either their normal gene or their abnormal gene to their child. This occurs randomly.
- Each child of parents who both carry the same abnormal gene therefore has a 25% (1 in 4) chance of inheriting a abnormal gene from both parents and being affected by the condition.
- This also means that there is a 75% ( 3 in 4) chance that a child will not be affected by the condition. This chance remains the same in every pregnancy and is the same for boys or girls.
- There is also a 50% (2 in 4) chance that the child will inherit just one copy of the abnormal gene from a parent. If this happens, then they will be healthy carriers like their parents.
- Lastly, there is a 25% (1 in 4) chance that the child will inherit both normal copies of the gene. In this case the child will not have the condition, and will not be a carrier.
These possible outcomes occur randomly. The chance remains the same in every pregnancy and is the same for boys and girls.
Figure 2. Nager syndrome autosomal recessive inheritance pattern

People with specific questions about genetic risks or genetic testing for themselves or family members should speak with a genetics professional.
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://www.findageneticcounselor.com/) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://www.abgc.net/about-genetic-counseling/find-a-certified-counselor/) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counselors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (http://www.acmg.net/ACMG/Genetic_Services_Directory_Search.aspx) has a searchable database of medical genetics clinic services in the United States.
Nager syndrome symptoms
The specific symptoms that occur may vary from one person to another, even among members of the same family. Affected individuals may develop a variety of craniofacial and limb abnormalities which usually are noticeable at birth (congenital).
Common craniofacial abnormalities include underdevelopment of the cheekbones (malar hypoplasia); an abnormally small lower jaw (micrognathia); incomplete closure of the roof of the mouth (cleft palate) and/or velopharyngeal insufficiency, in which the soft palate of the mouth does not close properly during speech; narrowing of the back of the nasal cavity (choanal atresia); malformation of the internal or external ears that can range from mild abnormality to absence of the external portion of the ear. Additional craniofacial findings in or around the eyes include downward-slanting palpebral fissures (which means that opening between the upper and lower lids slants downward), absence of tissue (colobomas) from the lower eyelids, partial or total absence of the eyelashes of the lower eyelids, and droopy or sagging of the upper eyelids (ptosis). In some patients, scalp hair may extend onto the cheek.
Micrognathia is caused by underdevelopment (hypoplasia) of the lower jaw bone (mandible). Severe mandibular hypoplasia along with cleft palate and choanal atresia can result in feeding difficulties and/or severe breathing difficulties during infancy. In some cases, if left untreated, breathing difficulties can cause life-threatening complications. Affected individuals may have temporomandibular joint dysfunction (TMJD); the temporomandibular joint connects the jaws to the side of the head. Temporomandibular joint dysfunction can cause pain of the jaw, face and neck, stiff jaw muscles, and upper and lower teeth that do not meet properly when closing the mouth (malocclusion).
Malformation of the ears can contribute to affected individuals developing conductive hearing loss. Conductive hearing loss occurs due to lack of conduction of sound from the outer or middle ear to the inner ear. Degree of hearing loss can vary. Hearing impairment may cause speech development to be delayed.
Individuals with Nager syndrome also have abnormalities affecting the arms and hands including underdevelopment or absence of the thumbs, the presence of an extra (third) copy of a bone known as the phalange within the thumb (triphalangeal thumbs), and underdevelopment of the forearm bone on the thumb side of the arm (radius). Less often, webbing (syndactyly) of the fingers may occur, or certain fingers may be fixed or stuck in a bent position (camptodactyly). The formation of an abnormal bone or soft tissue connection between the ulna and the radius, two main bones of the forearm (radioulnar synostosis) may also occur. Because of these abnormalities, the forearms may appear abnormally short. Some individuals may have difficulty fully straightening their arms because the range of motion of the elbow is limited. A few very severely affected individuals have severely shortened upper limbs (phocomelia).
Although abnormalities of the hands and forearms are more common, some affected individuals have abnormalities affecting the feet and lower legs including underdeveloped or absent toes, webbing of the toes, clubfeet, and the abnormal turning inward of the big toe towards the index toe (hallux valgus).
While most individuals with Nager syndrome are healthy, a few severely affected individuals have serious internal malformations involving the kidney and/or the heart. Additional rare symptoms that have been reported in the medical literature include diaphragmatic hernia (an abnormal connection between the chest and abdomen), and underdevelopment of the larynx which can contribute to respiratory problems, as well as additional skeletal abnormalities such as underdevelopment of the first rib, abnormal curvature of the spine (scoliosis), or dislocation of the hip.
Nager syndrome diagnosis
A diagnosis of Nager syndrome is based upon a thorough clinical evaluation, a detailed patient history, and identification of characteristic physical findings. Most of the associated abnormalities are present at birth (congenital).
Molecular genetic testing can confirm a diagnosis of Nager syndrome. Molecular genetic testing can detect a mutation the SF3B4 gene, but is available only as a diagnostic service at specialized laboratories.
Clinical testing and workup
Specialized x-ray studies will confirm the presence and/or extent of certain observed craniofacial abnormalities. For example, such imaging tests show the abnormally small jaw (micrognathia) due to underdevelopment of the lower jaw bone (mandibular hypoplasia) as well as the underdeveloped cheekbone (malar hypoplasia).
Nager syndrome treatment
The treatment of Nager syndrome is directed toward the specific symptoms that are apparent in each individual. Treatment may require the coordinated efforts of a team of specialists. Pediatricians, oral surgeons, plastic surgeons, pediatric ear, nose and throat specialists (pediatric otolaryngologists), specialists in diagnosing and treating eye disorders (ophthalmologists), specialists in diagnosing and treating ear disorders (otologists), specialists in treating hearing loss (audiologists), psychologists, and other healthcare professionals may need to systematically and comprehensively plan an affect child’s treatment. Affected individuals may benefit from referral to a craniofacial center.
In infants with Nager acrofacial dysostosis who experience respiratory distress require immediate attention and may require a tracheostomy. A tracheostomy is a surgical procedure on the neck that opens a direct airway through an incision in the windpipe , through which a small tube is inserted to assist with breathing.
Infants with feeding difficulties may require surgery and/or placement of a feeding tube (gastrostomy) in order to maintain proper nutrition.
Surgery may be required to correct abnormalities of the jaws, limbs, and eyes. Surgery and/or speech therapy may be necessary when cleft palate or cleft lip is present. Skeletal malformations such as rib abnormalities, limited range of motion of the elbows, and scoliosis may require surgical intervention. Congenital heart defects often require surgery.
Early intervention with appropriate physical, occupational, and speech therapy services is important in ensuring that affected children reach their full potential. Physical and occupational therapy may be necessary to aid in walking and using one’s hands. Speech therapy may be of benefit for individuals with speech development delays due to hearing loss. Hearing loss may require tubes to be implanted in the ears or the use of a hearing aid.
Genetic counseling is recommended for affected individuals and their families. Psychosocial support for the entire family is essential as well.
References




{kind=link}