
What is pitted keratolysis
Pitted keratolysis is a descriptive term for a superficial bacterial skin infection that affects the soles of the feet, and less often, the palms of the hands 1. Pitted keratolysis is one of the causes of smelly feet. Pitted keratolysis is characterized by whitish skin and clusters of punched-out pits. Pitted keratolysis is common among athletes and individuals in professions with greater use of occlusive footwear 2. Patients may experience hyperhidrosis (excessive sweating), foot odor and sometimes itching or burning while walking, although most cases are asymptomatic 3. The lesions tend to be multiple, superficial rounded depressions, 0.5 to 7 mm in diameter, affecting mainly weight-bearing areas of the soles. Palms are less commonly involved. Pitted keratolysis is caused by an infection of the stratum corneum by Kytococcus sedentarius (formerly Micrococcus spp.), though Dermatophilus congolensis and Corynebacterium spp. have also been implicated 4. Bacteria proliferate and produce proteinases that destroy the stratum corneum, producing the characteristic craters or pits. The odor linked to pitted keratolysis is due to the production of sulphur compounds.
The diagnosis of pitted keratolysis is clinical 5. Cultures, if taken, show gram-positive coccobacilli or bacilli. Examination with a Wood light is not reliable for diagnosis and may be negative or show coral-red fluorescence when Corynebacterium spp. is implicated 6. Dermoscopy usually reveals abundant pits with well-marked walls that sometimes show the bacterial colonies 7. A potassium hydroxide examination of the lesions can exclude tinea pedis 5.
Pitted keratolysis has an excellent prognosis; effective treatment clears both the lesion and the odor in 3-4 weeks. Topical antibiotics are effective, easy to use and accepted by patients. Recommendations include twice daily application of erythromycin solution or gel 8, 1% clindamycin hydrochloride solution 9, fusidic acid cream and mupirocin cream 10.
Figure 1. Pitted keratolysis feet

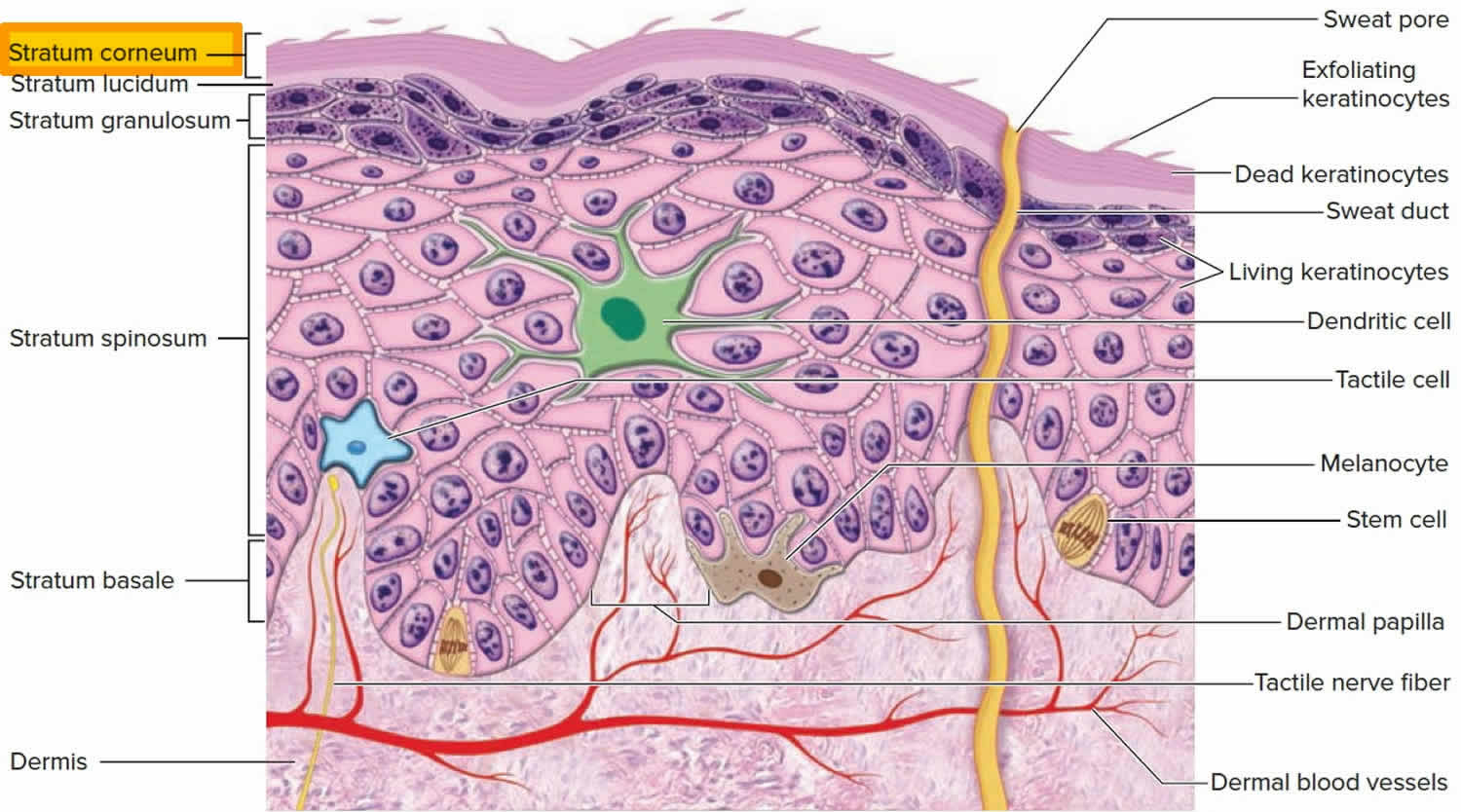
Figure 2. Skin structure

Figure 3. Skin epidermis
Is pitted keratolysis contagious?
Yes. More than the half of the female patients (58.8%) with pitted keratolysis had a history of regular pedicure and foot care in a spa salon 11. Moisture and inappropriate hygiene may be the predisposing factors in such patients.
Pitted keratolysis is caused by a cutaneous infection with Kytococcus sedentarius 12, Dermatophilus congolensis 13 and the Corynebacterium species 14. Under appropriate conditions (i.e. prolonged occlusion, hyperhidrosis, increased skin surface pH), these bacteria proliferate and produce proteinases that destroy the stratum corneum, creating pits. Kytococcus sedentarius has been found to produce two keratin-degrading enzymes, protease P1 and P2 respectively 15. The malodor associated with pitted keratolysis is presumed to be due to the production of sulfur-compound by-products, such as thiols, sulfides and thioesters 16.
What is the cause of pitted keratolysis?
Pitted keratolysis is caused by several bacterial species, including corynebacteria, Dermatophilus congolensis, Kytococcus sedentarius, actinomyces and streptomyces.
The bacteria proliferate in moist conditions. The pitting is due to destruction of the horny cells (stratum corneum) by protease enzymes produced by the bacteria.
The bad smell is due to sulfur compounds produced by the bacteria: thiols, sulfides and thioesters.
Who’s at risk of pitted keratolysis?
Pitted keratolysis is much more common in males than in females. Occupations at risk include:
- Farmers
- Athletes
- Sailors or fishermen
- Industrial workers
- Military personnel
Females offering pedicure and foot care in a spa salon may also be affected by pitted keratolysis.
Theoretically, both males and females should be affected; however, most written case reports or studies have involved male patients 10. Adult males with sweaty feet are most susceptible to pitted keratolysis (97% of the cases) 17. Few cases have been reported in the elderly 17. Pitted keratolysis is reported to be more common among barefooted laborers/farmers, marine workers, soldiers and industrial workers wearing occluded shoes for prolonged periods.
Factors that lead to the development of pitted keratolysis include:
- Hot, humid weather
- Occlusive footwear, such as rubber boots or vinyl shoes
- Excessive sweating of hands and feet (hyperhidrosis)
- Thickened skin of palms and soles (keratoderma)
- Diabetes mellitus
- Advanced age
- Immunodeficiency
How can pitted keratolysis be prevented?
Pitted keratolysis will quickly recur unless the feet are kept dry. The following precautions should be taken to prevent recurrences:
- Wear boots for as short a period as possible
- Wear socks which effectively absorb sweat, i.e., cotton and/or wool
- Wear open-toed sandals whenever possible
- Wash feet with soap or antiseptic cleanser twice daily
- Apply antiperspirant to the feet at least twice weekly
- Do not wear the same shoes two days in a row — dry them out
- Do not share footwear or towels with others.
Pitted keratolysis symptoms
The result is very smelly feet, due to infection of the soles. Either the forefoot or the heel or both become white with clusters of punched-out pits. The appearance is more dramatic when the feet are wet. Very rarely, the fingers are similarly affected. There is a variant of pitted keratolysis where there are more diffuse red areas on the soles.
- Mostly affects the soles, forefoot, the heel or both. Palms are rarely infected.
- Results in a whitish skin surface with clusters of multiple, fine punched-out pits.
- Pits often join together (coalesce) to form larger, crater-like lesion.
- A variant of pitted keratolysis presents with diffuse red areas on the soles.
The most commonly reported symptom is malodor. The pits themselves are usually asymptomatic but may cause soreness or itching when walking.
Pitted keratolysis treatment
Changing footwear and socks regularly as well as airing out or rotating shoes is key to management. Avoiding use of occlusive footwear, reduction of foot friction with properly fitting footwear, using absorbent cotton socks, wearing open toed sandals whenever possible, washing feet with soap or antibacterial cleanser twice a day, and avoiding sharing of footwear or towels. In some cases it may be helpful to reduce any associated hyperhidrosis with the application of a roll-on antiperspirant or 20% aluminum chloride solution 10.
Topical antibiotics are the first line of medical treatment 18.
Pitted keratolysis can be successfully treated with topical antibiotics and antiseptics including:
- Erythromycin
- Clindamycin
- Mupirocin
- Fusidic acid
- Benzoyl peroxide
Oral erythromycin is also helpful, may shorten the treatment period 19.
Twice-daily application of erythromycin 1% (solution or gel), 1% clindamycin hydrochloride solution, fusidic acid or mupirocin 2% are recommended 20. Botulinum toxin or iontophoresis for localized treatment of sweating may be useful 20. There is also evidence for adding benzoyl peroxide to the antibiotics treatment 21. Prognosis is excellent, and lesions usually resolve in three to four weeks 22.
References- Pitted keratolysis. https://www.dermnetnz.org/topics/pitted-keratolysis/
- Pitted keratolysis; physicians’ treatment and their perceptions in Dutch army personnel. van der Snoek EM, Ekkelenkamp MB, Suykerbuyk JC. J Eur Acad Dermatol Venereol. 2013 Sep; 27(9):1120-6
- Fernández-Crehuet P, Ruiz-Villaverde R. Pitted keratolysis: an infective cause of foot odour. CMAJ : Canadian Medical Association Journal. 2015;187(7):519. doi:10.1503/cmaj.140809. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4401600/
- Corynebacterium-associated skin infections. Blaise G, Nikkels AF, Hermanns-Lê T, Nikkels-Tassoudji N, Piérard GE. Int J Dermatol. 2008 Sep; 47(9):884-90.
- Pranteda G, Carlesimo M, Pranteda G, et al. Pitted keratolysis, erythromycin, and hyperhidrosis. Dermatol Ther 2014;27:101–4.
- Blaise G, Nikkels AF, Hermanns-Lê T, et al. Corynebacterium-associated skin infections. Int J Dermatol 2008;47:884–90.
- Lockwood LL, Gehrke S, Navarini AA. Dermoscopy of pitted keratolysis. Case Rep Dermatol 2010;2:146–8.
- Michel L, Ramsey. Pitted keratolysis. Phys Sport Med 1996;24:1-4.
- Burkhart CG. Pitted keratolysis. A new form of treatment. Arch Dermatol 1980;116:1104.
- English JC. Pitted keratolysis. eMedicine J 2003;11:1-7.
- Kaptanoglu AF, Yuksel O, Ozyurt S. Plantar pitted keratolysis: a study from non-risk groups. Dermatology Reports. 2012;4(1):e4. doi:10.4081/dr.2012.e4. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4212664/
- Nordstrom KM, McGinley KJ, Cappiello L, Zechman JM, Leydel JJ. Pitted keratolysis. The role of Micrococcus sedentarius . Arch Dermatol 1987;123:1320-5.
- Woodgyer AJ, Baxter M, Rush-Munro FM. Isolation of Dermatophilus congolensis from two New Zealand cases of pitted keratolysis. Aust J Dermatol 1985;26:29-35.
- Taplin D, Zaias N. The etiology of pitted keratolysis. Excerpta Medica Princeton. Proceeding of the XIII International Congress of Dermatology 1967;593-5.
- Longshaw CM, Wright JD, Farrell AM, Holland KT. Kytococcus sedentarius the organism associated with pitted keratolysis, produces two Keratin – degrading enzymes. J Appl Microbiol 2002;93:810-6.
- Nordstrom KM, McGinley KJ, Cappiello L, Leyden JJ. The etiology of the malodor associated with pitted keratolysis. J Invest Dermatol 1986;87:159.
- Takama H, Tamada Y, Yano K, Nitta Y, Ikeya T. Pitted keratolysis. Clinical manifestations in 53 cases. Br J Dermatol 1997;137:282-5.
- van der Snoek EM, Ekkelenkamp MB, Suykerbuyk JC. Pitted keratolysis: physicians’ treatment and their perceptions in Dutch army personnel. J Eur Acad Dermatol Venereol 2013;27:1120–6. ((Pitted keratolysis. Singh G, Naik CL. Indian J Dermatol Venereol Leprol. 2005 May-Jun; 71(3):213-5.
- Pitted keratolysis. Singh G, Naik CL. Indian J Dermatol Venereol Leprol. 2005 May-Jun; 71(3):213-5.
- van der Snoek EM, Ekkelenkamp MB, Suykerbuyk JC. Pitted keratolysis: physicians’ treatment and their perceptions in Dutch army personnel. J Eur Acad Dermatol Venereol 2013;27:1120–6.
- Vlahovic TC, Dunn SP, Kemp K. The use of a clindamycin 1%–benzoyl peroxide 5% topical gel in the treatment of pitted keratolysis: a novel therapy. Adv Skin Wound Care 2009;22: 564–6. https://www.ncbi.nlm.nih.gov/pubmed/19935134
- Kaptanoglu AF, Yuksel O, Ozyurt S. Plantar pitted keratolysis: a study from non-risk groups. Dermatology Reports. 2012;4(1):e4. doi:10.4081/dr.2012.e4. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4212664





{kind=link}