What is pneumonia
Pneumonia is an infection of the air sacs (alveoli) in one or both lungs that is usually caused by a bacterial infection. The air sacs or the alveoli may fill with fluid or pus (purulent material), causing cough with phlegm (mucus or sputum or a slimy substance) or pus, fever, chills, and difficulty breathing. Viruses, bacteria, and fungi can all cause pneumonia. In the United States, common causes of viral pneumonia are influenza and respiratory syncytial virus (RSV). A common cause of bacterial pneumonia is Streptococcus pneumoniae (pneumococcus that cause pneumococcal pneumonia). Many different types of bacteria, including Haemophilus influenzae and Staphylococcus aureus, can also cause pneumonia, as well as other viruses and, more rarely, fungi. Pneumonia can also result from being on a ventilator, which is known as ventilator-associated pneumonia.
Pneumonia can range in seriousness from mild to life-threatening. How serious your pneumonia is depends on your age, your overall health, and what caused your infection. Pneumonia is most serious for infants and young children, people older than age 65, and people with health problems or weakened immune systems.
Your lungs have 2 main parts: airways (also called bronchial tubes) and alveoli (also called airsacs). When you breathe, the air moves down through your airways and into your alveoli (see Figures 4 and 5). From the alveoli, oxygen goes into your blood while carbon dioxide moves out of your blood. When you have pneumonia, your alveoli get inflamed (irritated and swollen) and fill with fluid. This makes it difficult for you to breathe.
Pneumonia is usually caused by bacteria or a virus. It can also be caused by fungi or irritants that you breathe into your lungs.
The symptoms of pneumonia can develop suddenly over 24 to 48 hours, or they may come on more slowly over several days.
Common symptoms of pneumonia include:
- a cough – which may be dry, or produce thick yellow, green, brown or blood-stained mucus (phlegm)
- difficulty breathing – your breathing may be rapid and shallow, and you may feel breathless, even when resting
- rapid heartbeat
- fever
- feeling generally unwell
- sweating and shivering
- loss of appetite
- chest pain – which gets worse when breathing or coughing
Less common symptoms include:
- coughing up blood (hemoptysis)
- headaches
- fatigue
- nausea or vomiting
- wheezing
- joint and muscle pain
- feeling confused and disorientated, particularly in elderly people
In the US, pneumonia affects around 8 in 1,000 adults each year. It’s more widespread in autumn and winter.
Pneumonia can affect people of any age, but it’s more common and can be more serious in certain groups of people, such as the very young or the elderly. People in these groups are more likely to need hospital treatment if they develop pneumonia.
Some types of pneumonia can be prevented by vaccines. Good hygiene and heart-healthy living can also lower your risk for pneumonia.
To diagnose pneumonia, your healthcare provider will review your medical history, perform a physical exam, and order diagnostic tests such as a chest X-ray. This information can help determine what type of pneumonia you have.
Treatment for pneumonia depends on the type of pneumonia, which germ is causing it, and how severe it is:
- Antibiotics treat bacterial pneumonia and some types of fungal pneumonia. They do not work for viral pneumonia.
- In some cases, your doctor may prescribe antiviral medicines for viral pneumonia
- Antifungal medicines treat other types of fungal pneumonia
You may need to be treated in a hospital if your symptoms are severe or if you are at risk for complications. While there, you may get additional treatments. For example, if your blood oxygen level is low, you may receive oxygen therapy.
It may take time to recover from pneumonia. Some people feel better within a week. For other people, it can take a month or more.
Is pneumonia contagious?
It’s usually safe for someone with pneumonia to be around others, including family members.
However, people with a weakened immune system are less able to fight off infections, so it’s best they avoid close contact with a person with pneumonia.
Pneumonia is commonly caused by viruses or bacteria passed from one person to another. But healthy people are normally able to fight off these germs without pneumonia developing. So it’s usually safe for someone with pneumonia to be around others, including family members.
You can help prevent pneumonia and other respiratory infections by following good hygiene practices, such as washing your hands regularly and disinfecting frequently touched surfaces, taking good care of your medical problems, and quitting smoking.
Pneumonia can be life-threatening if left untreated, especially in people who smoke, have heart disease, weakened immune system or have lung problems, children younger than age 2 with signs and symptoms and in adults 65 years of age and older. People receiving chemotherapy or taking medication that suppresses the immune system.
You should see your doctor if you have a cough that won’t go away especially if you’re coughing up pus, shortness of breath, difficulty breathing, chest pain and persistent fever of 102 °F (39 °C) or higher.
You should also see your doctor if you suddenly begin to feel worse after having a cold or the flu.
It’s especially important that people in these high-risk groups see a doctor:
- Adults older than age 65
- Children younger than age 2 with signs and symptoms
- People with an underlying health condition or weakened immune system
- People receiving chemotherapy or taking medication that suppresses the immune system
For some older adults and people with heart failure or chronic lung problems, pneumonia can quickly become a life-threatening condition.
Figure 1. Lungs anatomy
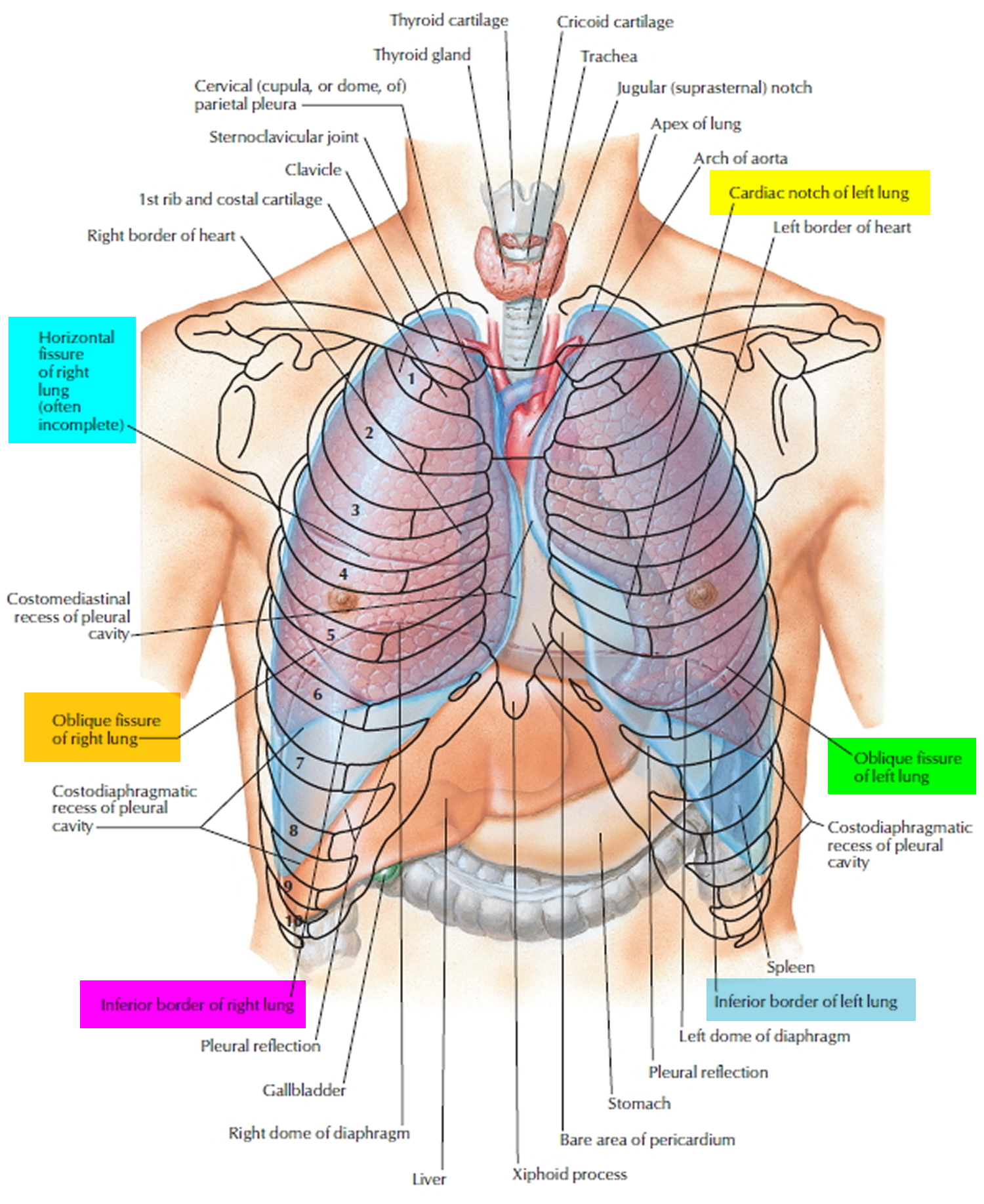
Figure 2. Bronchial tree of the lungs
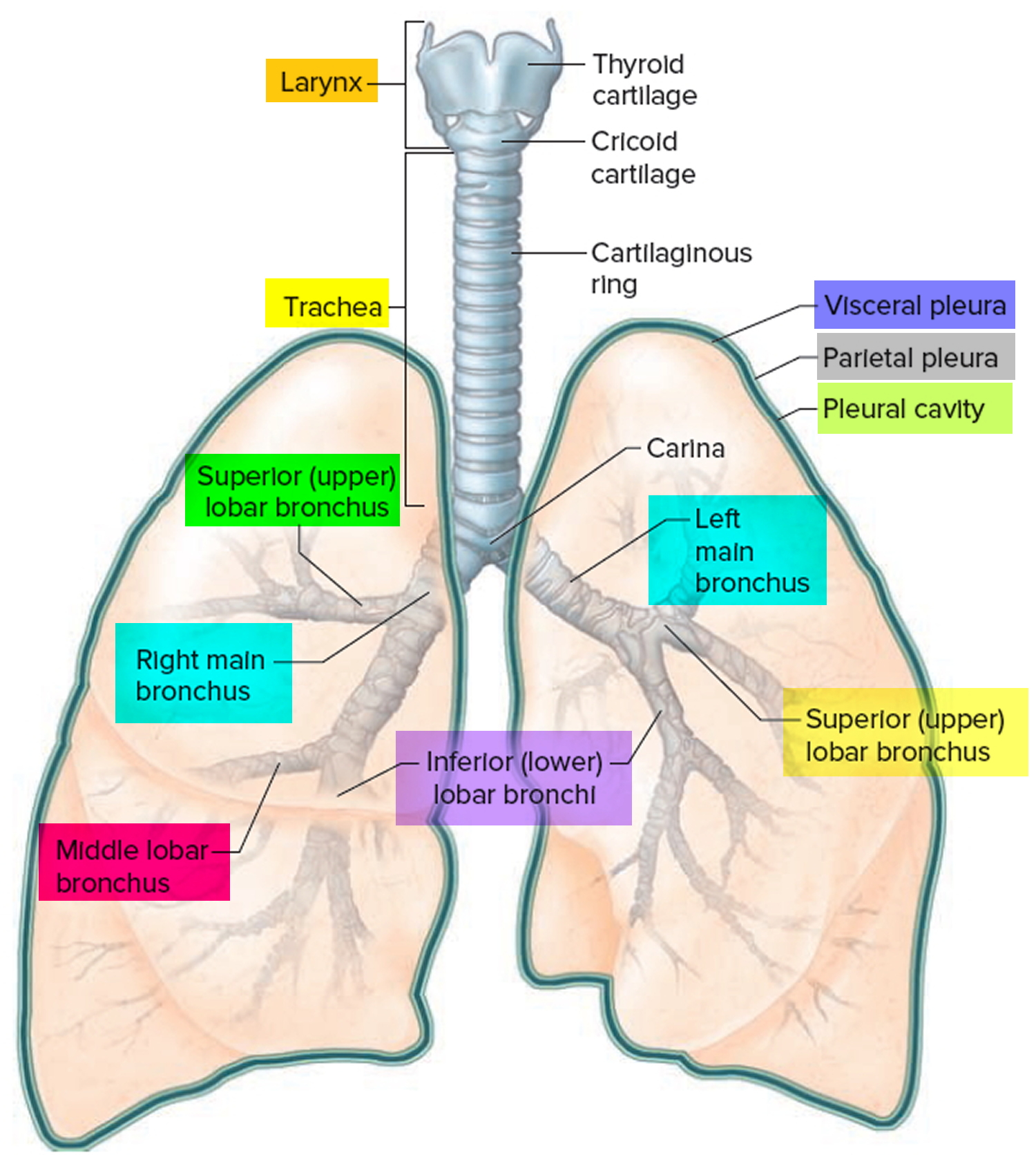
Figure 3. Bronchopulmonary segments
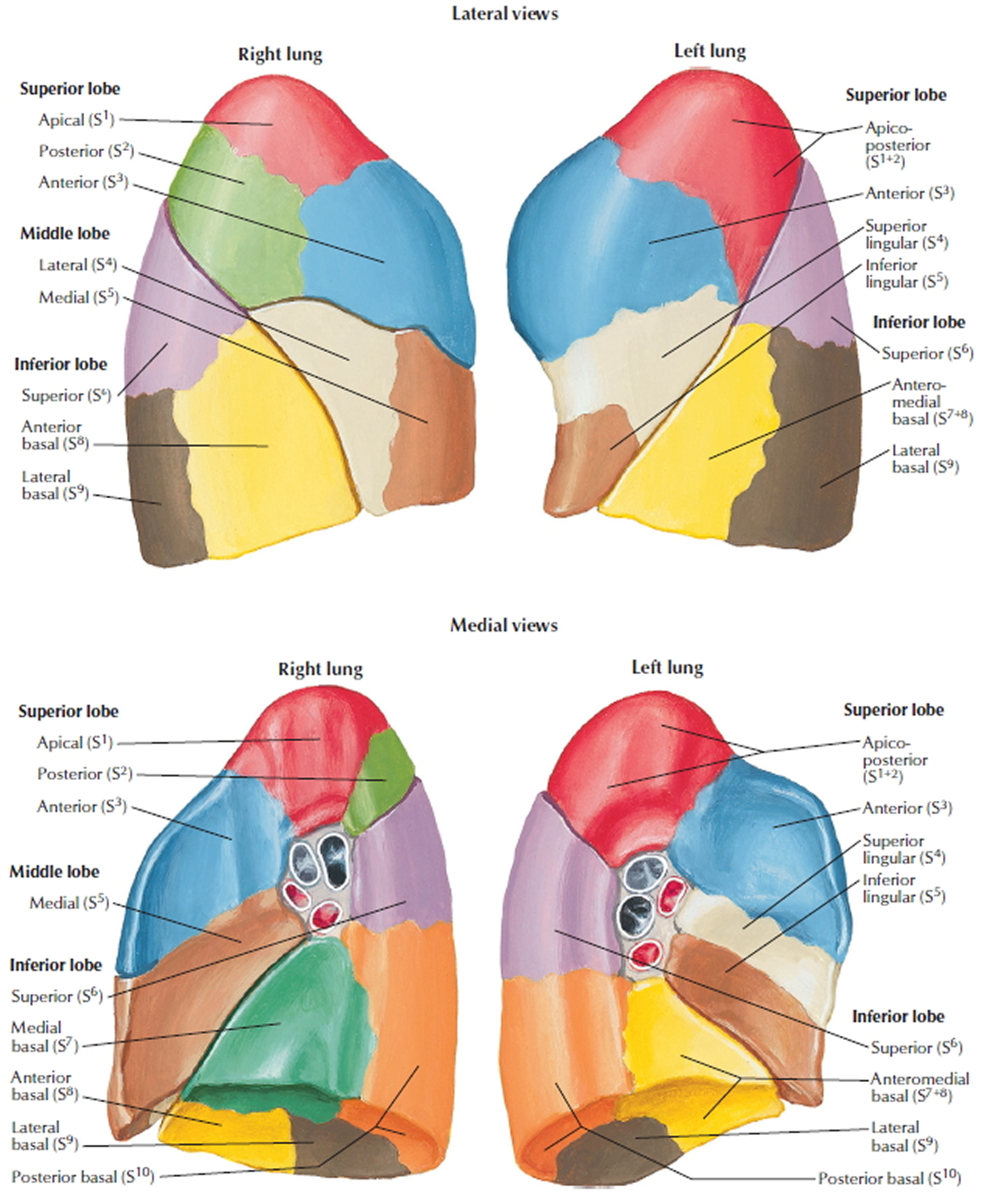
Figure 4. Lungs alveoli
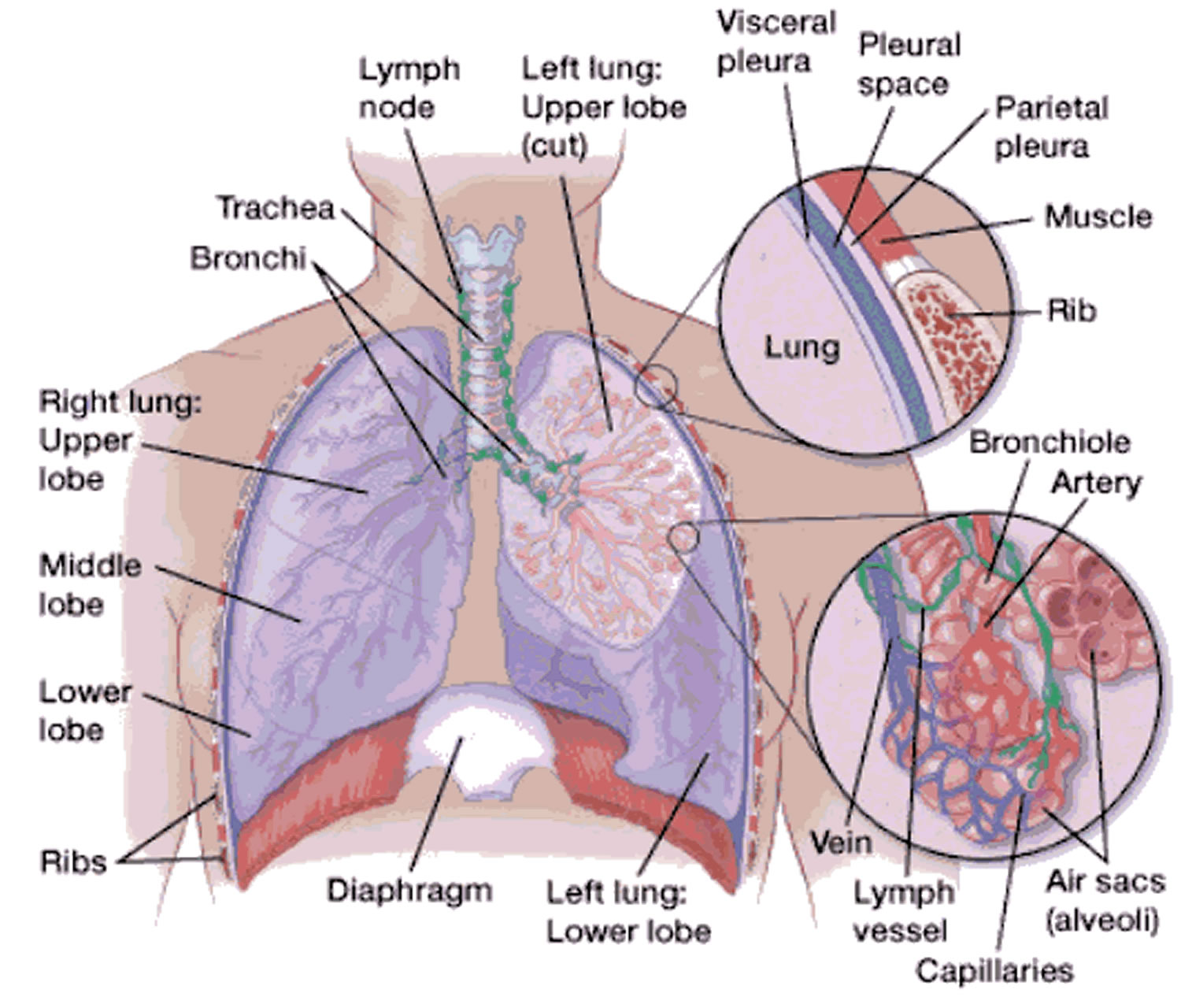 Figure 5. Pulmonary Alveoli (microscopic view)
Figure 5. Pulmonary Alveoli (microscopic view)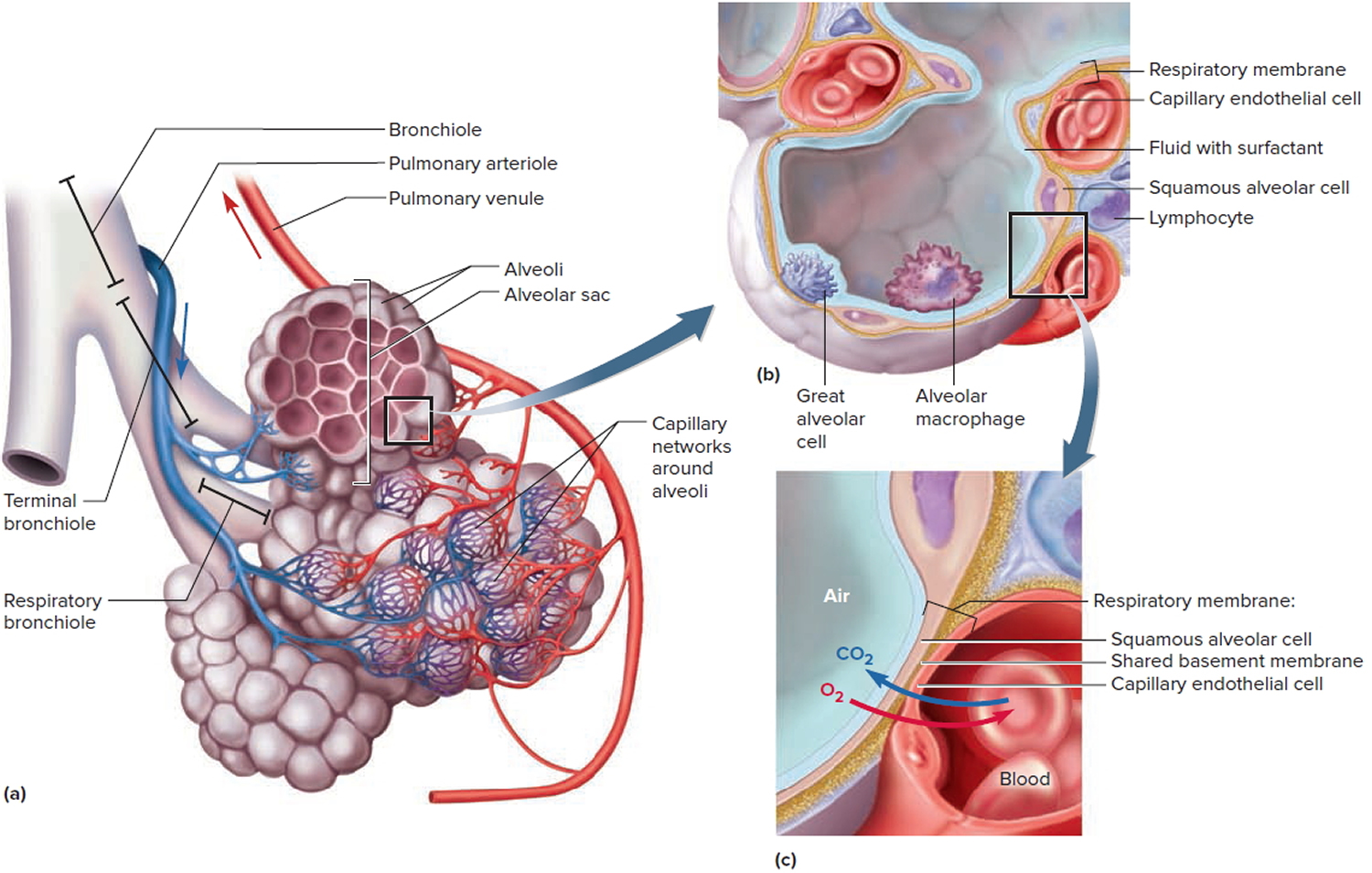
Pneumonia signs and symptoms
The signs and symptoms of pneumonia vary from mild to severe, depending on your risk factors, the type of germ causing the infection, and the type of pneumonia you have. Common symptoms are similar to the symptoms caused by a cold or the flu.
Signs and symptoms of pneumonia may include:
- Cough with or without mucus
- Fever, sweating and shaking chills
- Difficulty breathing
- Chills
- Chest pain when you breathe or cough
- Confusion or changes in mental awareness (in adults age 65 and older)
- Fatigue
- Lower than normal body temperature (in adults older than age 65 and people with weak immune systems)
- Nausea, vomiting or diarrhea
- Shortness of breath
- Low oxygen levels in your blood, measured with a pulse oximeter
You may also have other symptoms, including a headache, muscle pain, extreme tiredness, nausea (feeling sick to your stomach) and sweat.
If you have any of these symptoms, or if you suddenly start getting worse after having a cold or the flu, see your doctor.
Older adults and people who have serious illnesses or weakened immune systems may not have the typical symptoms. They may have a lower-than-normal temperature instead of a fever. Older adults who have pneumonia may feel weak or suddenly confused.
Sometimes newborns and babies don’t have typical symptoms either. They may vomit, have a fever, cough, or appear restless or tired and without energy. Babies may also show the following signs of breathing problems:
- Bluish tone to the skin and lips
- Grunting
- Pulling inward of the muscles between the ribs when breathing
- Rapid breathing
- Widening of the nostrils with each breath.
Pneumonia types
There are 4 types of pneumonia:
- Community-acquired pneumonia is the most common type of pneumonia. You can catch it in public areas (such as work, school, the grocery store or the gym). Bacteria, a virus, fungi or irritants in the air can cause community-acquired pneumonia. The bacteria Streptococcus pneumoniae is the most common cause of this type of pneumonia (pneumococcal pneumonia). This type of pneumonia can also develop after you have a cold or the flu.
- Hospital-acquired pneumonia (also called institution-acquired pneumonia) is a type of pneumonia that you can catch while you are staying in the hospital, especially if you are staying in an intensive care unit (ICU) or are using a ventilator to help you breathe. This type of pneumonia also includes pneumonia that develops after you have major surgery (such as chest surgery) and pneumonia that develops while staying in or receiving treatment in kidney dialysis centers and chronic care centers. It can be very dangerous, especially for young children, older adults and people who have weakened immune systems.
- Aspiration pneumonia is type of pneumonia that develops after you inhale particles into your lungs. This occurs most often when small particles enter your lungs after vomiting and you are not strong enough to cough the particles out of your lungs.
- Opportunistic pneumonia is a type of pneumonia that affects people who have weakened immune systems. It is caused by certain organisms that do not typically make healthy people sick, but they can be dangerous for people who have conditions such as the human immunodeficiency virus (HIV), acquired immunodeficiency syndrome (AIDS), chronic obstructive pulmonary disease (COPD) or people who have recently had an organ transplant.
Community-acquired pneumonia
Community-acquired pneumonia is the most common type of pneumonia. Community-acquired pneumonia occurs outside of hospitals, nursing homes, long‐term care facilities or other health care facilities 1. Community-acquired pneumonia may be caused by:
- Bacteria. The most common cause of bacterial pneumonia in the U.S. is Streptococcus pneumoniae. This type of pneumonia can occur on its own or after you’ve had a cold or the flu. It may affect one part (lobe) of the lung, a condition called lobar pneumonia.
- Bacteria-like organisms. Mycoplasma pneumoniae also can cause pneumonia. It typically produces milder symptoms than do other types of pneumonia. Walking pneumonia is an informal name given to this type of pneumonia, which typically isn’t severe enough to require bed rest.
- Fungi. This type of pneumonia is most common in people with chronic health problems or weakened immune systems, and in people who have inhaled large doses of the organisms. The fungi that cause it can be found in soil or bird droppings and vary depending upon geographic location.
- Viruses. Some of the viruses that cause colds and the flu can cause pneumonia. Viruses are the most common cause of pneumonia in children younger than 5 years. Viral pneumonia is usually mild. But in some cases it can become very serious.
More than 100 different micro‐organisms have been associated with community-acquired pneumonia 2. Furthermore, a patient with community-acquired pneumonia can be infected with more than one microbe, as in the case of a bacterial superinfection of an underlying influenza infection. The most common pathogens in normal hosts include Streptococcus pneumoniae (S. pneumoniae) (usually by far the most common), Chlamydia pneumoniae (C. pneumoniae), Haemophilus influenzae (H. influenzae), Mycoplasma pneumoniae (M. pneumoniae) and influenza viruses 3.
The incidence of community-acquired pneumonia in the United States is more than 5 million per year; 80% of these new cases are treated as outpatients with a mortality rate of less than 1%, and 20% are treated as in hospital with a mortality rate of 12% to 40% 4.
The incidence of community-acquired pneumonia varies among different genders; for example, it is more common in males and African Americans than females and other Americans 4. However, the total number of deaths has been on the rise among females 5. The incidence rates are higher at extremes of age; the adult rate is usually 5.15 to 7.06 cases per 1000 persons per year, but in the population of age less than 4 years and greater than 60 years, the rate is more than 12 cases per 1000 persons. In 2005, influenza and pneumonia combined was the eighth most common cause of death in the United States and the seventh most common cause of death in Canada. The mortality rate is variable among different regions, such as 7.3% for the United States and Canada, 9.1% for Europe, and 13.3% for Latin America 6, 7.
Severe community-acquired pneumonia is defined as the presence of one major criterion or at least three minor criteria 8:
- Major criteria
- Respiratory failure requiring mechanical ventilation
- Severe shock requiring vasopressors
- Minor criteria
- Blood urea nitrogen ≥ 20 mg per dL (7.14 mmol per L)
- Confusion or disorientation
- Core temperature < 96.8°F (36°C)
- Hypotension requiring aggressive fluid resuscitation
- Multilobar infiltrates
- Partial pressure of oxygen (PaO2)/fraction of inspired oxygen (FiO2) ratio ≤ 250
- Platelet count < 100 × 10³ per μL (100 × 109 per L)
- Respiratory rate ≥ 30 breaths per minute
- White blood cell count < 4,000 per μL (4.00 × 109 per L) due to infection alone (i.e., not chemotherapy induced)
Note: Diagnosis of severe community-acquired pneumonia requires one major criterion or three or more minor criteria. Features of severe community-acquired pneumonia in children and young people include difficulty breathing, oxygen saturation less than 90%, raised heart rate, grunting, very severe chest indrawing, inability to breastfeed or drink, lethargy and a reduced level of consciousness.
The Pneumonia Severity Index (Table 1) also known as PORT score, is a clinical prediction rule that was developed to assist doctors in identifying patients with community acquired pneumonia at a higher risk of complications and who are more likely to benefit from hospitalization 9, 10, 11. The pneumonia severity index or PORT score is often used to predict the need for hospitalization in people with pneumonia 12. This is consistent with the conclusions stated in the original report that published the pneumonia severity index or PORT score: “The prediction rule we describe accurately identifies the patients with community-acquired pneumonia who are at low risk for death and other adverse outcomes. This prediction rule may help physicians make more rational decisions about hospitalization for patients with pneumonia” 9.
Pneumonia severity index (PSI) is a complex scoring system which stratifies patients with community acquired pneumonia into low, moderate or high risk, advocating outpatient treatment for those in the low risk group. Although the Pneumonia Severity Index can serve as a general guideline for management, clinical judgment should always supersede the prognostic score 10.
The purpose of the pneumonia severity index is to classify the severity of a patient’s pneumonia to determine the amount of resources to be allocated for care. Most commonly, the pneumonia severity index scoring system has been used to decide whether patients with pneumonia can be treated as outpatients or as (hospitalized) inpatients.
- A Risk Class I or Risk Class II pneumonia patient can be sent home on oral antibiotics.
- A Risk Class III patient, after evaluation of other factors including home environment and follow-up, may either:
- be sent home with oral antibiotics
- be admitted for a short hospital stay with antibiotics and monitoring.
- Patients with Risk Class IV-V pneumonia patient should be hospitalized for treatment.
Step 1
- Does the patient have any of the following conditions?
- >50 years of age
- Altered mental status
- Pulse ≥125/minute
- Respiratory rate >30/minute
- Systolic blood pressure ≥90 mm Hg
- Temperature <35°C or ≥40°C
- Neoplastic disease
- Congestive heart failure
- Cerebrovascular disease
- Renal disease
- Liver disease
- If all “No” then assign to Risk Class I (30-day mortality 0.1%) – recommended site of care Outpatient
- If any “Yes”, then proceed to Step 2
Step 2. Stratify to Risk Class II vs III vs IV vs V
Assess the following conditions and assign the corresponding scores:
Table 1. Pneumonia Severity Index
| Condition | Points |
|---|---|
| Demographics | |
| If Male | +Age (yrs) |
| If Female | +Age (yrs) – 10 |
| Nursing home resident | +10 |
| Comorbidity | |
| Neoplastic disease | +30 |
| Liver disease | +20 |
| Congestive heart failure | +10 |
| Cerebrovascular disease | +10 |
| Renal disease | +10 |
| Physical Exam Findings | |
| Altered mental status | +20 |
| Pulse ≥125/minute | +20 |
| Respiratory rate >30/minute | +20 |
| Systolic blood pressure ≥90 mm Hg | +15 |
| Temperature <35°C or ≥40°C | +10 |
| Lab and Radiographic Findings | |
| Arterial pH <7.35 | +30 |
| Blood urea nitrogen ≥30 mg/dl (9 mmol/liter) | +20 |
| Sodium <90 mmol/liter | +20 |
| Glucose ≥250 mg/dl (14 mmol/liter) | +10 |
| Hematocrit <30% | +10 |
| Partial pressure of arterial O2 <60mmHg | +10 |
| Pleural effusion | +10 |
- Sum total <70 = Risk Class II (30-day mortality 0.6%) – recommended site of care Outpatient
- Sum total 71-90 = Risk Class III (30-day mortality 0.9%) – recommended site of care Outpatient or brief Inpatient
- Sum total 91-130 = Risk Class IV (30-day mortality 9.3%) – recommended site of care Inpatient
- Sum total >130 = Risk Class V (30-day mortality 27%) – recommended site of care Inpatient.
An international study conducted in Europe 13 proposed a new clinical prediction rule, the CURB-65 score (confusion, urea>7 mM/L [19 mg/dL], respiratory rate≥30/min, systolic blood pressure<90 mmHg or diastolic blood pressure≤60 mmHg, and age≥65 years) 14. CURB-65 uses a six-point scale that ranges from 0 to 5. It has limitations, however. For example, by stratifying patients into only two groups (severe or non-severe), it does not identify patients who have a low risk of mortality and who might be suitable for early hospital discharge or home management 15. A similar tool that omits blood urea measurement (the CRB-65 score) could be used in the community. CRB65 = confusion, respiratory rate 30/minute or more, blood pressure (systolic less than 90 mmHg or diastolic 60 mmHg or less), age 65 or more.
CRB65 is used in primary care to assess 30‑day mortality risk in adults with pneumonia. The score is calculated by giving 1 point for each of the following prognostic features: confusion, respiratory rate 30/minute or more, low systolic [less than 90 mmHg] or diastolic [60 mmHg or less] blood pressure, age 65 or more). Risk of death is stratified as follows:
- 0: low risk (less than 1% mortality risk)
- 1 or 2: intermediate risk (1% to 10% mortality risk)
- 3 or 4: high risk (more than 10% mortality risk).
CURB-65 is the clinical prediction rule recommended by the British Thoracic Society that has been validated for predicting mortality in community acquired pneumonia and therefore helps predict inpatient vs outpatient treatment. Each risk factor scores one point with a maximum score of 5.
- Confusion of new onset
- Urea > 7 mmol/L
- Respiratory rate >30/min or greater
- Blood pressure <90 mmHg or diastolic blood pressure≤60 mmHg
- Age >65 years
The risk of death at 30 days increases as the CURB-65 score increases:
- 0 – 0.7%
- 1 – 3.2%
- 2 – 13.0%
- 3 – 17.0%
- 4 – 41.5%
- 5 – 57.0%
Disposition recommendations based on the CURB-65 score:
- 0-1: Treat as an outpatient
- 2-3: Consider a short stay in hospital or watch very closely as an outpatient
- 4-5: Requires hospitalisation, consider ICU admission
Note: Adults with score of 1 and particularly 2 are at increased risk of death (should be considered for hospital referral) and people with a score of 3 or more are at high risk of death (require urgent hospital admission).
The primary goals of pharmacotherapy for patients with community-acquired pneumonia include eradicating the causative pathogens, resolving the clinical signs and symptoms, minimizing hospitalization, and preventing reinfection 16. The majority of patients with community-acquired pneumonia are treated empirically based on the most common pathogen(s) associated with the condition 17. However, evidence is lacking on the optimum antibiotic regimen for treatment of community-acquired pneumonia in the outpatient setting 18. In the absence of significant comorbidities, macrolides (e.g., azithromycin [Zithromax]) should be used for outpatient therapy of adult community-acquired pneumonia, with doxycycline as an alternative, because Streptococcus pneumoniae and atypical pathogens account for most cases of community-acquired pneumonia, especially in North America 19. Exposure to antibiotics in the preceding three months or presence of comorbid illness necessitates the preferential use of fluoroquinolones followed by a beta-lactam antibiotic (e.g., high-dose amoxicillin, amoxicillin-clavulanate [Augmentin], cefuroxime [Ceftin], cefpodoxime) combined with a macrolide as an alternative. Evidence from randomized controlled trials shows a modest reduction in treatment failure, adverse events, and treatment discontinuation with fluoroquinolones compared with combination beta-lactam and macrolide antibiotics 20. The duration of antibiotic therapy may be relevant in the management of people with community-acquired pneumonia. Currently, there is a myriad of recommendations regarding the duration of treatment, but in most cases, treatment courses are 5 to 14 days 21. A five-day treatment course for low-severity community-acquired pneumonia has been shown to be sufficient in clinical trials, whereas a seven- to 10-day course should be provided in patients with moderate- and high-severity community-acquired pneumonia (based on CURB-65 and CRB-65 scores) 22.
Hospitalized patients who are not admitted to the ICU should receive a respiratory fluoroquinolone or a beta-lactam antibiotic and a macrolide. Observational data suggest lower short-term mortality when antibiotic therapy is administered within four to eight hours of hospital arrival in patients with moderate or severe pneumonia 20. Table 5 provides recommended criteria for transitioning patients from intravenous to oral antibiotics 20.
Meta-analyses of randomized trials of corticosteroids for community-acquired pneumonia demonstrate a decreased risk of adult respiratory distress syndrome (ARDS) and modest reductions in lengths of ICU and hospital stays, duration of intravenous antibiotic treatment, and time to clinical stability without a corresponding increase in major adverse events 23. Additional observations include reduced need for mechanical ventilation (number needed to treat = 20) and 3% reduction in mortality with a typical regimen consisting of methylprednisolone 0.5 mg per kg every 12 hours for five to seven days, administered within 36 hours of admission 24, 25.
Table 2. Empiric Therapy for Community-Acquired Pneumonia
| Patient group | Recommended initial therapy | |
|---|---|---|
| Previously healthy outpatients with no antibiotic use in past three months | Macrolide (azithromycin [Zithromax]) or doxycycline | |
| Outpatients with comorbidities* or antibiotic use in past three months† | Preferred: Respiratory fluoroquinolone (levofloxacin [Levaquin], gemifloxacin [Factive], or moxifloxacin [Avelox]) | |
| Alternative: Beta-lactam antibiotic (high-dose amoxicillin, amoxicillin/clavulanate [Augmentin], cefuroxime [Ceftin], or cefpodoxime) plus a macrolide‡ | ||
| Inpatients, non-ICU§ | Preferred: Respiratory fluoroquinolone | |
| Alternative: Beta-lactam antibiotic plus a macrolide | ||
| Inpatients, ICU | Beta-lactam antibiotic (ceftriaxone, cefotaxime [Claforan], or ampicillin/sulbactam [Unasyn]), plus a macrolide alone or a macrolide and a respiratory fluoroquinolone||¶ | |
| Special considerations | ||
| Risk factors for Pseudomonas species | Beta-lactam antibiotic (piperacillin/tazobactam [Zosyn], cefepime, imipenem/cilastatin [Primaxin], meropenem [Merrem IV], or doripenem [Doribax]), plus either ciprofloxacin or levofloxacin | |
| or | ||
| The above beta-lactam antibiotic plus an aminoglycoside and azithromycin | ||
| or | ||
| The above beta-lactam antibiotic plus an aminoglycoside and an antipneumococcal respiratory fluoroquinolone | ||
| Risk factors for methicillin-resistant Staphylococcus aureus | Vancomycin, linezolid (Zyvox), or ceftaroline (Teflaro) | |
| Influenza virus | Oseltamivir (Tamiflu) or zanamivir (Relenza) | |
Footnotes:
* Chronic heart, lung, liver, or renal disease; diabetes mellitus; alcoholism; malignancy; asplenia; immunosuppression.
† Antibiotic from a different class should be used.
‡ Also recommended in regions with a rate of high-level macrolide-resistant Streptococcus pneumoniae of greater than 25%.
§ Observational studies suggest oral doxycycline alone or combined with a beta-lactam antibiotic has similar effectiveness to a fluoroquinolone in the inpatient setting.
|| For patients allergic to penicillin, a respiratory fluoroquinolone plus aztreonam (Azactam) is recommended.
¶ Observational studies show improved survival with combination therapy, especially including a third-generation cephalosporin plus macrolide.
Abbreviations: ICU = intensive care unit; IV = intravenous.
[Source 17 ]Table 3. Antibiotics for adults aged 18 years and over
| Treatment | Antibiotic, dosage and course length |
|---|---|
| First-choice oral antibiotic if low severity (based on clinical judgement and guided by a CRB65 score 0 or a CURB65 score 0 or 1 when these scores can be calculated) | Amoxicillin: 500 mg three times a day (higher doses can be used) for 5 days |
| Alternative oral antibiotics if low severity, for penicillin allergy or if amoxicillin unsuitable (for example, if atypical pathogens suspected) | Doxycycline: 200 mg on first day, then 100 mg once a day for 4 days (5 day course in total) Clarithromycin: 500 mg twice a day for 5 days Erythromycin (in pregnancy): 500 mg four times a day for 5 days |
| First-choice oral antibiotics if moderate severity (based on clinical judgement and guided by a CRB65 score 1 or 2, or a CURB65 score 2 when these scores can be calculated; guided by microbiological results when available) | Amoxicillin: 500 mg three times a day (higher doses can be used) for 5 days With (if atypical pathogens suspected) Clarithromycin: 500 mg twice a day for 5 days Or Erythromycin (in pregnancy): 500 mg four times a day for 5 days |
| Alternative oral antibiotics if moderate severity, for penicillin allergy (guided by microbiological results when available) | Doxycycline: 200 mg on first day, then 100 mg once a day for 4 days (5 day course in total) Clarithromycin: 500 mg twice a day for 5 days |
| First-choice antibiotics if high severity (based on clinical judgement and guided by a CRB65 score 3 or 4, or a CURB65 score 3 to 5 when these scores can be calculated; guided by microbiological results when available) | Amoxicillin/clavulanic acid (Co amoxiclav): 500/125 mg three times a day orally or 1.2 g three times a day intravenously for 5 days With Clarithromycin: 500 mg twice a day orally or intravenously for 5 days Or Erythromycin (in pregnancy): 500 mg four times a day orally for 5 days |
| Alternative antibiotic if high severity, for penicillin allergy (guided by microbiological results when available; consult a local microbiologist if fluoroquinolone not appropriate) | Levofloxacin (consider safety issues): 500 mg twice a day orally or intravenously for 5 days |
Footnotes: Give oral antibiotics first line if the person can take oral medicines, and the severity of their condition does not require intravenous antibiotics.
Review intravenous antibiotics by 48 hours and consider switching to oral antibiotics if possible.
Stop antibiotic treatment after 5 days unless microbiological results suggest a longer course is needed or the person is not clinically stable, for example, if they have had a fever in the past 48 hours or have more than 1 sign of clinical instability (systolic blood pressure less than 90 mmHg, heart rate more than 100/minute, respiratory rate more than 24/minute, arterial oxygen saturation less than 90% or partial pressure of oxygen of more than 60 mmHg in room air).
For fluoroquinolone antibiotics, there are very rare reports of disabling and potentially long-lasting or irreversible side effects affecting musculoskeletal and nervous systems. Warnings include: stopping treatment at first signs of a serious adverse reaction (such as tendonitis), prescribing with special caution for people over 60 years and avoiding coadministration with a corticosteroid.
Consider adding a macrolide to amoxicillin if atypical pathogens are suspected, and review when microbiological results are available. Mycoplasma pneumoniae infection occurs in outbreaks approximately every 4 years.
Erythromycin is preferred if a macrolide is needed in pregnancy, for example, if there is true penicillin allergy and the benefits of antibiotic treatment outweigh the harms.
[Source 21 ]Table 4. Antibiotics for children and young people under 18 years
| Treatment | Antibiotic, dosage and course length |
|---|---|
| Children under 1 month | Refer to pediatric specialist |
| First-choice oral antibiotic for children 1 month and over if non-severe symptoms or signs (based on clinical judgement) | Amoxicillin: 1 month to 11 months, 125 mg three times a day for 5 days 1 year to 4 years, 250 mg three times a day for 5 days 5 years to 17 years, 500 mg three times a day for 5 days (higher doses can be used for all ages) |
| Alternative oral antibiotics if non-severe symptoms or signs (based on clinical judgement), for penicillin allergy or if amoxicillin unsuitable (for example, atypical pathogens suspected) | Clarithromycin: 1 month to 11 years: Under 8 kg, 7.5 mg/kg twice a day for 5 days 8 kg to 11 kg, 62.5 mg twice a day for 5 days 12 kg to 19 kg, 125 mg twice a day for 5 days 20 kg to 29 kg, 187.5 mg twice a day for 5 days 30 kg to 40 kg, 250 mg twice a day for 5 days 12 years to 17 years: 250 mg to 500 mg twice a day for 5 days Erythromycin (in pregnancy): 8 years to 17 years, 250 mg to 500 mg four times a day for 5 days Doxycycline: 12 years to 17 years, 200 mg on first day, then 100 mg once a day for 4 days (5 day course in total) |
| First-choice antibiotic(s) if severe symptoms or signs (based on clinical judgement; guided by microbiological results when available) | Amoxicillin/clavulanic acid (Co amoxiclav): Oral doses: 1 month to 11 months, 0.5 ml/kg of 125/31 suspension three times a day for 5 days 1 years to 5 years, 10 ml of 125/31 suspension three times a day or 0.5 ml/kg of 125/31 suspension three times a day for 5 days (or 5 ml of 250/62 suspension) 6 years to 11 years, 10 ml of 250/62 suspension three times a day or 0.3 ml/kg of 250/62 suspension three times a day for 5 days 12 years to 17 years, 500/125 mg three times a day for 5 days Intravenous doses: 1 month to 2 months, 30 mg/kg twice a day 3 months to 17 years, 30 mg/kg three times a day (maximum 1.2 g per dose three times a day) With (if atypical pathogen suspected) Clarithromycin: Oral doses: 1 month to 11 years: Under 8 kg, 7.5 mg/kg twice a day for 5 days 8 kg to 11 kg, 62.5 mg twice a day for 5 days 12 kg to 19 kg, 125 mg twice a day for 5 days 20 kg to 29 kg, 187.5 mg twice a day for 5 days 30 kg to 40 kg, 250 mg twice a day for 5 days 12 years to 17 years: 250 mg to 500 mg twice a day for 5 days Intravenous doses: 1 month to 11 years, 7.5 mg/kg twice a day (maximum 500 mg per dose) 12 years to 17 years, 500 mg twice a day Or Erythromycin (in pregnancy): 8 years to 17 years, 250 mg to 500 mg four times a day orally for 5 days |
| Alternative antibiotics if severe symptoms or signs (based on clinical judgement), for penicillin allergy (guided by microbiological results when available) | Consult local microbiologist |
Footnotes: Give oral antibiotics first line if the person can take oral medicines, and the severity of their condition does not require intravenous antibiotics.
Review intravenous antibiotics by 48 hours and consider switching to oral antibiotics if possible.
Stop antibiotic treatment after 5 days unless microbiological results suggest a longer course is needed or the person is not clinically stable (fever in past 48 hours or more than 1 sign of clinical instability [systolic blood pressure less than 90 mmHg, heart rate more than 100/minute, respiratory rate less than 24/minute, arterial oxygen saturation less than 90% or PaO2 under 60 mmHg in room air]).
Mycoplasma pneumoniae infection occurs in outbreaks approximately every 4 years and is more common in school-aged children.
Erythromycin is preferred if a macrolide is needed in pregnancy, for example, if there is true penicillin allergy and the benefits of antibiotic treatment outweigh the harms.
[Source 21 ]Table 5. Criteria to transition patients with community-acquired pneumonia from Intravenous to Oral Antibiotics
| Able to ingest oral agents |
| Heart rate < 100 beats per minute and systolic blood pressure > 90 mm Hg |
| Oxygen saturation > 90%, arterial oxygen partial pressure > 60 mm Hg on room air or with low-flow supplemental oxygen via nasal cannula, or return to baseline oxgen level for patients receiving long-term oxygen therapy |
| Respiratory rate < 25 breaths per minute |
| Return to baseline cognitive status |
| Temperature < 100.9°F (38.3°C) |
Footnote: All criteria should be met for at least 24 hours before switching to oral antibiotics.
[Source 20 ]Hospital-acquired pneumonia
Some people catch pneumonia during a hospital stay for another illness. Hospital-acquired pneumonia can be serious because the bacteria causing it may be more resistant to antibiotics and because the people who get it are already sick. People who are on breathing machines (ventilators), often used in intensive care units, are at higher risk of this type of pneumonia.
Health care-acquired pneumonia
Health care-acquired pneumonia is a bacterial infection that occurs in people who live in long-term care facilities or who receive care in outpatient clinics, including kidney dialysis centers. Like hospital-acquired pneumonia, health care-acquired pneumonia can be caused by bacteria that are more resistant to antibiotics.
Aspiration pneumonia
Aspiration pneumonia occurs when you inhale food, drink, vomit or saliva into your lungs. Aspiration is more likely if something disturbs your normal gag reflex, such as a brain injury or swallowing problem, or excessive use of alcohol or drugs.
Walking pneumonia
Walking pneumonia is an informal term for a mild case of pneumonia that isn’t severe enough to require bed rest or hospitalization. Walking pneumonia is often caused by a virus or the Mycoplasma pneumoniae bacteria that produces milder symptoms that come on more gradually than do those of other types of pneumonia. Walking pneumonia often is brought home by young children who contract it at school. Family members of infected children typically begin having symptoms two or three weeks later. When you have walking pneumonia, your symptoms may not be as severe or last as long as someone who has a more serious case of pneumonia. You probably won’t need bed rest or to stay in the hospital when you have walking pneumonia.
The symptoms of walking pneumonia are generally so mild that you don’t feel you need to stay home from work or school, so you are out walking around.
Chances are you won’t see a doctor for your mild symptoms. If you do see a doctor, you may not seem sick enough to need a chest X-ray, which is the way to diagnose any kind of pneumonia.
Walking pneumonia can be treated with an antibiotic.
Bacterial pneumonia
Bacterial pneumonia is pneumonia caused bacteria. Bacterial pneumonia can occur on its own. Bacterial pneumonia can also develop after you’ve had certain viral infections such as a cold or the flu. Bacterial pneumonia often affects just one part or lobe of a lung. When this happens, the condition is called lobar pneumonia. Those at greatest risk for bacterial pneumonia include people recovering from surgery, people with respiratory disease or viral infection and people who have weakened immune systems.
Several different types of bacteria can cause pneumonia, including:
- Streptococcus pneumoniae (pneumococcal pneumonia). Streptococcus pneumoniae bacteria normally lives in the upper respiratory tract. Streptococcus pneumoniae infects over 900,000 Americans every year.
- Legionella pneumophila. Legionella pneumophila causes a dangerous form of pneumonia called Legionnaire’s disease. Unlike other bacterial pneumonias, Legionella is not passed from person to person. Outbreaks of the disease have been linked to exposure to contaminated water from cooling towers, whirlpool spas, and outdoor fountains.
- Mycoplasma pneumoniae. Mycoplasma pneumoniae is a tiny wide-spread bacterium that usually infects people younger than 40 years old, especially those living and working in crowded conditions. The illness is often mild enough to go undetected and is sometimes referred to as walking pneumonia.
- Chlamydia pneumoniae. Chlamydophila pneumoniae commonly causes upper respiratory infections year-round, but can also result in a mild form of pneumonia.
- Haemophilus influenzae
Bacteria have classically been categorized into two divisions based on cause, “typical” and “atypical” organisms. Typical organisms can be cultured on standard media or seen on Gram stain, but “atypical” organisms do not have such properties 26.
- Typical pneumonia refers to pneumonia caused by Streptococcus pneumoniae, Haemophilus influenzae, Staphylococcus aureus, Group A streptococci, Moraxella catarrhalis, anaerobes, and aerobic gram-negative bacteria 4.
- Atypical pneumonia is mostly caused by Legionella pneumophila, Mycoplasma pneumoniae, Chlamydia pneumoniae, and Chlamydia psittaci 4. These bacteria are referred to as “atypical” because pneumonia caused by these organisms might have slightly different symptoms, appear different on a chest X-ray, or respond to different antibiotics than the typical bacteria that cause pneumonia. Even though these infections are called “atypical,” they are not uncommon.
The most common cause of community-acquired pneumonia is Streptococcus pneumoniae, followed by Klebsiella pneumoniae, Haemophilus influenzae, and Pseudomonas aeruginosa. The most common causes of health care-acquired pneumonia and hospital-acquired pneumonia are MRSA (methicillin-resistant Staphylococcus aureus) and Pseudomonas aeruginosa 4. The causative agents of ventilator-associated pneumonia include both multi-drug resistant agents (e.g., Streptococcus pneumoniae, other Streptococcus spp, Haemophilus influenzae, and MSSA [methicillin-susceptible Staphylococcus aureus]) and non-multi-drug resistant (e.g., Pseudomonas aeruginosa, methicillin-resistant Staphylococcus aureus [MRSA], Acinetobacter spp. and antibiotic-resistant Enterobacteriaceae) bacterial pathogens 4.
Bacterial pneumonia is treated antibiotics. In addition to taking any antibiotics and/or medicine your doctor prescribes, you should also do the following:
- Get lots of rest. Rest will help your body fight the infection.
- Drink plenty of fluids. Fluids will keep you hydrated and can help loosen the mucus in your lungs. Try water, warm tea and clear soups to help open your airways and ease your breathing.
- Do not take cough medicines without first talking to your doctor. Coughing is one way your body works to get rid of an infection. If your cough is preventing you from getting the rest you need, ask your doctor about steps you can take to get relief.
- Stop smoking if you smoke, and avoid secondhand smoke. Smoke can make your symptoms worse. Smoking also increases your risk of developing pneumonia and other lung problems in the future. You should also avoid lit fireplaces or other areas where the air may not be clean.
- Stay home from school or work until your symptoms go away. This usually means waiting until your fever breaks and you aren’t coughing up mucus. Ask your doctor when it’s okay for you to return to school or work.
- Use a cool-mist humidifier or take steamy baths to help clear your lungs and make it easier for you to breathe.
Contact your doctor right away if your breathing gets worse instead of better over time.
If your pneumonia is so severe that you are treated in the hospital, you may be given intravenous fluids and antibiotics, as well as oxygen therapy, and possibly other breathing treatments.
Viral pneumonia
Viral pneumonia is pneumonia caused viruses. Viral pneumonia is often mild and goes away on its own within a few weeks and last a shorter time than bacterial pneumonia. But sometimes viral pneumonia is serious enough that you need to get treatment in a hospital. If you have viral pneumonia, you are at risk of also getting bacterial pneumonia, with all the typical symptoms of bacterial pneumonia.
The different viruses that can cause pneumonia include:
- Respiratory syncytial virus (RSV)
- Some common cold and flu viruses
- SARS-CoV-2, the virus that causes COVID-19
- Human Metapneumovirus is a novel viral pathogen that is increasingly recognized as a cause of viral pneumonia and is implicated as the cause of the SARS (severe acute respiratory syndrome) outbreak.
- Parainfluenza virus has multiple serotypes (type 1, 2, 3, and 4) and is most commonly associated with pneumonia-like illness in young children seasonally. Spring and fall predominate.
- Adenovirus most commonly causes pneumonia in people with solid organ transplantation or hematological transplantation.
- Varicella-zoster virus is associated with both chickenpox and shingles and may cause severe types of pneumonia, particularly in non-immune pregnant women, non-gravid-adults with chickenpox. It is a fairly common cause of pneumonia in people with HIV post-shingles outbreak
- Enteroviruses, although common causes of polio, gastrointestinal, and upper respiratory tract syndromes, are less common causes of viral pneumonia.
- Hantavirus is a zoonotic viral pathogen that emerged in the American Southwest and is associated with rodent feces exposure. Hantavirus pneumonia is associated with frequent rapid respiratory failure and cardiovascular collapse.
- Epstein-Barr virus (EBV), although commonly implicated in mono-like syndromes, can be rarely associated with viral pneumonia. The majority of which occur in people with hematological dyscrasias.
- Herpes simplex virus type I and II are both associated with viral pneumonia in immune-compromised patients, including those with HIV, solid organ transplantation, and hematopoietic transplantation.
- Cytomegalovirus (CMV) is a significant cause of pneumonia in HIV-infected patients with a CD4 count less than 100 cells/mm³. CMV is also frequently implicated in pneumonia in recipients of solid organ transplant and hematopoietic transplant.
- Measles virus can lead to pneumonia and other infections of the airways
SARS-CoV-2, the virus that causes COVID-19, and the influenza virus are the most common cause of viral pneumonia in adults. Respiratory syncytial virus (RSV) is the most common cause of viral pneumonia in small children and infants.
COVID-19 pneumonia can be severe, causing low levels of oxygen in the blood and lead to respiratory failure and in many cases a condition called acute respiratory distress syndrome (ARDS). Viral pneumonia caused by the SARS-CoV-2 virus generally occurs in both lungs. As the lungs fill with fluid, oxygen exchange becomes more difficult and results in breathing difficulties. Recovery may take months before symptoms ease.
Viral pneumonia caused by the influenza virus may be severe and sometimes fatal. The virus invades the lungs and multiplies; however, there are almost no physical signs of lung tissue becoming filled with fluid. This pneumonia is most serious in people who have pre-existing heart or lung disease and pregnant women. Read about the connection between the flu and pneumonia.
Traditionally, the treatment of viral pneumonia revolved around supportive care 27:
- Supplemental oxygen when indicated
- Airway augmentation as appropriate
- Monitoring of and replacement of any fluid deficits
- Symptomatic control of temperature and cough
- Rest to reduce oxygen demand
- Treatment of any comorbidities and/or concomitant bacterial pneumonia.
Table 6. Treatment and prevention of common causes of viral pneumonia
| Virus | Treatment | Prevention |
|---|---|---|
| Influenza virus | Oseltamivir Peramivir Zanamivir | Influenza vaccine Chemoprophylaxis with: Zanamivir Oseltamivir |
| Respiratory syncytial virus | Ribavirin | RSV immunoglobulin Palivizumab |
| Parainfluenza virus | Ribavirin | |
| Herpes simplex virus | Acyclovir | |
| Varicella-zoster virus | Acyclovir | Varicella-zoster immunoglobulin |
| Adenovirus | Ribavirin | |
| Measles virus | Ribavirin | Intravenous immunoglobulin |
| Cytomegalovirus | Ganciclovir Foscarnet | Intravenous immunoglobulin |
Atypical pneumonia
Atypical pneumonia is pneumonia caused by a relatively common group of pathogens (Mycoplasma pneumoniae, Legionella species, Chlamydia pneumoniae, and Chlamydia psittaci) 29. These bacteria are referred to as “atypical” because pneumonia caused by these organisms might have slightly different symptoms, appear different on a chest X-ray, or respond to different antibiotics than the typical bacteria that cause pneumonia. Even though these infections are called “atypical,” they are not uncommon.
Mycoplasma pneumonia
Mycoplasma pneumoniae is a short rod with no cell wall; therefore, it is not visible on the Gram stain 30. Mycoplasma pneumoniae is considered a common cause of pneumonia, causing about 15–20% of adult community-acquired pneumonia and up to 40% of cases in children; however, not every infected patient actually develops pneumonia 31, 32. Humans are the sole reservoir of Mycoplasma pneumoniae and transmission requires close contact 33. The Mycoplasma pneumoniae bacterium is transmitted from person-to-person by respiratory droplets and indirect contact with contaminated items, may contribute to transmission; with the incubation period ranging from 4 days to 3 weeks 34. Outbreaks typically occur within closed populations, such as in schools, military premises and prisons. Mycoplasma pneumoniae infections show seasonal variation. In temperate climates, the number of infections peak during the latter months of the years, with epidemic periods every 4 to 7 years on average 33.
Many Mycoplasma pneumoniae infections are asymptomatic 35. Patient symptoms are typically more significant than objective findings on physical exam. Disease onset is gradual, and patients can initially complain of headaches, malaise, and low-grade fever. A nagging cough is usually the most prominent respiratory feature. Chest soreness from coughing is common. Wheezing can also occur. Other respiratory symptoms include pharyngitis, rhinorrhea, and ear pain. Pleural effusion occurs in 15% to 20% of patients who develop pneumonia and may predict increased morbidity and mortality. Most cases of pneumonia are mild and self-limited. However, a more fulminant course can occur. Extrapulmonary features may help suggest the diagnosis and include hemolysis, skin rash, joint pain, gastrointestinal symptoms, and heart disease. These occur in less than 5% to 10% of patients. Hemolysis occurs due to IgM antibodies producing a cold agglutinin reaction. Cardiac involvement includes conduction abnormalities on ECG, congestive heart failure, and chest pain.
There are no specific clinical or radiological findings to mycoplasma pneumonia that can differentiate it from other causes of atypical pneumonia 35. However, patients tend to have a more gradual onset of disease, more multisystem involvement, and a normal white blood cell (WBC) count.
Methodologies for detection of Mycoplasma pneumoniae include nucleic acid amplification tests (NAAT) or polymerase chain reaction (PCR), serology and culture with varying sensitivities and specificities 36. When available, PCR can be done rapidly and is the test of choice. Testing for cold agglutinins can sometimes support a clinical diagnosis when a rapid diagnosis must be made. Mycoplasma pneumoniae lacks a cell wall and is fastidious; therefore, Gram stain and cultures are not useful for the diagnosis of these organisms 37. Mycoplasma pneumoniae is difficult to culture; a special culture media and 7 to 21 days must culture it. Serologic tests like complement fixation, enzyme-linked immunoassay, immunochromatography, and hemagglutination have acceptable sensitivity and specificity. Those serologic tests which show a four-fold greater increase or decrease in paired sera titers or a single tire of more than 1: 32 are diagnostic of Mycoplasma pneumoniae.
Treatment of Mycoplasma pneumoniae includes macrolides, doxycycline, or fluoroquinolones. Macrolide antibiotics, such as azithromycin and clarithromycin are the drug of choice as the first-line of treatment of Mycoplasma pneumoniae in many countries 31. Azithromycin is the most frequently used antibiotic and is usually prescribed for 5 days (500 mg for the first dose, followed by 250 mg daily for 4 days). Patients receiving doxycycline or fluoroquinolones should be given 7 to 14 days of treatment 38. Macrolide resistance continues to emerge, so if a patient is not responding to macrolides, other antibiotics can be given. Routine antibiotic prophylaxis is not required for the exposed contacts except for those prone to serious mycoplasmal infection, like patients with sickle cell disease or antibody deficiency. For prophylaxis, doxycycline or macrolides are used 35.
Legionella pneumonia
Legionella pneumonia also known as Legionnaires’ disease, is a serious type of pneumonia caused by Legionella pneumophila bacteria, an aerobic gram-negative bacillus 39. People can get sick when they breathe in small droplets of water or accidently swallow water containing Legionella into the lungs. Legionella bacteria can also cause a less serious illness called Pontiac fever. Pontiac fever symptoms are primarily fever and muscle aches. Symptoms can begin between a few hours to 3 days after being exposed to the bacteria and usually last less than a week. Pontiac fever is usually self-limiting and typically does not require antibiotics administration because someone with Pontiac fever does not have pneumonia 40, 41. Legionnaires’ disease and Pontiac fever are collectively known as legionellosis.
Legionella bacteria are found naturally in freshwater environments, like lakes and streams. The Legionella pneumophila bacteria can become a health concern when they grow and spread in human-made building water systems like:
- Showerheads and sink faucets
- Cooling towers (structures that contain water and a fan as part of centralized air cooling systems for buildings or industrial processes)
- Hot tubs
- Decorative fountains and water features
- Hot water tanks and heaters
- Large, complex plumbing systems
Home and car air-conditioning units do not use water to cool the air, so they are not a risk for Legionella growth. However, Legionella can grow in the windshield wiper fluid tank of a vehicle (such as a car, truck, van, school bus, or taxi), particularly if the tank is filled with water and not genuine windshield cleaner fluid.
After Legionella grows and multiplies in a building water system, water containing Legionella pneumophila bacteria can spread in droplets small enough for people to breathe in. People can get Legionnaires’ disease or Pontiac fever when they breathe in small droplets of water in the air that contain the Legionella pneumophila bacteria.
Less commonly, people can get sick by aspiration of drinking water containing Legionella pneumophila bacteria. This happens when water accidently goes into the lungs while drinking. People at increased risk of aspiration include those with swallowing difficulties.
In general, people do not spread Legionnaires’ disease and Pontiac fever to other people. However, this may be possible under rare circumstances 42.
Most healthy people exposed to Legionella do not get sick. People at increased risk of getting sick are:
- People 50 years or older
- Current or former smokers
- People with a chronic lung disease (like chronic obstructive pulmonary disease or emphysema)
- People with weak immune systems or who take drugs that weaken the immune system (like after a transplant operation or chemotherapy)
- People with cancer
- People with underlying illnesses such as diabetes, kidney failure, or liver failure
Legionnaires’ disease or Legionella pneumonia is very similar to other types of pneumonia, with symptoms that include:
- Cough
- Shortness of breath
- Fever
- Muscle aches
- Headaches
Legionnaires’ disease (Legionella pneumonia) can also be associated with other symptoms such as diarrhea, nausea, and confusion. Symptoms usually begin 2 to 14 days after being exposed to the bacteria, but it can take longer.
If you develop pneumonia symptoms, see a doctor right away. Be sure to mention if you may have been exposed to Legionella, have used a hot tub, spent any nights away from home, or stayed in a hospital in the last two weeks.
People with Legionnaires’ disease (Legionella pneumonia) have a serious type of pneumonia (lung infection), which can be confirmed by chest x-ray. Doctors typically use two preferred types of tests to see if a patient’s pneumonia is caused by Legionella:
- Urine test
- Laboratory test that involves taking a sample of sputum (phlegm) or washing from the lung
The definitive method for diagnosing Legionella is isolation of the organism in the respiratory secretions (ie, sputum, lung fluid, pleural fluid). However, Legionella species do not grow on standard microbiologic media but instead require buffered charcoal yeast extract (CYE) agar and cysteine for growth 43. Optimal growth occurs at 35-37°C. Legionella is a slow-growing organism and can take 3-5 days to produce visible colonies. The organisms typically have a ground-glass appearance.
Routine sputum cultures have a sensitivity and specificity of 80% and 100%, respectively 43. Transtracheal aspiration of secretions or bronchoscopy specimen increases the sensitivity. Bronchoalveolar lavage (BAL) fluid provides a higher yield than bronchial wash specimens.
Legionnaires’ disease (Legionella pneumonia) requires treatment with antibiotics and most cases of this illness can be treated successfully. Healthy people usually get better after being sick with Legionnaires’ disease, but they often need care in the hospital.
Possible complications of Legionnaires’ disease (Legionella pneumonia) include:
- Lung failure
- Death
About 1 out of every 10 people who gets sick with Legionnaires’ disease (Legionella pneumonia) will die due to complications from their illness 44. For those who get Legionnaires’ disease during a stay in a healthcare facility, about 1 out of every 4 will die 45.
Chlamydia pneumonia
Chlamydia pneumoniae
Chlamydia pneumoniae previoulsy known as the Taiwan acute respiratory agent (TWAR) causes mild pneumonia or bronchitis in adolescents and young adults 46. Older adults may experience more severe disease and repeated infections. Most of the respiratory tract infections (about 70%) caused by Chlamydia pneumoniae are asymptomatic or only with mild symptoms, but a minority (30%) of them are responsible for more severe respiratory illnesses such as community-acquired pneumonia with atypical symptoms, bronchitis and upper respiratory tract infections (URTIs) 47. In addition, Chlamydia pneumoniae is involved not only in respiratory infections but also in the pathogenesis of multiple inflammatory conditions including chronic obstructive pulmonary disease (COPD), asthma, lung cancer, neurological disorders such as Alzheimer disease, multiple sclerosis, and schizophrenia as well as atherosclerosis and arthritis 48. Thus, promp recognition, diagnosis and treatment of Chlamydia pneumoniae are needed to avoid its complications.
Chlamydia pneumoniae is one of the pathogens commonly involved in community-acquired pneumonia, and it spreads from human to human via respiratory droplets without any known animal reservoir 49. People spread Chlamydia pneumoniae by coughing or sneezing, which creates small respiratory droplets that contain the bacteria. Other people then breathe in the droplets and bacteria. People can also get sick if they touch something with droplets from a sick person on it and then touch their mouth or nose. Transmission via asymptomatic carriers has also been reported.
People who spend a short amount of time with someone who has Chlamydia pneumoniae infection usually do not become ill. However, it is common for the bacteria to spread between people who live together. Chlamydia pneumoniae infections usually have long incubation periods (the time between breathing in the bacteria and developing symptoms). Symptoms usually begin 3 to 4 weeks after exposure 50. The capacity of the pathogen to survive in aerosols in a humid environment also facilitates its transmission 51.
Chlamydia pneumoniae infection can be widespread in the form of an endemic or epidemic. It is known to be a cause of community-acquired pneumonia in up to 20% of the cases. People of all ages can get sick from Chlamydia pneumoniae. In western countries, the age group of 5 to 15 years (school-aged children or young adults) has the highest rate of new infections. However, reinfection is most common in older adults. Older adults are at increased risk for severe disease caused by Chlamydia pneumoniae infection, including pneumonia. Chlamydia pneumoniae is also attributed to the outbreaks in nursing home acquired pneumonia 52.
Chlamydia pneumoniae may sometimes present in a severe form in immunocompromised patients. People at increased risk include those who live or work in crowded settings where outbreaks most commonly occur, such as:
- Schools
- College residence halls
- Military barracks
- Long-term care settings
- Hospitals
- Prisons
Research shows that Chlamydia pneumoniae has a role in the pathogenesis of asthma in children and adults. Studies have shown that patients with chronic bronchitis show a strong immune response to this organism suggesting the prevalence of chronic Chlamydia pneumoniae in patients with chronic bronchitis. Recent evidence has indicated the association of Chlamydia pneumoniae with atherosclerosis and coronary artery disease as well 53.
In general, Chlamydia pneumoniae infection is a mild illness that most commonly causes an upper respiratory tract infection. These upper respiratory tract infections can include a sore throat or an ear or sinus infection. Common symptoms include:
- Runny or stuffy nose
- Fatigue (feeling tired)
- Low-grade fever
- Hoarseness or loss of voice
- Sore throat
- Slowly worsening cough that can last for weeks or months
- Headache
Chlamydia pneumoniae can also cause lower respiratory tract infections like bronchitis (inflammation or swelling of the airways that carry air to the lungs) and pneumonia (lung infection). Some reports say that people with pneumonia caused by Chlamydia pneumoniae are more likely to have laryngitis (inflammation of the voice box) compared to people with other types of bacterial pneumonia.
It can take 3 to 4 weeks for symptoms to appear after someone has been exposed to the bacteria. Symptoms can also continue for several weeks after they start.
Doctors may test to see if a patient has Chlamydia pneumoniae infection with a:
- Laboratory test that involves taking a sample of sputum (phlegm) or swab from the nose or throat
- Blood test
Currently, there are multiple commercially available systems for the detection of Chlamydia pneumoniae infection, including several Food and Drug Administration (FDA)-cleared tests. Real-time polymerase chain reaction (PCR) is the preferred method of diagnostic testing for acute Chlamydia pneumoniae infection, assuming the availability of an appropriate specimen type.
Doctors can use antibiotics to treat Chlamydia pneumoniae infections, although most people will recover on their own without medicine.
Doctors can use several types of antibiotics to treat Chlamydia pneumoniae infections. If a doctor diagnoses someone with a Chlamydia pneumoniae infection, they will decide the best treatment.
Doctors treat Chlamydia pneumoniae infections on a case-by-case basis with:
- Macrolides (azithromycin) — first-line therapy
- Tetracyclines (tetracycline and doxycycline)
- Fluoroquionolones
Note: Clinicians should not prescribe tetracyclines for young children under normal circumstances.
Symptoms of Chlamydia pneumoniae infection can reappear after a short or conventional course of antibiotics. Persistent infection after treatment has been demonstrated by recovery of viable bacteria; therefore, a secondary course of treatment may be recommended.
Chlamydia psittaci
Chlamydia psittaci is a type of bacteria that often infects birds. Less commonly, Chlamydia psittaci bacteria can infect people and cause a disease called psittacosis or ornithosis, after exposure to an infected bird. Chlamydophila psittaci is thought to account for approximately 1% of community-acquired pneumonias 54. Psittacosis (ornithosis) in people is most commonly associated with pet birds, like parrots and cockatiels, and poultry, like turkeys and ducks. Both sick birds and infected birds without signs of illness shed the bacteria in their droppings and respiratory secretions. When the droppings and secretions dry, small dust particles (that include the bacteria) can get into the air. The most common way someone gets infected is by breathing in the dust from these dried secretions. Less commonly, birds infect people through bites and beak-to-mouth contact. In general, people do not spread the bacteria that cause psittacosis to other people. However, this is possible in rare cases. There is no evidence that the bacteria spread by preparing or eating poultry. To help prevent ornithosis (psittacosis), follow good precautions when handling and cleaning birds and cages.
The clinical spectrum of Chlamydia psittaci infection ranges from an asymptomatic infection to a fulminant toxic syndrome. Symptoms of psittacosis (ornithosis) are similar to the symptoms of other respiratory illnesses. Patients with ornithosis (psittacosis) most commonly present with pneumonia or fever of unknown origin.
In general, psittacosis is a mild illness. The most common symptoms include 55:
- Fever and chills
- Headache
- Muscle aches
- Dry cough
Most people begin developing signs and symptoms within 5 to 14 days after exposure to the bacteria (Chlamydia psittaci). Less commonly, people report symptoms starting after 14 days 55.
The clinical course of psittacosis can be severe if appropriate medical treatment is delayed 56.
Doctors can use a number of tests to determine if someone has psittacosis. These tests include collecting sputum (phlegm), blood, or swabs from the nose and/or throat to detect the bacteria.
People diagnosed with psittacosis usually take tetracycline antibiotics (unless contraindicated due to reported macrolide failures) to treat the infection. Tetracyclines are generally avoided in children aged <8 years, and macrolides are the drug of choice for children; however, tetracyclines could be considered when the benefits outweigh the risks, such as in life-threatening conditions or when macrolide failure is suspected. People with more severe presentation should be treated with doxycycline right away if psittacosis is suspected. Most people improve quickly if they start antibiotics soon after they get sick.
Streptococcus pneumoniae
Streptococcus pneumoniae bacteria (pneumococcus) is leading cause of community-acquired pneumonia, meningitis, and bacteremia in children and adults 57 and the most common cause of otitis media in infants and young children 58. However, Streptococcus pneumoniae bacteria are also commonly found in the respiratory track of healthy people, especially children. Streptococcus pneumoniae are lancet-shaped, gram-positive, facultative anaerobic bacteria with more than 100 known serotypes.
The Streptococcus pneumoniae bacteria may be isolated from the nasopharynx of 5–90% of healthy persons, depending on the population and setting:
- 5–10% of adults without children are carriers
- 20–60% of school-aged children may be carriers
- 50–60% of service personnel on military installations may be carriers
The duration of carriage varies and is generally longer in children than adults. In addition, researchers do not clearly understand the relationship of carriage to the development of natural immunity.
The main way people spread Streptococcus pneumoniae to others is through direct contact with respiratory droplets. The bacteria often spread within households and in crowded conditions.
Pneumococcal pneumonia is the most common clinical presentation of Streptococcus pneumoniae among adults. The incubation period of pneumococcal pneumonia is short, about 1 to 3 days.
Pneumococcal pneumonia symptoms generally include an abrupt onset of fever and chills or rigors. Typically, there is a single rigor, and repeated shaking chills are uncommon. Other common symptoms include
- Pleuritic chest pain
- Cough productive of mucopurulent
- Rusty sputum
- Shortness of breath (dyspnea)
- Tachypnea (rapid breathing) or tachycardia (fast heartbeat)
- Hypoxia
- Malaise or weakness
Nausea, vomiting, and headaches occur less frequently.
The case-fatality rate is 5–7% and may be much higher among older adults or people with underlying medical conditions.
Complications of pneumococcal pneumonia include empyema (a collection of pus in the pleural space), pericarditis (swelling and irritation of the thin, saclike tissue called pericardium that surrounds the heart) and respiratory failure.
Definitively diagnosing Streptococcus pneumoniae infection generally relies on isolating the organism from blood or other normally sterile body sites. Tests are also available to detect capsular polysaccharide antigen in body fluids.
Doctors use antibiotics to treat pneumococcal disease. Antibiotic treatment for serious pneumococcal infections typically includes ‘broad-spectrum’ antibiotics until results of antibiotic sensitivity testing are available. Antibiotic sensitivity testing shows which antibiotics will be most successful at treating a bacterial infection. Broad-spectrum antibiotics work against a wide range of bacteria. Once the sensitivity of the bacteria is known, doctors may choose a more targeted (or ‘narrow-spectrum’) antibiotic.
Klebsiella pneumoniae
Klebsiella pneumoniae is a Gram-negative pathogenic bacterium that can cause different types of hospital-acquired infections (healthcare-associated infections) in the United States, including pneumonia, urinary tract infections (UTIs), bloodstream infections, wound or surgical site infections, and meningitis 59. Klebsiella pneumoniae bacteria are normally found in the human intestines (where they do not cause disease) 60. They are also found in human stool (feces). In healthcare settings, Klebsiella infections commonly occur among sick patients who are receiving treatment for other conditions. Patients whose care requires devices like ventilators (breathing machines) or intravenous (vein) catheters, and patients who are taking long courses of certain antibiotics are most at risk for Klebsiella infections. Klebsiella pneumoniae has classically been considered an opportunistic pathogen, since it typically causes infections in hospitalized or otherwise immunocompromised individuals 61. Healthy people usually do not get Klebsiella infections.
Pneumonia caused by Klebsiella pneumoniae can be broken down into two categories: community-acquired pneumonia or hospital-acquired pneumonia. Although community-acquired pneumonia is a fairly common diagnosis, infection with Klebsiella pneumoniae is rather uncommon. In the western culture, it is estimated that approximately 3% to 5% of all community-acquired pneumonia is related to an infection caused by Klebsiella pneumoniae, but in developing countries such as Africa, it can account for approximately 15% of all cases of pneumonia 62. Overall, Klebsiella pneumoniae accounts for approximately 11.8% of all hospital-acquired pneumonia in the world. In those who develop pneumonia while on a ventilator, between 8% to 12% are caused by Klebsiella pneumoniae, while only 7% occur in those patients who are not ventilated. Mortality ranges from 50% to 100% in patients with alcoholism and septicemia.
In fact, Klebsiella species have been identified as the number three cause of hospital-acquired pneumonia in the United States, defined as a pneumonia occurring ≥48 hours after hospital admission 59. Klebsiella species are also a leading cause of ventilator-associated pneumonia among patients in intensive care units (ICUs) 63 and ventilator-associated pneumonia is responsible for 83% of hospital-acquired pneumonias 64. Mortality rates in Klebsiella pneumoniae pneumonia have been reported as high as 50% 61.
To get a Klebsiella infection, a person must be exposed to the bacteria. For example, Klebsiella must enter the respiratory (breathing) tract to cause pneumoniae, or the blood to cause a bloodstream infection.
In healthcare settings, Klebsiella bacteria can be spread through person-to-person contact (for example, from patient to patient via the contaminated hands of healthcare personnel, or other persons) or, less commonly, by contamination of the environment. The bacteria are not spread through the air.
Patients in healthcare settings also may be exposed to Klebsiella when they are on ventilators (breathing machines), or have intravenous (vein) catheters or wounds (caused by injury or surgery). Unfortunately, these medical tools and conditions may allow Klebsiella to enter the body and cause infection.
Klebsiella pneumoniae are the second leading cause of bloodstream infections caused by Gram-negative bacteria, behind only E. coli 59. Cancer is the primary underlying disease associated with hospital-acquired bloodstream infections, while liver disease and diabetes mellitus had the highest association among community-acquired Klebsiella pneumoniae bloodstream infections 65. Bloodstream infection can be a primary infection with no identifiable source. However, bloodstream infection is often a secondary infection that results from dissemination into the bloodstream from a known source. Common sources of secondary bloodstream infections include the urinary tract, the gastrointestinal tract, intravenous or urinary catheters, and respiratory sites 66. The case mortality rate of bloodstream infections due to Klebsiella pneumoniae is ~20–30%, and the population mortality rate is estimated at 1.3 per 100,000 people 67.
The urinary tract is the most common site of infection by Klebsiella pneumoniae 61. As with other infections, urinary tract infection (UTI) due to Klebsiella pneumoniae are associated with diabetes mellitus 68. Catheter-associated urinary tract infections (CAUTIs) are another infection caused by Klebsiella pneumoniae. It is thought that these are facilitated by the ability for form biofilms and adhere to catheters (Schroll et al., 2010). Klebsiella are also responsible for wound/surgical site infections. This site represents ~13% of all infections caused by Klebsiella 69.
Some Klebsiella bacteria have become highly resistant to antibiotics. When bacteria such as Klebsiella pneumoniae produce an enzyme known as a carbapenemase (referred to as KPC-producing organisms), then the class of antibiotics called carbapenems will not work to kill the bacteria and treat the infection.
Klebsiella infections that are not drug-resistant can be treated with antibiotics. Infections caused by KPC-producing bacteria can be difficult to treat because fewer antibiotics are effective against them. In such cases, a microbiology laboratory must run tests to determine which antibiotics will treat the infection.
Current regimens for community-acquired Klebsiella pneumoniae pneumonia include a 14-day treatment with either a third or fourth-generation cephalosporin as monotherapy or a respiratory quinolone as monotherapy or either of the previous regimes in conjunction with an aminoglycoside 62. If the patient is penicillin-allergic, then a course of aztreonam or a respiratory quinolone should be undertaken. For hospital-acquired infections (healthcare-associated infections), a carbapenem can be used as monotherapy until sensitivities are reported 70.
When extended-spectrum beta-lactamase (ESBL) is diagnosed, carbapenem therapy should be initiated due to its rate of sensitivity across the globe. When CRE (carbapenem-resistant Enterobacteriaceae) is diagnosed, infectious disease consultation should be obtained to guide treatment. Several antibiotic options to treat CRE (carbapenem-resistant Enterobacteriaceae) include antibiotics from the polymyxin class, tigecycline, fosfomycin, aminoglycosides, or dual therapy carbapenems. Combination therapy of two or more of the agents, as mentioned earlier, may decrease mortality as compared to monotherapy alone.
Pneumocystis pneumonia
Pneumocystis pneumonia is a serious infection caused by the fungus Pneumocystis jirovecii (previously known as Pneumocystis carinii) 71. Most people who get pneumocystis pneumonia have a medical condition that weakens their immune system, like HIV/AIDS, or take medicines (such as corticosteroids) that lower the body’s ability to fight germs and sickness. In the United States, people with HIV/AIDS are less likely to get pneumocystis pneumonia today than before the availability of antiretroviral therapy (ART). However, pneumocystis pneumonia is still a substantial public health problem 72. Much of the information we have about pneumocystis pneumonia and its treatment comes from caring for patients with HIV/AIDS.
Scientists have changed both the classification and the name of Pneumocystis jirovecii since it first appeared in patients with HIV in the 1980s. Pneumocystis jirovecii used to be classified as a protozoan but is now considered a fungus 73. Pneumocystis jirovecii used to be called Pneumocystis carinii. When scientists renamed Pneumocystis carinii to Pneumocystis jirovecii, some people considered using the abbreviation “PJP,” but to avoid confusion, Pneumocystis jirovecii pneumonia is still abbreviated “pneumocystis pneumonia” 74.
Pneumocystis pneumonia is extremely rare in healthy people, but the fungus that causes this disease can live in their lungs without causing symptoms. In fact, up to 20% of adults might carry this fungus at any given time, and the immune system removes the fungus after several months 75.
Most people who get pneumocystis pneumonia have weakened immune systems, meaning that their bodies don’t fight infections well. About 30-40% of people who get pneumocystis pneumonia have HIV/AIDS 76. The other people who get pneumocystis pneumonia are usually taking medicine (such as corticosteroids) that lowers the body’s ability to fight germs or sickness or have other medical conditions, such as 76, 77:
- Chronic lung diseases
- Cancer
- Inflammatory diseases or autoimmune diseases (for example, lupus or rheumatoid arthritis)
- Solid organ or stem cell transplant
Pneumocystis pneumonia spreads from person to person through the air 78, 79. Some healthy adults can carry the Pneumocystis fungus in their lungs without having symptoms, and it can spread to other people, including those with weakened immune systems 75.
Many people are exposed to Pneumocystis jirovecii as children, but they likely do not get sick because their immune systems prevent the fungus from causing an infection 80. In the past, scientists believed that people who had been exposed to Pneumocystis jirovecii as children could later develop pneumocystis pneumonia from that childhood infection if their immune systems became weakened 81. However, it is more likely that people get pneumocystis pneumonia after being exposed to someone else who has pneumocystis pneumonia or who is carrying the fungus in their lungs without having symptoms.
The symptoms of pneumocystis pneumonia can develop over several days or weeks and include 72, 82, 75:
- Fever
- Cough
- Difficulty breathing
- Chest pain
- Chills
- Fatigue (tiredness)
Contact your healthcare provider if you have symptoms that you think are related to pneumocystis pneumonia.
Pneumocystis pneumonia is diagnosed using a sample from a patient’s lungs. The sample is usually mucus that is either coughed up by the patient called sputum or collected by a procedure called bronchoalveolar lavage (BAL). Sometimes, a small sample of lung tissue (a biopsy) is used to diagnose pneumocystis pneumonia. The patient’s sample is sent to a laboratory, usually to be examined under a microscope. Polymerase chain reaction (PCR) can also be used to detect Pneumocystis DNA in different types of samples. A blood test to detect beta-D-glucan (a part of the cell wall of many different types of fungi) can also help diagnose pneumocystis pneumonia 83.
Pneumocystis pneumonia must be treated with prescription medicine. Without treatment, pneumocystis pneumonia can cause death. The most common form of treatment is trimethoprim/sulfamethoxazole (TMP/SMX), which is also known as co-trimoxazole and by several different brand names, including Bactrim, Septra, and Cotrim. This medicine is given by mouth or through a vein for 3 weeks. Trimethoprim/sulfamethoxazole can cause side effects such as rash and fever. Other medicines are available for patients who cannot take trimethoprim/sulfamethoxazole.
For mild to moderate treatment, trimethoprim 15 to 20 mg/kg/day and sulfamethoxazole 75 to 100 mg/kg/day, given orally in 3 divided doses or trimethoprim-sulfamethoxazole double strength, 2 tablets 3 times per day 84. For moderate to severe cases, trimethoprim 15 to 20 mg/kg/day and sulfamethoxazole 75-100 mg/kg/day given intravenously (IV) every 6 to 8 hours with a switch to oral when the patient shows clinical improvement. In patients with a mild allergy to trimethoprim/sulfamethoxazole (TMP/SMX), desensitization should be attempted as this is the most effective drug of choice. In patients with severe allergies to trimethoprim/sulfamethoxazole (TMP/SMX), desensitization is no longer recommended, and it is more appropriate to choose a different drug regimen.
Alternative drug regimens for the treatment of pneumocystis pneumonia in those with sulfa allergies and mild to moderate disease include Atavaquone 750 mg, by mouth twice per day, Trimethoprim 15 mg/kg/day by mouth twice per day plus Dapsone 100 mg by mouth every day, or Primaquine 30 mg by mouth every day plus Clindamycin by mouth 450 mg every 6 hours or 600 mg every 8 hours 84. Alternative treatment for moderate to severe cases includes Pentamidine 4 mg/kg IV once daily over 60 minutes or Primaquine 30 mg by mouth every day plus Clindamycin IV 600 mg every 6 hours or 900 mg every 8 hours 84. Primaquine can only be orally administered, and patients who cannot tolerate oral medications should be given IV Pentamidine, but caution should be used due to its increased toxicity and side effects when compared to Primaquine. Caution must be used in patients with glucose-6-phosphate dehydrogenase (G6PD) deficiency if Dapsone or Primaquine are used as they can cause an increased risk of hemolytic anemia.
In HIV-infected patients with a moderate or severe disease, current recommendations suggest the addition of glucocorticoids to the treatment regimen as their use has been shown to improve clinical outcome and mortality 84. HIV-infected patients with a room air arterial blood gas partial pressure of oxygen that is less than or equal to 70 mm Hg, an alveolar-arterial (A-a) gradient greater than or equal to 35 mm Hg, or hypoxia on pulse oximetry should receive steroids 84. Corticosteroids also may be recommended in HIV-uninfected patients with pneumocystis pneumonia due to the potential for high mortality and fulminant course of illness, but data is limited on whether there are benefits or a decrease in in-hospital mortality. Dosing for prednisone should be started as soon as possible or within 72 hours of starting treatment for pneumocystis pneumonia and is as follows: 40 mg by mouth twice per day on days 1 through 5, 40 mg by mouth daily days 6 through 10, and 20 mg orally daily on days 11 through 21 84. IV methylprednisone can be given at 75% of the prednisone dose if oral therapy cannot be tolerated. HIV-infected patients who are not already on them should have antiretroviral therapy (ART) initiated within two weeks of Pneumocystis treatment or as soon as they are stable enough to begin treatment. Patients will usually show slightly worsening clinical signs around days 3 to 4 due to the host’s inflammatory response to dying organisms and then improvement afterward.
Prophylaxis treatment guidelines have been established for certain patient populations. Patients who are immunocompromised such as those with malignancy and who are taking glucocorticoid doses greater than 20 mg daily for one month or longer, patients who have received bone marrow suppressive therapies or antineoplastic therapies, and those who have undergone hematopoietic cell or solid organ transplantation should receive primary prophylaxis for Pneumocystis. First-line prophylaxis treatment is trimethoprim-sulfamethoxazole 1 double-strength tablet by mouth daily or 1 single-strength tablet by mouth daily 84. For those with sulfa allergies, recommended prophylaxis includes Dapsone 100 mg by mouth daily or 50 mg by mouth twice each day, Dapsone 50 mg by mouth daily plus pyrimethamine 50 mg plus leucovorin 25 mg by mouth weekly, Dapsone 200 mg plus pyrimethamine 75 mg plus leucovorin 25 mg by mouth weekly, Atovaquone 1500 mg by mouth daily, Atovaquone 1500 mg plus pyrimethamine 25 mg plus leucovorin 10 mg by mouth daily, or Aerosolized pentamidine 300 mg monthly via Respigard II nebulizer. HIV-infected individuals should receive prophylaxis with the same medications recommended above when CD4+ count is below 200 cells/microL or CD4+ less than 14 percent, presence of oropharyngeal candidiasis, and a CD4+ of 200-250 cells/microL when ART cannot be started or if monitoring of CD4+ count every 3 months is not possible.
Currently, at least 10-20% of patients with pneumocystis pneumonia will die. Pneumocystis pneumonia carries an even worse prognosis in patients without HIV infection, with mortality rates over 50%. In general, the mortality rates are much higher when there is an underlying lung disorder and in patients who require mechanical ventilation 85.
Fungal pneumonia
Fungal pneumonia is a pneumonia caused by one or more endemic or opportunistic fungi. Fungal infection occurs following the inhalation of spores, after the inhalation of conidia, or by the reactivation of a latent infection. Blood dissemination frequently occurs, especially in an immunocompromised host.
Endemic fungal pathogens (eg, Histoplasma capsulatum, Coccidioides immitis, Blastomyces dermatitidis, Paracoccidioides brasiliensis, Sporothrix schenckii, Cryptococcus neoformans) cause infection in healthy hosts and in immunocompromised persons, in defined geographic locations of the Americas and around the world 86.
Opportunistic fungal organisms (eg, Candida species, Aspergillus species, Mucor species) tend to cause pneumonia in patients with congenital or acquired defects in the host immune defenses 87. Hyalohyphomycosis is a broad term that describes infections due to a number of rare and emerging heterogeneous fungi that when isolated from infected lung tissue, appear as hyaline (lightly colored), filamentous fungi difficult to distinguish from Aspergillus. These genera include Scedosporium, Fusarium, Paecilomyces, Acremonium, and Trichoderma 86.
The diagnosis of fungal pneumonias is difficult to prove and is often made on a presumptive basis 86. It relies on a combination of clinical, radiologic, and microbiological factors 88. Candida organisms and some ubiquitous filamentous fungi (Aspergillus and Scedosporium) can be isolated from oropharyngeal and respiratory tracts as colonizers without evidence of invasion or symptoms until a breakdown of tissue barriers or of the host’s immune system occurs. Nonmolecular fungal markers in serum or other biological samples represent a noninvasive diagnostic tool, which can help in therapeutic decisions 87.
Conditions that predispose people to any of the opportunistic fungal pathogens are as follows:
- Acute leukemia or lymphoma during myeloablative chemotherapy
- Bone marrow or peripheral blood stem cell transplantation
- Solid organ transplantation on immunosuppressive treatment
- Prolonged corticosteroid therapy
- Acquired immunodeficiency syndrome (AIDS)
- Prolonged neutropenia from various causes
- Congenital immune deficiency syndromes
- Postsplenectomy state
- Genetic predisposition
Workers or farmers with heavy exposure to bird, bat, or rodent droppings or other animal excreta in endemic areas are predisposed to any of the endemic fungal pneumonias, such as histoplasmosis, in which the environmental exposure to avian or bat feces encourages the growth of the organism. In addition, farmers, nursery workers, landscapers, and gardeners are at higher risk of acquiring sporotrichosis because of their chance of cuts or puncture wounds while working with soil. The Pseudoallescheria boydii/Scedosporium apiospermum complex has been implicated as an important pathogen in delayed disseminated infections among victims of near-drowning in polluted waters 89 or recent natural disasters 90.
Complications of fungal pneumonia include:
- disease dissemination to other sites (ie, brain, meninges, skin, liver, spleen, kidneys, adrenals, heart, eyes) and sepsis syndrome and
- blood vessel invasion, which can lead to hemoptysis, pulmonary infarction, myocardial infarction, cerebral septic emboli, cerebral infarction, or blindness.
Other complications may include the following:
- Bronchopleural or tracheoesophageal fistulas
- Chronic pulmonary symptoms
- Mediastinal fibromatosis (histoplasmosis)
- Broncholithiasis (histoplasmosis)
- Pericarditis and other rheumatologic symptoms
Signs and symptoms of fungal pneumonia may include the following 91:
- Fever
- Cough, usually nonproductive
- Pleuritic chest pain or dull discomfort
- Progressive dyspnea leading to respiratory failure
- Airway obstructive symptoms from enlarged mediastinal adenopathy in the endemic mycoses
- Hemoptysis (in invasive aspergillosis or mucormycosis)
- History of travel to or exposure in areas containing endemic mycoses
- Symptoms from involvement of extrapulmonary systems (may suggest disease)
- Rheumatologic syndromes (common among endemic mycoses) – Arthritis and arthralgia, erythema nodosum, erythema multiforme, and pericarditis
- Endemic mycoses with associated dissemination
- Hypersensitivity or allergic reactions
- Extrapulmonary sites in individuals who are immunocompromised
- Meningoencephalitis in patients with AIDS and cryptococcosis
In individuals who are neutropenic or immunocompromised, persistent fever (even before pulmonary findings) may be an early sign of infection, especially if the fever is unresponsive to broad-spectrum antibiotics.
Hypersensitivity or allergic reactions include allergic bronchial asthma (Aspergillus species, Candida species), allergic bronchopulmonary mycoses (Aspergillus species, Candida species), bronchocentric granulomatosis (necrotizing granulomatous replacement and eosinophilic infiltration of bronchial mucosa in infection with Aspergillus species), and extrinsic allergic alveolitis (malt worker’s lung, farmer’s lung).
Nonculture-based diagnostic tools, such as galactomannan and beta-D-glucan, are part of the diagnostic workup of invasive fungal pneumonia with other clinical, radiologic, and microbiologic criteria. Galactomannan enzyme immunoassay (GM-EIA) for detection of invasive aspergillosis, are now in clinical use. Polymerase chain reaction (PCR)–based assays are also available for detecting various pathogens, including Aspergillus, Histoplasma, and Candida species 92, 93.
Therapy for fungal pneumonias must include antifungal agents. The type of antifungal drug employed must be selected based on the particular pathogen that is isolated or that is clinically suspected. Many classes of antifungal agents are now available, including the classic antibiotics; first-, second-, and third-generation triazoles; and the echinocandins. In patients with invasive aspergillosis, including pulmonary aspergillosis, voriconazole is the new standard of care, based on its superiority over amphotericin B as primary therapy 94. Vary the dose and treatment duration depending on the underlying pathogen causing the pneumonia. Care should be taken regarding patients on long-term voriconazole treatment. Bone pain with radiologic evidence of periostitis and 10-fold increased fluoride levels have been reported in allogeneic stem cell transplant patients taking the drug for at least 3 months. Symptoms and findings were reversed with discontinuation of voriconazole 95. There is a possible association between the use of voriconazole in markedly immunosuppressed patients as prophylactic agent and the development of mucormycosis, but this matter is still controversial 94.
Amphotericin B is less frequently used and, when used, is often given as a liposomal formulation to decrease toxicity 94.
Complications of pneumonia
Complications of pneumonia are more common in young children, the elderly and those with pre-existing health conditions, such as diabetes.
People who have heart or lung problems, people who smoke, and people who are 65 years of age and older are more likely to experience complications from pneumonia.
Possible complications of pneumonia include:
- Difficulty breathing. If your pneumonia is severe or you have chronic underlying lung diseases, you may have trouble breathing in enough oxygen. You may need to be hospitalized and use a breathing machine (ventilator) while your lung heals.
- Pleurisy – where the thin linings between your lungs and ribcage (pleura) become inflamed, which can lead to respiratory failure
- Pleural effusion is when fluid builds up in the layers of tissue between your lungs and the wall of your chest cavity (pleura) and becomes infected. Pleural effusion can make breathing very difficult. To drain the fluid, a tube may need to be placed between your lungs and your chest wall, or you may need surgery.
- Lung abscess – a rare complication that’s mostly seen in people with a serious pre-existing illness or a history of severe alcohol misuse. An abscess occurs if pus forms in a cavity in the lung. An abscess is usually treated with antibiotics. Sometimes, surgery or drainage with a long needle or tube placed into the abscess is needed to remove the pus.
- Kidney failure (renal failure) is a term used to describe a situation in which the kidneys are no longer able to function effectively. If your kidneys fail, you need treatment to replace the work they normally do. The treatment options are dialysis or a kidney transplant.
- Respiratory failure. Respiratory failure is a condition in which your blood doesn’t have enough oxygen (O2) or has too much carbon dioxide (CO2). Sometimes you can have both problems. A low oxygen level in the blood can cause shortness of breath and air hunger (the feeling that you can’t breathe in enough air). Your skin, lips, and fingernails may also have a bluish color. A high carbon dioxide level can cause rapid breathing and confusion. Some people who have respiratory failure may become very sleepy or lose consciousness. They also may have arrhythmia (irregular heartbeat). You may have these symptoms if your brain and heart are not getting enough oxygen.
- Bacteria in the bloodstream (bacteremia). Bacteria that enter the bloodstream from your lungs can spread the infection to other organs, potentially causing organ failure.
- Blood poisoning (septicemia) – also a rare but serious complication
You’ll be admitted to hospital for treatment if you develop one of these complications.
Your doctor may give you oxygen to help you breathe or antibiotics through an IV.
Bacteria in the bloodstream occur when the pneumonia infection in your lungs spreads to your blood. This increases the risk that the infection will spread to other organs in your body. Bacteria in the bloodstream are treated with antibiotics.
Bronchitis vs Pneumonia
Bronchitis is the inflammation of the larger airways in your lungs, causing an ongoing cough.
Bronchitis can be caused by viruses, bacteria, or breathing in smoke or dust.
- Acute bronchitis is usually caused by a viral infection, such as cold viruses or influenza virus and can last for weeks, whereas chronic bronchitis lasts for months and may come back each year.
- Chronic bronchitis is usually related to smoking. Chronic bronchitis is defined as a productive cough that lasts at least three months, with recurring bouts occurring for at least two consecutive years.
Most people with acute bronchitis will feel better with time and rest, with a number of treatments available to help ease the cough and other symptoms.
If you think you have bronchitis, your doctor can assess you and discuss treatment.
Is bronchitis contagious?
Mostly, bronchitis is caused by contagious viruses. These can be spread by air when someone coughs, or by touch after the virus is left on a surface.
Hand washing, covering your mouth when coughing and staying home while unwell can reduce the spread.
People at risk of developing bronchitis include:
- the elderly
- people breathing in irritating chemicals
- smokers
- those with a lung condition, such as asthma
- people with poor immunity
You can reduce your risk by hand washing, and if you smoke, cutting down or quitting. The annual flu vaccine is recommended for people with chronic bronchitis.
Bronchitis causes
Acute bronchitis is usually caused by viruses, typically the same viruses that cause colds and flu (influenza). Antibiotics don’t kill viruses, so this type of medication isn’t useful in most cases of bronchitis.
The most common cause of chronic bronchitis is cigarette smoking. Air pollution and dust or toxic gases in the environment or workplace also can contribute to the condition.
Bronchitis symptoms
Someone with bronchitis may have:
- cough (either dry or bringing up phlegm). Mucus (phlegm or sputum), which can be clear, white, yellowish-gray or green in color — rarely, it may be streaked with blood
- wheezing
- aches and pains
- fever
- feeling short of breath
- chest tightness
Risk factors for bronchitis
Factors that increase your risk of bronchitis include:
- Cigarette smoke. People who smoke or who live with a smoker are at higher risk of both acute bronchitis and chronic bronchitis.
- Low resistance. This may result from another acute illness, such as a cold, or from a chronic condition that compromises your immune system. Older adults, infants and young children have greater vulnerability to infection.
- Exposure to irritants on the job. Your risk of developing bronchitis is greater if you work around certain lung irritants, such as grains or textiles, or are exposed to chemical fumes.
- Gastric reflux. Repeated bouts of severe heartburn can irritate your throat and make you more prone to developing bronchitis.
Bronchitis complications
Although a single episode of bronchitis usually isn’t cause for concern, it can lead to pneumonia in some people. Repeated bouts of bronchitis, however, may mean that you have chronic obstructive pulmonary disease (COPD).
Do you need a chest X-ray for bronchitis?
An X-ray is usually not necessary for simple cases of bronchitis.
Bronchitis treatment
Because most cases of bronchitis are caused by viral infections, antibiotics aren’t effective. Most people with acute bronchitis will feel better with time and rest, usually within a couple of weeks.
You can help ease the cough and other symptoms by:
- inhaling steam or having a warm bath
- avoiding cigarette smoke and other irritants
- drinking plenty of fluids
- simple pain relief medication, such as paracetamol (follow the directions on the label)
- a teaspoon of honey at night, either by itself or in warm water
- consider a face mask outside. If cold air aggravates your cough and causes shortness of breath, put on a cold-air face mask before you go outside.
Cough medicines are available, but they might or might not help.
If you are very unwell or not getting better, or if you get worse, see your doctor.
Pneumonia causes
Many germs can cause pneumonia. The most common are bacteria and viruses in the air we breathe. Your body usually prevents these germs from infecting your lungs. But sometimes these germs can overpower your immune system, even if your health is generally good.
Pneumonia is usually the result of a pneumococcal infection, caused by bacteria called Streptococcus pneumoniae.
Many different types of bacteria, including Haemophilus influenzae and Staphylococcus aureus, can also cause pneumonia, as well as viruses and, more rarely, fungi.
As well as bacterial pneumonia, other types include:
- Viral pneumonia – most commonly caused by the respiratory syncytial virus (RSV) and sometimes influenza type A or B; viruses are a common cause of pneumonia in young children
- Aspiration pneumonia – caused by breathing in vomit, a foreign object, such as a peanut, or a harmful substance, such as smoke or a chemical
- Fungal pneumonia – rare in the US and more likely to affect people with a weakened immune system
- Hospital-acquired pneumonia – pneumonia that develops in hospital while being treated for another condition or having an operation; people in intensive care on breathing machines are particularly at risk of developing ventilator-associated pneumonia
Higher Risk groups
The following groups have an increased risk of developing pneumonia:
- babies and very young children
- elderly people
- people who smoke
- people with other health conditions, such as asthma, cystic fibrosis, or a heart, kidney or liver condition
- people with a weakened immune system – for example, as a result of a recent illness, such as flu, having HIV or AIDS, having chemotherapy, or taking medication following an organ transplant.
Who is at risk of developing pneumonia?
You are more at risk of developing pneumonia if:
- Chronic obstructive pulmonary disease (COPD), especially if you have taken inhaled corticosteroids for 24 weeks or longer
- Human immunodeficiency virus (HIV)
- Acquired immunodeficiency syndrome (AIDS)
- Heart disease
- Emphysema
- Diabetes
You are older than 65 years of age. As you get older, your immune system becomes less able to fight off infections like pneumonia. Babies and young children are also at increased risk because their immune systems are not yet fully developed.
You have a disease or condition that weakens your immune system. When your immune system is weakened, it’s easier for you to get pneumonia because your body can’t fight off the infection. People who have weakened immune systems are also more likely to develop pneumonia from bacteria, viruses and germs that don’t cause pneumonia in healthy people.
People who have any of the following are at increased risk:
- People who have recently had an organ transplant and people who are receiving chemotherapy are also at increased risk.
- You work in construction or agriculture. Working in environments where you breathe in dust, chemicals, air pollution or toxic fumes can damage your lungs and make them more vulnerable to infections like pneumonia.
- You smoke or abuse alcohol. Smoking damages the tiny hairs in the lungs that help remove germs and bacteria. Alcohol abuse can put you at increased risk of aspiration pneumonia,a type of pneumonia that develops after you inhale particles into your lungs.This occurs most often when you vomit and small particles enter your lungs because you are not strong enough to cough the particles out. Alcohol abuse also interferes with the way your white blood cells (which are responsible for fighting infection) work.
- You are hospitalized, especially in an intensive care unit (ICU). Pneumonia that you catch in a hospital (called hospital-acquired pneumonia) can be more serious than other types of pneumonia. Your risk increases if you are using a ventilator to help you breathe. Ventilators make it hard for you to cough and can trap germs that cause infection in your lungs.
- You have recently had major surgery or a serious injury. Recovering from major surgery or a serious injury often makes you weak. It can also make it difficult for you to cough, which is the body’s quickest defense for getting particles out of the lungs. Recovery also typically requires a lot of bed rest. Lying down on your back for an extended period of time can allow fluid or mucus to gather in your lungs, giving bacteria a place to grow.
- You are of Native Alaskan or Native American descent. For reasons unknown to doctors, people of these ethnic groups are at increased risk for pneumonia.
Risk factors for developing pneumonia
Pneumonia can affect anyone. But the two age groups at highest risk for pneumonia are:
- Children who are 2 years old or younger
- People who are age 65 or older
Other risk factors include:
- Being hospitalized. You’re at greater risk of pneumonia if you’re in a hospital intensive care unit, especially if you’re on a machine that helps you breathe (a ventilator).
- Chronic disease. You’re more likely to get pneumonia if you have asthma, chronic obstructive pulmonary disease (COPD) or heart disease.
- Smoking. Smoking damages your body’s natural defenses against the bacteria and viruses that cause pneumonia.
- Weakened or suppressed immune system. People who have HIV/AIDS, who’ve had an organ transplant, or who receive chemotherapy or long-term steroids are at risk.
Pneumonia prevention
Although most cases of pneumonia are bacterial and aren’t passed on from one person to another, ensuring good standards of hygiene will help prevent germs spreading.
You can help prevent pneumonia by doing the following:
- Get the flu vaccine each year. People often develop bacterial pneumonia after a case of the flu. You can reduce this risk by getting the yearly flu shot. The flu shot doesn’t protect against all strains of the flu, just the 3 to 4 strains that doctors feel will be most dangerous or wide spread in the coming year. The seasonal flu vaccine protects against the influenza viruses that research indicates will be most common during the upcoming season. Traditional flu vaccines (called “trivalent” vaccines) are made to protect against three flu viruses; an influenza A (H1N1) virus, an influenza A (H3N2) virus, and an influenza B virus. There are also flu vaccines made to protect against four flu viruses (called “quadrivalent” vaccines). These vaccines protect against the same viruses as the trivalent vaccine and an additional B virus. The flu vaccine is usually given in September through October, before flu season starts.
- Get the pneumococcal vaccine. Pneumococcus vaccines are especially important for people at high risk of pneumonia, including:
- Adults age 65 or older
- Children age 2 or younger
- People who have chronic (ongoing) diseases, serious long-term health problems, or weak immune systems. This may include people who have cancer, HIV, asthma, sickle cell disease, or damaged or removed spleens.
- People who smoke
- Haemophilus influenzae type b (Hib) vaccine. Haemophilus influenzae type b (Hib) is a type of bacteria that can cause pneumonia and meningitis. The Haemophilus influenzae type b (Hib) vaccine is recommended for all children under 5 years old in the United States. The Hib vaccine often is given to infants starting when they are 2 months old.
- Keep your immune system strong. Get enough sleep, exercise regularly and eat a healthy diet.
- Practice good hygiene. Your hands come in contact with many germs throughout the day. You pick them up from surfaces such as doorknobs, other people’s hands and your computer keyboard. Take time to wash your hands often, especially after using the restroom and before eating. Use lukewarm water and soap for at least 20 seconds. If soap and water are not available,using an alcohol-based hand sanitizer is the next best thing.
- cover your mouth and nose with a handkerchief or tissue when you cough or sneeze
- throw away used tissues immediately – germs can live for several hours after they leave your nose or mouth
- Don’t smoke. Smoking damages your lungs and makes it harder for your body to defend itself from germs and disease. If you smoke, talk to your doctor about quitting as soon as possible.
- Practice a healthy lifestyle. Eat a balanced diet full of fruits and vegetables. Exercise regularly. Get plenty of sleep. These things help your immune system stay strong.
- Excessive and prolonged alcohol misuse also weakens your lungs’ natural defences against infections, making you more vulnerable to pneumonia.
- Avoid sick people. Being around people who are sick increases your risk of catching what they have.
- If you have problems swallowing, eat smaller meals of thickened food and sleep with the head of your bed raised up. These steps can help you avoid getting food, drink, or saliva into your lungs.
- If you have a planned surgery, your doctor may recommend that you don’t eat for 8 hours or drink liquids for 2 hours before your surgery. This can help prevent food or drink from getting into your airway while you are sedated.
- If your immune system is impaired or weakened, your doctor may recommend you take antibiotics to prevent bacteria from growing in your lungs.
Pneumonia shot
Pneumococcal disease is common in young children, but older adults are at greatest risk of serious illness and death. There are two kinds of vaccines that help prevent pneumococcal disease.
There isn’t a vaccine for all types of pneumonia, but 2 vaccines are available that help prevent pneumococcal disease, which is any type of infection caused by Streptococcus pneumoniae bacteria.
- The first is called the pneumococcal conjugate vaccine (PCV) or (PCV13 or Prevnar 13®). It is recommended for all children younger than 5 years of age.
- The pneumococcal polysaccharide vaccine (PPSV) or (PPSV23 or Pneumovax23®) is recommended for children 2 years of age and older who are at increased risk for pneumonia (such as children who have weakened immune systems), and for adults who have risk factors for pneumonia.
The Centers for Disease Control and Prevention (CDC) recommends pneumococcal conjugate (PCV) vaccination for:
- All babies and children younger than 2 years old
- All adults 65 years or older
- People 2 through 64 years old with certain medical conditions
CDC recommends pneumococcal polysaccharide (PPSV) vaccination for:
- All adults 65 years or older
- People 2 through 64 years old with certain medical conditions
- Adults 19 through 64 years old who smoke cigarettes
The pneumococcal vaccine is recommended if you:
- Are 65 years of age or older
- Smoke
- Abuse alcohol
- Have certain chronic conditions, such as asthma, diabetes, heart disease or lung disease
- Have cirrhosis
- Have a condition that weakens your immune system, such as the human immunodeficiency virus (HIV), acquired immunodeficiency syndrome (AIDS), kidney failure or a damaged spleen
- Have had your spleen removed for any reason
- Have sickle cell disease
- Have cochlear implants (an electronic device that helps you hear)
- Are taking medicine for a recent organ transplant (these medicines suppress your immune system)
- Are receiving chemotherapy
Pneumococcal vaccines that help protect against pneumococcal disease work well, but cannot prevent all cases. But they can make it less likely that people who are at risk will experience the severe, and possibly life-threatening, complications of pneumonia.
Studies* show that at least 1 dose of pneumococcal conjugate vaccine (PCV) protects:
- At least 8 in 10 babies from serious infections called invasive pneumococcal disease
- 75 in 100 adults 65 years or older against invasive pneumococcal disease
- 45 in 100 adults 65 years or older against pneumococcal pneumonia
Studies* show that 1 dose of pneumococcal polysaccharide vaccine (PPSV) protects:
- Between 50 to 85 in 100 healthy adults against invasive pneumococcal disease.
Who Should NOT Get These Vaccines?
Because of age or health conditions, some people should not get certain vaccines or should wait before getting them. Read the guidelines below and ask your or your child’s healthcare professional for more information.
Pneumococcal Conjugate Vaccine (PCV)
Tell the person who is giving you or your child a pneumococcal conjugate vaccine if:
You or your child have had a life-threatening allergic reaction or have a severe allergy.
- Anyone who has had a life-threatening allergic reaction to any of the following should not get PCV13:
- A dose of this vaccine
- An earlier pneumococcal conjugate vaccine called PCV7 (or Prevnar®)
- Any vaccine containing diphtheria toxoid (for example, DTaP)
- Anyone with a severe allergy to any component of PCV13 should not get the vaccine. Your or your child’s healthcare professional can tell you about the vaccine’s components.
You or your child are not feeling well.
People who have a mild illness, such as a cold, can probably get the vaccine. People who have a more serious illness should probably wait until they recover. Your or your child’s healthcare professional can advise you.
Pneumococcal Polysaccharide Vaccine (PPSV)
Children younger than 2 years old should not get this vaccine. In addition, tell the person who is giving you or your child a pneumococcal polysaccharide vaccine if:
You or your child have had a life-threatening allergic reaction or have a severe allergy.
- Anyone who has had a life-threatening allergic reaction to PPSV23 should not get another dose.
- Anyone who has a severe allergy to any component of PPSV23 should not get it. Your or your child’s healthcare professional can tell you about the vaccine’s components.
You or your child are not feeling well.
- People who have a mild illness, such as a cold, can probably get the vaccine. People who have a more serious illness should probably wait until they recover. Your or your child’s healthcare professional can advise you.
You are pregnant.
- There is no evidence that PPSV23 is harmful either to a pregnant woman or to her baby. However, as a precaution, women who need the vaccine should get it before becoming pregnant, if possible.
What Are the Possible Side Effects of pneumococcal vaccination?
Most people who get a pneumococcal vaccine do not have any serious problems with it. With any medicine, including vaccines, there is a chance of side effects. These are usually mild and go away on their own within a few days, but serious reactions are possible.
Mild Problems
Pneumococcal Conjugate Vaccine (PCV)
Mild problems following pneumococcal conjugate vaccination can include:
- Reactions where the shot was given
- Redness
- Swelling
- Pain or tenderness
- Fever
- Loss of appetite
- Fussiness (irritability)
- Feeling tired
- Headache
- Chills
Young children who get pneumococcal conjugate vaccine at the same time as inactivated flu vaccine may be at increased risk for seizures caused by fever. Ask your doctor for more information.
Pneumococcal Polysaccharide Vaccine (PPSV)
Mild problems following pneumococcal polysaccharide vaccination can include:
- Reactions where the shot was given
- Redness
- Pain
- Fever
- Muscle aches
If these problems occur, they usually go away within about two days.
Problems that Could Happen After Getting Any Injected Vaccine
- People sometimes faint after a medical procedure, including vaccination. Sitting or lying down for about 15 minutes can help prevent fainting and injuries caused by a fall. Tell your healthcare professional if you or your child:
- Feels dizzy
- Has vision changes
- Has ringing in the ears
- Some people get severe pain in the shoulder and have difficulty moving the arm where the doctor gave the shot. This happens very rarely.
- Any medicine can cause a severe allergic reaction. Such reactions from a vaccine are very rare, estimated at about 1 in a million doses. These types of reactions would happen within a few minutes to a few hours after the vaccination.
- As with any medicine, there is a very remote chance of a vaccine causing a serious injury or death.
Pneumonia diagnosis
Your doctor will diagnose pneumonia based on your medical history and the results from a physical exam.
Pneumonia can be difficult to diagnose because it shares many symptoms with other conditions, such as the common cold, bronchitis and asthma.
To help make a diagnosis, your doctor may ask you:
- whether you feel breathless or you’re breathing faster than usual
- how long you’ve had your cough, and whether you’re coughing up mucus and what color it is
- if the pain in your chest is worse when you breathe in or out
Your doctor may also take your temperature and listen to your chest and back with a stethoscope to check for any crackling or rattling sounds.
They may also listen to your chest by tapping it. Lungs filled with fluid produce a different sound from normal healthy lungs.
If you have mild pneumonia, you probably won’t need to have a chest X-ray or any other tests.
If pneumonia is suspected, your doctor may recommend the following tests:
- Blood tests. Blood tests are used to confirm an infection and to try to identify the type of organism causing the infection. However, precise identification isn’t always possible.
- Chest X-ray. A chest X-ray looks for inflammation in your lungs. This helps your doctor diagnose pneumonia and determine the extent and location of the infection. However, it can’t tell your doctor what kind of germ is causing the pneumonia.
- Pulse oximetry. Pulse oximetry measures how much oxygen is in your blood. Pneumonia can prevent your lungs from moving enough oxygen into your bloodstream. To measure the levels, a small sensor called a pulse oximeter is attached to your finger or ear.
- Sputum test. A sample of fluid from your lungs (sputum) is taken after a deep cough and analyzed to help pinpoint the cause of the infection and to find out what germ is causing your pneumonia.
Your doctor might order additional tests if you’re older than age 65, are in the hospital, or have serious symptoms or health conditions. These may include:
- CT scan. If your pneumonia isn’t clearing as quickly as expected, your doctor may recommend a chest CT scan to obtain a more detailed image of your lungs. Chest CT scan can also show whether you have complications such as lung abscesses or pleural disorders. A CT scan shows more detail than a chest X-ray.
- Arterial blood gas test. A blood gas test may be done if you are very sick. For this test, your doctor measures your blood oxygen levels using a blood sample from an artery, usually in your wrist.
- Blood culture. A blood culture is a test that checks samples of your blood for the presence of disease-causing germs like bacteria and fungi. During blood culture test, a blood sample is placed in a special container in a laboratory and watched to see if germs grow. Blood culture testing is frequently used to identify the germ causing your pneumonia and determine if germs have entered the bloodstream. A blood culture test identifies the specific germ causing an infection and enables further testing to determine what type of treatment may be most effective.
- Polymerase chain reaction (PCR) test quickly checks your blood or sputum sample to find the DNA of germs that cause pneumonia.
- Bronchoscopy looks inside your airways. If your treatment is not working well, this procedure may be needed. At the same time, your doctor may also collect samples of your lung tissue and fluid from your lungs to help find the cause of your pneumonia.
- Pleural fluid culture. A fluid sample from the pleural space between your lungs and chest wall is taken by putting a needle between your ribs from the pleural area (thoracentesis) and analyzed to help determine the type of infection.
Pneumonia treatment
Treatment for pneumonia depends on the type of pneumonia you have, which germ is causing it, how severe your symptoms are, how healthy you are overall and your age.
The goals of treatment are to cure the infection and prevent complications. It is important to follow your treatment plan carefully until you are fully recovered.
Treatment for pneumonia may include:
- Antibiotics treat bacterial pneumonia and some types of fungal pneumonia. They do not work for viral pneumonia.
- In some cases, your doctor may prescribe antiviral medicines for viral pneumonia
- Antifungal medicines treat other types of fungal pneumonia
You may need to be treated in a hospital if your symptoms are severe or if you are at risk for complications. While there, you may antibiotics given through an intravenous (IV) line and oxygen therapy. For example, if your blood oxygen level is low, you may receive oxygen therapy.
It may take several weeks to recover from pneumonia. Some people feel better within a week. For other people, it can take a month or more.
Mild pneumonia can usually be treated at home by:
- getting plenty of rest
- taking antibiotics
- drinking plenty of fluids
If you don’t have any other health problems, you should respond well to treatment and soon recover, although your cough may last for some time.
It’s usually safe for someone with pneumonia to be around others, including family members.
However, people with a weakened immune system are less able to fight off infections, so it’s best they avoid close contact with a person with pneumonia.
For at-risk groups, pneumonia can be severe and may need to be treated in hospital. This is because it can lead to serious complications, which in some cases can be fatal, depending on a person’s health and age.
For bacterial pneumonia, your doctor will probably prescribe antibiotics. Most of your symptoms should improve within a few days, although a cough can last for several weeks. Be sure to follow your doctor’s directions carefully. Take all the antibiotic medicine that your doctor prescribes. If you don’t, some bacteria may stay in your body. This can cause your pneumonia to come back. It can also increase your risk of antibiotic resistance.
- Unless a healthcare professional tells you otherwise, you should always finish taking a prescribed course of antibiotics, even if you feel better.
- If you stop taking an antibiotic part way through a course, the bacteria can become resistant to the antibiotic.
After starting treatment, your symptoms should steadily improve.
However, how quickly they improve will depend on how severe your pneumonia is.
As a general guide, after:
- one week – fever should have gone
- four weeks – chest pain and mucus production should have substantially reduced
- six weeks – cough and breathlessness should have substantially reduced
- three months – most symptoms should have resolved, but you may still feel very tired (fatigue)
- six months – most people will feel back to normal
Visit your doctor if your symptoms don’t improve within three days of starting antibiotics.
Symptoms may not improve if:
- the bacteria causing the infection is resistant to antibiotics – your doctor may prescribe a different antibiotic, or they may prescribe a second antibiotic for you to take with the first one
- a virus is causing the infection, rather than bacteria – antibiotics have no effect on viruses, and your body’s immune system will have to fight the viral infection by creating antibodies
Painkillers, such as acetaminophen (paracetamol) or ibuprofen, may help relieve pain and reduce fever. DO NOT give aspirin to children.
However, you shouldn’t take ibuprofen if you:
- are allergic to aspirin or other non-steroidal anti-inflammatory drugs (NSAIDs)
- have asthma, kidney disease, a history of stomach ulcers or indigestion
Cough medicines aren’t recommended as there’s also little evidence they are effective. A warm honey and lemon drink can help relieve discomfort caused by coughing.
Your cough may persist for two to three weeks after you finish your course of antibiotics, and you may feel tired for even longer as your body continues to recover.
Drink plenty of fluids to avoid dehydration, and get plenty of rest to help your body recover.
If you smoke, it’s more important than ever to stop, as smoking damages your lungs.
See your doctor if, after following the above self-help measures, your condition is deteriorating or isn’t improving as expected.
Pneumonia is commonly caused by viruses or bacteria passed from one person to another. But healthy people are normally able to fight off these germs without pneumonia developing. So it’s usually safe for someone with pneumonia to be around others, including family members.
However, people with a weakened immune system are less able to fight off infections, so it’s best they avoid close contact with a person with pneumonia.
Antibiotics don’t work to treat viral infections. If you have viral pneumonia, your doctor will likely talk to you about ways to treat your symptoms and your doctor may prescribe an antiviral medication to treat it. Sometimes, though, symptom management and rest are all that is needed. Over-the-counter (OTC) medicines are available to lower fever,relieve pain and ease your cough. However, some coughing is okay because it can help clear your lungs. Be sure to talk to your doctor before you take a cough suppressant.
If a fungus is causing your pneumonia, your doctor may prescribe an antifungal medicine.
If your case of pneumonia is severe, you may need to be hospitalized. If you are experiencing shortness of breath, you may be given oxygen to help your breathing. You might also receive antibiotics intravenously(through an IV). People who have weakened immune systems, heart disease or lung conditions, and people who were already very sick before developing pneumonia are most likely to be hospitalized. Babies, young children and adults who are 65 years of age and older are also at increased risk.
Home remedies
In addition to taking any antibiotics and/or medicine your doctor prescribes, you should also do the following:
- Get lots of rest. Rest will help your body fight the infection.
- Drink plenty of fluids. Fluids will keep you hydrated and can help loosen the mucus in your lungs. Try water, warm tea and clear soups to help open your airways and ease your breathing.
- Do not take cough medicines without first talking to your doctor. Coughing is one way your body works to get rid of an infection. If your cough is preventing you from getting the rest you need, ask your doctor about steps you can take to get relief.
- Stop smoking if you smoke, and avoid secondhand smoke. Smoke can make your symptoms worse. Smoking also increases your risk of developing pneumonia and other lung problems in the future. You should also avoid lit fireplaces or other areas where the air may not be clean.
- Stay home from school or work until your symptoms go away. This usually means waiting until your fever breaks and you aren’t coughing up mucus. Ask your doctor when it’s okay for you to return to school or work.
- Use a cool-mist humidifier or take steamy baths to help clear your lungs and make it easier for you to breathe.
Contact your doctor right away if your breathing gets worse instead of better over time.
If your pneumonia is so severe that you are treated in the hospital, you may be given intravenous fluids and antibiotics, as well as oxygen therapy, and possibly other breathing treatments.
Follow up with your doctor
Your doctor may schedule a follow-up appointment after he or she diagnoses you with pneumonia. At this visit, your doctor might take another chest X-ray to make sure the pneumonia infection is clearing up. Keep in mind that chest X-rays can take months to return to normal. However, if your symptoms are not improving, your doctor may decide to try another form of treatment.
Although you may be feeling better, it’s important to keep your follow-up appointment, especially if you smoke. The infection can still be in your lungs even if you’re no longer experiencing symptoms.
Your doctor will probably arrange another follow-up appointment for you about six weeks after you start your course of antibiotics.
In some cases, they may arrange follow-up tests, such as a chest X-ray, if:
- your symptoms haven’t improved
- your symptoms have come back
- you smoke
- you’re over the age of 50
Some people may be advised to have a flu vaccination or pneumococcal vaccination after recovering from pneumonia.
Aspiration pneumonia
If you’ve breathed in an object that’s causing pneumonia, it may need to be removed.
To do this, an instrument called a bronchoscope may be used to look into your airways and lungs so that the object can be located and removed. This procedure is known as a bronchoscopy.
Treatment in hospital
You may need treatment in hospital if your symptoms are severe. You’ll be given antibiotics and fluids intravenously through a drip, and you may need oxygen to help breathing.
In very serious cases of pneumonia, breathing assistance through a ventilator in an intensive care unit (ICU) may be required.
You may need to be hospitalized if:
- You are older than age 65
- You are confused about time, people or places
- Your kidney function has declined
- Your systolic blood pressure is below 90 millimeters of mercury (mm Hg) or your diastolic blood pressure is 60 mm Hg or below
- Your breathing is rapid (30 breaths or more a minute)
- You need breathing assistance
- Your temperature is below normal
- Your heart rate is below 50 or above 100
You may be admitted to the intensive care unit if you need to be placed on a breathing machine (ventilator) or if your symptoms are severe.
Children may be hospitalized if:
- They are younger than age 2 months
- They are lethargic or excessively sleepy
- They have trouble breathing
- They have low blood oxygen levels
- They appear dehydrated.
Pneumonia prognosis
Pneumonia prognosis depends on many factors, including age, comorbidities, and hospital setting (inpatient or outpatient). Generally, pneumonia prognosis is promising in otherwise healthy patients. Patients older than 60 years or younger than 4 years of age have a relatively poorer prognosis than young adults. If pneumonia is left untreated, the overall mortality may become 30%. Antibiotic resistance is very concerning due to the excessive and unjustified use of antibiotics. The Pneumonia Severity Index (PSI) may be utilized as a tool to establish a patient’s risk of mortality.
In a study conducted on causes of community-acquired pneumonia, Streptococcus pneumoniae (pneumococcus) was found to be the cause of mortality in most patients; however, Pseudomonas, Staphylococcus aureus, and mixed causes had the highest mortality rates in those affected 96.
Recovering from pneumonia
It may take time to recover from pneumonia. Some people feel better and are able to return to their normal routines within a week. For other people, it can take a month or more. Most people continue to feel tired for about a month. Adequate rest is important to maintain progress toward full recovery and to avoid relapse. Don’t rush your recovery! Talk with your doctor about when you can go back to your normal routine.
While you are recovering, try to limit your contact with family and friends, to help keep your germs from spreading to other people. Cover your mouth and nose when you cough, promptly dispose of tissues in a closed waste container and wash your hands often.
If you have taken antibiotics, your doctor will want to make sure your chest X-ray is normal again after you finish the whole prescription. It may take many weeks for your X-ray to clear up.
Possible pneumonia complications
People who may be more likely to have complications from pneumonia include:
- Older adults or very young children.
- People whose immune system does not work well.
- People with other, serious medical problems such as diabetes or cirrhosis of the liver.
Possible complications include:
- Respiratory failure, which requires a breathing machine or ventilator.
- Sepsis, a condition in which there is uncontrolled inflammation in the body, which may lead to widespread organ failure.
- Acute respiratory distress syndrome (ARDS), a severe form of respiratory failure.
- Lung abscesses, which are infrequent, but serious complications of pneumonia. They occur when pockets of pus form inside or around the lung. These may sometimes need to be drained with surgery.
- Metlay JP, Kapoor WN, Fine MJ. Does This Patient Have Community-Acquired Pneumonia? Diagnosing Pneumonia by History and Physical Examination. JAMA. 1997;278(17):1440–1445. doi:10.1001/jama.1997.03550170070035
- Loeb M. Community‐acquired pneumonia. Clinical Evidence. Vol. 8, London: BMJ Publishing Group, 2002.
- Welte T, Torres A, Nathwani D. Clinical and economic burden of community-acquired pneumonia among adults in Europe. Thorax. 2012 Jan;67(1):71-9. doi: 10.1136/thx.2009.129502
- Sattar SBA, Sharma S. Bacterial Pneumonia. [Updated 2021 Dec 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK513321
- Kung HC, Hoyert DL, Xu J, Murphy SL. Deaths: final data for 2005. Natl Vital Stat Rep. 2008 Apr 24;56(10):1-120. https://www.cdc.gov/nchs/data/nvsr/nvsr56/nvsr56_10.pdf
- Lat I, Daley MJ, Shewale A, Pangrazzi MH, Hammond D, Olsen KM; DEFINE study group and the Discovery Research Network. A Multicenter, Prospective, Observational Study to Determine Predictive Factors for Multidrug-Resistant Pneumonia in Critically Ill Adults: The DEFINE Study. Pharmacotherapy. 2019 Mar;39(3):253-260. doi: 10.1002/phar.2171
- Shin, E. J., Kim, Y., Jeong, J. Y., Jung, Y. M., Lee, M. H., & Chung, E. H. (2018). The changes of prevalence and etiology of pediatric pneumonia from National Emergency Department Information System in Korea, between 2007 and 2014. Korean journal of pediatrics, 61(9), 291–300. https://doi.org/10.3345/kjp.2017.06100
- Metlay, J. P., Waterer, G. W., Long, A. C., et al. (2019). Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. American journal of respiratory and critical care medicine, 200(7), e45–e67. https://doi.org/10.1164/rccm.201908-1581ST
- Fine MJ, Auble TE, Yealy DM, Hanusa BH, Weissfeld LA, Singer DE, Coley CM, Marrie TJ, Kapoor WN. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med. 1997 Jan 23;336(4):243–250. DOI: 10.1056/NEJM199701233360402
- Mandell, L. A., Bartlett, J. G., Dowell, S. F., File, T. M., Jr, Musher, D. M., Whitney, C., & Infectious Diseases Society of America (2003). Update of practice guidelines for the management of community-acquired pneumonia in immunocompetent adults. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 37(11), 1405–1433. https://doi.org/10.1086/380488
- Fine MJ, Hough LJ, Medsger AR, Li YH, Ricci EM, Singer DE, Marrie TJ, Coley CM, Walsh MB, Karpf M, Lahive KC, Kapoor WN. The hospital admission decision for patients with community-acquired pneumonia. Results from the pneumonia Patient Outcomes Research Team cohort study. Arch Intern Med. 1997 Jan 13;157(1):36-44.
- Mark Williams; Scott A. Flanders; Winthrop F. Whitcomb (28 September 2007). Comprehensive hospital medicine: an evidence based approach. Elsevier Health Sciences. pp. 273–. ISBN 978-1-4160-0223-9
- Capelastegui A, España PP, Quintana JM, Areitio I, Gorordo I, Egurrola M, Bilbao A. Validation of a predictive rule for the management of community-acquired pneumonia. Eur Respir J. 2006;27:151–157.
- Chalmers JD, Singanayagam A, Akram AR, et al. (October 2010). “Severity assessment tools for predicting mortality in hospitalised patients with community-acquired pneumonia. Systematic review and meta-analysis”. Thorax. 65 (10): 878–83. doi:10.1136/thx.2009.133280
- Lim WS, van der Eerden MM, Laing R, Boersma WG, Karalus N, Town GI, Lewis SA, Macfarlane JT. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax. 2003;58:377–382.
- Mandell LA, Marrie TJ, Grossman RF, Chow AW, Hyland RH. Canadian guidelines for the initial management of community-acquired pneumonia: an evidence-based update by the Canadian Infectious Diseases Society and the Canadian Thoracic Society. The Canadian Community-Acquired Pneumonia Working Group. Clin Infect Dis. 2000 Aug;31(2):383-421. doi: 10.1086/313959
- Mandell, L. A., Wunderink, R. G., Anzueto, A., Bartlett, J. G., Campbell, G. D., Dean, N. C., Dowell, S. F., File, T. M., Jr, Musher, D. M., Niederman, M. S., Torres, A., Whitney, C. G., Infectious Diseases Society of America, & American Thoracic Society (2007). Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 44 Suppl 2(Suppl 2), S27–S72. https://doi.org/10.1086/511159
- Pakhale, S., Mulpuru, S., Verheij, T. J., Kochen, M. M., Rohde, G. G., & Bjerre, L. M. (2014). Antibiotics for community-acquired pneumonia in adult outpatients. The Cochrane database of systematic reviews, 2014(10), CD002109. https://doi.org/10.1002/14651858.CD002109.pub4
- Common Questions About Pneumonia in Nursing Home Residents. Am Fam Physician. 2015 Oct 1;92(7):612-620. https://www.aafp.org/afp/2015/1001/p612.html
- Lee JS, Giesler DL, Gellad WF, Fine MJ. Antibiotic Therapy for Adults Hospitalized With Community-Acquired Pneumonia: A Systematic Review. JAMA. 2016 Feb 9;315(6):593-602. doi: 10.1001/jama.2016.0115
- Pneumonia (community-acquired): antimicrobial prescribing. https://www.nice.org.uk/guidance/ng138/chapter/Recommendations
- Lim, W. S., Smith, D. L., Wise, M. P., & Welham, S. A. (2015). British Thoracic Society community acquired pneumonia guideline and the NICE pneumonia guideline: how they fit together. BMJ open respiratory research, 2(1), e000091. https://doi.org/10.1136/bmjresp-2015-000091
- Wan YD, Sun TW, Liu ZQ, Zhang SG, Wang LX, Kan QC. Efficacy and Safety of Corticosteroids for Community-Acquired Pneumonia: A Systematic Review and Meta-Analysis. Chest. 2016 Jan;149(1):209-19. doi: 10.1378/chest.15-1733
- Siemieniuk RA, Meade MO, Alonso-Coello P, Briel M, Evaniew N, Prasad M, Alexander PE, Fei Y, Vandvik PO, Loeb M, Guyatt GH. Corticosteroid Therapy for Patients Hospitalized With Community-Acquired Pneumonia: A Systematic Review and Meta-analysis. Ann Intern Med. 2015 Oct 6;163(7):519-28. doi: 10.7326/M15-0715
- Torres A, Sibila O, Ferrer M, Polverino E, Menendez R, Mensa J, Gabarrús A, Sellarés J, Restrepo MI, Anzueto A, Niederman MS, Agustí C. Effect of corticosteroids on treatment failure among hospitalized patients with severe community-acquired pneumonia and high inflammatory response: a randomized clinical trial. JAMA. 2015 Feb 17;313(7):677-86. doi: 10.1001/jama.2015.88
- Calik, S., Ari, A., Bilgir, O., Cetintepe, T., Yis, R., Sonmez, U., & Tosun, S. (2018). The relationship between mortality and microbiological parameters in febrile neutropenic patients with hematological malignancies. Saudi medical journal, 39(9), 878–885. https://doi.org/10.15537/smj.2018.9.22824
- Freeman AM, Leigh, Jr TR. Viral Pneumonia. [Updated 2021 Jul 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK513286
- Viral Pneumonia Treatment & Management. https://emedicine.medscape.com/article/300455-treatment
- Murdoch, D. R., & Chambers, S. T. (2009). Atypical pneumonia–time to breathe new life into a useful term?. The Lancet. Infectious diseases, 9(8), 512–519. https://doi.org/10.1016/S1473-3099(09)70148-3
- Rhim, J. W., Kang, H. M., Yang, E. A., & Lee, K. Y. (2019). Epidemiological relationship between Mycoplasma pneumoniae pneumonia and recurrent wheezing episode in children: an observational study at a single hospital in Korea. BMJ open, 9(4), e026461. https://doi.org/10.1136/bmjopen-2018-026461
- Beeton, Michael L et al. “Mycoplasma pneumoniae infections, 11 countries in Europe and Israel, 2011 to 2016.” Euro surveillance : bulletin Europeen sur les maladies transmissibles = European communicable disease bulletin vol. 25,2 (2020): 1900112. https://doi.org/10.2807/1560-7917.ES.2020.25.2.1900112
- Dumke R, Strubel A, Cyncynatus C, Nuyttens H, Herrmann R, Lück C, Jacobs E. Optimized serodiagnosis of Mycoplasma pneumoniae infections. Diagn Microbiol Infect Dis. 2012 Jun;73(2):200-3. doi: 10.1016/j.diagmicrobio.2012.02.014
- Zhang, X. S., Zhao, H., Vynnycky, E., & Chalker, V. (2019). Positively interacting strains that co-circulate within a network structured population induce cycling epidemics of Mycoplasma pneumoniae. Scientific reports, 9(1), 541. https://doi.org/10.1038/s41598-018-36325-z
- Sánchez-Vargas FM, Gómez-Duarte OG. Mycoplasma pneumoniae-an emerging extra-pulmonary pathogen. Clin Microbiol Infect. 2008 Feb;14(2):105-17. doi: 10.1111/j.1469-0691.2007.01834.x
- Abdulhadi B, Kiel J. Mycoplasma Pneumonia. [Updated 2022 Jan 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430780
- Liu, J., & Li, Y. (2021). Thrombosis associated with mycoplasma pneumoniae infection (Review). Experimental and therapeutic medicine, 22(3), 967. https://doi.org/10.3892/etm.2021.10399
- Bajantri, B., Venkatram, S., & Diaz-Fuentes, G. (2018). Mycoplasma pneumoniae: A Potentially Severe Infection. Journal of clinical medicine research, 10(7), 535–544. https://doi.org/10.14740/jocmr3421w
- Wen, Z., Wei, J., Xue, H., Chen, Y., Melnick, D., Gonzalez, J., Hackett, J., Li, X., & Cao, Z. (2018). Epidemiology, microbiology, and treatment patterns of pediatric patients hospitalized with pneumonia at two hospitals in China: a patient chart review study. Therapeutics and clinical risk management, 14, 501–510. https://doi.org/10.2147/TCRM.S143266
- Brady MF, Sundareshan V. Legionnaires’ Disease. [Updated 2021 Jul 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430807
- Legionnaires Disease. https://emedicine.medscape.com/article/220163-overview
- Legionella (Legionnaires’ Disease and Pontiac Fever). https://www.cdc.gov/legionella/about/signs-symptoms.html
- Correia AM, GonCalves J, Gomes, JP, et al. Probable Person-to-Person Transmission of Legionnaires’ Disease. N Engl J Med. 2016;374:497–8. DOI: 10.1056/NEJMc1505356
- Legionnaires Disease Workup. https://emedicine.medscape.com/article/220163-workup#c5
- Active Bacterial Core Surveillance for Legionellosis — United States, 2011–2013. https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6442a2.htm
- Soda EA, Barskey AE, Shah PP, et al. Vital Signs: Health Care–Associated Legionnaires’ Disease Surveillance Data from 20 States and a Large Metropolitan Area — United States, 2015. MMWR Morb Mortal Wkly Rep 2017;66:584–589. DOI: http://dx.doi.org/10.15585/mmwr.mm6622e1
- Kuo, C. C., Jackson, L. A., Campbell, L. A., & Grayston, J. T. (1995). Chlamydia pneumoniae (TWAR). Clinical microbiology reviews, 8(4), 451–461. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC172870/pdf/080451.pdf
- Hahn DL, Azenabor AA, Beatty WL, Byrne GI. Chlamydia pneumoniae as a respiratory pathogen. Front Biosci. 2002 Mar 1;7:e66-76. doi: 10.2741/hahn
- Porritt, R. A., & Crother, T. R. (2016). Chlamydia pneumoniae Infection and Inflammatory Diseases. Forum on immunopathological diseases and therapeutics, 7(3-4), 237–254. https://doi.org/10.1615/ForumImmunDisTher.2017020161
- Gautam J, Krawiec C. Chlamydia Pneumonia. [Updated 2021 Aug 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560874
- Kuo, C. C., Jackson, L. A., Campbell, L. A., & Grayston, J. T. (1995). Chlamydia pneumoniae (TWAR). Clinical microbiology reviews, 8(4), 451–461. https://doi.org/10.1128/CMR.8.4.451
- Theunissen, H. J., Lemmens-den Toom, N. A., Burggraaf, A., Stolz, E., & Michel, M. F. (1993). Influence of temperature and relative humidity on the survival of Chlamydia pneumoniae in aerosols. Applied and environmental microbiology, 59(8), 2589–2593. https://doi.org/10.1128/aem.59.8.2589-2593.1993
- Cunha B. A. (2006). The atypical pneumonias: clinical diagnosis and importance. Clinical microbiology and infection : the official publication of the European Society of Clinical Microbiology and Infectious Diseases, 12 Suppl 3, 12–24. https://doi.org/10.1111/j.1469-0691.2006.01393.x
- Blasi F, Tarsia P, Arosio C, Fagetti L, Allegra L. Epidemiology of Chlamydia pneumoniae. Clin Microbiol Infect. 1998 Jan;4 Suppl 4:S1-S6.
- Hogerwerf L, DE Gier B, Baan B, VAN DER Hoek W. Chlamydia psittaci (psittacosis) as a cause of community-acquired pneumonia: a systematic review and meta-analysis. Epidemiol Infect. 2017 Nov;145(15):3096-3105. doi: 10.1017/S0950268817002060
- Psittacosis Signs and Symptoms. https://www.cdc.gov/pneumonia/atypical/psittacosis/about/signs-symptoms.html
- Soni R., Seale J.P., Young I.H. Fulminant psittacosis requiring mechanical ventilation and demonstrating serological cross-reactivity between Legionella longbeachae and Chlamydia psittaci. Respirology. 1999;4(2):203–205. doi: 10.1046/j.1440-1843.1999.00176.x
- Lynch JP 3rd, Zhanel GG. Streptococcus pneumoniae: epidemiology, risk factors, and strategies for prevention. Semin Respir Crit Care Med. 2009 Apr;30(2):189-209. doi: 10.1055/s-0029-1202938
- Kim, L., McGee, L., Tomczyk, S., & Beall, B. (2016). Biological and Epidemiological Features of Antibiotic-Resistant Streptococcus pneumoniae in Pre- and Post-Conjugate Vaccine Eras: a United States Perspective. Clinical microbiology reviews, 29(3), 525–552. https://doi.org/10.1128/CMR.00058-15
- Magill, S. S., Edwards, J. R., Bamberg, W., Beldavs, Z. G., Dumyati, G., Kainer, M. A., Lynfield, R., Maloney, M., McAllister-Hollod, L., Nadle, J., Ray, S. M., Thompson, D. L., Wilson, L. E., Fridkin, S. K., & Emerging Infections Program Healthcare-Associated Infections and Antimicrobial Use Prevalence Survey Team (2014). Multistate point-prevalence survey of health care-associated infections. The New England journal of medicine, 370(13), 1198–1208. https://doi.org/10.1056/NEJMoa1306801
- Klebsiella pneumoniae in Healthcare Settings. https://www.cdc.gov/hai/organisms/klebsiella/klebsiella.html
- Podschun, R., & Ullmann, U. (1998). Klebsiella spp. as nosocomial pathogens: epidemiology, taxonomy, typing methods, and pathogenicity factors. Clinical microbiology reviews, 11(4), 589–603. https://doi.org/10.1128/CMR.11.4.589
- Ashurst JV, Dawson A. Klebsiella Pneumonia. [Updated 2022 Feb 2]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK519004
- Kalanuria, A. A., Ziai, W., & Mirski, M. (2014). Ventilator-associated pneumonia in the ICU. Critical care (London, England), 18(2), 208. https://doi.org/10.1186/cc13775
- Richards MJ, Edwards JR, Culver DH, Gaynes RP. Nosocomial infections in combined medical-surgical intensive care units in the United States. Infect Control Hosp Epidemiol. 2000 Aug;21(8):510-5. doi: 10.1086/501795
- Kang, C. I., Kim, S. H., Bang, J. W., Kim, H. B., Kim, N. J., Kim, E. C., Oh, M. D., & Choe, K. W. (2006). Community-acquired versus nosocomial Klebsiella pneumoniae bacteremia: clinical features, treatment outcomes, and clinical implication of antimicrobial resistance. Journal of Korean medical science, 21(5), 816–822. https://doi.org/10.3346/jkms.2006.21.5.816
- Montgomerie JZ, Ota JK. Klebsiella bacteremia. Arch Intern Med. 1980 Apr;140(4):525-7.
- Meatherall BL, Gregson D, Ross T, Pitout JD, Laupland KB. Incidence, risk factors, and outcomes of Klebsiella pneumoniae bacteremia. Am J Med. 2009 Sep;122(9):866-73. doi: 10.1016/j.amjmed.2009.03.034
- Lye WC, Chan RK, Lee EJ, Kumarasinghe G. Urinary tract infections in patients with diabetes mellitus. J Infect. 1992 Mar;24(2):169-74. doi: 10.1016/0163-4453(92)92876-k
- Schroll, C., Barken, K. B., Krogfelt, K. A., & Struve, C. (2010). Role of type 1 and type 3 fimbriae in Klebsiella pneumoniae biofilm formation. BMC microbiology, 10, 179. https://doi.org/10.1186/1471-2180-10-179
- Liu, C., & Guo, J. (2018). Characteristics of ventilator-associated pneumonia due to hypervirulent Klebsiella pneumoniae genotype in genetic background for the elderly in two tertiary hospitals in China. Antimicrobial resistance and infection control, 7, 95. https://doi.org/10.1186/s13756-018-0371-8
- Pneumocystis pneumonia. https://www.cdc.gov/fungal/diseases/pneumocystis-pneumonia
- Harris, J.R., Balajee, S.A. & Park, B.J. Pneumocystis Jirovecii Pneumonia: Current Knowledge and Outstanding Public Health Issues. Curr Fungal Infect Rep 4, 229–237 (2010). https://doi.org/10.1007/s12281-010-0029-3
- Edman JC, Kovacs JA, Masur H, Santi DV, Elwood HJ, Sogin ML. Ribosomal RNA sequence shows Pneumocystis carinii to be a member of the fungi. Nature. 1988 Aug 11;334(6182):519-22. doi: 10.1038/334519a0
- Stringer, J. R., Beard, C. B., Miller, R. F., & Wakefield, A. E. (2002). A new name (Pneumocystis jiroveci) for Pneumocystis from humans. Emerging infectious diseases, 8(9), 891–896. https://doi.org/10.3201/eid0809.020096
- Medrano, F. J., Montes-Cano, M., Conde, M., de la Horra, C., Respaldiza, N., Gasch, A., Perez-Lozano, M. J., Varela, J. M., & Calderon, E. J. (2005). Pneumocystis jirovecii in general population. Emerging infectious diseases, 11(2), 245–250. https://doi.org/10.3201/eid1102.040487
- Jeremy A W Gold, Brendan R Jackson, Kaitlin Benedict, Possible Diagnostic Delays and Missed Prevention Opportunities in Pneumocystis Pneumonia Patients Without HIV: Analysis of Commercial Insurance Claims Data—United States, 2011–2015, Open Forum Infectious Diseases, Volume 7, Issue 7, July 2020, ofaa255, https://doi.org/10.1093/ofid/ofaa255
- Roux, A., Canet, E., Valade, S., Gangneux-Robert, F., Hamane, S., Lafabrie, A., Maubon, D., Debourgogne, A., Le Gal, S., Dalle, F., Leterrier, M., Toubas, D., Pomares, C., Bellanger, A. P., Bonhomme, J., Berry, A., Durand-Joly, I., Magne, D., Pons, D., Hennequin, C., … Azoulay, É. (2014). Pneumocystis jirovecii pneumonia in patients with or without AIDS, France. Emerging infectious diseases, 20(9), 1490–1497. https://doi.org/10.3201/eid2009.131668
- Gianella S, Haeberli L, Joos B, Ledergerber B, Wüthrich RP, Weber R, Kuster H, Hauser PM, Fehr T, Mueller NJ. Molecular evidence of interhuman transmission in an outbreak of Pneumocystis jirovecii pneumonia among renal transplant recipients. Transpl Infect Dis. 2010 Feb;12(1):1-10. doi: 10.1111/j.1399-3062.2009.00447.x
- A Cluster of Pneumocystis jirovecii Infection Among Outpatients with Rheumatoid Arthritis. The Journal of Rheumatology Jul 2010, 37 (7) 1547-1548; DOI: 10.3899/jrheum.091294
- Pifer LL, Hughes WT, Stagno S, Woods D. Pneumocystis carinii infection: evidence for high prevalence in normal and immunosuppressed children. Pediatrics. 1978 Jan;61(1):35-41.
- Wakefield AE, Lindley AR, Ambrose HE, Denis CM, Miller RF. Limited asymptomatic carriage of Pneumocystis jiroveci in human immunodeficiency virus-infected patients. J Infect Dis. 2003 Mar 15;187(6):901-8. doi: 10.1086/368165
- Kovacs JA, Hiemenz JW, Macher AM, Stover D, Murray HW, Shelhamer J, Lane HC, Urmacher C, Honig C, Longo DL, et al. Pneumocystis carinii pneumonia: a comparison between patients with the acquired immunodeficiency syndrome and patients with other immunodeficiencies. Ann Intern Med. 1984 May;100(5):663-71. doi: 10.7326/0003-4819-100-5-663
- Accuracy of β-D-glucan for the diagnosis of Pneumocystis jirovecii pneumonia: a meta-analysis. Karageorgopoulos, D.E. et al. Clinical Microbiology and Infection, Volume 19, Issue 1, 39 – 49. https://doi.org/10.1111/j.1469-0691.2011.03760.x
- Truong J, Ashurst JV. Pneumocystis Jirovecii Pneumonia. [Updated 2022 Feb 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482370
- Newberry L, O’Hare B, Kennedy N, Selman A, Omar S, Dawson P, Stevenson K, Nishihara Y, Lissauer S, Molyneux E. Early use of corticosteroids in infants with a clinical diagnosis of Pneumocystis jiroveci pneumonia in Malawi: a double-blind, randomised clinical trial. Paediatr Int Child Health. 2017 May;37(2):121-128. doi: 10.1080/20469047.2016.1260891
- Fungal Pneumonia. https://emedicine.medscape.com/article/300341-overview
- Lamoth F, Alexander BD. Nonmolecular methods for the diagnosis of respiratory fungal infections. Clin Lab Med. 2014 Jun;34(2):315-36. doi: 10.1016/j.cll.2014.02.006
- Limper AH. The changing spectrum of fungal infections in pulmonary and critical care practice: clinical approach to diagnosis. Proc Am Thorac Soc. 2010 May;7(3):163-8. doi: 10.1513/pats.200906-049AL
- Chen TC, Ho MW, Chien WC, Lin HH. Disseminated Scedosporium apiospermum infection in a near-drowning patient. J Formos Med Assoc. 2016 Mar;115(3):213-4. doi: 10.1016/j.jfma.2015.02.007
- Garzoni, C., Emonet, S., Legout, L., Benedict, R., Hoffmeyer, P., Bernard, L., & Garbino, J. (2005). Atypical infections in tsunami survivors. Emerging infectious diseases, 11(10), 1591–1593. https://doi.org/10.3201/eid1110.050715
- Fungal Pneumonia. https://emedicine.medscape.com/article/300341-overview#a5
- White, P. L., Archer, A. E., & Barnes, R. A. (2005). Comparison of non-culture-based methods for detection of systemic fungal infections, with an emphasis on invasive Candida infections. Journal of clinical microbiology, 43(5), 2181–2187. https://doi.org/10.1128/JCM.43.5.2181-2187.2005
- Lass-Flörl C, Gunsilius E, Gastl G, Freund M, Dierich MP, Petzer A. Clinical evaluation of Aspergillus-PCR for detection of invasive aspergillosis in immunosuppressed patients. Mycoses. 2005;48 Suppl 1:12-7. doi: 10.1111/j.1439-0507.2005.01104.x
- Smith JA, Kauffman CA. Pulmonary fungal infections. Respirology. 2012 Aug;17(6):913-26. doi: 10.1111/j.1440-1843.2012.02150.x
- Gerber B, Guggenberger R, Fasler D, Nair G, Manz MG, Stussi G, Schanz U. Reversible skeletal disease and high fluoride serum levels in hematologic patients receiving voriconazole. Blood. 2012 Sep 20;120(12):2390-4. doi: 10.1182/blood-2012-01-403030
- Cillóniz C, Ewig S, Polverino E, Marcos MA, Esquinas C, Gabarrús A, Mensa J, Torres A. Microbial aetiology of community-acquired pneumonia and its relation to severity. Thorax. 2011 Apr;66(4):340-6. doi: 10.1136/thx.2010.143982





{kind=link}