Pronation and Supination
Supination and pronation are known primarily as forearm movements, but see also the later discussion of foot movements.
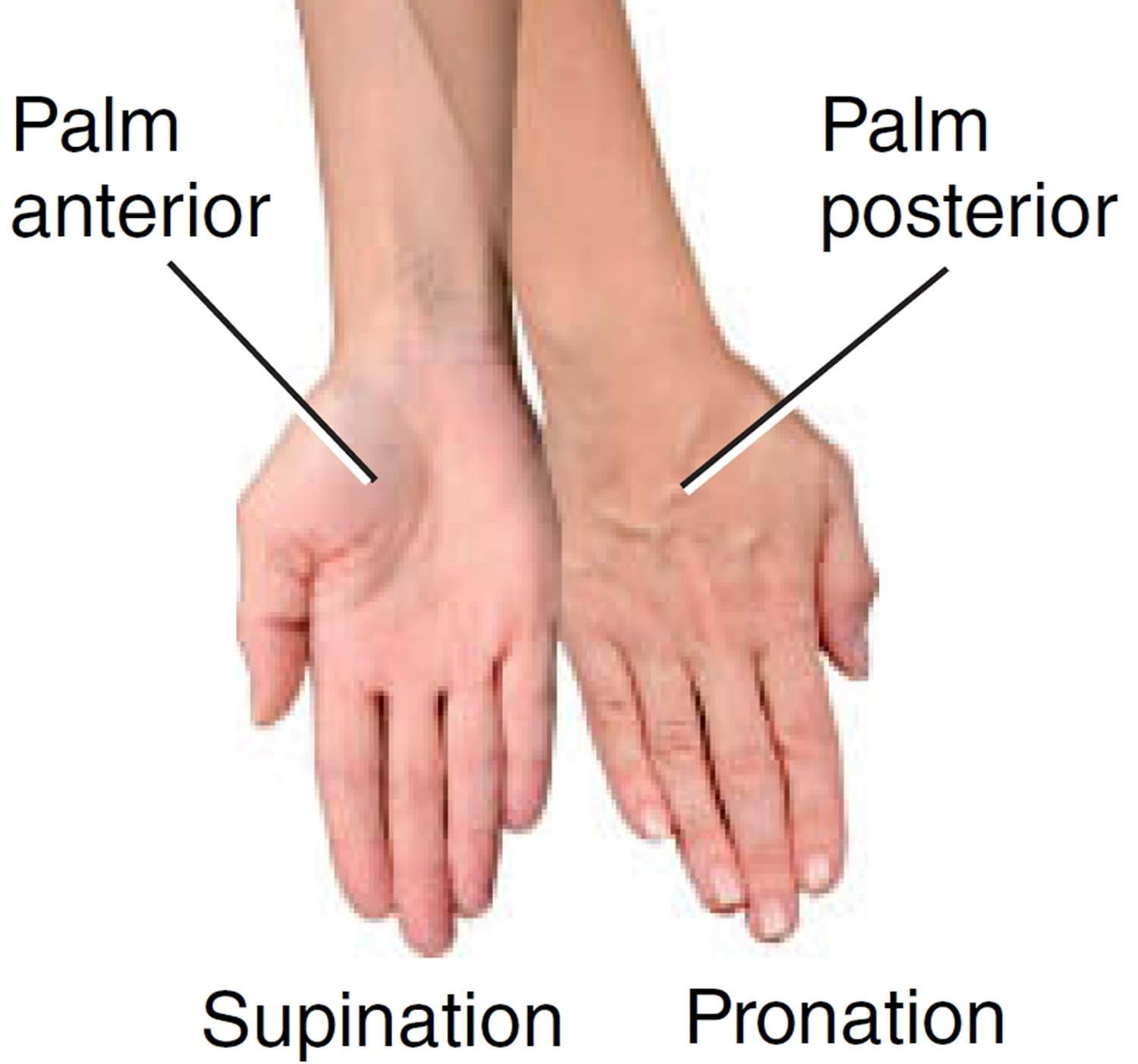
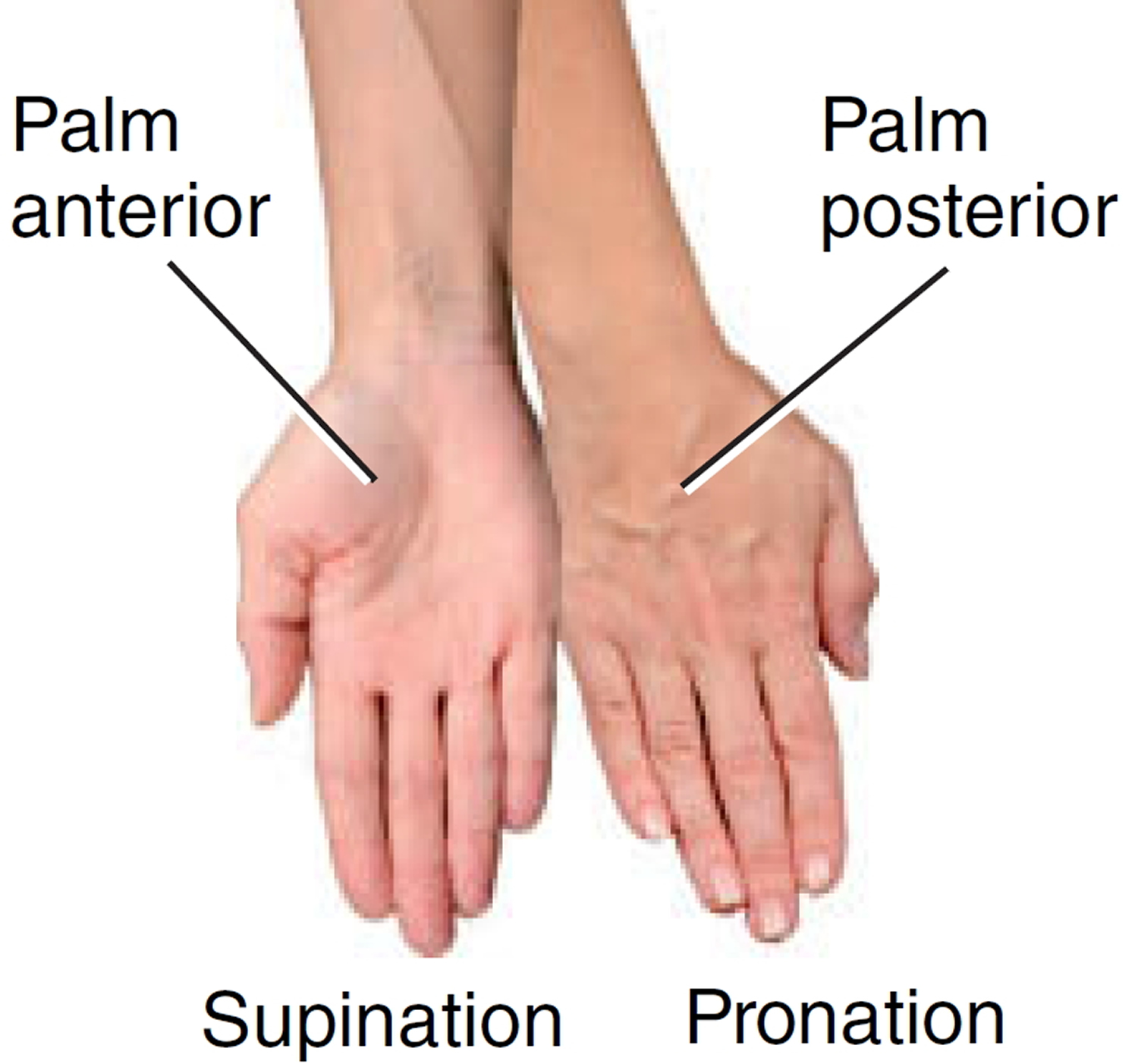
Supination of the forearm is a movement that turns the palm to face anteriorly (in anatomical position) or palm facing up; in anatomical position, the forearm is supinated and the radius is parallel to the ulna.
Pronation is the opposite movement, causing the palm to face posteriorly or palm facing down and the radius to cross the ulna like an X. During these movements, the concave end of the disc-shaped head of the radius spins on the capitulum of the humerus, and the edge of the disc spins in the radial notch of the ulna. The ulna remains relatively stationary.
As an aid to remembering these terms, think of it this way: pronation = palm facing down; supination = palm facing up. You are prone to stand in the most comfortable position, which is with the forearm pronated. But if you were holding a bowl of soup in your palm, you would need to supinate the forearm to keep from spilling it.
The movements of supination and pronation occur through approximately 180° at the radioulnar joints. During pronation the radius rotates across the ulna and twists the forearm and hand so that the palm faces posteriorly. Supination returns the limb to the anatomical position. The axis of the movement passes through the head of the radius and the styloid process of the ulna. Supination is the more powerful movement and is produced by biceps and supinator, although biceps is ineffective when the elbow is fully extended. Pronation is produced by pronator teres and pronator quadratus. Also, when the elbow is flexed, brachioradialis rotates the forearm and returns the limb to the midposition from the extremes of supination or pronation. The head of the radius can be felt rotating about 2 cm distal to the lateral epicondyle during these movements.
Figure 1. Movements of the forearm
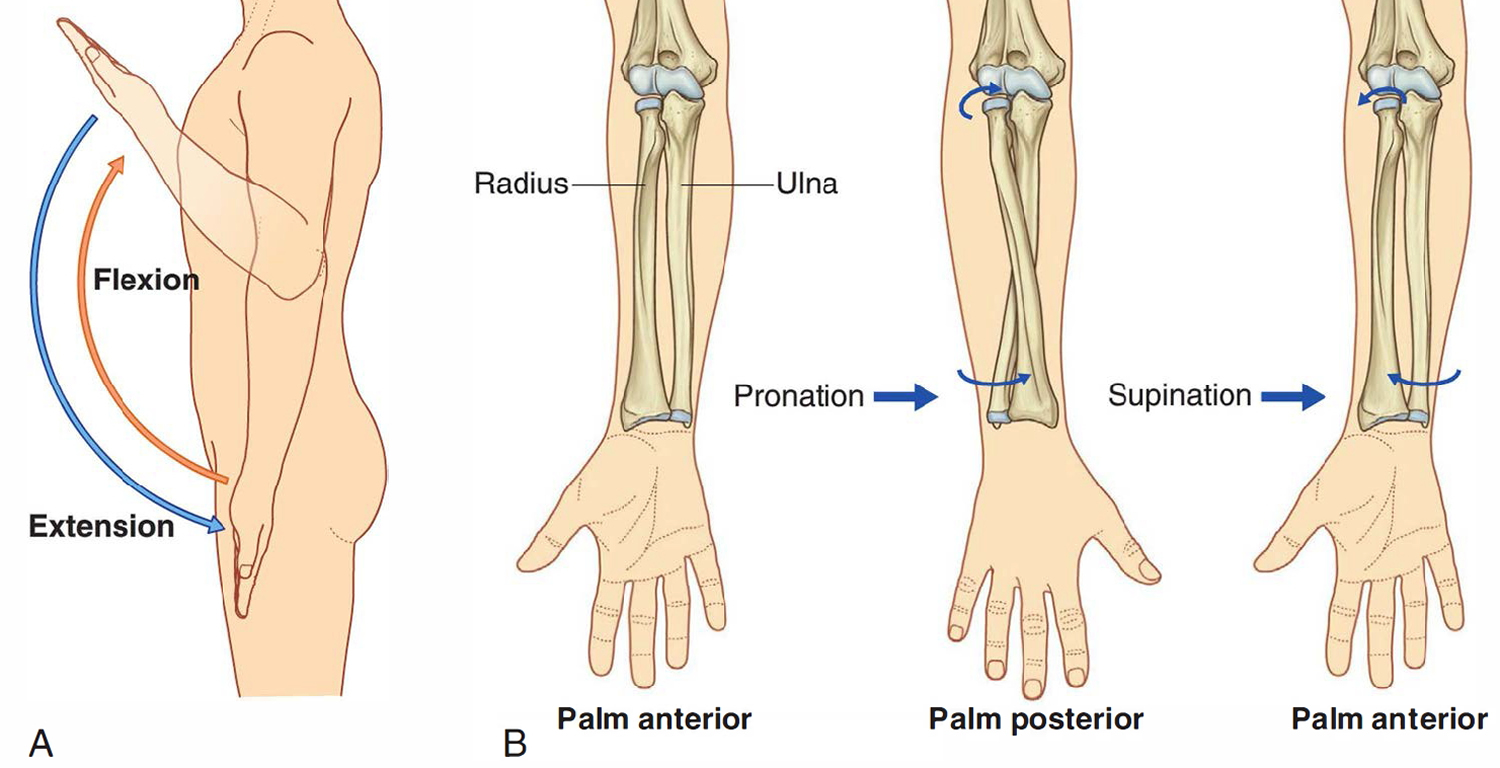
Note: Movements of the forearm. A. Flexion and extension at the elbow joint. B. Pronation and supination.
Figure 2. Supination and pronation of the hand
Supination and pronation of foot
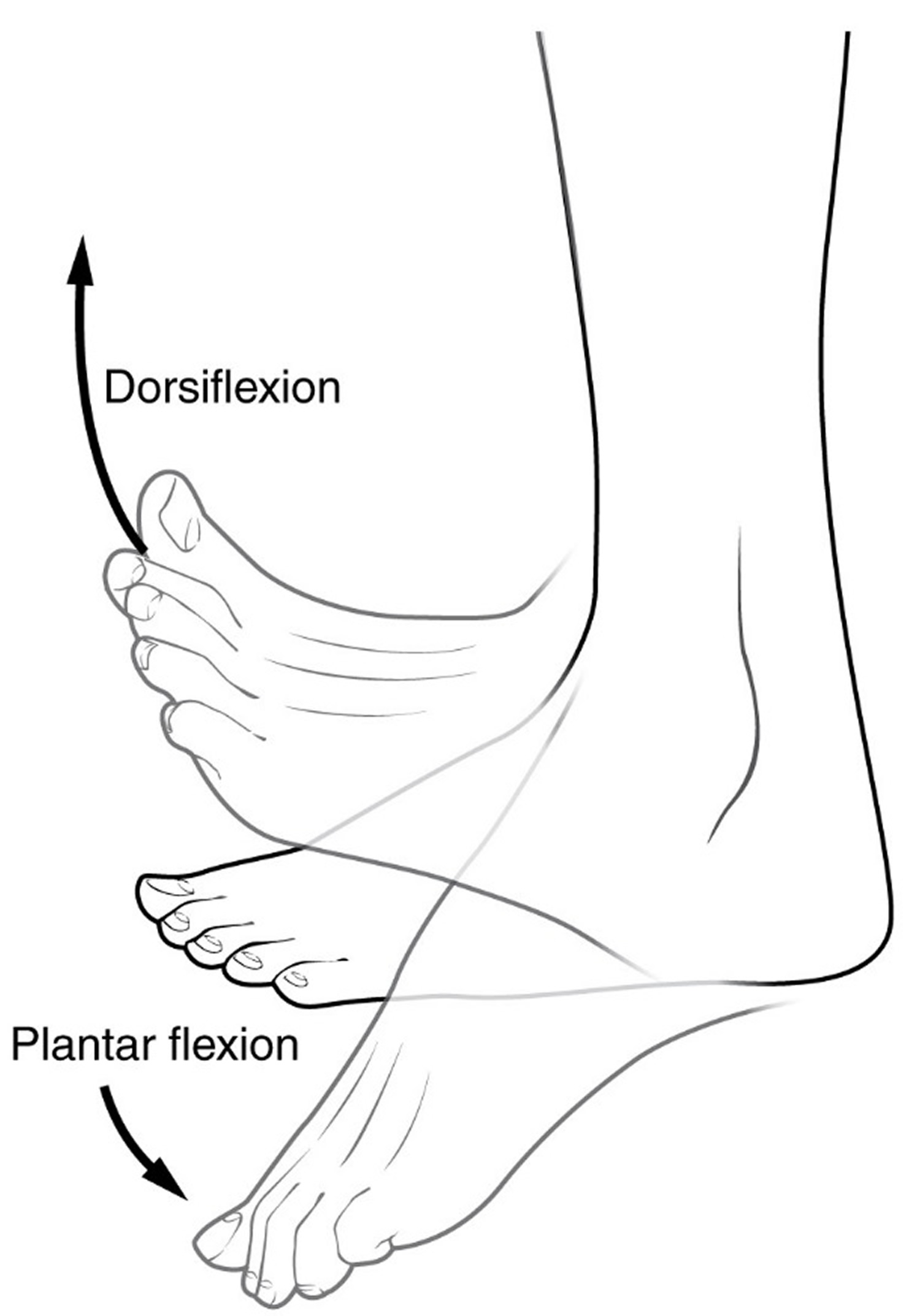
The ankle joint is synovial (a type of joint which is surrounded by a thick flexible membrane forming a sac into which is secreted a viscous fluid that lubricates the joint) in type and involves the talus of the foot and the tibia and fibula of the leg (Figure 3). The ankle joint mainly allows hinge-like dorsiflexion and plantarflexion of the foot on the leg.
Figure 3. Ankle joint
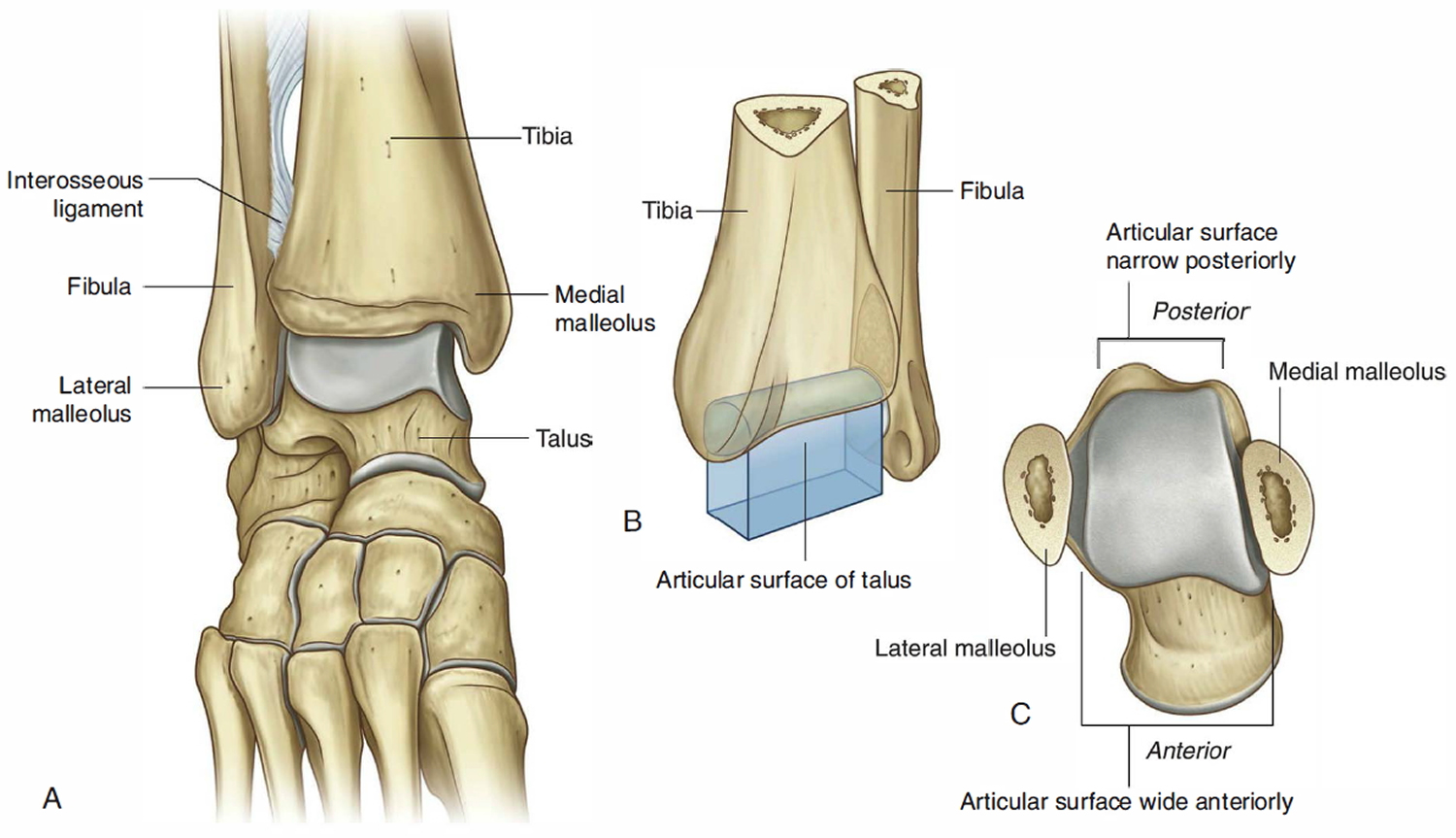
Note: Ankle joint. (A) Anterior view with foot plantarflexed. (B) Schematic of joint. (C) Superior view of the talus to show the shape of the articular surface.
Figure 4. Ankle joint dorsiflexion and plantarflexion
The distal end of the fibula is firmly anchored to the larger distal end of the tibia by strong ligaments. Together, the fibula and tibia create a deep bracket-shaped socket for the upper expanded part of the body of the talus (Figure 3):
- The roof of the socket is formed by the inferior surface of the distal end of the tibia.
- The medial side of the socket is formed by the medial malleolus of the tibia.
- The longer lateral side of the socket is formed by the lateral malleolus of the fibula.
The articular surfaces are covered by hyaline cartilage. The articular part of the talus is shaped like a short half cylinder tipped onto its flat side with one end facing lateral and the other end facing medial. The curved upper surface of the half-cylinder and the two ends are covered by hyaline cartilage and fit into the bracket-shaped socket formed by the distal ends of the tibia and fibula.
When viewed from above, the articular surface of the talus (ankle joint) is much wider anteriorly than it is posteriorly. As a result, the bone fits tighter into its socket when the foot is dorsiflexed and the wider surface of the talus moves into the ankle joint than when the foot is plantarflexed and the narrower part of the talus is in the joint. The joint is therefore most stable when the foot is dorsiflexed.
The articular cavity is enclosed by a synovial membrane, which attaches around the margins of the articular surfaces, and by a fibrous membrane, which covers the synovial membrane and is also attached to the adjacent bones.
The ankle joint is stabilized by medial (deltoid) and lateral ligaments.
Medial ligament (deltoid ligament)
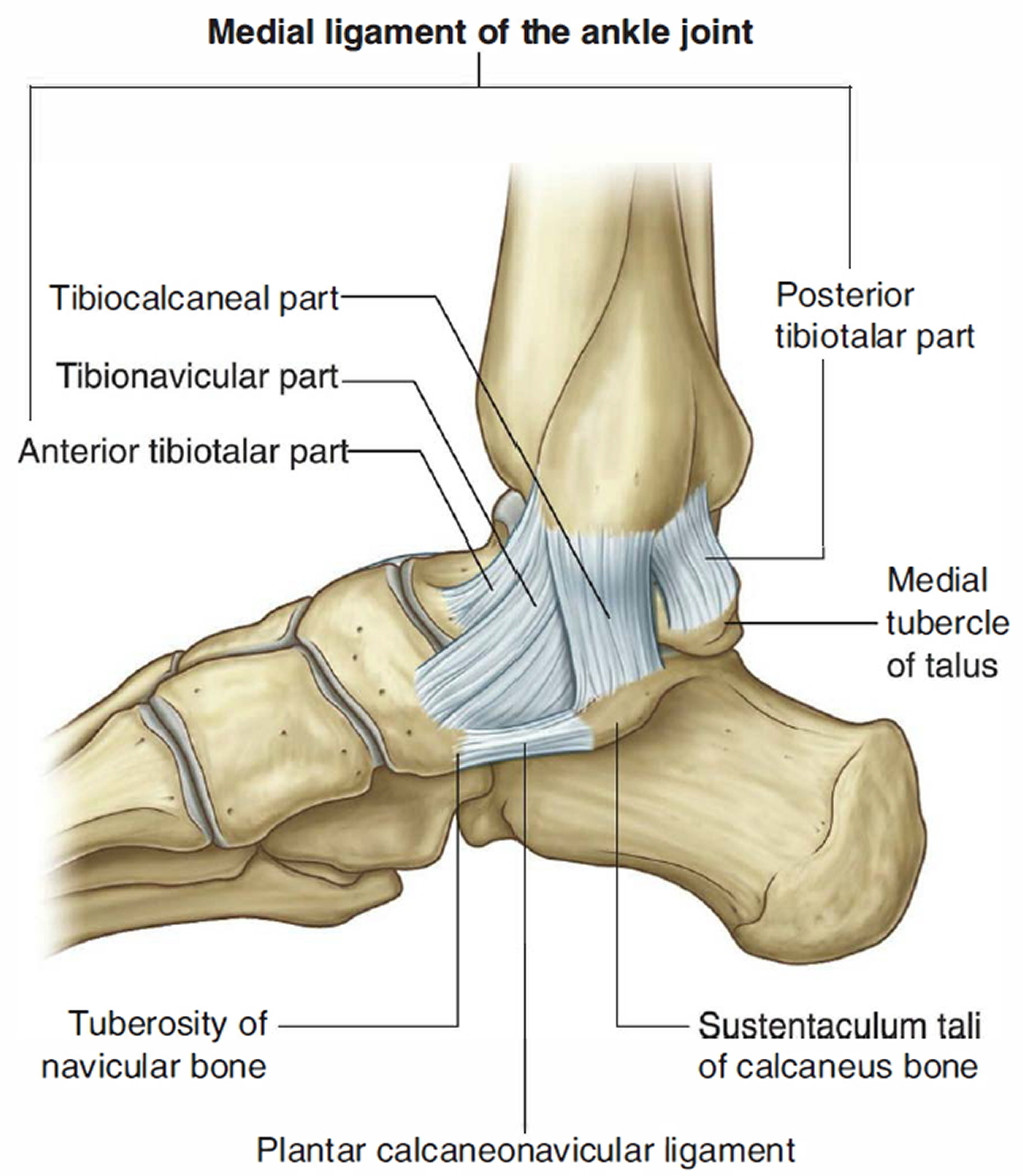
The medial (deltoid) ligament is large, strong (Figure 5) and triangular in shape. Its apex is attached above to the medial malleolus and its broad base is attached below to a line that extends from the tuberosity of the navicular bone in front to the medial tubercle of the talus behind.
The medial ligament is subdivided into four parts based on the inferior points of attachment:
- The part that attaches in front to the tuberosity of the navicular and the associated margin of the plantar calcaneonavicular ligament (spring ligament), which connects the navicular bone to the sustentaculum tali of the calcaneus bone behind, is the tibionavicular part of the medial ligament.
- The tibiocalcaneal part, which is more central, attaches to the sustentaculum tali of the calcaneus bone.
- The posterior tibiotalar part attaches to the medial side and medial tubercle of the talus.
- The fourth part (the anterior tibiotalar part) is deep to the tibionavicular and tibiocalcaneal parts of the medial ligament and attaches to the medial surface of the talus.
Figure 5. Ankle bones and medial ankle ligaments (medial or inner ankle view)
Lateral ankle ligament ligament
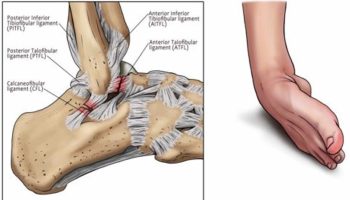
The lateral ligament of the ankle is composed of three separate ligaments , the anterior talofibular ligament, the posterior talofibular ligament, and the calcaneofibular ligament (Figure 6):
- The anterior talofibular ligament is a short ligament and attaches the anterior margin of the lateral malleolus to the adj acent region of the talus.
- The posterior talofibular ligament runs horizontally backward and medially from the malleolar fossa on the medial side of the lateral malleolus to the posterior process of the talus.
- The calcaneofibular ligament is attached above to the malleolar fossa on the posteromedial side of the lateral malleolus and passes posteroinferiorly to attach below to a tubercle on the lateral surface of the calcaneus.
Figure 6. Ankle bones and lateral ankle ligaments (lateral or outer ankle view)

Note: Lateral ligament of the ankle joint. (A) Lateral view. (B) Posterior view.
Intertarsal joints
The numerous synovial joints between the individual tarsal bones mainly invert, evert, supinate, and pronate the foot:
- Inversion and eversion. Inversion is turning the sole of the foot inward. Eversion is turning the whole sole of the foot outward.
- Pronation and supination, while used mainly for forearm movements, also apply to the feet but refer here to a more complex combination of movements. Pronation of the foot is a combination of dorsiflexion, eversion, and abduction—that is, the toes are elevated and turned away from the other foot and the sole is tilted away. Supination of the foot is a combination of plantar flexion, inversion, and adduction—the toes are lowered and turned toward the other foot and the sole is tilted toward it. These may seem a little difficult to visualize and perform, but they are ordinary motions in walking, running, ballet, and crossing uneven surfaces such as stepping stones. Pronation and supination allow the foot to maintain normal contact with the ground when in different stances or when standing on irregular surfaces. You can perhaps understand why these terms apply to the feet if you place the palms of your hands on a table and pretend they are your soles. Tilt your hands so the inner edge (thumb side) of each is raised from the table. This is like raising the medial (inner) edge of your foot from the ground, and as you can see, it involves a slight supination of your forearms. Resting your hands palms down on a table, your forearms are already pronated; but if you raise the outer edges of your hands (the little finger side), like pronating the feet, you will see that it involves a continuation of the pronation movement of the forearm.
Figure 7. Foot inversion and eversion

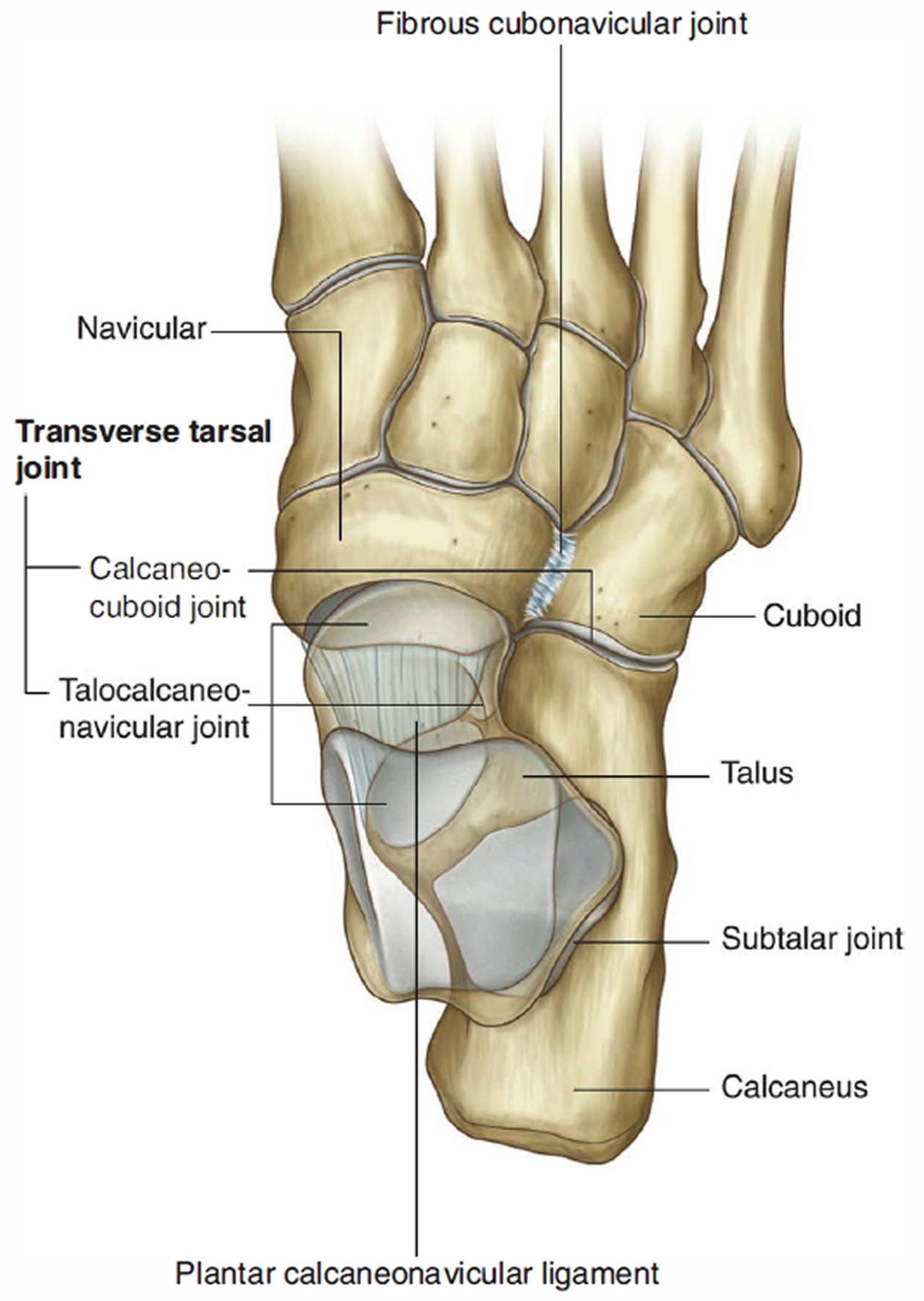
Figure 8. Intertarsal joint




{kind=link}