
What is retinal artery occlusion
Retinal artery occlusion is a blockage in one of the small retinal arteries that carry blood and oxygen to the nerve cells in the retina at the back of your eye. The retina is a layer of tissue in the back of the eye that is able to sense light. The lack of oxygen delivery to the retina may result in severe loss of vision. Most retinal artery occlusion patients are in their 60s, and are more commonly men than women. Only 1% to 2% of cases involve both eyes.
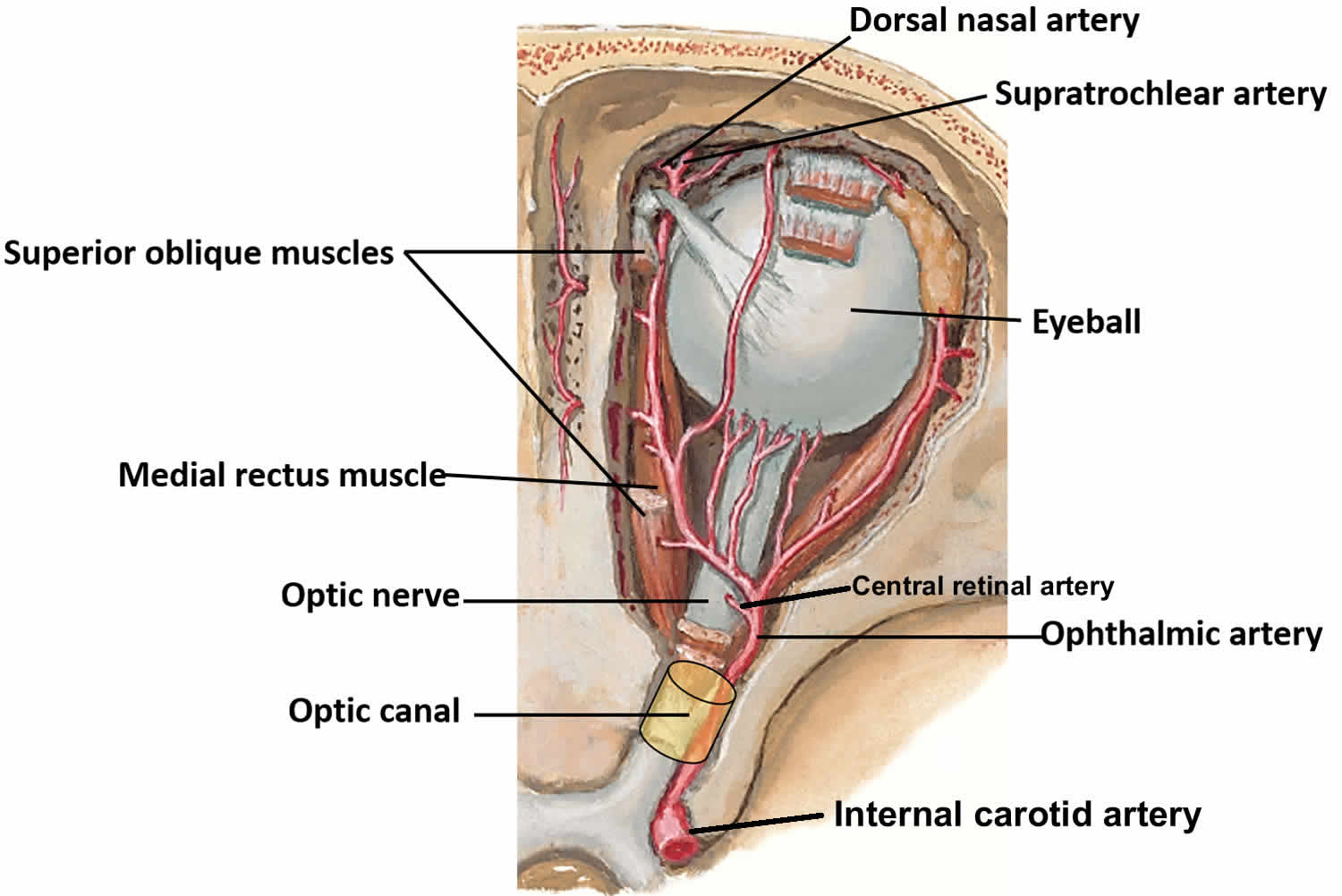
Retinal artery occlusion may occur in any of the vessels supplying the eye. The main artery that supplies the eye and surrounding structures is the ophthalmic artery. The central retinal artery is the first branch of the ophthalmic artery, and it enters the eye through the optic disc and divides into multiple branches to supply nerve fibers in the optic nerve as well as the inner layers of the retina. After entering the eye, the central retinal artery divides into superior and inferior branches. In addition, the cilio-retinal artery is a branch of the short posterior ciliary arteries, which is a separate branch of the ophthalmic artery. Ophthalmic artery artery occlusion results in ischemia of both the inner and outer retina. This results in very severe loss of vision, often resulting in no light perception.
The blood-flow through any of these vessels may be disrupted during a retinal artery occlusion. Blackage may be caused by emboli, vasculitis, or spasms. Occlusion of the ophthalmic artery is often due to giant cell arteritis, while occlusion of the cilioretinal artery may be secondary to a central retinal vein occlusion, due to increased outflow resistance.
Central retinal artery occlusions (CRAOs) account for 58% of acute retinal artery obstructions, branch retinal artery occlusions (BRAOs) account for 38%, and cilioretinal artery occlusions account for 5% 1.
Multiple studies have shown increased mortality in patients with retinal arterial emboli. Increased mortality secondary to fatal stroke has been shown in studies, but the most common cause of death in this population is cardiovascular disease. One study found that acute coronary syndrome occurred 1.72 times more often in patients with retinal artery occlusion than in controls 2. A10-fold increase in the annual rate of stroke in patients with retinal emboli compared to controls after a follow-up period of 3.4 years was demonstrated in another study 3. Over a similar period, another study showed a 20% incidence of stroke in patients with retinal artery occlusion 4.
Regarding mortality, one study found a 3-fold higher risk of 8-year mortality from stroke in patients with documented retinal emboli at baseline compared with patients without emboli. A case series reported that 15% of patients with retinal emboli died within 1 year, and a mortality rate of 54% was shown within 7 years. Given the higher incidence of cardiovascular and cerebrovascular complications in these patients, appropriate subspecialist referrals should be made at the time of diagnosis.
From an ocular standpoint, and in the absence of subsequent retinal artery occlusions, vision usually stabilizes soon after the ischemic event. A rare, long-term ophthalmic complication is neovascularization. The incidence of neovascularization in all retinal artery obstructions is less than 5%. In branch retinal artery occlusion, the incidence is even less common. One large study demonstrated a < 1.0% incidence of neovascularization after branch retinal artery occlusion 5. Neovascularization, when it does occur, is more likely in patients with diabetes. Clinical cases have been reported in which neovascular glaucoma developed after branch retinal artery occlusion 6.
Figure 1. Ophthalmic artery
Retinal artery occlusion causes
Retinal artery occlusion occurs due to blockage of the retinal artery, often by an embolus (a small piece of cholesterol that blocks blood flow) or thrombus (blood clot) that get stuck in the retinal arteries. These blockages are more likely if there is hardening of the arteries (atherosclerosis) in the eye. The retinal artery occlusion may be transient and last for only a few seconds or minutes if the blockage breaks up and restores blood flow to the retina, or it may be permanent.
Clots may travel from other parts of the body and block an artery in the retina. The most common sources of clots are the heart and carotid artery in the neck.
Most retinal artery blockages occur in people with conditions such as:
- Carotid artery disease, in which the two large blood vessels in the neck become narrowed or blocked
- Diabetes
- Heart rhythm problem (atrial fibrillation)
- Heart valve problem
- High levels of fat in the blood (hyperlipidemia)
- High blood pressure
- Intravenous drug abuse
- Temporal arteritis (damage to arteries due to an immune response)
If a branch of the retinal artery is blocked, part of the retina will not receive enough blood and oxygen. If this happens, you may lose part of your vision.
Risk factors for retinal artery occlusion
Common risk factors for retinal artery occlusion include:
- Carotid artery disease
- Atherosclerosis (fatty deposits in the arteries)
- Faulty heart valves (valvular heart disease)
- Tumors in the heart (myxoma)
- Abnormal heart rhythms such as atrial fibrillation
- Diabetes
- High blood pressure
- Intravenous drug abuse
- Giant-cell arteritis
- Disorders contributing to blood clot formation, such as sickle cell disease
- Use of oral contraceptives
- Homocystinuria (a hereditary disorder that prevents your body from processing the amino acid methionine; this leads to an excess accumulatio of homocysteine in the blood and urine)
- Pregnancy
- Blood platelet abnormalities
Retinal artery occlusion prevention
Measures used to prevent other blood vessel (vascular) diseases, such as coronary artery disease, may decrease the risk for retinal artery occlusion. These include:
- Eating a low-fat diet
- Exercising
- Stopping smoking
- Losing weight if you are overweight
Sometimes, blood thinners may be used to prevent the artery from becoming blocked again. Aspirin or other anti-clotting drugs are used if the problem is in the carotid arteries. Warfarin or other more potent blood thinners are used if the problem is in the heart.
The most important risk factor to manage is giant cell arteritis. Patients who are suspected to have ophthalmic artery occlusion secondary to giant cell arteritis should be started immediately on corticosteroids and continued for six to twelve months. A temporal artery biopsy may be performed 2 weeks after initiation of steroids and some authors have found positive biopsy results 4 weeks after steroid initiation 7. Starting steroids in patients under the age of 50 years, in African-american patients, or patients with elevated ESR in the setting of chronic kidney disease may not be clinically indicated. A new agent, tocilizumab, may reduce the amount of time that patients need to be treated with corticosteroids.
Retinal artery occlusion symptoms
Retinal artery occlusion is usually associated with sudden painless blurring or loss of vision in one eye. The area of the retina affected by the blocked vessels determines the area and extent of visual loss.
- The main artery supplying blood to the eye is the ophthalmic artery; when it is blocked, it produces the most damage. A blockage in the main artery in the retina is called central retinal artery occlusion (CRAO), which often results in severe loss of vision. However, about 25% of people who develop central retinal artery occlusion have an extra artery called a cilioretinal artery in their eyes. When central retinal artery occlusion occurs, having a cilioretinal artery can greatly lessen the chances of damage to your central vision, as long as the cilioretinal artery is not affected.
- A blockage in a smaller artery is called branch retinal artery occlusion (BRAO); this may cause a loss of a section of your visual field, such as your vision to one side. If the affected area is not in the center of the eye or is relatively small, a branch retinal artery occlusion may go unnoticed with no symptoms.
The retinal artery occlusion may last for only a few seconds or minutes, or it may be permanent.
A blood clot in the eye may be a warning sign of clots elsewhere. A clot in the brain may cause a stroke.
Retinal artery occlusion complications
Formation of new blood vessels of the retina or iris that are prone to bleed is a rare complication seen after a central retinal artery occlusion or branch retinal artery occlusion. Growth of these vessels can further decrease vision by causing vitreous hemorrhage and glaucoma. Findings of neovascularization may be delayed in patients treated with clot busting tissue plasminogen activator (tPA) or hyperbaric oxygen. If neovascularization happens, laser photocoagulation therapy is used to create burns in the area of the blocked artery to try to lower the oxygen demand of the retina and thus stop the abnormal blood vessels from growing.
Intravitreal injections of anti-VEGF medications such as Avastin® (bevacizumab), Lucentis® (ranibizumab) or Eylea® (aflibercept) may also be used in such cases.
Complications from invasive intervention with intravenous or intra-arterial tPA may include symptomatic intracranial hemorrhage, choroidal hemorrhage, or death 8.
Retinal artery occlusion diagnosis
Patients typically describe sudden, painless, vision loss that occurs over seconds. Visual acuity may vary depending on the location of the obstruction. Complete vision loss to no light perception should raise suspicion of an ophthalmic artery occlusion. Patients with central retinal artery occlusion complain of visual loss over the entire field of vision, while those with a branch retinal artery occlusion complain of hemifield defect. A patient with cilioretinal artery sparing may have 20/20 vision. Visual loss may have been preceded by transient loss of vision in the past (amaurosis fugax) in the case of embolic sources. In the case of branch retinal artery occlusions, there may be artery-to-artery anastomoses.
Sudden vision loss in a patient older than 50 years of age should immediately raise suspicion for Giant Cell Arteritis. An erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and complete blood count (CBC) with platelets should be obtained in patients over the age of 50 who have symptoms of giant cell arteritis 9. Urgent systemic steroids may be needed to preserve vision in the affected eye and prevent vision loss in the unaffected eye 9. Diabetic patients may need close follow-up as steroids will cause hyperglycemia.
Patients younger than 50 should have a vasculitis and/or hypercoagulable workup including antiphospholipid antibody syndrome, autoimmune conditions, inflammatory disorders, and other hypercoagulable states 9. In a young patient with multiple or recurrent branch retinal artery occlusions, Susac syndrome should be considered.
In older individuals, atherosclerosis and emoboli are the most likely cause of the ischemia. Evaluation of the heart with echocardiography should be performed to determine cardiac function and abnormalities of the valves. Electrocardiograms and heart monitoring may reveal a rhythm defect. Cartotid artery stenosis should be evaluated with carotid ultrasound 9.
General tests should include:
- Blood pressure
- Blood tests, including cholesterol and triglyceride levels and the erythrocyte sedimentation rate
- Physical examination
Tests to identify the source of a clot from another part of the body:
- Echocardiogram
- Electrocardiogram
- Heart monitor for abnormal heart rhythm
- Duplex Doppler ultrasound of the carotid arteries
Tests to evaluate your retina may include:
- Examination of the retina after dilating the pupil
- Fluorescein angiography
- Intraocular pressure
- Pupil reflex response
- Refraction
- Retinal photography
- Slit lamp examination
- Testing of side vision (visual field examination)
- Visual acuity
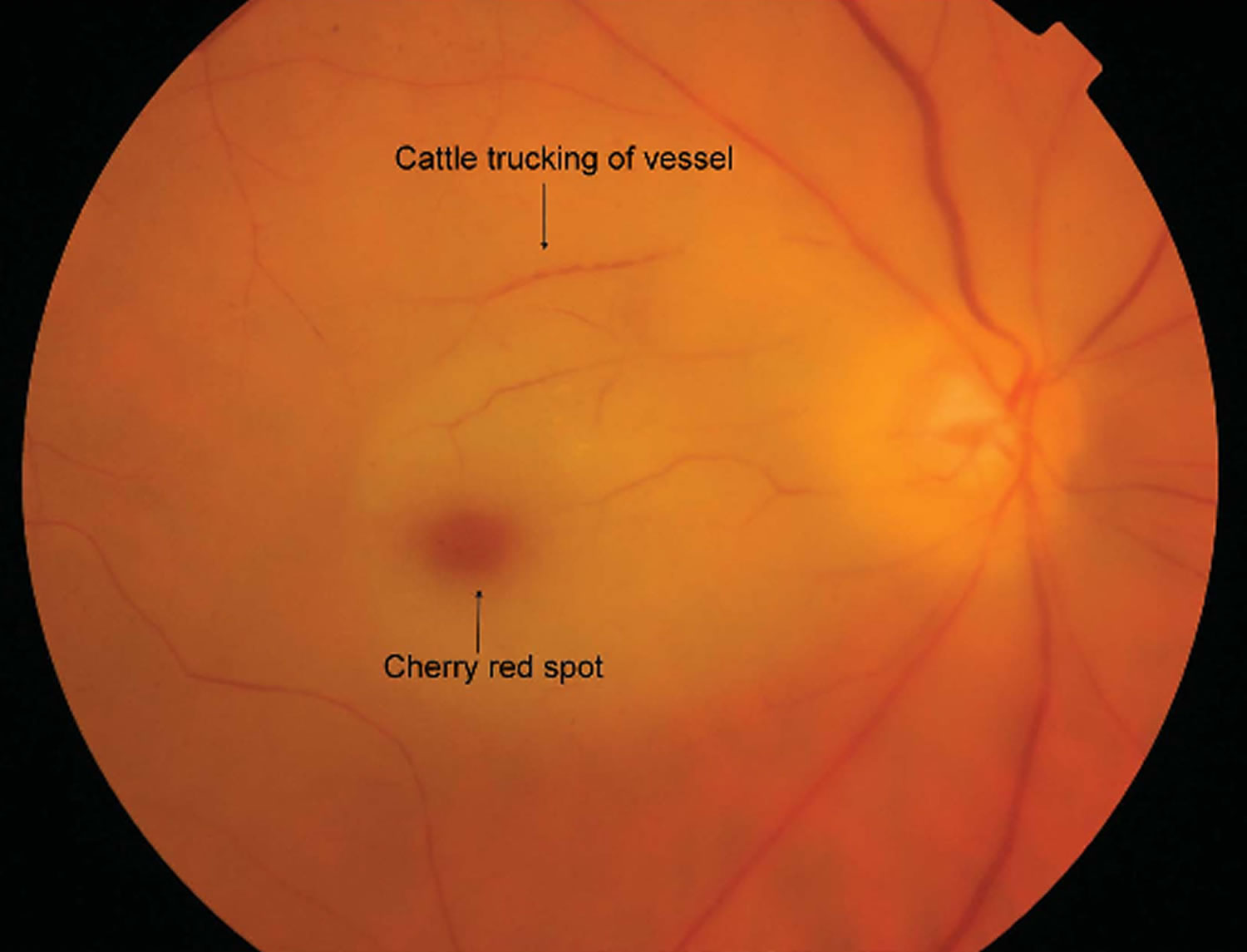
Central retinal artery occlusion is usually diagnosed by a dilated eye examination that shows a “cherry red spot,” where the center of the macula appears red, with the surrounding retina pale due to the lack of blood flow (Figure 2). Branch retinal artery occlusion appears as an area of superficial retinal whitening along the blocked vessel (Figure 3). The whitening of the retina generally lasts 4 to 6 weeks before fading.
Optical coherence tomography (OCT) provides detailed images of the central retina, and shows swelling in the inner layers of the retina in the affected area. Optical coherence tomography (OCT) reveals hyperreflectivity of the inner retina in acute stages. The amount of retinal edema is related to visual prognosis 10. Over the course of about 1 month, the inner retinal becomes atrophic and much thinner than normal.
Fluorescein angiography shows a delay in filling of the retinal arteries and a delayed arteriovenous transit time in the affected areas. The flow of blood in retinal arteries are very sluggish. The front edge of fluorescein (an arterial dye front-the angiographic feature with highest specificity) is seen to travel very slowly to the peripheral retina along the branches of retinal arteries. Complete lack of filling of the retinal vessels is very rare. Delayed choroidal filling should point to an ophthalmic or carotid artery obstruction. Over time, the vessels re-open and flow reverts to normal, despite the persistence of retinal vessel narrowing. When retinal circulation re-establishes, the retinal fluorescein angiogram may be unremarkable, despite clinically pale retina, and cherry red spot, especially in cases where no emboli or boxcarring is clinically visible.
Poor perfusion of the arterial tree can be demonstrated by the ability to induce retinal pulsations in the central retinal artery by digital pressure on the eyeball (ophthaldynomometry).
Electroretinography (ERG), shows a characteristic diminution of the b-wave. This is due to inner retinal ischemia. The electroretinography (ERG) may be normal in some cases (despite poor visual acuity) if the blood flow renormalizes.
Retinal artery occlusion treatment
Retinal artery occlusion is an eye emergency. Patients should be referred to the nearest stroke center for further immediate management. Your eye doctor should look for the cause of the blockage. Blockages may be signs of a life-threatening medical problem. However, the evidence is limited for asymptomatic branch retinal artery occlusion 9.
There is no proven treatment for vision loss that involves the whole eye, unless it is caused by another illness that can be treated.
There are no evidence based therapies that have demonstrated efficacy in improving visual outcomes, and a meta-study has suggested that some therapies may be worse than the natural course 8. Some of these are described below.
Several treatments may be tried. To be helpful, these treatments must be given within 2 to 4 hours after symptoms begin. However, the benefit of these treatments has never been proven, and they are rarely used.
- Breathing in (inhaling) a carbon dioxide-oxygen mixture. This treatment causes the arteries of the retina to widen (dilate).
- Massage of the eye.
- Removal of fluid from within the eye. The doctor uses a needle to drain a small amount of fluid from the front of the eye. This causes a sudden drop in eye pressure, which can sometimes cause the clot to move into a smaller branch artery where it will cause less damage.
- The clot-busting drug, tissue plasminogen activator (tPA).
Clot busting tissue plasminogen activator (tPA) was evaluated in the EAGLE study 11, which was a randomized controlled trial comparing intra-arterial fibrinolysis to placebo. The study did not recommend intra-arterial tPA for acute central retinal artery occlusion because of significant symptomatic intracranial hemorrhage without evidence of visual benefit. The trial was terminated early due to the adverse effects of tPA.
A randomized controlled trial 12 comparing intravenous tPA to placebo did not show improved short term visual benefit when given within 6 hours, but this was not sustained. There was no long term visual benefit and intracranial hemorrhage was an adverse reaction noted in this small study. Although recent meta-analysis of observation studies 8 suggest that there may be mild benefit to intravenous tPA when given within 4.5 hours, they also reported several fatalities associated with tPA. Their analysis also suggested that conservative treatments (ocular massage, paracentesis, hemodilution) led to worse outcomes 8.
Ocular massage is a conservative therapy that may theoretically cause emboli to travel more distally to reduce the area of ischemia. A three-mirror contact lens is placed on the eye and pressure is applied for 10 s, to obtain retinal artery pulsation or flow cessation followed by a 5 s release 13. Similar, anterior chamber paracentesis may be performed by removing 0.1-0.4 ml of aqueous fluid from the anterior chamber using a small gauge needle (27 or 30 gauge) 14. Theoretically, the paracentesis lowers the intraocular pressure and may allow the embolus (if any) to move further down the vessel and away from the central retina. In addition, the intraocular pressure may be decreased medically with eyedrops.
Increasing carbon dioxide concentration has also been proposed to induce vasodilation. The patient is instructed to breathe into a bag in order to increase carbon dioxide concentration 15. Alternatively, a patient may be given an oxygen mask to try to increase oxygen perfusion through the choroidal circulation. A mixture of 95 % oxygen and 5 % carbon dioxide has also been proposed to increase bloodflow.
Retinal artery occlusion prognosis
People with blockages of the retinal artery may not get their vision back. Visual loss with central retinal artery occlusion is usually severe, and is strongly correlated with the amount of retinal edema 10. However, with central retinal artery occlusions, in the presence of a cilioretinal artery, visual acuity usually recovers to 20/50 or better in over 80 % of eyes 16. Neovascularization may occur and patients should be followed closely 17. Patients need to be examined for development of iris neovascularization, which has been reported to occur in 2.5 % to 31.6 % of patients. A recent study showed an prevalence of 18 % with a mean onset of 8.5 weeks post-occlusion.
Visual field loss in branch retinal artery occlusions is usually permanent. Visual acuity may recover to 20/40 or better in 80 % of eyes.
Central retinal artery occlusion
The central retinal artery supplies the inner retina. Occlusion of the central retinal arteries results in ischemia of the inner retina. When the inner retina is damaged, it first becomes very edematous (swollen). Over time, the edema (swelling) resolves and the inner retina atrophies. In central retinal artery occlusion , the outer retina is perfused by the choroidal circulation and some inner retina tissue may survive, thus some vision is preserved. Over the course of about week, the occlusion may recannulate 18. Unfortunately, the retina is very sensitive to ischemia and animal models have demonstrated irreparable damage occurs after 105 minutes of occlusion 19. Thus, the vision loss is often permanent with only mild visual recovery.
Figure 2. Central retinal artery occlusion
Central retinal artery occlusion causes
Emboli dislodged from the carotid artery are the most common cause of central retinal artery occlusion, from either an unstable atherosclerotic plaque or a cardiac source.
The probable causes of central retinal artery occlusion vary depending on the age of the patient. A detailed analysis of comorbid disease is necessary to elucidate the cause of the acute visual loss:
- Systemic hypertension, seen in two-thirds of patients
- Diabetes mellitus
- Cardiac valvular disease, seen in a quarter of patients
- Cardiac anomalies, such as patent foramen ovale (PFO)
- Embolism, as follows:
- Cholesterol is the most common type, but it can also be from calcium, bacteria, or talc from intravenous drug use.
- This is associated with poorer visual acuity and higher overall morbidity and mortality.
- Emboli from the heart are the most common cause of central retinal artery occlusion in patients younger than 40 years.
- Atherosclerotic changes, as follows:
- Carotid atherosclerosis is seen in 45% of cases of central retinal artery occlusion, with 60% or greater stenosis in 20% of cases. Callizo et al 20 found that ipsilateral carotid stenosis was the most significant risk factor for central retinal artery occlusion.
- Atherosclerotic disease is the leading cause of central retinal artery occlusion in patients aged 40-60 years.
- Chang et al 21 have found an increased risk of acute coronary syndrome (indicative of coronary atherosclerosis) in patients with retinal arterial occlusions.
- Amaurosis fugax preceding persistent vision loss suggests transient central retinal artery occlusion, branch retinal artery occlusion (BRAO), or temporal arteritis.
- A hypercoagulable state, such as in patients with sickle cell anemia, polycythemia, or antiphospholipid syndrome or in those taking oral contraceptives, is a common etiology of central retinal artery occlusion in patients younger than 30 years.
- Giant cell arteritis, as follows:
- Giant cell arteritis should be considered in elderly patients
- Giant cell arteritis may produce central retinal artery occlusion, cilioretinal artery occlusion, ischemic optic neuropathy, or a combination of these findings
- Giant cell arteritis needs to be treated immediately with corticosteroids to preserve vision in the fellow eye.
- Collagen vascular disease
- Polyarteritis nodosa
- Behçet disease
- Syphilis
- Migraine
- Increased intraocular pressure due to glaucoma
- Hydrostatic arterial occlusion
- Iatrogenic: With the increasing popularity of cosmetic facial filler injections, Chen et al 22 and Carle et al 23 report that these injections are a cause of retinal artery occlusions. Other associations with central retinal artery occlusion, such as extracapsular cataract extraction with retrobulbar anesthesia, strangulation, or injection of stem cells for scalp baldness, have been published 24.
Central retinal artery occlusion symptoms
The most common presenting complaint of central retinal artery occlusion (central retinal artery occlusion) is acute, unilateral, persistent, painless vision loss in the range of counting fingers to light perception in 90% of patients. The clinician should consider an ophthalmic artery occlusion if the visual acuity is worse or if the cherry red spot is absent (indicating possible choroidal as well as retinal artery occlusive disease).
Some patients with central retinal artery occlusion reveal a history of amaurosis fugax (transient vision loss lasting seconds to minutes but that may last up to 2 hours), which may result from transient central retinal artery occlusion. The vision usually returns to baseline after an episode of amaurosis fugax.
The clinician should inquire about the symptoms of temporal arteritis in older patients (eg, headache, jaw claudication, scalp tenderness, proximal muscle and joint aches, anorexia, weight loss, fever).
The past medical history should include any medical problems that could predispose to embolus formation (eg, atrial fibrillation, endocarditis, atherosclerotic disease, hypercoagulable state). Other predisposing factors include prolonged direct pressure to the globe during drug-induced stupor or improper positioning during face-down surgical procedures. The physician should also inquire about any illicit drug history.
Central retinal artery occlusion complications
Patients with central retinal artery occlusion may develop a cerebrovascular accident due to secondary emboli. Park et al 25 found that patients with central retinal artery occlusion had a significantly increased risk for stroke and acute myocardial infarction, particularly during the first week following central retinal artery occlusion. Further emboli could travel to the same or contralateral eye, resulting in further visual loss. Ocular neovascularization, including neovascular glaucoma, occurs in approximately 15% of patients with central retinal artery occlusion, especially in those with diabetes mellitus, type 2 5.
Central retinal artery occlusion diagnosis
Patients typically describe sudden, painless, vision loss that occurs over seconds. Visual acuity may vary depending on the location of the obstruction. Complete vision loss to no light perception should raise suspicion of an ophthalmic artery occlusion. Patients with central retinal artery occlusion complain of visual loss over the entire field of vision. A patient with cilioretinal artery sparing may have 20/20 vision. Visual loss may have been preceded by transient loss of vision in the past (amaurosis fugax) in the case of embolic sources.
A relative afferent pupillary defect may be present in central retinal artery occlusion or ophthalmic artery occlusion.
Early in the course, the fundus may appear normal.
In central retinal artery occlusion, the classic findings of retinal whitening and a cherry red spot are due to opacification of the nerve fiber layer as it becomes edematous from ischemia. The fovea is cherry red because it has no overlying nerve fiber layer. This finding may take hours to develop, and the edema is associated with a worse visual prognosis. Over the course of about a month, the inner retina becomes atrophic as the swelling resolves.
Examination of the retinal blood vessels shows segmental blood flow, classically described as boxcarring. This is best appreciated with slit-lamp biomicroscopy. Over about the course of a week, the vessels reperfuse.
Chronic signs of retinal artery occlusion include pale optic disc, thinned retinal tissue, attenuated vessels, retinal pigment epithelial mottling, and severely decreased vision.
Laboratory studies
Laboratory studies may be helpful in determining the etiology of central retinal artery occlusion, as follows:
- Complete blood count (CBC) (eg, anemia, leukemia, polycythemia, platelet disorders)
- Erythrocyte sedimentation rate (ESR) evaluation for giant cell arteritis in elderly patients
- Hypercoagulable state evaluation (eg, factor V Leiden, prothrombin mutation, homocysteine levels, fibrinogen, antiphospholipid antibodies, prothrombin time/activated partial thromboplastin time [PT/aPTT], serum protein electrophoresis, among others)
- Fasting blood sugar, cholesterol, triglycerides, and lipid panel to evaluate for atherosclerotic disease
- Blood cultures to evaluate for suspected bacterial endocarditis and septic emboli
Imaging Studies
Imaging studies are helpful in determining the etiology of central retinal artery occlusion.
Carotid ultrasonography
Carotid ultrasonography may be used to evaluate for atherosclerotic plaque; this appears to be more sensitive than carotid ultrasonography with Doppler, which determines only the flow.
Magnetic resonance imaging (MRI)
Approximately 20% of patients with a central retinal artery occlusion also have cerebral ischemia; therefore, magnetic resonance imaging (MRI) of the brain may reveal concurrent cerebral ischemia in patients without accompanying neurological symptoms 4. Magnetic resonance angiography (MRA) of the head and neck may be more accurate in detecting vascular occlusive disease. Computerized tomography (CT) or computerized tomography angiography (CT/CTA) or MRI/MRA of the neck may be needed for carotid dissection.
Fundus autofluorescence
In the acute phase, fundus autofluorescence in ischemic areas is decreased because of retinal edema blocking the normal RPE. Eventually, this could return to normal baseline or may be associated with increased autofluorescence owing to a window defect created by the thinned-out inner retinal layers 26.
Fluorescein angiography
Fluorescein angiography may be a prognostic test 27. Poor perfusion on fluorescein angiography has been associated with lower vision than exudative and mixed perfusion 27. This finding does not influence therapy.
- Normal choroidal filling begins 1-2 seconds before retinal filling and is complete within 5 seconds of dye appearance in healthy eyes. A delay of 5 or more seconds is seen in 10% of patients. Consider ophthalmic artery occlusion or carotid artery obstruction if choroidal filling is significantly delayed.
- Delay in arteriovenous transit time (reference range, < 11 seconds)
- Delay in retinal arterial filling
- Arterial narrowing with normal fluorescein transit after recanalization
Spectral-domain optical coherent tomography
Spectral-domain optical coherent tomography (OCT) has been proposed as one modality that might be used to diagnose and monitor central retinal artery occlusion.
In central retinal artery occlusion, there is an observed increase in intensity of inner retinal layers compared with age-matched controls, and it corresponds to the layers supplied by central retinal arteries. Chen et al showed that optical intensity on OCT can be correlated with visual prognosis 28. Incomplete central retinal artery occlusion shows minimal retinal architectural disruption and inner layer hyper-reflectivity without retinal edema. Subtotal central retinal artery occlusion demonstrated inner macular thickening and loss of organization of the inner retina, and total central retinal artery occlusion demonstrated marked inner retinal thickening and subfoveal choroidal thinning 29. In the chronic phase, there is a corresponding thinning of the inner retinal layers.
Optical coherent tomography angiography
Optical coherent tomography angiography (OCTA) is a novel noninvasive technique that eliminates the need for dye injection to evaluate the retinal microvasculature. It is based on the principle that static and nonstatic structures (ie, blood flowing through vessels) generate different signal amplitudes on repeated B scans from the same cross-sections. OCTA provides structural and functional (blood flow) information at a fixed point; however, it is not useful to appreciate leakage from vessels 30.
OCTA shows decreased vascular perfusion in superficial and deep retinal plexus that corresponds to poor perfusion on fluorescein angiography. In patients with the cilioretinal artery–sparing variant, the deep capillary plexus retained perfusion. However, unlike fundus fluorescein angiography, OCTA cannot demonstrate a delay in transit time 31.
Electroretinography
Electroretinography shows a diminished b-wave corresponding to Muller and/or bipolar cell ischemia.
Other Tests
Systemic tests are used to identify additional risks that may lead to cerebral ischemia, myocardial infarction, and cardiovascular death.
Electrocardiography
Electrocardiography (ECG) is used to evaluate for possible atrial fibrillation.
Holter monitor
A 24-hour Holter monitor may be necessary if arrhythmia is suspected but not detected on ECG testing.
Echocardiography
Echocardiography may reveal valvular disease, wall motion abnormalities, and/or mural thrombi.
Central retinal artery occlusion treatment
Unfortunately, there is no clinically proven treatment for central retinal artery occlusion. Several therapies may be used including:
- Hyperventilation—inhaling carbogen, a mixture of 95% oxygen and 5% carbon dioxide, to attempt to dilate the retinal arteries and cause the clot to dislodge
- Paracentesis (removal of fluid from the front of the eye using a small-gauge needle) to lower
the intraocular pressure to try to dislodge the embolus - Lowering the intraocular pressure with medication
- Ocular massage with a thumb to dislodge the clot
However, for any treatment to be potentially effective in central retinal artery occlusion, it must be deployed within a short time window, probably within 4 to 6 hours after symptoms begin. Unfortunately, none of these therapies have been shown to predictably alter the natural history of disease.
Thrombolytic therapy (“clot-busting” drugs), delivered either intravenously or directly through the ophthalmic artery, has also been tried but clinical trials have not shown this treatment to be effective.
An important aspect of managing retinal artery occlusion is for your doctor to identify and manage risk factors that may lead to other vascular conditions. The risk factors for central retinal artery occlusion are the same atherosclerotic risk factors as for stroke and heart disease; tests are important to try to identify the source of a clot from another part of the body. These tests include:
- A carotid ultrasound to determine whether there are carotid plaques present
- Cardiac echocardiography to look for disease in the heart valves
A doctor may also order a test of your blood’s sedimentation rate (ESR) and a temporal artery biopsy may be useful if giant cell arteritis is suspected.
Central retinal artery occlusion prognosis
Vision loss with central retinal artery occlusion is usually severe. However, central retinal artery occlusions in patients who have a cilioretinal artery have better visual prognosis, usually recovering to 20/50 vision or better in over 80% of eyes.
Branch retinal artery occlusion
A branch retinal artery occlusion (BRAO) occurs when one of retinal branches of the arterial supply to the retina becomes occluded. In branch retinal artery occlusion, only part of the retina is involved. The area of retina affected by the occluded vessels is associated with the area and degree of visual loss.
Typically, branch retinal artery occlusion presents in the seventh decade of life. branch retinal artery occlusion due to embolic causes is rare in patients younger than 30 years. Less than 1 per 50,000 outpatient visits to the ophthalmologist are estimated to involve a person younger than 30 years with retinal arterial obstruction. These cases are more likely to be nonembolic causes of retinal arterial occlusions.
Figure 3. Branch retinal artery occlusion

Branch retinal artery occlusion causes
Most commonly, branch retinal artery occlusion results from an embolus. Emboli typically originate within vessels upstream where they dislodge and travel within the circulatory system to ultimately become lodged downstream in a vessel with a smaller lumen. The most common include cholesterol emboli from aorto-carotid atheromatous plaques, platelet-fibrin emboli from thrombotic disease, and calcific emboli from cardiac valvular disease. Various other endogenous emboli as well as exogenous emboli and nonembolic causes have been reported 32.
Ischemia of the inner layers of the retina leads to intracellular edema as a result of cellular injury and necrosis. This intracellular edema has the ophthalmoscopic appearance of grayish whitening of the superficial retina. Primate studies have shown that complete occlusion of arterial supply to the retina results in reversible ischemic injury in up to 97 minutes. This may help explain why patients may give a history of transient loss of vision prior to an episode of branch retinal artery occlusion. Possibly, these episodes are secondary to emboli transiently becoming lodged, causing temporary occlusions and then reperfusing the retina as the emboli are released.
Branch retinal artery occlusion is most likely to occur at the bifurcation of an artery because bifurcation sites are associated with a narrowed lumen. In 90% of cases, branch retinal artery occlusions involve the temporal retinal vessels. Whether the temporal retinal vessels are affected more often or whether the nasal retinal vessel occlusions are more often undetected is unclear.
Patients with branch retinal artery occlusion have a higher risk for morbidity and mortality secondary to cardiovascular and cerebrovascular disease. A thorough medical workup is indicated for all patients with branch retinal artery occlusion, and a cause can be identified in as many as 90% of patients.
In elderly patients, embolic disease is the most common cause of a branch retinal artery occlusion. In a study of 70 patients with retinal emboli, 40 were found to have cholesterol emboli, 8 platelet-fibrin emboli, 6 calcific emboli, and 1 possible myxomatous embolus 33. These types of emboli can also be iatrogenically displaced during cardiac angiography, catheterization procedures, or any interventional embolization of any branch of the carotid artery.
Types of emboli (endogenous and exogenous) include the following:
- Cholesterol – Atheromatous plaques from the aorto-carotid system
- Platelet-fibrin – Carotid or cardiac thrombosis
- Calcific – Calcified cardiac valves and atheromatous plaques of the carotid artery
- Leukoemboli -Vasculitis, Purtscher retinopathy, septic endocarditis
- Fat emboli – Following long bone fractures
- Amniotic fluid emboli – Complication of pregnancy
- Tumors – Atrial myxoma, mitral valve papillary fibroelastoma
- Talc emboli – Long-term intravenous drug abusers
- Corticosteroid emboli – Complication of intralesional or retrobulbar steroid injection
- Air emboli – Following trauma or surgery
- Synthetic particles – From synthetic materials used in artificial cardiac valves and other vascular procedures; facial dermal filler (Restylane)
- Interventional embolization material (Onyx) (this has been observed at the current authors’ institution)
In younger patients, other more obscure and diverse etiologies are more likely. In patients younger than 30 years with retinal artery occlusion, associations have been noted with migraines, coagulation abnormalities, trauma, increased intraocular pressure, optic nerve drusen, oral contraceptives, and other entities, which merit a more comprehensive review. Atheromatous disease is a rare cause of retinal artery occlusion in this age group, and routine carotid angiography for embolic cause is not recommended. Visual prognosis is similar to older patients.
Nonembolic causes of branch retinal artery occlusion include the following:
- Thrombosis – Atherosclerosis, chemotherapeutic agents, bone marrow transplants
- Inflammatory conditions – Syphilis, toxoplasma, retinochoroiditis, Behçet disease, Lyme disease, pseudotumor cerebri, Bartonella infection, HIV infection, posterior scleritis, varicella-zoster infection, multifocal retinitis with optic nerve edema, West Nile virus infection, giant cell arteritis
- Vasospasm – Migraines, cocaine abuse, sildenafil citrate use
- Coagulopathies – Sickle cell disease, Hodgkin disease, pregnancy, anemia, platelet and clotting factor abnormalities, protein C, protein S, antithrombin III, factor V Leiden deficiencies, oral contraceptives, homocystinuria, antiphospholipid syndrome, chelation therapy
- Autothrombosis – From a ruptured arteriolar macroaneurysm
- Compression – Preretinal arterial loops, vitrectomy surgery, trauma
- Idiopathic – Syndrome involving recurrent episodes of multiple branch retinal artery occlusions in otherwise healthy individuals, association with Susac syndrome (microangiopathy of brain, retina, and cochlea) in some of patients
Branch retinal artery occlusion symptoms
Patients with branch retinal artery occlusion typically present with acute, unilateral, painless, partial visual loss. Visual field defects may be central or sectoral. Patients may also be asymptomatic.
Risk factors include smoking, hypertension, hypercholesterolemia, diabetes, coronary artery disease, or history of stroke or transient ischemic attack (TIA). Seventy-five percent of patients have hypertension or carotid occlusive disease.
Patients may give a history of temporary episodes of visual loss (amaurosis fugax) or neurologic loss (transient ischemic attack). A study showed a prevalence of amaurosis fugax of 14.2% in branch retinal artery occlusion 34.
The physician should ask about any medical problems related to increased risk for embolus formation (eg, heart valve disorders, history of endocarditis, carotid stenosis, coagulopathies, atrial fibrillation), as well as family history of blood clots or clotting disorders. These patients have a significantly higher risk of stroke or cardiovascular events compared with the general population, so appropriate evaluation and referral is necessary 35.
Branch retinal artery occlusion diagnosis
Laboratory tests to consider in patients with suspected branch retinal artery occlusion include the following:
- In patients older than 50 years, consider ordering an immediate erythrocyte sedimentation rate (ESR) to help rule out giant cell arteritis.
- In patients younger than 50 years or in patients with the appropriate risk factors, consider the following tests to evaluate for coagulopathies: antitreponemal antibody, antiphospholipid antibody, antinuclear antibody, rheumatoid factor, serum protein electrophoresis, hemoglobin electrophoresis, prothrombin time/activated partial thromboplastin time (PT/aPTT), fibrinogen, protein C and S, antithrombin III, and factor V Leiden.
- A complete blood count (CBC) is obtained to evaluate for anemia, polycythemia, and platelet disorders.
- Fasting blood sugar, glycosylated hemoglobin, cholesterol, triglycerides, and lipid panel are obtained to evaluate for atherosclerotic disease.
- Blood cultures are obtained to evaluate for bacterial endocarditis and septic emboli.
Physical examination
Partial visual field deficit may respect the horizontal midline but never the vertical midline.
Funduscopic examination shows retinal whitening along the distribution of the affected artery. The site of obstruction is most often at the bifurcation of the arteries where emboli are most likely to become lodged. Affected retina may be edematous.
Narrowed branch retinal artery, boxcarring, segmentation of the blood columns, cotton-wool spots, and emboli are other possible findings. Emboli are visible in 62% of eyes with a branch retinal artery occlusion.
Some of the more common emboli include the following:
- Cholesterol emboli (also known as Hollenhorst plaques) appear as iridescent, reflective, thin yellow plates. These yellow plates are white rhomboid crystals measuring 10-250 µm in length and less than 3 µm in thickness. They appear yellow on funduscopic examination because of blood showing through their translucent thinness. Digital pressure on the eye can make them turn within the vessel causing them to become more or less visible to the examiner. They usually do not cause occlusion of the artery by themselves because blood can flow around them. However, if they occur in conjunction with platelet-fibrin or if they are large, then they can obstruct arterial blood flow. Because their sources are most likely atheromatous plaques in the aorto-carotid system, even asymptomatic patients need a medical workup.
- Platelet-fibrin emboli appear as whitish-gray, nonreflective plugs that are mobile. They may appear in “showers” and may pass through without causing an occlusion. They are usually associated with mural thrombus in the carotid artery or cardiac valvular structures.
- Calcific emboli appear as large, yellowish-white, nonreflective plaques. They more likely are found in the larger arterioles near the optic disc. They are associated with calcified cardiac valves and atheromatous plaques of the carotid artery.
One study demonstrated that attempts to categorize emboli into cholesterol, calcific, or other by funduscopic examination had large intraobserver and interobserver variability 36. The authors recommended that systemic evaluation not be based on qualitative assessment of the type of emboli.
Auscultation of the heart and carotid arteries and comparison of ophthalmodynamometry may help identify the source of emboli.
Imaging Studies
Acute branch retinal artery occlusion or central retinal artery occlusion should be treated as ocular and systemic emergencies, as they can be harbingers for subsequent stroke. Thus, guidelines necessitate urgent imaging and clinical evaluation 37. Imaging studies are imperative to determine the etiology of the embolus for the purpose of treatment and subsequent prevention of further artery occlusions or stroke.
Two-dimensional or transesophageal echocardiography
Elderly patients and patients with high-risk characteristics for cardioembolic disease warrant medical workup involving either 2-dimensional or transesophageal echocardiography. High-risk characteristics include a history of rheumatic heart disease, mitral valve prolapse, prosthetic valve placement, history of subacute bacterial endocarditis, recent heart attack, intravenous (IV) drug abuse, any type of valvular heart disease (congenital or acquired), detectable heart murmurs, and ECG changes (eg, atrial fibrillation, changes indicating myocardial damage).
Carotid ultrasonography studies and magnetic resonance angiography (MRA)
Considering the higher incidence of fatal stroke in the elderly population, atherosclerotic disease should be evaluated if no other etiology is obvious.
ECG/Holter monitor
ECG/Holter monitor is used to evaluate for atrial fibrillation.
Magnetic resonance imaging (MRI)
MRI can be used to evaluate for additional, possibly occult, vessel occlusions in the brain. In cases of suspected Susac syndrome, MRI may be helpful to look for classic findings in the corpus callosum. Any concern for concurrent stroke symptoms would warrant the appropriate brain imaging and workup, usually guided by neurologic consultation.
Fluorescein angiography
Delayed filling of the affected artery and hypofluorescence in the surrounding retina will be visible immediately after onset of the occlusion. Vessels distal to the site of obstruction may show retrograde filling from surrounding perfused capillaries. Late staining of the vessel walls may be seen.
After resolution of the obstruction, reperfusion can occur, and flow may return to normal. However, narrowing or sclerosis of the affected artery can occur. Artery-to-artery collaterals may form in the retina and are highly suggestive of an old branch retinal artery occlusion.
Optical coherence tomography
Optical coherence tomography (OCT) has been used to demonstrate structural damage of the retinal layers after retinal artery occlusion 38.
Increased thickening and hyperreflectivity of the inner retinal layers with decreased reflectivity of the photoreceptors and retinal pigment epithelium is often present, which supports the pathophysiology of increasing intracellular fluid within the inner retinal layer. The inner retina, rather than the outer retina, is preferentially affected, because the inner retinal layers receive blood flow from the central retinal artery and its branches, whereas the outer retinal layers are fed by the choroidal vasculature.
One study used OCT to demonstrate the long-term structural results after arterial occlusion. One year after diagnosis of branch retinal artery occlusion, the authors found segmental inner retinal layer and peripapillary retinal nerve fiber layer thickness to be reduced. They correlated visual field deficits with OCT thickness and found that a worse functional outcome was associated with a more extensive thinning of the macula and retinal nerve fiber layer.
Another study suggested that spectral domain OCT may be a useful adjunct in the acute phase in characterizing retinal artery emboli, including perfusion characteristics (eg, extent of luminal occlusion) and emboli characteristics and embolus structure (eg, more crystalline in appearance or softer and more conforming to the shape of the vessel lumen) 39.
Branch retinal artery occlusion treatment
Considering the increased rate of mortality, patients with branch retinal artery occlusion should receive a full medical workup with special attention to the cerebrovascular and cardiovascular system. Depending on the findings, carotid endarterectomy or anticoagulation may be indicated. Laboratory workup for coagulopathies should also be performed if no embolic source is found.
Branch retinal artery occlusion prognosis
Visual field loss in branch retinal artery occlusion is usually permanent, but central visual acuity may recover to 20/40 or better in 80% of eyes.
References- Branch Retinal Artery Occlusion (BRAO). https://emedicine.medscape.com/article/1223362-overview
- Chang YS, Chu CC, Weng SF, Chang C, Wang JJ, Jan RL. The risk of acute coronary syndrome after retinal artery occlusion: a population-based cohort study. Br J Ophthalmol. 2015 Feb. 99 (2):227-31.
- Bruno A, Jones WL, Austin JK, Carter S, Qualls C. Vascular outcome in men with asymptomatic retinal cholesterol emboli. A cohort study. Ann Intern Med. 1995 Feb 15. 122(4):249-53.
- Chang YS, Jan RL, Weng SF, Wang JJ, Chio CC, Wei FT, et al. Retinal artery occlusion and the 3-year risk of stroke in Taiwan: a nationwide population-based study. Am J Ophthalmol. 2012 Oct. 154 (4):645-652.e1
- Mason JO 3rd, Patel SA, Feist RM, Albert MA Jr, Huisingh C, McGwin G Jr, et al. Ocular neovascularization in eyes with a central retinal artery occlusion or a branch retinal artery occlusion. Clin Ophthalmol. 2015. 9:995-1000
- Yamamoto K, Tsujikawa A, Hangai M, Fujihara M, Iwawaki T, Kurimoto Y. Neovascular glaucoma after branch retinal artery occlusion. Jpn J Ophthalmol. 2005 Sep-Oct. 49(5):388-90
- Ray-Chaudhuri N, Kiné DA, Tijani SO, Parums DV, Cartlidge N, Strong NP, et al. Effect of prior steroid treatment on temporal artery biopsy findings in giant cell arteritis. British Journal of Ophthalmology. 2002 May 1;86(5):530–2.
- Schrag, M., Youn, T., Schindler, J., Kirshner, H. & Greer, D. Intravenous Fibrinolytic Therapy in Central Retinal Artery Occlusion: A Patient-Level Meta-analysis. JAMA Neurol 2015, 72, 1148–1154
- Retinal and Ophthalmic Artery Occlusions PPP – 2016. https://www.aao.org/preferred-practice-pattern/retinal-ophthalmic-artery-occlusions-ppp-2016
- Ahn SJ, Woo SJ, Park KH, Jung C, Hong J-H, Han M-K. Retinal and Choroidal Changes and Visual Outcome in Central Retinal Artery Occlusion: An Optical Coherence Tomography Study. American Journal of Ophthalmology. 2015 Apr 1;159(4):667–676.e1
- Schumacher, M. et al. Central retinal artery occlusion: local intra-arterial fibrinolysis versus conservative treatment, a multicenter randomized trial. Ophthalmology 2010, 117, 1367–1375.e1
- Chen, C. S. et al. Efficacy of intravenous tissue-type plasminogen activator in central retinal artery occlusion: report from a randomized, controlled trial. Stroke J. Cereb. Circ. 2011, 42, 2229–2234
- Cugati S, Varma DD, Chen CS, Lee AW. Treatment Options for Central Retinal Artery Occlusion. Curr Treat Options Neurol. 2013 Feb;15(1):63–77
- Atebara NH, Brown GC, Cater J. Efficacy of anterior chamber paracentesis and Carbogen in treating nonarteritic central retinal arterial occlusion. Am J Ophthalmol 1995; 102:2029-2034.
- Frayser R, Hickham JB. Retinal vascular response to breathing increased carbon dioxide and oxygen concentrations. Invest Ophthalmol 1964;3:427-431.
- Brown GC,and Shields JA. Cilioretinal arteries and retinal artery occlusion. Arch Ophthalmol 1979;97:84-92
- Rudkin AK, Lee AW, Chen CS. Ocular neovascularization following central retinal artery occlusion: prevalence and timing of onset. Eur J Ophthalmol 2010 May 28 Epub.
- Retinal Artery Occlusion. https://eyewiki.org/Retinal_Artery_Occlusion
- Hayreh SS, Zimmerman MB, Kimura A, Sanon A. Central retinal artery occlusion. Retinal survival time. Exp Eye Res. 2004 Mar;78(3):723–36.
- Callizo J, Feltgen N, Pantenburg S, Wolf A, Neubauer AS, Jurklies B, et al. Cardiovascular Risk Factors in Central Retinal Artery Occlusion: Results of a Prospective and Standardized Medical Examination. Ophthalmology. 2015 Sep. 122 (9):1881-8
- Chang YS, Chu CC, Weng SF, Chang C, Wang JJ, Jan RL. The risk of acute coronary syndrome after retinal artery occlusion: a population-based cohort study. Br J Ophthalmol. 2014 Aug 21
- Chen Y, Wang W, Li J, Yu Y, Li L, Lu N. Fundus artery occlusion caused by cosmetic facial injections. Chin Med J (Engl). 2014. 127(8):1434-7
- Carle MV, Roe R, Novack R, Boyer DS. Cosmetic facial fillers and severe vision loss. JAMA Ophthalmol. 2014 May. 132(5):637-9.
- Burke SP, Henderson AD, Lam BL. Central Retinal Artery Occlusion and Cerebral Infarction Following Stem Cell Injection for Baldness. J Neuroophthalmol. 2017 Jun. 37 (2):216-217.
- Park SJ, Choi NK, Yang BR, Park KH, Lee J, Jung SY, et al. Risk and Risk Periods for Stroke and Acute Myocardial Infarction in Patients with Central Retinal Artery Occlusion. Ophthalmology. 2015 Nov. 122 (11):2336-2343.e2
- Dattilo M, Biousse V, Newman NJ. Update on the Management of Central Retinal Artery Occlusion. Neurol Clin. 2017 Feb. 35 (1):83-100
- Gong H, Song Q, Wang L. Manifestations of central retinal artery occlusion revealed by fundus fluorescein angiography are associated with the degree of visual loss. Exp Ther Med. 2016 Jun. 11 (6):2420-2424
- Chen H, Xia H, Qiu Z, Chen W, Chen X. CORRELATION OF OPTICAL INTENSITY ON OPTICAL COHERENCE TOMOGRAPHY AND VISUAL OUTCOME IN CENTRAL RETINAL ARTERY OCCLUSION. Retina. 2016 Mar 10.
- Mehta N, Marco RD, Goldhardt R, Modi Y. Central Retinal Artery Occlusion: Acute Management and Treatment. Curr Ophthalmol Rep. 2017 Jun. 5 (2):149-159.
- de Carlo TE, Romano A, Waheed NK, Duker JS. A review of optical coherence tomography angiography (OCTA). Int J Retina Vitreous. 2015. 1:5.
- Bonini Filho MA, Adhi M, de Carlo TE, Ferrara D, Baumal CR, Witkin AJ, et al. OPTICAL COHERENCE TOMOGRAPHY ANGIOGRAPHY IN RETINAL ARTERY OCCLUSION. Retina. 2015 Nov. 35 (11):2339-46.
- Zamora RL, Adelberg DA, Berger AS, Huettner P, Kaplan HJ. Branch retinal artery occlusion caused by a mitral valve papillary fibroelastoma. Am J Ophthalmol. 1995 Mar. 119(3):325-9.
- Arruga J, Sanders MD. Ophthalmologic findings in 70 patients with evidence of retinal embolism. Ophthalmology. 1982 Dec. 89(12):1336-47.
- Hayreh SS, Zimmerman MB. Amaurosis fugax in ocular vascular occlusive disorders: prevalence and pathogeneses. Retina. 2014 Jan. 34(1):115-22.
- Biousse V, Nahab F, Newman NJ. Management of Acute Retinal Ischemia: Follow the Guidelines!. Ophthalmology. 2018 Apr 30.
- Sharma S, Pater JL, Lam M, Cruess AF. Can different types of retinal emboli be reliably differentiated from one another? An inter- and intraobserver agreement study. Can J Ophthalmol. 1998 Apr. 33(3):144-8.
- Biousse V, Nahab F, Newman NJ. Management of Acute Retinal Ischemia: Follow the Guidelines!. Ophthalmology. 2018 Apr 30
- Aleman TS, Tapino PJ, Brucker AJ. Evidence of recurrent microvascular occlusions associated with acute branch retinal artery occlusion demonstrated with spectral-domain optical coherence tomography. Retina. 2012 Sep. 32(8):1687-8
- Ahmed HJ, Klefter ON, Willerslev A, Munch IC, Larsen M. Embolus characterization in branch retinal artery occlusion by optical coherence tomography. Acta Ophthalmol. 2014 Aug 13.





{kind=link}