
What causes skin discoloration
The color of your skin and hair is mainly due to the amount of brown melanin pigment mixed with blue (from reduced hemoglobin), red (from oxyhemoglobin) and yellow (from carotenoids in the diet). The amount of melanin is determined by constitutional color (white, brown or black skin) and skin phototype, i.e. the result of exposure to ultraviolet (UV) radiation (tanning).
- Increase in melanin (hyperpigmentation or hypermelanosis) can be due to an increased number of pigment cells (melanocytes) or from increased production of melanin.
- Reduction in melanin results in pale patches (hypopigmentation or hypomelanosis) or white patches (leucoderma).
Pigmentation of the skin normally varies according to racial origin (see Fitzpatrick phototypes below) and the amount of sun exposure. Pigmentation disorders are often more troublesome in skin of color.
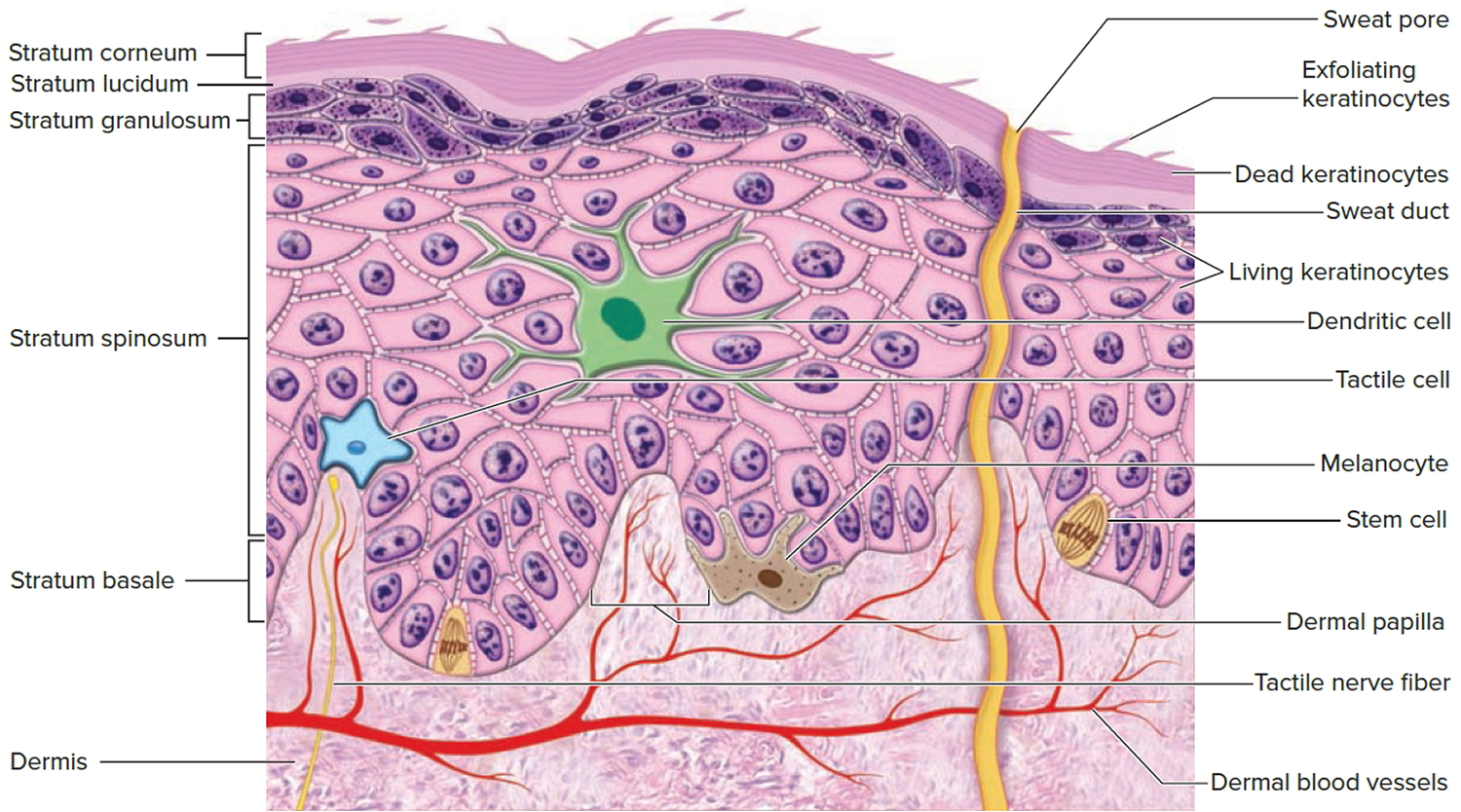
The pigment cells or melanocytes are located at the base of the epidermis and produce the protein melanin. Melanin is carried by keratinocytes to the skin surface. The melanocytes of dark skinned people produce more melanin than those of people with light skin. More melanin is produced when the skin is injured, for example following exposure to ultraviolet (UV) radiation. The melaninization process in dark skin is protective against sun damage, but melanization in white skin (for example after sunburn) is much less protective.
Hormonal effects of estrogen during pregnancy or due to medication can cause pigmentation of nipples, vulva and abdomen (linea nigra).
Some skin diseases and conditions result in generalized or localized hyperpigmentation (increased skin color or hypermelanosis), hypopigmentation (reduced skin color or hypomelanosis), or depigmentation (absent skin color or achromoderma).
A Wood lamp may be used to assess pigmentation during the examination of the skin, as pigmentary changes are often easier to identify while exposing the affected skin to long wavelength ultraviolet-A rays (UV-A).
Figure 1. Skin structure

Figure 2. Structure and skin cells of the Epidermis
Fitzpatrick skin type
Skin color is usually defined by the Fitzpatrick’s phototype classification created in 1975 (see Table 1) 1. The Fitzpatrick skin type (or phototype) depends on the amount of melanin pigment in the skin.This is determined by constitutional color (white, brown or black skin) and the result of exposure to ultraviolet radiation (tanning). Pale or white skin burns easily and tans slowly and poorly: it needs more protection against sun exposure. Darker skin burns less and tans more easily. It is also more prone to develop post-inflammatory pigmentation after injury (brown marks).
The Fitzpatrick skin type classification is based on a self-reported questionnaire, in which individuals grade their erythema (redness) sensitivity and tanning ability, respectively, 24 hour and seven days after the first unprotected sun-exposure in the early summer 1. It was originally created to categorize Caucasian skin into four skin phototypes, I–IV (1 to 4), with decreasing erythema (redness) sensitivity and increasing tanning ability. Skin type V (5) was added afterwards for individuals with brown skin of Asian and Latin American origin, and skin type VI (6) for dark skin of African extraction. Skin types I–IV are thus based on clinical response to UV (ultraviolet radiation), whereas classification into types V–VI is based on constitutive pigmentation or ethnic origin. Although this classification is helpful to determine the appropriate dose for phototherapy and is widely used in epidemiological studies of skin cancers and in experimental and clinical photobiology, it is limited by its subjective and qualitative nature. Self-reporting is prone to recall errors; evidence shows that individuals typically underestimate their UV skin sensitivity 2 and on repeat questioning a few months later, only two out of three self-classified in the same phototype 3. The Fitzpatrick skin type classification is also based on ethnic origin and is irrelevant for all skin types, especially non-Caucasian, i.e., African 4, Asian 5, Arab/Middle East 6 or Hispanic skin types 7 as well as multiethnic populations. Furthermore, due to unprecedented mixing of ethnic populations today, ethnic origin is no longer a representative criterion for classifying human populations.
Other more objective systems have been created to measure constitutive pigmentation. These include spectrometry and colorimetry 2 or skin color identification charts 8.
Currently, the main skin chromophores (melanin and hemoglobin) can be studied by three strategies based on reflectance technology: tristimulus colorimetry, specialized narrow-band reflectometry, and diffuse reflectance spectroscopy 9.
Table 1. Fitzpatrick skin type
| Skin type | Typical features | Tanning ability |
|---|---|---|
| I | White; very fair; red or blond hair; blue eyes; freckles | Always burns, never tans |
| II | White; fair; red or blond hair; blue, hazel, or green eyes | Usually burns, tans with difficulty |
| III | Cream white; fair with any eye or hair color; very common | Sometimes mild burn, gradually tans |
| IV | Brown; typically Mediterranean skin | Rarely burns, tans easily |
| V | Dark brown; Middle-Eastern skin types | Very rarely burns, tans darkly easily |
| VI | Black skin | Never burns, always tans darkly |
Causes of skin discoloration
Generally dark skin
- Acromegaly
- Addison disease
- Drug-induced pigmentation (phenothiazines, silver, chemotherapy)
- Hemochromatosis
- Ichthyosis
- Sézary syndrome
- Porphyria cutanea tarda
- Systemic sclerosis
- Wilson disease
Darker skin patches
- Acanthosis nigricans
- Alkaptonuria
- Becker nevus
- Berloque dermatitis
- Chloasma (melasma)
- Confluent and reticulated papillomatosis
- Congenital nevi
- Dark circles under the eyes
- Diffuse melanosis cutis
- Dowling-Degos disease
- Fixed drug eruption
- Erythema ab igne
- Erythrasma
- Flagellate erythema
- Freckles, lentigines
- Idiopathic eruptive macular pigmentation
- Laugier-Hunziker syndrome
- Lichen planus pigmentosa
- Lipodermatosclerosis
- Melanoma
- Moles
- Mongolian spot
- Morphoea (morphea)
- Naevi of Ota and Ito
- Neurofibromatosis
- Ochronosis
- Pigmented contact cheilitis
- Pigmented purpura
- Pityriasis versicolor (tinea versicolor)
- Poikiloderma of Civatte
- Postinflammatory (trauma, burns, skin disease)
- Prurigo pigmentosa
- Purpura
- Systemic sclerosis
- Tinea nigra
- Urticaria pigmentosa, mastocytosis
Pale or white skin/patches
- Albinism
- Atrophie blanche
- Bleaching creams
- Degos disease
- Griscelli syndrome
- Hermansky-Pudlak syndrome
- Halo moles
- Contact leukoderma
- Hypomelanosis of Ito
- Idiopathic guttate hypomelanosis
- Leprosy
- Leukoderma
- Lichen sclerosus
- Lupus erythematosus
- Topical medications including topical retinoids, topical steroids, benzoyl peroxide, azelaic acid, hydroquinone
- Morphoea
- Mycosis fungoides
- Nevus anemicus
- Nevus depigmentosus
- Piebaldism
- Pityriasis alba
- Pityriasis versicolor
- Poliosis
- Postinflammatory hypopigmentation (trauma, burns, skin disease especially atopic eczema, seborrhoeic dermatitis, discoid eczema, contact dermatitis, psoriasis, pityriasis rosea)
- Progressive macular hypopigmentation
- Sarcoidosis
- Systemic sclerosis
- Tinea corporis
- Tuberous sclerosis (ashleaf spots)
- Vitiligo
- Waardenburg syndrome
Generalized hyperpigmentation
Generalized hyperpigmentation or hypermelanosis may rarely arise from excessive circulating melanocyte stimulating hormone (MSH), when it often has a bronze hue. It occurs:
- In 95% of patients with Addison disease when it is more prominent on pressure areas, in skin folds, on scars and within the mouth
- In 90% of patients with hemochromatosis, when it is more prominent on the genitals, in skin folds and on sun-exposed sites
- Rarely in metastatic melanoma: diffuse melanosis cutis
- In people treated with afamelanotide
A differential diagnosis is carotenaemia, in which the skin colour takes on a yellow-orange hue due to ingestion of coloured vegetables.
Localized hyperpigmentation
Localized pigmentation may be due to melanin, hemosiderin or externally-derived pigment.
If dark patches are observed, the main diagnoses to consider are:
- Benign pigmented skin lesions, such as café-au-lait macules, melanocytic nevi (moles), freckles (ephelides), seborrheic keratoses and solar lentigines
- Skin cancers, such as melanoma and precursors and pigmented basal cell carcinoma
- Post-inflammatory pigmentation due to prior injury, current or prior inflammatory skin disease such as eczema, especially in dark skinned individuals or fixed drug eruption
- Current or previous superficial skin infection, particularly pityriasis versicolor and erythrasma
- Chronic pigmentary disorders, particularly melasma (facial pigmentation)
- Photocontact dermatitis to certain plants
- Thickened skin (e.g., acanthosis nigricans or ichthyosis)
- Pigmented purpura due to bleeding into the skin, such as capillaritis or senile purpura
- Intentional or accidental tattoo.
White discoloration on skin
- Acquired (common)
- Vitiligo
- Pityriasis alba
- Tinea versicolor
- Postinflammatory hypopigmentation
- Congenital (uncommon)
- Albinism
- Piebaldism
- Tuberous sclerosis
- Hypomelanosis of Ito
Common skin discoloration disorders
Skin discoloration or skin pigmentation disorders of the skin are commonly benign and easily distinguishable based on appearance and location, it may be necessary to perform a skin biopsy to exclude melanoma and its precursors 10. Some skin discoloration disorders result in cosmetic or psychological concerns to the patient, necessitating evaluation and treatment.
Typical skin hyperpigmentation disorders include post-inflammatory hyperpigmentation, melasma, solar lentigines, ephelides (freckles), and café au lait macules. These conditions are generally benign but can be distressing to patients. Appropriate dermatologic history, skin examination, and skin biopsy, when appropriate, can help exclude melanoma and its precursors.
In addition to addressing the underlying condition, skin hyperpigmentation is treated with topical agents, chemical peels, cryotherapy, light or laser therapy, or a combination of these methods. Café au lait macules are treated with surgical excision or laser therapy if treatment is desired.
Skin hypopigmentation disorders include vitiligo, pityriasis alba, tinea versicolor, and postinflammatory hypopigmentation. Treatment of vitiligo depends on the distribution and extent of skin involvement, and includes topical corticosteroids and calcineurin inhibitors, ultraviolet A therapy (with or without psoralens), narrowband ultraviolet B therapy, and cosmetic coverage. Patients with stable, self-limited vitiligo may be candidates for surgical grafting techniques, whereas those with extensive disease may be candidates for depigmentation therapy to make skin tone appear more even. Other hypopigmentation disorders may improve or resolve with treatment of the underlying condition.
Skin discoloration pathophysiology
Pigmentation of skin depends on the amount and type of melanin, degree of skin vascularity, presence of carotene, and thickness of the stratum corneum.
- Skin hyperpigmentation usually results from an increased number, or activity, of melanocytes. Epidermal increases in melanin usually enhance with a Wood lamp, whereas dermal increases do not. Some disorders, such as melasma, may have dermal and epidermal changes and can be classified as mixed 11.
- Hypopigmentation of skin may result from a reduction of melanocytes or from an inability of the melanocytes to produce melanin or properly transport melanosomes. Causes of hyper- and hypopigmentation are discussed in this article and are listed in Table 1. Certain skin pigmentation disorders are more common in certain skin types. The most commonly used system for identifying skin types is the Fitzpatrick system (Table 2).2,3
Table 2. Summary of Common Pigmentation Disorders
| Disorder | Description | Location | Cause | Treatment |
|---|---|---|---|---|
Postinflammatory hyperpigmentatin | Irregular, darkly-pigmented macules or patches | Previous sites of injury or inflammation | Trauma, inflammation | Hydroquinone (Eldoquin Forte), azelaic acid (Azelex), retinoids, chemical peels, laser therapy; combination therapy is most effective |
Melasma | Pigmented, well-defined macules; light brown, brown, or gray in color | Face (63 percent centrofacial, 21 percent malar, 16 percent mandibular), forearms | Pregnancy, oral contraceptives, phenytoin (Dilantin), idiopathic | Sunscreen; combinations of: hydroquinone, retinoids, glycolic acid peels, topical steroids; laser therapy, intense pulsed light therapy for dermal lesions |
Solar lentigines | 1- to 3-cm macules, well-circumscribed, light yellow to dark brown, variegated color | Face, hands, forearms, chest, back, shins | Acute, chronic ultraviolet light exposure | Hydroquinone, retinoids, chemical peels, laser therapy, cryotherapy |
Ephelides | 1- to 2-mm, shaply defined macules, red to tan to light brown in color | Childhood onset, face, neck, chest, arms, legs | Sun exposure in susceptible persons (i.e., skin types I to II) | None needed; fades in winter months |
Café-au-lait macules | Tan to brown patches, 1 to 20 cm, epidermal, present at birth or early childhood | Usually on trunk, but possible anywhere | Increased melanin in melanocytes, basal keratinocytes | Laser therapy, surgical excision; cosmetic treatment |
Vitiligo | Unpigmented macules and patches, sharply defined, 5 to 50 mm, coalescent | Face, hands, forearms, neck, genitalia, body folds, periorificial | Unknown, possibly immune-mediated | Sunscreens, concealers, dyes, topical steroids, oral psoralens with psoralen ultr]aviolet A-range, narrow-band ultraviolet-B therapy, depigmentation, grafting |
Hyperpigmentation Disorders
Postinflammatory hyperpigmentation
Postinflammatory hyperpigmentation also called acquired melanosis, is a common consequence of an injury (e.g. thermal burn) or inflammatory disorder (e.g. dermatitis, infection) of the dark skin (Fitzpatrick types IV to VI), resulting in lesions that can persist for months or years. A typical example can be seen in Figure 3. More severe injury results in postinflammatory hypopigmentation, which is usually permanent. Postinflammatory hyperpigmentation follows damage to the epidermis and/or dermis with deposition of melanin within the keratinocytes (skin cells) and/or dermis. Inflammation in the epidermis stimulates melanocytes to increase melanin synthesis and to transfer the pigment to surrounding keratinocytes (epidermal melanosis). If the basal layer is injured (e.g. lichen planus), melanin pigment is released and subsequently trapped by macrophages in the papillary dermis (dermal melanosis or pigment incontinence).
Postinflammatory hyperpigmentation can occur in anyone, but is more common in darker skinned individuals, in whom the colour tends to be more intense and persist for a longer period than in lighter skin colours. Pigmentation tends to more pronounced in sun-induced skin conditions such as phytophotodermatitis and lichenoid dermatoses (skin conditions with lichen planus-like inflammation, such as erythema dyschromicum perstans).
Some medications may also darken postinflammatory pigmentation. These include antimalarial drugs, clofazimine, tetracycline, anticancer drugs such as bleomycin (flagellate erythema), doxorubicin, 5-fluorouracil and busulfan.
Postinflammatory hyperpigmentation may also occur after laser therapy for other pigmented skin lesions, and may be transient or long lasting.
Postinflammatory hyperpigmentation be psychologically devastating to some patients.
Postinflammatory hyperpigmentation presents as irregular, darkly pigmented macules and patches at sites of previous injury or inflammation. Treatment is often difficult, requiring prolonged courses of therapy and excellent patient compliance.
Figure 3. Postinflammatory pigmentation

Postinflammatory hyperpigmentation treatment
Available methods of treatment for postinflammatory hyperpigmentation include hydroquinone 3% or 4% (Eldoquin Forte) twice daily, azelaic acid 20% cream (Azelex) twice daily, salicylic or glycolic acid peels, retinoids, and laser therapy. However, monotherapy often produces unsatisfactory results. In one study, the addition of serial glycolic acid peels to a hydroquinone 2%/glycolic acid 10% combination twice daily and tretinoin 0.05% (Retin-A) at bedtime resulted in faster lightening without significant adverse effects 13. Additionally, retinoids such as tazarotene 0.1% cream (Tazorac) are well-tolerated and somewhat effective at reducing hyper-pigmentation and disease severity 14.
Pretreatment with topical therapies has been studied in patients with skin types I to III undergoing carbon dioxide laser resurfacing. No conclusive benefit was noted in one limited trial involving patients at the lowest risk for postin-flammatory hyperpigmentation 15. At present, no preventative measures have proven beneficial in any skin type.
Topical treatments for postinflammatory hyperpigmentation
A variety of topical treatments are available to lighten/bleach hyperpigmented lesions in epidermal hypermelanosis. Varying degrees of success are achieved but combinations of the treatments below are usually required for significant improvement.
- Hydroquinone
- Azelaic acid
- Cysteamine cream
- Vitamin C cream
- Tretinoin cream
- Corticosteroid creams
- Glycolic acid peels
- Others: kojic acid, arbutin, licorice extracts, mequinol, niacinamide, N-acetyl glucosamine, soy
Physical treatments for postinflammatory hyperpigmentation
Chemical peels, laser treatments and intense pulsed light therapies (IPL) may be helpful for epidermal pigmentation, but physical treatments may also aggravate it by injuring the epidermis.
These treatments are not effective in dermal hypermelanosis.
Melasma
Melasma is a chronic skin disorder that results in symmetrical, blotchy, brownish facial pigmentation. Melasma is a progressive, macular, nonscaling hypermelanosis of sun-exposed areas of the skin, primarily on the face and dorsal forearms. It is usually associated with pregnancy, oral contraceptives, or anticonvulsants (e.g., phenytoin [Dilantin]), or it may be idiopathic. Melasma affects women nine times more often than men, and it is more prominent in patients with skin types IV to VI (e.g., Asian, Middle Eastern, South American). It is usually asymptomatic, but it is often cosmetically distressing to the patient. Melasma typically presents in one of three patterns of distribution: centrofacial (63 percent), malar (21 percent), and mandibular (16 percent). It is usually, but not always, bilateral (Figure 4).
The cause of melasma is complex. The pigmentation is due to overproduction of melanin by the pigment cells, melanocytes, which is taken up by the keratinocytes (epidermal melanosis) and/or deposited in the dermis (dermal melanosis, melanophages). There is a genetic predisposition to melasma, with at least one-third of patients reporting other family members to be affected. In most people melasma is a chronic disorder.
Known triggers for melasma include:
- Sun exposure and sun damage—this is the most important avoidable risk factor
- Pregnancy—in affected women, the pigment often fades a few months after delivery
- Hormone treatments—oral contraceptive pills containing oestrogen and/or progesterone, hormone replacement, intrauterine devices and implants are a factor in about a quarter of affected women
- Certain medications (including new targeted therapies for cancer), scented or deodorant soaps, toiletries and cosmetics—these may cause a phototoxic reaction that triggers melasma, which may then persist long term
- Hypothyroidism (low levels of circulating thyroid hormone)
Melasma commonly arises in healthy, non-pregnant adults. Lifelong sun exposure causes deposition of pigment within the dermis and this often persists longterm. Exposure to ultraviolet radiation (UVR) deepens the pigmentation because it activates the melanocytes to produce more melanin.
Research is attempting to pinpoint the roles of stem cell, neural, vascular and local hormonal factors in promoting melanocyte activation.
Three types of melasma exist:
- Epidermal melasma:
- Well-defined border
- Dark brown color
- Appears more obvious under black light
- Responds well to treatment
- Dermal melasma:
- ill-defined border
- Light brown or bluish in color
- Unchanged under black light
- Responds poorly to treatment
- Mixed melasma:
- The most common type
- Combination of bluish, light and dark brown patches
- Mixed pattern seen under black light
- Partial improvement with treatment
Epidermal melasma tends to be light brown, enhancing under Wood lamp examination. Dermal melasma is usually grayish in color and nonenhancing. Mixed types are dark brown with variable enhancement.
Prevention of melasma involves decreasing exposure of susceptible skin to ultraviolet (UV) rays. Opaque sunblocks with titanium dioxide or zinc oxide are most effective, use broad-spectrum with very high protection factor (SPF 50+) sunscreen. There are transparent sunscreens containing these agents as well (e.g., Blue Lizard Sunscreen Sensitive SPF 30+, Neutrogena Sensitive Skin Sunblock 30+, Sol-bar Zinc Sunscreen SPF 38). Melasma that is induced by pregnancy or oral contraceptive use tends to fade within several months after delivery or medication cessation, so watchful waiting should be encouraged in these instances whenever possible.
Figure 4. Melasma

Melasma treatment
Melasma can be very slow to respond to treatment, especially if it has been present for a long time. Treatment may result in irritant contact dermatitis in patients with sensitive skin, and this can result in post-inflammatory pigmentation.
Generally a combination of the following measures is helpful.
Topical treatment with hydroquinone 3% or 4%, glycolic acid 10% peel, azelaic acid 20% cream, and retinoids (e.g., tretinoin 0.05% or 0.1% cream; adapalene 0.1% or 0.3% gel [Differin]) all have some effectiveness. Combination products with hydroquinone and retinoids, glycolic acid, or topical steroids seem to be somewhat more effective. Typically, treatment must be continued indefinitely to maintain effect 16. In one drug-company-sponsored study, a triple-combination treatment of fluocinonide 0.01%/hydroquinone 4%/tretinoin 0.05% cream (Tri-Luma) showed significantly greater effectiveness at improving dyspigmentation than treatment with any two of these ingredients combined, with mild side effects 17. Epidermal and mixed types are not often responsive to laser therapies and frequently result in significant postinflammatory hyperpigmentation; therefore, their use cannot be recommended. However, several small studies suggest that dermal or refractory/mixed-type melasmas may be effectively treated with laser therapy or by a combination of intense pulsed-light therapy and hydroquinone with sunscreen 18.
General measures
- Discontinue hormonal contraception.
- Year-round life-long sun protection. Wear a broad-brimmed hat.
- Use broad-spectrum very high protection factor (SPF 50+) sunscreen applied to the whole face daily, year-round. It should be reapplied every 2 hours if outdoors during the summer months. Sunscreens containing iron oxides are preferred, as they screen out some visible light as well as ultraviolet radiation.
- Alternatively or as well, use a make-up that contains sunscreen.
- Use a mild cleanser, and if the skin is dry, a light moisturiser.
- Cosmetic camouflage (make-up) is invaluable to disguise the pigment.
Topical therapy
Tyrosinase inhibitors are the mainstay of treatment. The aim is to prevent new pigment formation by inhibiting formation of melanin by the melanocytes.
- Hydroquinone 2–4% as cream or lotion, applied accurately to pigmented areas at night for 2–4 months. This may cause contact dermatitis (stinging and redness) in 25% of patients. It should not be used in higher concentration or for prolonged courses as it has been associated with ochronosis (a bluish grey discolouration similar to that seen in alkaptonuria).
- Azelaic acid cream, lotion or gel can be applied twice daily long term, and is safe in pregnancy. This may also sting.
- Kojic acid or kojic acid dipalmitate is often included in formulations, as it binds copper, required by L-DOPA (a cofactor of tyrosinase). Kojic acid can cause irritant contact dermatitis and less commonly, allergic contact dermatitis.
- The mechanism of action of cysteamine cream is unclear, but is thought to involve inhibition of tyrosinase. A study of 50 patients with melasma found cysteamine cream to be significantly more effective than placebo cream.
- Ascorbic acid (vitamin C) also acts through copper to inhibit pigment production. It is well tolerated but highly unstable, so is usually combined with other agents.
- Methimazole (antithyroid drug) cream has been reported to reduce melanin synthesis and pigmentation in hydroquinone-resistant melasma.
- New agents under investigation include zinc sulfate mequinol, arbutin and deoxyarbutin (from berries), licorice extract, rucinol, resveratrol, 4-hydroxy-anisole, 2,5-dimethyl-4-hydroxy-3(2H)-furanone and/or N-acetyl glucosamine
Other active compounds used for melasma include:
- Topical corticosteroids such as hydrocortisone. These work quickly to fade the colour and reduce the likelihood of contact dermatitis caused by other agents. Potent topical steroids are best avoided due to their potential to cause adverse effects.
- Soybean extract, which is thought to reduce the transfer of pigment from melanocytes to skin cells (keratinocytes) and to inhibit receptors.
- Tranexamic acid has been used experimentally for melasma as a cream or injected into the skin (mesotherapy), showing some benefit. It may cause allergy or irritation.
Superficial or epidermal pigment can be peeled off. Peeling can also allow tyrosinase inhibitors to penetrate more effectively. These must be done carefully as peels may also induce post-inflammatory pigmentation.
- Topical alpha hydroxyacids including glycolic acid and lactic acid, as creams or as repeated superficial chemical peels, remove the surface skin and their low pH inhibits the activity of tyrosinase.
- Topical retinoids, such as tretinoin (a prescription medicine) are effective. Tretinoin can be hard to tolerate and sometimes causes contact dermatitis. Do not use during pregnancy.
- Salicylic acid, a common peeling ingredient in skin creams, can also be used for chemical peels, but it is not very effective in melasma.
The most successful formulation has been a combination of hydroquinone, tretinoin, and moderate potency topical steroid. This has been found to result in improvement or clearance in up to 60–80% of those treated. Many other combinations of topical agents are in common use, as they are more effective than any one alone. However, these products are often expensive.
Oral treatment of melasma
Oral medications for melasma are under investigation, including tranexamic acid. Tranexamic acid is a lysine analogue that inhibits plasmin and is usually used orally to stop bleeding. It reduces production of prostaglandins, the precursors of tyrosine. In low dose, tranexamic acid has been reported to be effective and safe in the treatment of melasma, providing patients have been carefully selected and are at low risk of thromboembolic disease.
Glutathione is also under investigation as a systemic skin whitening agent, but has potentially serious adverse effects.
Devices used to treat melasma
The ideal treatment for melasma would destroy the pigment, while leaving the cells alone. Unfortunately, this is hard to achieve. Machines can be used to remove epidermal pigmentation but with caution—over-treatment may cause postinflammatory pigmentation. Patients should be pretreated with a tyrosinase inhibitor (see above).
Fractional lasers, Q-switched Nd:YAG lasers and intense pulsed light (IPL) appear to be the most suitable options. Several treatments may be necessary and post-inflammatory hyperpigmentation may complicate recovery.
Carbon dioxide or erbium:YAG resurfacing lasers, pigment lasers (Q-switched ruby and Alexandrite devices) and mechanical dermabrasion and microdermabrasion should be used with caution in the treatment of melasma.
What is the outcome of treatment of melasma?
Results take time and the above measures are rarely completely successful.
Unfortunately, even in those that get a good result from treatment, pigmentation may reappear on exposure to summer sun and/or because of hormonal factors. New topical and oral agents are being studied and offer hope for effective treatments in the future.
Solar lentigines
Solar lentigines (i.e., liver spots) are macular, 1- to 3-cm, hyperpigmented, well-circumscribed lesions on sun-exposed surfaces of the skin. Sometimes they are also known as an “old age spot” or “senile freckle”. Solar lentigines result from exposure to ultraviolet (UV) radiation, which causes local proliferation of melanocytes and accumulation of melanin within the skin cells (keratinocytes). Solar lentigos or lentigines are very common, especially in people over the age of 40 years. Solar lentigines vary in color from light yellow to dark brown, and they often have a variegated appearance. The face, hands, forearms, chest, back and shins are the most common locations, erupting after acute or chronic UV exposure. White or Asian persons are most likely to develop solar lentigines, especially those with skin types I to III and a tendency to freckle (Figure 5).
Solar lentigines result from a local proliferation of basal melanocytes and a subsequent increase in melanization, differing from freckles, which result from increased melanin production. Systemic disorders presenting with multiple lentigines may include Peutz-Jeghers syndrome (gastrointestinal hamartomas; buccal, lip, perioral, or digital macules; onset at birth or early childhood), LEOPARD syndrome (multiple lentigines, electrocardiogram abnormalities, ocular hypertelorism, pulmonic stenosis, abnormal genitalia, retarded growth, and sensorineural deafness), and LAMB syndrome (multiple lentigines, atrial and/or mucocutaneous myxomas, myxoid neurofibromas, ephelides, and blue nevi). Solar lentigines must be differentiated from premalignant lesions, such as pigmented actinic keratoses or lentigo maligna. Pigmented lesions with rapid growth or change, associated symptoms (e.g., pain, itching, easy or recurrent bleeding, poor healing), atypical lesions, or those with features suspicious for melanoma should be biopsied. Full thickness excisional biopsy or punch biopsy (for large lesions or those on the face or cosmetically sensitive area) is an acceptable method of biopsy in these instances. Solar lentigines can be distinguished clinically from flat seborrheic dermatoses or pigmented actinic keratoses by the absence of epidermal hyperkeratosis. Biopsy may facilitate diagnosis in uncertain cases.
Prevention of solar lentigines depends on limiting sun exposure, using sunscreen regularly (especially in patients with fair skin [types I to III] and those prone to freckling), and preventing sunburns, especially after 20 years of age.
Figure 5. Solar lentigines

Solar lentigines treatment
Treatment of solar lentigines consists of ablative therapies (e.g., chemical peels, cryotherapy, laser therapy) or topical therapies (e.g., hydroquinone, retinoids), and is summarized in Table 3. Chemical peels with 30% to 35% trichloroacetic acid (Trichlor) solution or brief (i.e., less than 10 seconds) cryotherapy with liquid nitrogen have resulted in significant lightening of lentigines, but data are limited on long-term improvements, and recurrences are common. Additionally, cryotherapy can be painful, and prolonged treatment is associated with hypopigmentation 19. Laser therapy for solar lentigines has shown benefit in at least one small, randomized controlled trial, with effectiveness superior to liquid nitrogen cryotherapy. The frequency-doubled Q-switched neodymium-doped yttrium aluminum garnet (ND: YAG) laser produced the best cosmetic results and was tolerated best. Postinflammatory hyperpigmentation is a known complication of laser therapy, and must be considered when determining the best treatment option for each patient 20.
Topical therapies for solar lentigines are also available. Hydroquinone has been available for more than 30 years and is moderately effective. Adverse effects to hydroquinone include hypersensitivity, acneiform eruptions, and, rarely, ochronosis (i.e., blotchy hyperpigmentation) 21. Additionally, the lightening effects of hydroquinone are slow (months), and relapse with medication discontinuation is the rule. More recently, a combination of mequinol/tretinoin (Solage) has been shown to be safe and effective in treating solar lentigines, and shows promise for prolonged maintenance 22. Retinoids such as tazarotene 0.1% cream and adapalene 0.1% or 0.3% gel may reduce the appearance of solar lentigines, but evidence is limited 23.
Table 3. Solar Lentigines Treatment
| Treatment | Type/dose | Side effects |
|---|---|---|
Chemical peels | 30% to 35% trichloroacetic acid (Trichlor) | Transient stinging, burning, pain |
Cryotherapy | Liquid nitrogen | Pain, hypopigmentation with prolonged exposure |
Laser therapy | Neodymium-doped yttrium aluminum garnet (ND: YAG) laser | Pain, postinflammatory hyperpigmentation, redness, textural changes, hypopigmentation |
Hydroquinone (Eldoquin Forte) | 3% to 4% topical | Hypersensitivity, acne, ochronosis |
Mequinol/tretinoin (Solage) | 2% mequinol/0.01% tretinoin topical solution | Redness, dryness, itching, sensitivity |
Retinoids | Tazarotene 0.1% cream (Tazorac); adapalene 0.1% or 0.3% gel (Differin) | Redness, dryness, itching, sensitivity |
Ephelides
Ephelides (i.e., freckles) are small, 1- to 2-mm, sharply defined macular lesions of uniform color, most often found on the face, neck, chest, and arms. Color may vary from red to tan to light brown, and they may vary in number from a few to hundreds. Onset is usually in childhood after sun exposure. They are asymptomatic. Treatment of these lesions is not usually necessary, as they tend to fade during winter months. Cosmetically, undesired lesions can be treated similarly to lentigines (i.e., cryotherapy, hydroquinone, azelaic acid, glycolic acid peels, and laser therapy). These lesions should be differentiated from juvenile lentigines (2 to 10 mm) and solar lentigines (2 to 20 mm), which usually arrive later in life.
Café-au-lait macules
Café-au-lait macules are tan or brown macules ranging in size from 1 to 20 cm, which are present at birth or occur early in life. They are epidermal in origin, representing an increase in melanin in melanocytes and basal keratinocytes. They may be found on any body part, but often are located on the trunk (Figure 6). Ten to 30 percent of the population has an isolated café-au-lait macule 24.
Café-au-lait macules are asymptomatic and require treatment for cosmesis only. Laser therapies and surgical excision are effective. More than six café-au-lait lesions (5 mm or larger, prepubertal; and 15 mm or larger, postpubertal) should raise suspicion for an underlying systemic disorder such as tuberous sclerosis, neurofibromatosis, Albright syndrome, or Fanconi anemia 25.
Figure 6. Café-au-lait macules
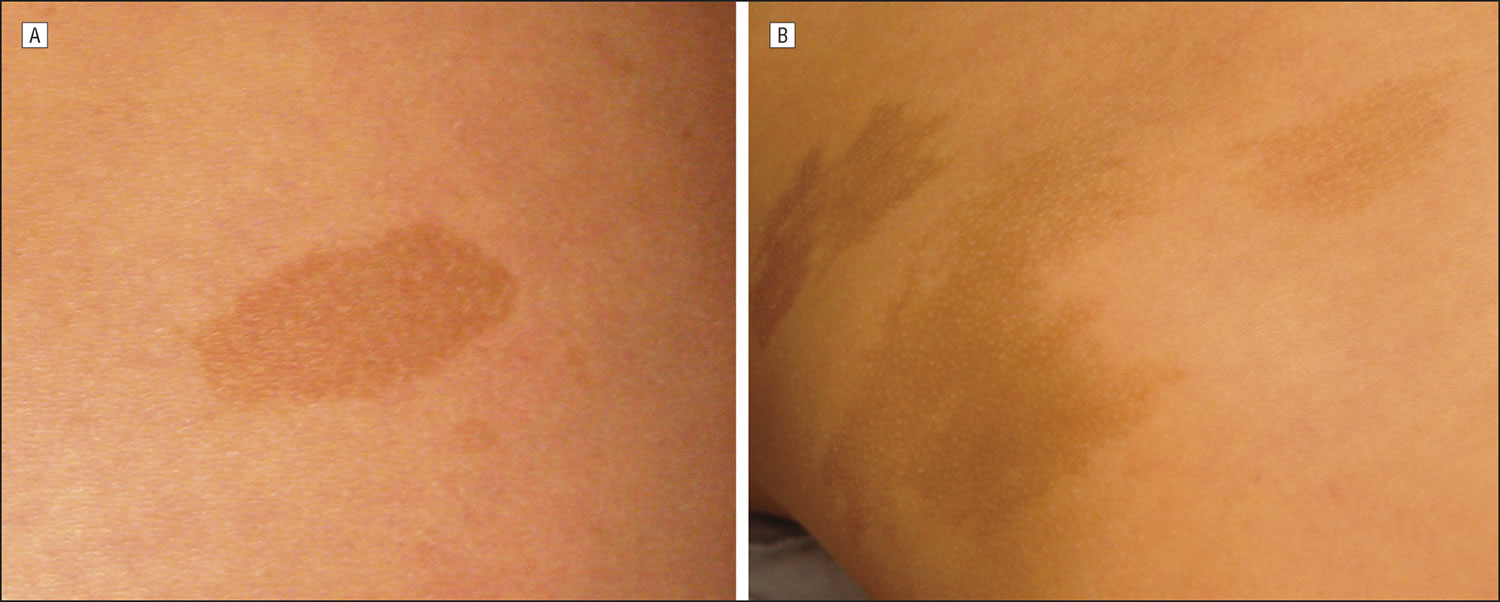
Footnote: Examples of a “typical” café au lait macule (CALM) with homogeneous pigmentation and regular borders (A) and an “atypical” CALM with irregular borders (B).
[Source 26 ]White discoloration on skin lesions
Vitiligo
Vitiligo is a disfiguring skin disease resulting in loss of pigmentation (melanocytes). Vitiligo results from an immune-mediated destruction of melanocytes (which are the cells that produce melanin). Melanin determines the color of skin, hair, and eyes. If melanocytes cannot form melanin or if their number decreases, skin color becomes progressively lighter. Vitiligo exact cause is unknown. Vitiligo affects all skin types and is generally considered a cosmetic condition, but it can cause significant psychological distress, particularly to some black patients.
Vitiligo is found in 1 percent of the general population. Vitiligo may be more common in India than elsewhere, with reports of up to 8.8% of the population affected. Family history of vitiligo is established in 25 to 30 percent of patients 24. Onset is often insidious, but is frequently related to a recent stress, illness, or trauma (e.g., sunburn). Peak onset is in the second and third decades of life. In 50% of sufferers, pigment loss begins before the age of 20, and in about 80% it begins before the age of 30 years 24. Males and females are equally affected.
Even though most people with vitiligo are in good general health, they face a greater risk of having autoimmune diseases such as diabetes, thyroid disease (in 20% of patients over 20 years with vitiligo), pernicious anaemia (B12 deficiency), Addison disease (adrenal gland disease), systemic lupus erythematosus, rheumatoid arthritis, psoriasis, and alopecia areata (round patches of hair loss).
A vitiligo-like leukoderma may occur in patients with metastatic melanoma. It can also be induced by certain drugs, such as immune checkpoint inhibitors (pembrolizumab, nivolumab) and BRAF inhibitors (vemurafenib, dabrafenib) used to treat metastatic melanoma. Vitiligo is also 3 times more common in haematology patients that have had allogeneic bone marrow and stem-cell transplants, than in the normal population.
Lesions in vitiligo consist of unpigmented, sharply defined macules ranging in size from 5 to 50 mm. Some will have a rim of hyperpigmentation or erythema. Common sites of involvement include the face, neck, dorsal hands, genitalia, body folds, and axillae (Figure 7). Perioral, periorbital, periumbilical, and perianal lesions also occur.
Four types of vitiligo exist:
- Generalized: Generalized vitiligo involves greater than 10 percent of the body surface area.
- Acral/acrofacial: Acral/acrofacial vitiligo typically involves the face and distal extremities (i.e., the so-called “tip/lip” pattern).
- Localized: Localized vitiligo tends to involve a smaller body surface area and is generally stable in nature.
- Segmental: Segmental (i.e., single dermatome or extremity) vitiligo is more often present in children and has a poorer prognosis for treatment.
Figure 7. Vitiligo

Vitiligo treatment
Treatment of vitiligo depends on the extent of the disease and the pattern of distribution. Lesions of the head and neck tend to be most responsive to treatment, whereas those on the extremities and genitalia tend to be more recalcitrant. Vitiligo treatments are summarized in Table 4.
Table 4. Vitiligo treatment
| Treatment | Examples and comments |
|---|---|
Sun protection | Hats, long-sleeved shirts, long pants, sunscreen |
Cosmetic coverage | Concealers (e.g., Dermablend, Covermark) |
Topical steroids | Topical steroid class II and III (e.g., betamethasone 0.05% [Diprolene], fluocinonide 0.05% [Lidex, brand no longer available in the United States]); head and neck most responsive to treatment |
Phototherapy | Topical or oral psoralens with psoralen ultraviolet A-range, narrow-band ultraviolet-B therapy |
Depigmentation | Monobenzone 20% cream (Benoquin) twice daily for six to 18 months |
Surgical grafting | Mini-graft, punch-graft techniques; for localized, stable disease |
Treatment is multifaceted and may involve sun protection, cosmesis, topical steroids and immune modifiers, topical and oral psoralens and psoralen ultraviolet A-range (PUVA) therapy, narrow-band ultraviolet-B (UV-B) therapy, depigmentation therapy, and surgical grafting techniques.
Sun protection is important for patients with vitiligo. Sunscreens that contain avobenzone (Parsol 1789) or titanium dioxide provide broad-spectrum UV protection and should be used regularly, because affected skin is especially sensitive to sun exposure. Sun-protective clothing (e.g., wide-brimmed hats, long-sleeved shirts, long pants) will limit UV exposure as well. Cosmetic concealers (e.g., Dermablend, Covermark), topical dyes, and sunless self-tanning products (best on skin types II and III) may reduce the disparity in pigmentation to a more acceptable level.
High-potency topical steroids (classes II and III) have been found to be beneficial in facilitating repigmentation (in limited disease), with the face and neck being the most responsive. For more extensive disease, other options (e.g., topical or oral psoralens with PUVA therapy, narrow-band UV-B therapy with or without tacrolimus [Protopic]) may prove beneficial 27.
Depigmentation therapy with monobenzone 20% cream (Benoquin) is reserved for patients with extensive (i.e., greater than 40 percent body surface area) involvements. Treatment is twice daily for six to 18 months, and patients must be counseled that its effects are irreversible, as melanocytes are permanently destroyed. Major side effects include contact or irritant dermatitis, pruritus, xerosis, and, less commonly, conjunctival melanosis and corneal pigment deposition. Sun protection is a mainstay of post-treatment care.
Patients with stable, localized vitiligo may elect to undergo surgical treatment of medically refractory lesions (e.g., hands, lips, genitalia). Multiple punch and mini-graft treatments are available 28.
Topical treatments
Topical treatments for vitiligo include:
- Corticosteroid creams. These can be used for vitiligo on trunk and limbs for up to 3 months. Potent steroids should be avoided on thin-skinned areas of face (especially eyelids), neck, armpits and groin.
- Calcineurin inhibitors (pimecrolimus cream and tacrolimus ointment. These can be used for vitiligo affecting eyelids, face, neck, armpits and groin.
- Experimental treatment with topical ruxolitinib, a janus kinase inhibitor, shows great promise for facial vitiligo.
Phototherapy
Phototherapy refers to treatment with ultraviolet (UV) radiation. Options include:
- Whole-body or localised broadband or narrowband (311 nm) UVB
- Excimer laser UVB (308 nm) or targeted UVB for small areas of vitiligo
- Oral, topical, or bathwater photochemotherapy (PUVA)
Phototherapy probably works in vitiligo by 2 mechanisms.
- Immune suppression—preventing destruction of the melanocytes
- Stimulation of cytokines (growth factors)
Treatment is usually given twice weekly for a trial period of 3–4 months. If repigmentation is observed, treatment is continued until repigmentation is complete or for a maximum of 1–2 years.
- Phototherapy is unsuitable for very fair skinned people.
- The treatment intensity aims for the vitiligo skin to be a light “carnation” pink
- If repigmentation is observed, treatment is continued until repigmentation is complete or for a maximum of 1–2 years.
- Treatment times are generally brief. The aim is to cause the treated skin to appear very slightly pink the following day.
- It is important to avoid burning (red, blistered, peeling, itchy or painful skin), as this could cause the vitiligo to get worse.
A meta-analysis included 35 unique studies reporting outcome after phototherapy for generalized vitiligo. Marked or clinically useful response was achieved in 36% after 12 months of narrowband UVB and in 62% after 12 months of PUVA. Face and neck responded better than trunk, which responded better than extremities. It was not very effective on hands and feet.
Systemic therapy
Systemic treatments for vitiligo include:
- Oral minocycline, a tetracycline antibiotic with anti-inflammatory properties
- Mini-pulses of oral steroids for 3 to 6 months, eg dexamethasone 2.5 mg, 2 days per week
- Subcutaneous afamelanotide
It is anticipated that monoclonal antibody biologic agents will be developed to treat vitiligo.
Surgical treatment of stable vitiligo
Surgical treatment for stable and segmental vitiligo requires removal of the top layer of vitiligo skin (by shaving, dermabrasion, sandpapering or laser) and replacement with pigmented skin removed from another site.
Techniques include:
- Non-cultured melanocyte-keratinocyte cell suspension transplantation.
- Punch grafting
- Blister grafts, formed by suction or cryotherapy
- Split skin grafting
- Cultured autografts of melanocytes grown in tissue culture
Depigmentation therapy
Depigmentation therapy, using monobenzyl ether of hydroquinone, may be considered in severely affected, dark skinned individuals.
Cyotherapy and laser treatment (eg 755 nm Q-switched alexandrite or 694 nm Q-switched ruby) have also been used successfully to depigment small areas of vitiligo.
Vitiligo results in reduced quality of life and psychological difficulties in many patients, especially in adolescents and in females. The psychosocial effects of vitiligo tend to be more severe in some countries, cultures and religions than in others. Family support, counselling and cognitive behavioral treatment (CBT) can be of benefit.
Other hypopigmentation disorders
Other disorders commonly associated with hypopigmentation include pityriasis alba, tinea versicolor, postinflammatory hypomelanosis (i.e., loss of melanin), atopic dermatitis, psoriasis, and guttate parapsoriasis. Additionally, it may also result from dermabrasion, chemical peels, and intralesional steroid therapy. A detailed description of these conditions is beyond the scope of this article and are described elsewhere 24.
Purple skin discoloration
Cherry hemangioma
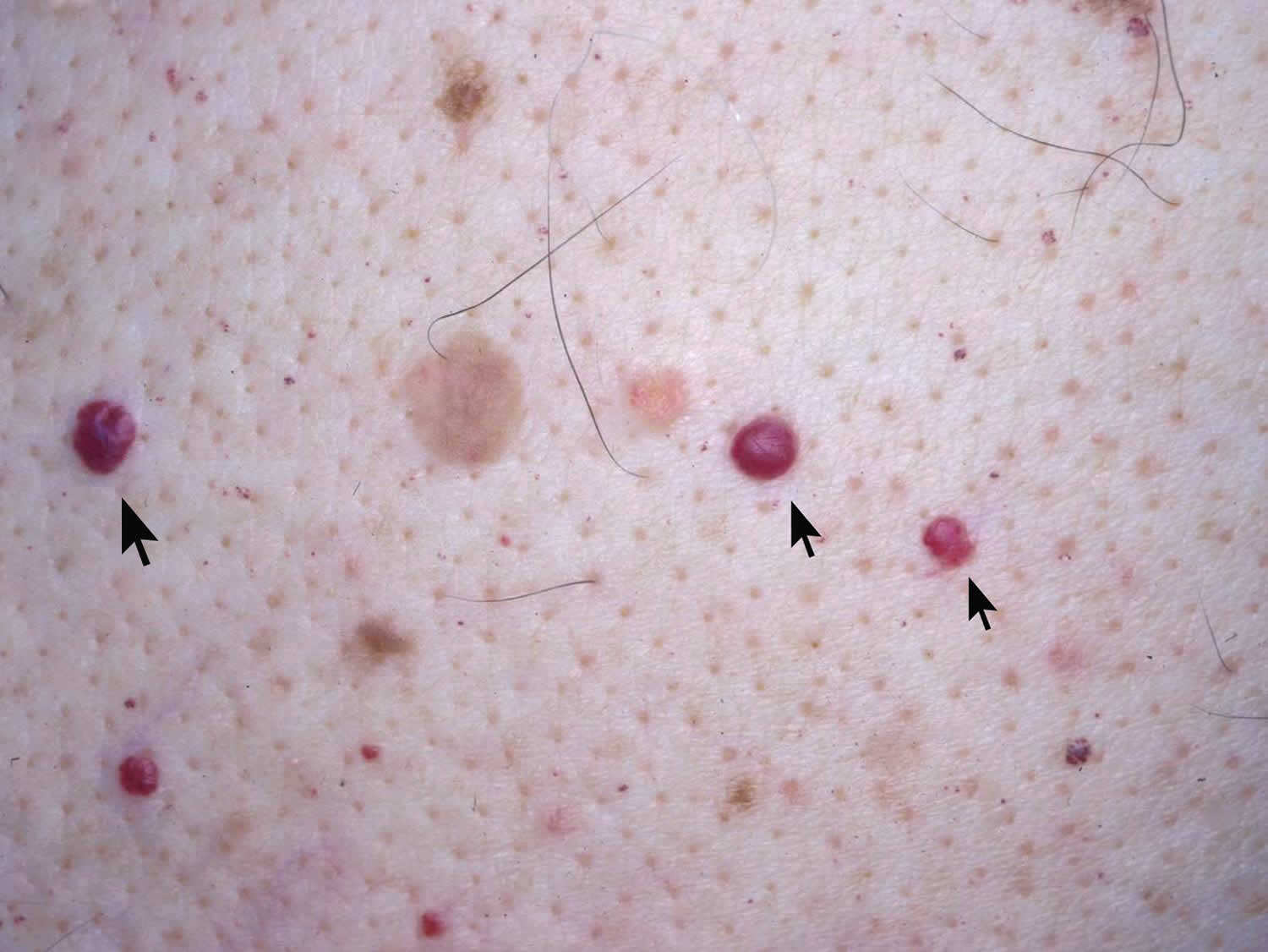
A cherry hemangioma also called cherry angioma or Campbell de Morgan spots, is a small (< 5 millimeter) non-cancerous, red-purple bump on the skin that is typically seen on the trunk in older adults (senile angioma), generally increasing in number with increasing age. Cherry hemangioma is formed from an overgrowth of capillaries that do not blanch (Figure 8). Their cause is unknown.
An angioma is due to proliferating endothelial cells; these are the cells that line the inside of a blood vessel. Microscopically the biopsy shows a well circumscribed sometimes lobular proliferation of capillaries with slightly thickened walls.
Cherry hemangiomas are found in individuals of all races and ethnic backgrounds. They occur more frequently with increasing age.
Cherry hemangiomas can arise in early life (infantile proliferative haemangioma) or later in life; the most common type of angioma is a cherry hemangioma.
Cherry angioma is usually diagnosed clinically and no investigations are necessary for the majority of lesions. It has a characteristic red-clod or lobular pattern on dermatoscopy (called lacunar pattern using conventional pattern analysis).
When there is uncertainty about the diagnosis, a biopsy may be performed. The angioma is composed of venules in a thickened papillary dermis. Collagen bundles may be prominent between the lobules.
Cherry hemangiomas typically require no treatment, although lesions that are irritated or bleeding (most commonly occurring due to injury) usually require removal. Cherry hemangioma lesions can also be removed if they are cosmetically undesirable.
Who gets cherry angioma?
Cherry angiomas are very common in males and females of any age or race. Cherry hemangiomas are more noticeable in white skin than in skin of color. They markedly increase in number from about the age of 40. There may be a family history of similar lesions. Eruptive cherry angiomas have been rarely reported to be associated with an internal malignancy.
Cherry hemangiomas signs and symptoms
Cherry hemangioma is a small, firm red, blue or purple dot to larger bright-cherry-red bump (papule), 0.1–1 cm in diameter. Sometimes cherry hemangiomas are more purple than red in color. When thrombosed (clotted), they can appear black in color until evaluated with a dermatoscope when the red or purple color is more easily seen. Cherry angioma may develop on any part of the body but most often appear on the scalp, face, lips and trunk. Rarely, a cherry hemangioma lesion demonstrates a dark brown to an almost black color.
Figure 8. Cherry hemangioma
Cherry hemangioma treatment
Cherry hemangiomas are harmless, so do not have to be treated. Occasionally, they are removed to exclude a malignant skin lesion such as nodular melanoma. Lesions may be surgically removed by cutting away the area (excision), burning away the area (electrocautery), vascular laser, or freezing the area (cryosurgery).
Salmon patch
Salmon patches are very common birthmark and occur in about 40-70% of all newborns. It is thought that salmon patches do not run in families. Salmon patches may also be called angel kisses (when they are on the baby’s face) and stork bites (when they are on the back of the baby’s neck). Salmon patches are caused by expansions (dilations) in tiny blood vessels called capillaries. Salmon patches are usually small flat patches of pink or red skin with poorly defined borders. Salmon patches are commonly found at the nape of the neck (stork bite, erythema nuchae), on the forehead between the eyebrows (angel’s kiss) or on the eyelids. Angel kisses tend to fade by age 1–2 (although some parents report that, for years, when their child cries, the angel kiss temporarily darkens and becomes apparent again), and stork bites tend to not go away at all and may remain unchanged into adult life in 50% of cases but are usually covered by the hair on the back of the head. Salmon patches are different from port-wine stains (discussed below) in that salmon patches do not grow larger or darker and are not associated with any syndromes involving the brain or development. Salmon patches are always noncancerous. It is sometimes difficult to tell the difference between a salmon patch and a port-wine stain.
In the past, port-wine stains and salmon patches were considered to be variations of the same kind of birthmark, but now it is now known that port-wine stains are truly malformations of capillaries and will never improve on their own, while salmon patches are temporary dilatations (expansions) of capillaries that do typically improve on their own.
There is no self-care required for a salmon patch. Treat the skin as you would any other part of the baby, with careful gentle cleansing and moisturization.
Salmon patches signs and symptoms
Salmon patches are diagnosed by their appearance. They are pink or red, flat, irregularly shaped patches that appear on the baby’s face or the back of the neck. On the face, they are commonly found between the eyebrows or on one of the eyelids. Salmon patches are never painful or itchy.
Figure 9. Salmon patch

Salmon patches treatment
There is no treatment necessary for a salmon patch. Salmon patches on the face almost always go away on their own within a year or two. The skin of the salmon patch should behave just like the skin on the rest of the baby; if the skin bleeds, develops cracks, if the area becomes darker or more raised or displays any other problems, contact your child’s doctor for further advice.
Port-wine stain
A port-wine stain is a type of birthmark that is caused by a malformation of tiny blood vessels called capillaries. The name port-wine stain comes from the color of the birthmark, which ranges from light pink to a dark red color. Port-wine stains are much less common than salmon patches, occurring in approximately 1 in 1,000 newborns. A port wine stain is usually a large flat patch of purple or dark red skin with well-defined borders. At birth the surface of the port-wine stain is flat, but in time it becomes bumpy and often more unsightly. The face is most commonly affected although they can occur anywhere on the body. Where present, they generally appear on one side of the body with a sharp mid-line cut-off.
Some port wine stains may fade over time but most remain unchanged or may even deepen in color. They do not shrink by themselves or disappear spontaneously. If the port-wine stain affects the face and neck, it may have a severe impact on the child’s social, psychological and economic development.
Like salmon patches, port-wine stains start as flat, pink or red patches; the difference between these birthmarks is that salmon patches tend to fade in the first year of life while port-wine stains become darker and grow along with the baby.
In the past, port-wine stains and salmon patches were considered to be variations of the same kind of birthmark, but now it is now known that port-wine stains are truly malformations of capillaries and will never improve on their own, while salmon patches are temporary dilatations (expansions) of capillaries that do typically improve on their own.
Port-wine stains and salmon patches birthmarks are noncancerous, but port-wine stains are sometimes associated with other syndromes involving the brain and development. Klippel-Trenaunay syndrome involves malformations of the veins (venous malformations), port-wine stains (capillary malformations), and excessive growth of the soft tissues. Additionally, some individuals with Klippel-Trenaunay syndrome have one limb that is longer and larger than the other limb. The syndrome is most frequently diagnosed in infancy or early childhood.
Port-wine stains are always present at birth, though they may change in appearance as the baby gets older and grows. There is no known association within families (genetic tendency) at this time. Due to their similarity, it is important to note that salmon patches are much more common, and about 7 in 10 babies will have one of these.
Port-wine stains signs and symptoms
Port-wine stains are never painful or itchy. It is sometimes difficult to tell the difference between a port-wine stain and other birthmarks, such as a salmon patch or a hemangioma, but it can be diagnosed by your child’s doctor, based on its appearance.
Figure 9. Port-wine stain

Port-wine stains treatment
Your child’s doctor will likely advise you to wait and see how the patch develops; if a port-wine stain is very large or on the baby’s face, however, he/she will likely recommend that your baby have further testing to make sure that there are no associated syndromes that might involve the brain or the baby’s development and will also recommend that you see a dermatologist in order to begin planning treatment. There is no treatment necessary for a port-wine stain, but some people are bothered by the appearance – particularly if it occurs on the face – and will choose to begin treatment earlier rather than later. The treatment usually involves laser therapy of the skin.
How to fix skin discoloration
Hyperpigmentation treatment
If pigmentation due to melanin affects an exposed site, daily application of broad-spectrum SPF 50+ sunscreen is important to minimize darkening caused by UV radiation. This is not effective for melanin residing in the dermis or to reduce pigmentation caused by carotene, drug or tattoo.
Cosmetic camouflage can be used.
The following agents can be used to lighten epidermal melanosis, alone or, more effectively, in combination:
- Hydroquinone
- Topical retinoid
- Topical corticosteroid
- Glycolic acid and other fruit acids
- Azelaic acid
- L-Ascorbic acid (vitamin C)
Resurfacing using chemical peels, laser (especially picosecond laser), intense pulsed light or dermabrasion may be effective but unfortunately risks further damage to the epidermis and formation of more pigment. Cautious cryotherapy to small areas of postinflammatory pigmentation can be effective but risks causing permanent hypopigmentation.
Cosmetic camouflage using make-up is sometimes the best advice.
Generalized hypopigmentation
Generalized reduction in melanin pigmentation at birth (congenital) may be racial in origin or due to albinism. Pituitary failure resulting in lack of melanocyte stimulating hormone (MSH) rarely results in acquired generalized hypomelanosis.
Pallor is much more frequently due to blood loss or anemia.
Localized hypopigmentation
Localized hypopigmentation may be due to partial or complete loss of melanin (achromoderma or leukoderma). Localized hypopigmentation can be congenital or a acquired.
If single or multiple pale or white patches are observed, the main diagnoses to consider are:
- Halo nevus
- Vitiligo
- Congenital piebaldism and Waardenburg syndrome (with deafness)
- Pityriasis alba
- Pityriasis versicolor
- Idiopathic guttate hypomelanosis
- Progressive macular hypomelanosis
- Postinflammatory hypopigmentation or scarring
- Lichen sclerosus
- Leprosy
The hypopigmentation due to inflammatory skin disorders and infections usually resolves by itself over weeks to months once the underlying disorder has been cleared. There is no effective treatment for achromia due to scarring. The response of vitiligo to therapy is highly variable.
References- The validity and practicality of sun-reactive skin types I through VI. Fitzpatrick TB. Arch Dermatol. 1988 Jun; 124(6):869-71.
- Comparing alternative methods of measuring skin color and damage. Daniel LC, Heckman CJ, Kloss JD, Manne SL. Cancer Causes Control. 2009 Apr; 20(3):313-21.
- Objective determination of Fitzpatrick skin type. Ravnbak MH. Dan Med Bull. 2010 Aug; 57(8):B4153.
- Measuring skin cancer risk in African Americans: is the Fitzpatrick Skin Type Classification Scale culturally sensitive? Pichon LC, Landrine H, Corral I, Hao Y, Mayer JA, Hoerster KD. Ethn Dis. 2010 Spring; 20(2):174-9.
- The difference between the constitutive and facultative skin color does not reflect skin phototype in Asian skin. Choe YB, Jang SJ, Jo SJ, Ahn KJ, Youn JI. Skin Res Technol. 2006 Feb; 12(1):68-72.
- Correlating skin phototype and minimum erythema dose in Arab skin. Venkataram MN, Haitham AA. Int J Dermatol. 2003 Mar; 42(3):191-2.
- Sun sensitivity in 5 US ethnoracial groups. Galindo GR, Mayer JA, Slymen D, Almaguer DD, Clapp E, Pichon LC, Hoerster K, Elder JP. Cutis. 2007 Jul; 80(1):25-30.
- Development and validation of a new Skin Color Chart. de Rigal J, Abella ML, Giron F, Caisey L, Lefebvre MA. Skin Res Technol. 2007 Feb; 13(1):101-9.
- Del Bino S, Duval C, Bernerd F. Clinical and Biological Characterization of Skin Pigmentation Diversity and Its Consequences on UV Impact. Int J Mol Sci. 2018;19(9):2668. Published 2018 Sep 8. doi:10.3390/ijms19092668 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6163216/
- Pigmentation Disorders: Diagnosis and Management. Am Fam Physician. 2017 Dec 15;96(12):797-804. https://www.aafp.org/afp/2017/1215/p797.html
- Stulberg DL, Clark N, Tovey D. Common hyperpigmentation disorders in adults: Part I. Diagnostic approach, café-au-lait macules, diffuse hyper-pigmentation, sun exposure, and phototoxic reactions. Am Fam Physician. 2003;68(10):1955–1960.
- Common Pigmentation Disorders. Am Fam Physician. 2009 Jan 15;79(2):109-116. https://www.aafp.org/afp/2009/0115/p109.html
- Burns RL, Prevost-Blank PL, Lawry MA, Lawry TB, Faria DT, Fivenson DP. Glycolic acid peels for postinflammatory hyperpigmentation in black patients. A comparative study. Dermatol Surg. 1997;23(3):171–175.
- Grimes P, Callender V. Tazarotene cream for postinflammatory hyper-pigmentation and acne vulgaris in darker skin: a double-blind, randomized, vehicle-controlled study. Cutis. 2006;77(1):45–50.
- West TB, Alster TS. Effect of pretreatment on the incidence of hyperpigmentation following cutaneous CO2 laser resurfacing. Dermatol Surg. 1999;25(1):15–17.
- Erbil H, Sezer E, Tastan B, Arca E, Kurumlu Z. Efficacy and safety of serial glycolic acid peels and a topical regimen in the treatment of recalcitrant melasma. J Dermatol. 2007;34(1):25–30.
- Torok H, Taylor S, Baumann L, et al. A large 12-month extension study of an 8-week trial to evaluate the safety and efficacy of triple combination (TC) cream in melasma patients previously treated with TC cream or one of its dyads. J Drugs Dermatol. 2005;4(5):592–597.
- Wang CC, Hui CY, Sue YM, Wong WR, Hong HS. Intense pulsed light for the treatment of refractory melasma in Asian persons. Dermatol Surg. 2004;30(9):1196–1200.
- Lugo-Janer A, Lugo-Somolinos A, Sanchez JL. Comparison of trichloroacetic acid solution and cryosurgery in the treatment of solar lentigines. Int J Dermatol. 2003;42(10):829–831.
- Wang CC, Sue YM, Yang CH, Chen CK. A comparison of Q-switched alexandrite laser and intense pulsed light for the treatment of freckles and lentigines in Asian persons: a randomized, physician-blinded, split-face comparative trial. J Am Acad Dermatol. 2006;54(5):804–810.
- Draelos ZD. Novel approach to the treatment of hyperpigmented photo-damaged skin: 4% hydroquinone/0.3% retinol versus tretinoin 0.05% emollient cream. Dermatol Surg. 2005;31(7 pt 2):799–804.
- Jarratt M. Mequinol 2%/tretinoin 0.01% solution: an effective and safe alternative to hydroquinone 3% in the treatment of solar lentigines. Cutis. 2004;74(5):319–322.
- Kang S, Kreuger GG, Tanghetti EA, et al., for the Tazarotene Cream in Photodamage Study Group. A multicenter, randomized, double-blind trial of tazarotene 0.1% cream in the treatment of photodamage. J Am Acad Dermatol. 2005;52(2):268–274.
- Fathman EM, Habif TP. Skin Disease: Diagnosis and Treatment. 1st ed. St. Louis, Mo.: Mosby; 2001:58,184–186,308–311,469.
- Fitzpatrick TB. Fitzpatrick’s Dermatology in General Medicine. 4th ed. New York, NY: McGraw-Hill; 1993:966–968,1694,1984.
- Nunley KS, Gao F, Albers AC, Bayliss SJ, Gutmann DH. Predictive Value of Café au Lait Macules at Initial Consultation in the Diagnosis of Neurofibromatosis Type 1. Arch Dermatol. 2009;145(8):883–887. doi:10.1001/archdermatol.2009.169 https://jamanetwork.com/journals/jamadermatology/fullarticle/712161
- Whitton ME, Ashcroft DM, Barrett CW, Gonzalez U. Interventions for vitiligo. Cochrane Database Syst Rev. 2006;(1):CD003263.
- Barman KD, Khaitan BK, Verma KK. A comparative study of punch grafting followed by topical corticosteroid versus punch grafting followed by PUVA therapy in stable vitiligo. Dermatol Surg. 2004;30(1):49–53.





{kind=link}