Sphenoid sinus
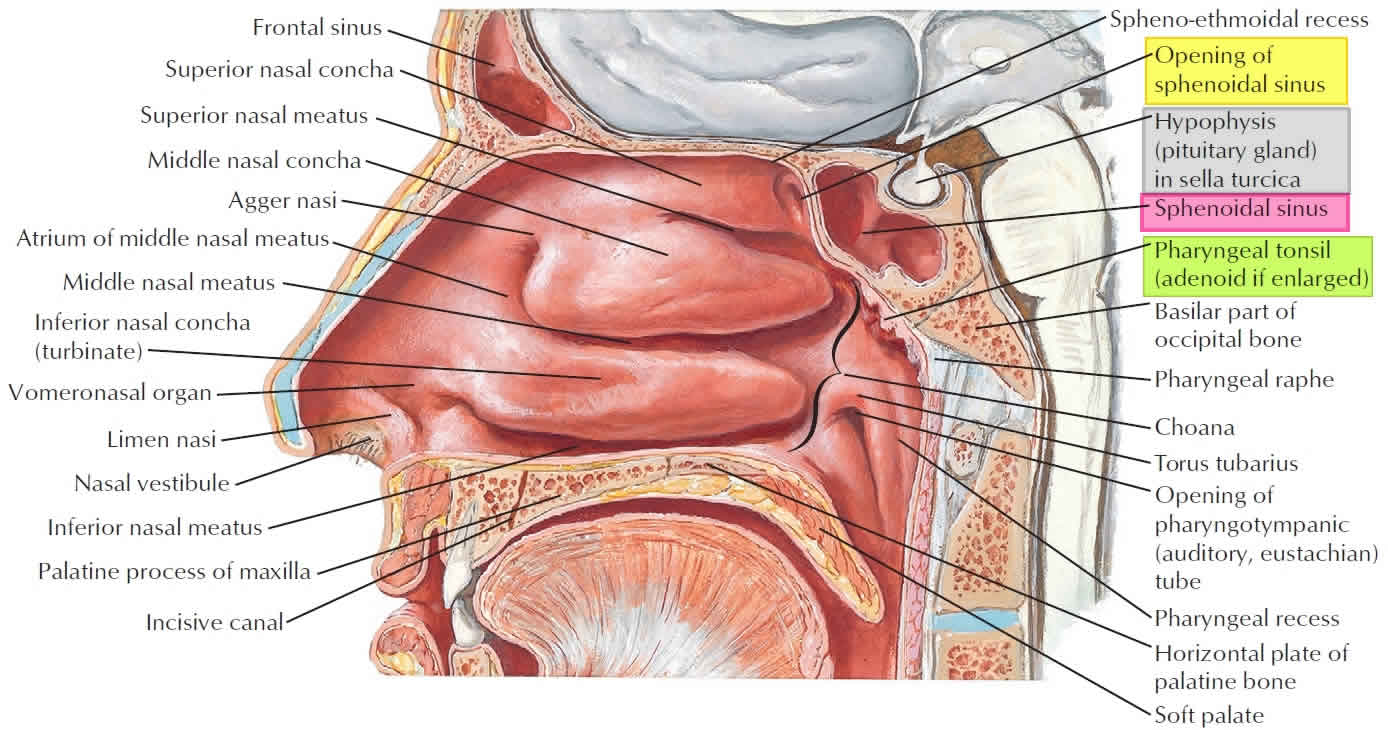
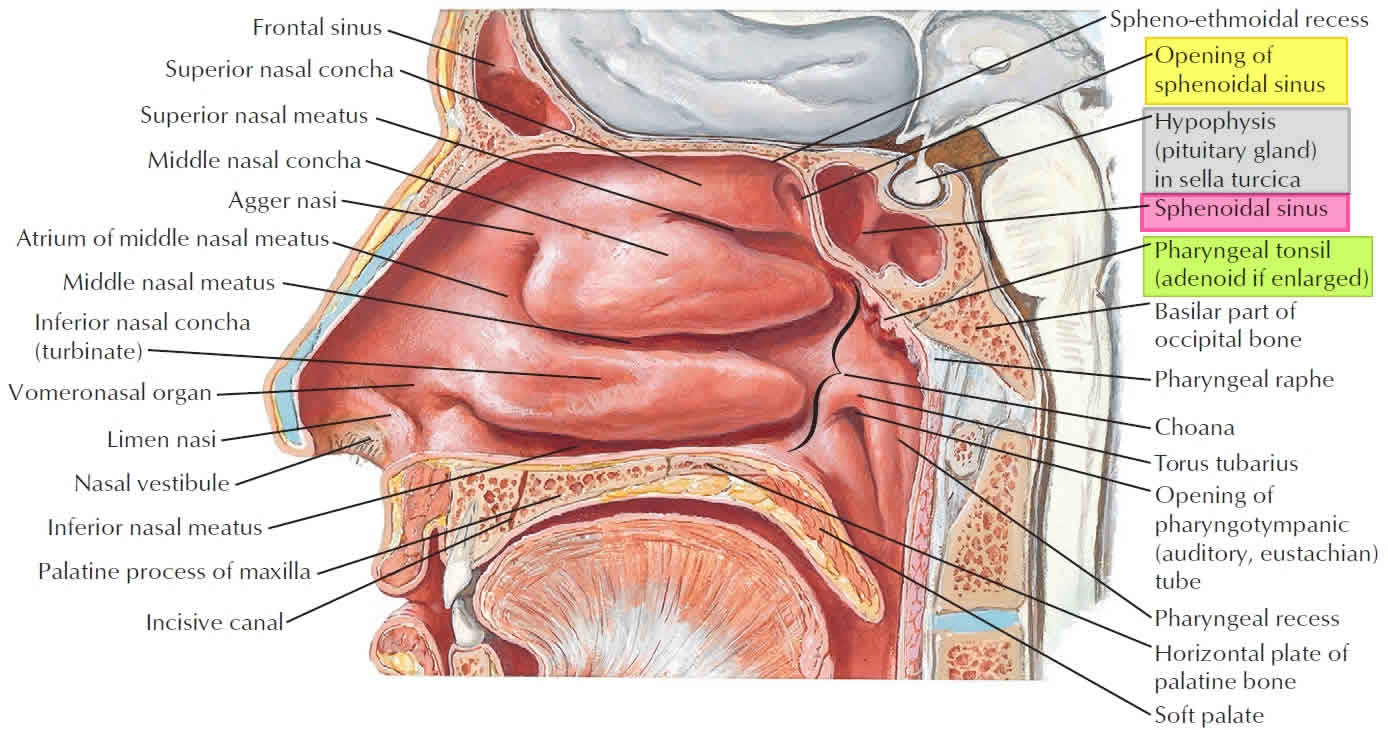
The sphenoid sinus is the most posterior paranasal sinus. The sphenoid sinuses are paired spaces formed within the body of the sphenoid bone, communicating with the roof of the nasal cavity via the sphenoethmoidal recess in its anterior wall (Figure 1). The apertures are high on the anterior walls of the sphenoid sinuses. The two sinuses are separated by a septum which may or may not be in the midline. The sphenoid sinus usually lies anteroinferior to the sella.
A large sinus can show a number of ridges and depressions related to closely adjacent structures. These can include the pituitary gland, optic nerve and internal carotid artery.
- Sphenoid sinus location: the central body of the sphenoid bone anteroinferior to the sella turcica
- Sphenoid sinus blood supply: posterior ethmoidal and sphenopalatine arteries
- Sphenoid sinus innervation: posterior ethmoidal nerve and orbital branch of pterygopalatine ganglion
The sphenoidal sinuses are related:
- above to the cranial cavity, particularly to the pituitary gland and to the optic chiasm,
- laterally, to the cranial cavity, particularly to the cavernous sinuses, and
- below and in front, to the nasal cavities.
Because only thin shelves of bone separate the sphenoidal sinuses from the nasal cavities below and hypophyseal fossa above, the pituitary gland can be surgically approached through the roof of the nasal cavities by passing first through the anteroinferior aspect of the sphenoid bone and into the sphenoidal sinuses and then through the top of the sphenoid bone into the hypophyseal fossa.
Innervation of the sphenoidal sinuses is provided by:
- the posterior ethmoidal branch of the ophthalmic nerve [V1] . and
- the maxillary nerve [V 2] via orbital branches from the pterygopalatine ganglion.
The sphenoidal sinuses are supplied by branches of the pharyngeal arteries from the maxillary arteries.
Relations
- superiorly: cavernous sinus, sella turcica and its contents
- inferiorly: nasal cavities
- anteriorly: nasal cavities, posterior ethmoid air cells
- posteriorly: contents of the middle cranial fossa
- laterally: cavernous sinus, cranial cavity
Types of pneumatization
- conchal
- lateral recess
- presellar
- sellar (which can be incomplete or complete)
The sphenoid sinuses are central aerations of the sphenoid bone that start developing at about 3 months’ gestation. Their development initiates as a vagination of the cartilaginous cupular process and continues to enlarge until the teenaged years.
Because of the high variability of sphenoid sinus pneumatization, the boundaries can differ from person to person.
The anterior boundaries of the sphenoid sinus are likely the most consistent. They include the sphenoid crest anterosuperiorly, which articulates with the perpendicular plate of the ethmoid bone, and the rostrum anteroinferiorly, which articulates with the vomer. The posterior boundaries of the sphenoid sinus usually include the sella turcica medially and cavernous sinuses laterally.
Hamberger 1 described 3 types of pneumatization based on its relationship to the sella turcica: conchal (rudimentary or absent sphenoid sinus), presellar (a posterior sphenoid sinus wall that is separated from sella by thick bone), and sellar (a posterior sphenoid sinus wall that is adjacent to sella). The most common configuration in his series was the sellar type, found in 86% of the population, compared to the presellar type (11%) and conchal type (3%).
Authors have described a quite common fourth configuration, postsellar type, in which sphenoid sinus extends beyond the sella turcica so that the sella forms a portion of the roof of the sphenoid sinus. In addition, the optic chiasm and internal carotid arteries are often intimately associated with posterior or lateral walls of sphenoid sinus.
The lateral limits of the sphenoid sinus vary greatly. The inferolateral area of the sphenoid sinus carries the vidian nerve, and the superolateral area carries V2 in foramen rotundum.
The lateral extent of the sphenoid sinus may extend to or beyond these nerves. The posterior septal branch of the sphenopalatine artery runs a few millimeters below the natural os of the sphenoid sinus.
Arterial supply
- posterior ethmoidal artery
- nasal branches of the sphenopalatine artery
Venous drainage
- superior ophthalmic veins via posterior ethmoidal veins
Lymphatic drainage
- Lymph drainage occurs via afferent vessels leading into the retropharyngeal nodes
Innervation
- parasympathetic: orbital branches of the pterygopalatine ganglion
- sensory: posterior ethmoidal nerve from the nasociliary nerve, a branch of the ophthalmic division of the trigeminal nerve
Variant anatomy
With respect to optic nerve relationship:
- type 1: adjacent to sphenoid sinus
- type 2: indenting the sinus
- type 3: traversing the sinus
- type 4: adjacent to posterior ethmoid sinus
Development
Pneumatization starts at around 2 years of age and it develops more slowly than the other paranasal sinuses.
Figure 1. Sphenoid sinus
Sphenoid sinus function
The total function of the paranasal sinuses is unclear 2. The cavities allow for the increase in the bony structure without adding significant mass. They also provide social cues that indicate such things as gender and sexual maturity. Respiratory mucosa lines the paranasal sinuses. This respiratory mucosa is ciliated and secretes mucus.
The sphenoidal sinuses are found in the body of the sphenoid. They open into the posterior wall of the sphenoid-ethmoidal recess.
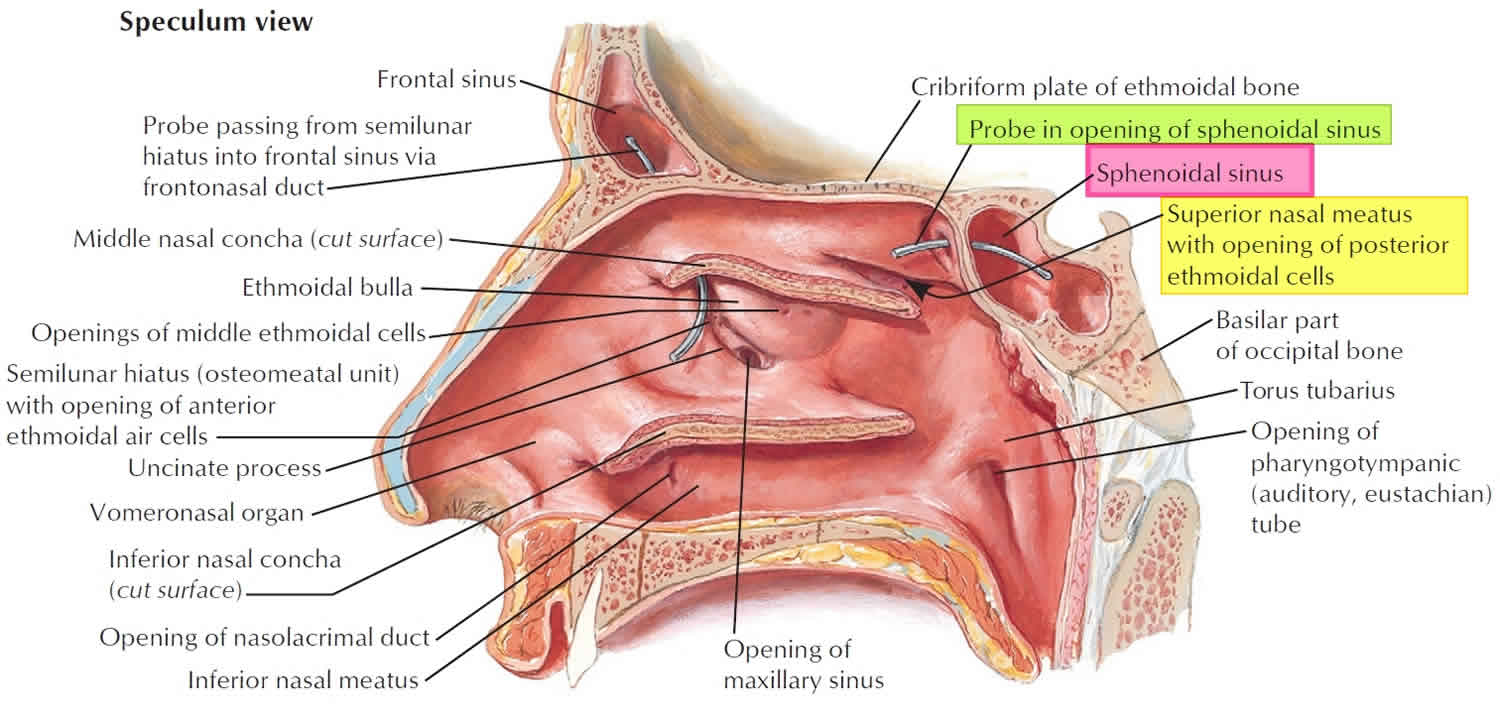
The ethmoid sinuses are found between the orbits. They typically are formed by a series of labyrinths which vary in number from 3 to 18. These ethmoidal air cells are divided regionally into anterior, middle and posterior, based on the location of their apertures. The anterior ethmoidal sinus opens into the ethmoidal infundibulum or the frontonasal duct. The middle group opens into the ethmoidal bulla or just superior to it. The posterior group opens onto the lateral wall of the superior nasal meatus.
The largest of the paranasal sinuses is the maxillary sinus. There are 2 pyramidal-shaped maxillary sinuses located bilaterally in the maxilla of the face. It fills the bone in its entirety to reduce the mass of the maxilla. The maxillary sinus opens into the center of the semilunar hiatus found in the lateral wall of the middle nasal meatus.
The triangular-shaped frontal sinuses are found in the frontal bone superior to the orbits. These sinuses vary in size. They open at the lateral wall of the middle meatus which then continues as the semilunar hiatus, which drains the maxillary sinus.
Sphenoid sinus infection
Sinusitis affects about 1 in 8 adults in the United States, resulting in over 30 million annual diagnoses 3. Sinusitis, also called rhinosinusitis because the symptoms involve both the nose and the sinuses, affects about one in eight adults annually. For many, the inflammation starts when viruses or bacteria infect your sinuses (often during a cold), and begin to multiply. Part of the body’s reaction to the infection causes the sinus lining to swell, blocking the channels that drain the sinuses. This causes mucus and pus to fill up the nose and sinus cavities. For others, the symptoms and inflammation may be the result of the nose and sinuses reacting to other things in the environment, but not be an infection.
Because sinusitis simply means inflammation of the sinuses, the word alone includes a variety of similar problems. Acute sinusitis is when the symptoms occur for less than four weeks. A diagnosis of chronic sinusitis requires that the symptoms last longer than 12 weeks. Sometimes these are caused by the same thing, but often chronic and acute sinusitis are very different from each other. Your primary care provider or an ENT (ear, nose, and throat) specialist, or otolaryngologist, can help sort out what type of sinusitis you have and how to treat it. Recurrent acute sinusitis is when someone has four or more sinus infections (acute sinusitis) in one year but does not have symptoms in between those infections.
Four sinusitis classifications:
- Acute rhinosinusitis: Sudden onset, lasting less than 4 weeks with complete resolution.
- Subacute rhinosinusitis: A continuum of acute rhinosinusitis but less than 12 weeks.
- Recurrent acute rhinosinusitis: Four or more episodes of acute, lasting at least 7 days each, in any 1-year period.
- Chronic rhinosinusitis: Signs of symptoms persist 12 weeks or longer.
What causes sinusitis?
Acute sinusitis is most commonly due to viruses or bacteria and is usually self-limiting. Approximately 90% of patients with colds have an element of viral sinusitis. Acute viral sinusitis is likely if you have been sick for less than 10 days and are not getting worse. Acute bacterial sinusitis is when you do not improve at all within 10 days of getting sick, or when you get worse within 10 days after beginning to get better. Those with atopy (allergy) commonly get sinusitis. It can be caused by allergens, irritants, viruses, fungi, and bacteria. Popular irritants are animal dander, polluted air, smoke, and dust.
Chronic sinusitis, however, is usually caused by prolonged inflammation, instead of a long infection. Infection can be a part of chronic sinusitis, especially when it worsens from time to time, but is not usually the main cause. The exact cause cannot always be determined; for some reason the nose and sinuses are overreacting to what they think is an infection.
There are higher rates of sinusitis in the South, Midwest, and among women. Children younger than 15 years of age and adults aged 25 to 64 years are affected the most 4.
Other risk factors or sinusitis include 4:
- Anatomic defects such as septal deviations, polyps, conchae bullosa, other trauma and fractures involving the sinuses or the facial area surrounding them
- Impaired mucous transport from diseases such as cystic fibrosis, ciliary dyskinesia
- Immunodeficiency from chemotherapy, HIV, diabetes mellitus, etc.
- Body positioning, intensive care unit (ICU) patients due to prolonged supine positioning that compromises mucociliary clearance.
- Rhinitis medicamentosa, toxic rhinitis, nasal cocaine abuse, barotrauma, foreign bodies
- Prolonged oxygen use due to drying of mucosal lining
- Patients with nasogastric or nasotracheal tubes
Are there any related conditions or complications?
Migraine headaches or tension headaches can cause symptoms of sinus pain or pressure. If you have sinus headaches without discolored drainage, talk to your primary care provider, or an ENT specialist, about the possibility of migraine headaches causing sinus pain or pressure and medications options for migraine treatment. Sometimes inflammation of the nasal cavity can also cause drainage and nasal congestion, but not involve your sinuses.
What are the symptoms of sinusitis?
You have acute sinusitis when you have had cloudy or colored drainage from your nose for up to four weeks, plus one or more of the following symptoms:
- Stuffy, congested, or blocked nose
- Pain, pressure, or fullness in the face, head, or around the eyes
- Long-lasting cold symptoms
- Symptoms that do not improve within 10 days of getting sick, or initially get better then worsen again
You might have chronic sinusitis if you have at least two of the four symptoms note below for at least 12 weeks. An ENT specialist would also need to see polyps, pus, or thickened mucous in nose, or get a CT scan, to fully diagnose chronic sinusitis. Possible symptoms include:
- Stuff congested, or blocked nose
- Pain, pressure or fullness in the face, head or around the eyes
- Thickened nasal drainage
- Loss of smell
Sinusitis diagnosis
No laboratory tests are indicated for acute uncomplicated sinusitis because the diagnosis is usually clinical. X-rays or CT scans of the sinuses are not necessary to diagnose uncomplicated sinusitis if you have the symptoms of sinusitis (discharge plus pressure or blockage). A plain sinus x-ray is most accurate for the maxillary, frontal, or sphenoid disease but is not useful for evaluating the anterior ethmoid cells or the ostiomeatal complex from which most sinus disease originates. Positive findings on plain films are air-fluid levels, sinus opacity, or mucosal thickening of 6 mm or more. Coronal CT at a thickness of 3 mm to 4 mm is the modality of choice. The CT findings suggestive of sinusitis are sinus opacification, air-fluid levels, sinus wall displacement, and 4 mm or greater mucosal thickening. Culture and biopsy are indicated for chronic bacterial and fungal sinusitis.
Sinusitis treatment options
Sinusitis is treated differently based on the cause. Most cases of acute sinusitis, about 98 percent, are caused by a virus, not bacteria, and should not be treated with antibiotics. Acute viral sinusitis may be treated using pain relievers such as acetaminophen or ibuprofen, steroid nasal sprays, or salt water irrigation in the nose. These treatments are also good options for acute bacterial sinusitis. Most people get better naturally from acute bacterial sinusitis, called “watchful waiting,” but some patients with acute bacterial sinusitis may get better faster with an antibiotic.
Antibiotics: Use empirically and based on community patterns of resistance. Ten to 14 days of amoxicillin or amoxicillin-clavulanate is first-line treatment. In some communities, amoxicillin effectiveness is less than 70%. Trimethoprim-sulfamethoxazole well for some, but there is a higher rate of resistance. Failure of symptoms to resolve after 7 days of therapy should prompt one to switch to a broader spectrum agent, such as ten to fourteen days of augmentin, cefuroxime axetil, other second or third-generation cephalosporins, clindamycin alone or along with ciprofloxacin, sulfamethoxazole, a macrolide, or one of the fluoroquinolones. Metronidazole may be added to any one of these agents to increase anaerobic coverage. For chronic sinusitis, antibiotics should cover S. aureus and be effective against the higher incidence of beta-lactamase producing organisms that are common in chronic disease. If the patient is not improving after 5 to 7 days, add metronidazole or clindamycin. Treat for 3 to 6 weeks.
Frontal or sphenoid sinusitis with air-fluid levels may require hospitalization with intravenous (IV) antibiotics. Patients who are immunocompromised or are toxic appearing require admission. Fungal sinusitis is associated with high morbidity and mortality.
Sinusitis may extend to the bones and soft tissues of the face and orbits. Facial cellulitis, periorbital cellulitis, orbital abscess, and blindness can develop. Sinusitis can lead to intracranial complications such as cavernous sinus thrombosis, epidural or subdural empyema, and meningitis.
Chronic sinusitis is treated differently than acute sinusitis. Because chronic sinusitis is caused more by inflammation than infection, the treatments for chronic sinusitis aim to control the inflammation. Salt water nasal irrigation and/or nasal steroid sprays are the main treatments for the symptoms of chronic sinusitis. Antibiotics may sometimes be helpful but not always.
Other factors, including allergies, nasal polyps, asthma, and problems with the body’s ability to fight infections, can go along with sinusitis and make it worse unless they are also treated.
Antihistamines are only of benefit in early allergic sinusitis. Topical steroids are used to diminish nasal mucosal edema but are more efficacious in chronic and allergic sinusitis. Only start antibiotics if you strongly suspect bacterial disease.
Surgery
Surgery is not recommended for acute sinusitis except in rare circumstances. Sometimes the sinus infection can spread to the eye, face, or brain; this would be considered an emergency, and surgery may be needed to reverse the infection and keep it from spreading.
For chronic sinusitis, surgery is an option when the symptoms cannot be controlled with medications and other treatments. The most common type of surgery for the sinuses is called endoscopic sinus surgery; a pencil-sized scope (endoscope) is used to see inside the nose and sinuses and guide the surgery. The surgery widens the natural drainage pathways between the sinuses and the nose, allowing mucus to get out of the sinuses and air to get in. Medications that are delivered into the nose and sinuses, like sprays and irrigations, can also get into the sinuses better after surgery.
Balloon sinus ostial dilation is a newer treatment option where an endoscope is also used, but instead of carefully removing the bone and tissue that may be blocking a sinus, a balloon is used to make the sinus openings bigger. Balloon dilation may not be appropriate for every type of chronic sinusitis and cannot be used on all of your sinuses, but can be helpful depending on your circumstances.
Sphenoid sinus surgery
Sphenoidotomy is the surgical opening of the sphenoid sinus, is usually performed under general anesthesia. There are rare occasions when a surgeon may elect to perform a sphenoidotomy under local anesthesia in the operating suite or office setting. The indications for sphenoidotomy include acute and chronic sphenoid rhinosinusitis that is refractory to medical therapy; sphenoid mass or lesion; endonasal skull base or pituitary surgery; sphenoid cerebrospinal fluid leak repair; endonasal vidian neurectomy; and optic nerve or orbital decompression 5.
Sphenoid sinus surgery has no absolute contraindications. Relative contraindications include comorbidities that limit general anesthesia or conditions that increase the risk of bleeding. Care should also be taken when performing surgery on a hypoplastic sphenoid sinus or sphenoid sinus cavities with dehiscence of the internal carotid artery or optic nerve.
Procedure planning
Preoperative imaging should include noncontrast CT scanning of the sinuses to provide information about the bony architecture and pneumatization patterns of the sphenoid sinus. Other imaging studies may be advisable depending on the particular disease being managed. The characteristics that should be evaluated with regard to the sphenoid sinus prior to performing a sphenoidotomy include the following:
- Pneumatization pattern in relation to the sella turcica (conchal, presellar, sellar, postsellar)
- Location of the natural ostium and its relationship to the superior turbinate (the image below demonstrates a right-sided sphenoid sinus natural ostium located medial to the superior turbinate).
- Location of the optic nerve, optic chiasm, and internal carotid artery with particular attention to presence or absence of bony dehiscence
- Presence or absence of a posterior ethmoid (Onodi) cell.
Complication prevention
Prior to performing sphenoidotomy, the surgeon should carefully inspect the patient’s anatomic variants and extent of sinusitis. The surgeon should also use a standard approach that allows safe entrance into the sphenoid sinus. Stereotactic navigation should be considered, when warranted. In an effort to avoid severe complications, the surgeon should recognize potential pitfalls, such as cerebrospinal fluid leaks from inadvertent skull base injury, blindness from optic nerve injury, hemorrhage from the posterior septal branch of the sphenopalatine artery, or catastrophic hemorrhage from the internal carotid artery.
Regardless of the technique performed, care should be taken to avoid vital structures. The optic nerve may traverse laterally, and sometimes superiorly, in proximity to the sphenoid sinus or within an Onodi cell. Care should especially be taken to avoid disturbing the posterior wall of the sphenoid sinus, as this can risk injury to the carotid artery, optic chiasm, cavernous sinus, or pituitary gland. In addition, the surgeon should be aware that the posterior septal branch of the sphenopalatine artery traverses just inferior to the nature os of the sphenoid sinus; thus, removal of bone and mucosa inferiorly may cause inadvertent injury to this artery with resultant epistaxis. Some ways to avoid injury to this artery include elevating the mucosa off the bone or cauterizing the approximate site of the artery prior to performing inferior dissection. If bleeding is encountered secondary to this artery, it is fortunately readily controlled with monopolar or bipolar cauterization.
Sphenoid sinus surgery technique
Several specific sphenoid procedures may be performed. Some procedures, including lavage of the sphenoid sinus and diagnostic sinuscopy, provide access to the sphenoid sinus without requiring surgical sphenoidotomy. Surgical dilation of the sphenoid ostium is a minimally invasive approach to widen the sinus ostium without removing tissue 6.
Sphenoidotomy is the surgical opening of the sphenoid sinus. Sphenoidotomy may be performed without or with tissue removal. The designation of “tissue removal” has been defined by the American Academy of Otolaryngology-Head and Neck Surgery as removal of material or tissue, not just suctioning of mucus or pus.
The techniques for endoscopic sphenoidotomy may be divided into (1) transethmoidal versus transnasal approach and (2) opening via the natural os versus through the anterior sinus wall.
The size limitations of the sphenoidotomy depend on the size of the sphenoid sinus. The optimal size of the sphenoidotomy is unknown; however, it is generally considered important to perform wider sphenoidotomies in obstructive sinonasal disease such as polyposis and allergic fungal sinusitis. Expanded endonasal approaches via the sphenoid sinus often require extended procedures, including concomitant posterior septectomy, removal of the intersinus septum, and drilling away a portion of the rostrum and inferior portion of the anterior sphenoid sinus wall.
Endoscopic Sphenoidotomy, Transnasal via the Natural Ostium
Endoscopic transnasal sphenoidotomy without ethmoidectomy via the natural ostium can be considered in cases of isolated sphenoid sinus disease 7. This approach has the advantage of being minimally destructive of nasal mucosa and can result in shorter operative and recovery times; however, access to the sphenoidotomy site postoperatively may be limited because the ethmoid sinus cavity has not been opened.
A 30° nasal endoscope is often beneficial to provide visualization of the sphenoid sinus opening. Removal of part of the superior turbinate may be necessary to access the ostium and to facilitate postoperative care and inspection. The natural ostium of the sphenoid sinus usually lies just posterior to the superior turbinate. The anatomic landmarks that may be used to locate the natural ostium of the sphenoid sinus include the following 8:
- Posterior to the superior turbinate in the sphenoethmoid recess; the natural ostium is medial to the superior turbinate in 80% of cases
- Approximately 6 cm from the nasal sill at an angle of 30° from the nasal cavity floor
- Approximately 1 cm above the superior extend of the choana
- At the approximate level of the maxillary sinus roof
Once the sphenoid ostium is identified, it is enlarged using a sphenoid sinus mushroom punch or a small Kerrison punch. The contents within the sphenoid sinus are then cultured, biopsied, irrigated, or removed. Care should be taken to avoid manipulation of the posterior wall of the sphenoid sinus, which could risk injury to the internal carotid artery, optic nerve, or skull base.
Endoscopic Sphenoidotomy, Transethmoidal via the Natural Ostium
Endoscopic transethmoidal sphenoidotomy is a sphenoidotomy performed through the passageway of an ethmoidectomy. This approach is the most commonly performed method, as it gives the widest view of the sphenoid sinus from lamina papyracea to rostrum. A total ethmoidectomy is first performed until the anterior face of the sphenoid sinus, skull base, and superior turbinate are identified. A decision can then be made to approach the sphenoid via the natural os or through a puncture into a thin section of bone of the anterior face of the sphenoid sinus. Although no comparison trials have evaluated these two methods, each has theoretical and anecdotal advantages and disadvantages.
Performing a sphenoidotomy via the natural os is theorized to limit postoperative recirculation of mucus and may be safer, as the sphenoid sinus is opened via a known opening in the sinus. In contrast, a sphenoidotomy via the anterior sinus wall avoids removing a potentially healthy superior turbinate and may lessen the risk of olfactory dysfunction. The comparative complication and patency rates between these two procedures are unknown.
A 0° nasal endoscope is typically used for the procedure. Angled endoscopes (30°, 45°, or 70°) are occasionally used to visualize the corners or floor of the large sphenoid sinus cavities once a sphenoidotomy has been performed. When identifying the natural ostium, the inferior one third to half of the superior turbinate is often resected using a straight thru-cutting forceps. It is not advisable to resect the superior turbinate too superiorly because of risks to olfactory dysfunction and skull base injury with cerebrospinal fluid leak. The natural ostium of the sphenoid sinus usually lies just posterior to the superior turbinate. The anatomic landmarks that may be used to locate the natural ostium of the sphenoid sinus include the following 8:
- Posterior to the superior turbinate in the sphenoethmoid recess; the natural ostium is medial to the superior turbinate in 80% of cases
- Approximately 6 cm from the nasal sill at an angle of 30° from the nasal cavity floor
- Approximately 1 cm above the superior extend of the choana
- At the approximate level of the maxillary sinus roof
A J-curette or image guidance probe are helpful to bluntly palpate and identify the os when it cannot be visualized initially 9. Once the natural os is identified, a straight mushroom punch, Kerrison punch, or other instrumentation may be used to enlarge the opening laterally and superiorly.
Endoscopic Sphenoidotomy, Transethmoidal via Anterior Sinus Wall
Endoscopic transethmoidal sphenoidotomy via the anterior sinus wall avoids removing a potentially healthy superior turbinate and may lessen the risk of olfactory dysfunction.
A total ethmoidectomy is first performed until the anterior face of the sphenoid sinus, skull base, and superior turbinate are identified. A 0° nasal endoscope is typically used for this approach. Angled endoscopes (30°, 45°, or 70°) may be used to visualize the corners or the floor of the large sphenoid sinus cavities once a sphenoidotomy has been performed.
The superior turbinate is usually not resected unless the surgeon decides to incorporate the natural os. The image guidance system may be used to locate a safe location for entering the sinus. If no image guidance is available, the surgeon should choose a location that is somewhat inferior and medial with palpably evident thin bone to avoid skull base injury. A blunt sickle knife or J-curette is used to puncture through a thin section of bone in the anterior face of the sphenoid sinus. The sphenoid sinus mushroom punch, Kerrison punch, or other instrumentation can then be used to widen the sphenoidotomy.
Lavage of the sphenoid sinus
The least invasive procedure of the sphenoid sinus is a lavage of the sphenoid sinus, in which the sphenoid sinus is accessed either via the natural opening or through the sphenoid sinus face. The sinus is irrigated with saline and aspirated. The contents can then be cultured or evaluated by a pathologist.
A nasal/sinus endoscopy with sphenoid sinuscopy
A nasal/sinus endoscopy, diagnostic with sphenoid sinuscopy is a procedure in which a puncture is created or cannulation is performed of a nonsurgically opened ostium. The contents can then be irrigated, aspirated, cultured, or biopsied.
Nasal/Sinus Endoscopy, with dilation of sphenoid sinus ostium
A nasal/sinus endoscopy with dilation of the sphenoid sinus ostium is procedure in which the sphenoid sinus ostium is dilated mechanically to allow improved drainage and access to the sphenoid sinus. The procedure can be performed in the office setting or the operating room. Topical anesthesia and decongestion is performed.
In an unoperated sinus, the natural ostium is typically identified medial to the superior turbinate. Depending on the style of catheter used, a probe or a wire is gently inserted into the ostium. Once the sinus is successfully cannulated, the dilation device or balloon is advanced into the sinus ostium. The balloon is then inflated to dilate the sinus ostium. The sinus contents may then be irrigated, aspirated, cultured, or biopsied.
Sphenoid sinus surgery risks
The risks of endoscopic sphenoidotomy include, but are not limited to, the following 10:
- Bleeding
- Infection
- Anesthetic risks
- Scarring
- Recurrence of disease
- Skull base injury, cerebrospinal fluid leak, and meningitis
- Eye or vision loss and orbital nerve or optic chiasm injury
- Carotid artery injury
- Postoperative ostial stenosis
- Mucocele formation
Sphenoid sinus surgery recovery
The postoperative management of a endoscopic sphenoidotomy is similar to that of other procedures in functional endoscopic sinus surgery. Patients are often asked to perform nasal saline irrigations or lavages several times a day. Postoperative antibiotics and oral corticosteroids are given per surgeon preference.
Patients are usually seen in clinic for nasal endoscopy with debridement at about 1-2 weeks after surgery. The debridement of crusts and blood clots, as well as the early identification of scar tissue, helps limit postoperative adhesions.
Sphenoid sinus surgery outcomes
Sphenoidotomy appears efficacious based on case series studies 7. No prospective randomized controlled trials have evaluated sphenoidotomy.
References- Hamberger CA, Hammer G, Norlen G, et al. Transantrosphenoidal hypophysectomy. Arch Otolaryngol. 74:2-8.
- Henson B, Edens MA. Anatomy, Head and Neck, Nose Sinuses. [Updated 2019 Apr 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK513272
- Blackwell DL, Lucas JW, Clarke TC. Summary health statistics for U.S. adults: national health interview survey, 2012. Vital Health Stat. 2014;10:1-171
- Battisti AS, Pangia J. Sinusitis. [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470383
- Beswick DM, Ramadan H, Baroody FM, Hwang PH. Practice patterns in pediatric chronic rhinosinusitis: A survey of the American Rhinologic Society. Am J Rhinol Allergy. 2016 Nov 1. 30 (6):418-423
- Yadav YR, Nishtha Y, Vijay P, Shailendra R, Yatin K. Endoscopic endonasal trans-sphenoid management of craniopharyngiomas. Asian J Neurosurg. 2015 Jan-Mar. 10(1):10-6
- David A. Kieff, MD; Micholas Busaba, MD. Treatment of Isolated Sphenoid Sinus Inflammatory Disease by Endoscopic Sphenoidotomy Without Ethmoidectomy. The Laryngoscope. December 2002. 112:2186-2188
- Hyun-Ung Kim, MD; Sung-Shik Kim, MD; Seong Seok Kang, MD; In Hyuk Chung, MD; Jeung-Gweon Lee, MD; Joo-Heon Yoon, et al. Surgical Anatomy of the Natural Ostium of the Sphenoid Sinus. The Laryngoscope. 2001. 111:1599-1602.
- Jiang RS, Liang KL. Image-guided sphenoidotomy in revision functional endoscopic sinus surgery. Allergy Rhinol (Providence). 2014 Jan. 5(3):116-9
- Cheng Y, Xue F, Wang TY, Ji JF, Chen W, Wang ZY, et al. Analyses and treatments of postoperative nasal complications after endonasal transsphenoidal resection of pituitary neoplasms. Medicine (Baltimore). 2017 Apr. 96 (15):e6614





{kind=link}