
What is strabismus
Strabismus commonly known “crossed eyes”, squint or misalignment of the eyes, is a disorder in which both eyes do not line up in the same direction and the eyes point in different directions. Therefore, the eyes do not look at the same object at the same time. In strabismus one eye may look straight ahead, while the other eye turns inward (esotropia), outward (exotropia), upward (hypertropia) or downward (hypotropia). The eye turn may be constant or it may come and go (intermittent). Which eye is straight (and which is misaligned) may switch or alternate; in other words the misaligned eye will fixate and the previously fixing eye will become the misaligned eye. This alternation of deviating eye is often a good sign suggesting that the vision in each eye is equal. On the other hand, if the eyes do not switch fixation (one eye is constantly the fixating eye and the other eye is constantly the misaligned eye), then the fixating eye is favored and almost always has better vision. Strabismus can lead to reduced vision and failure of the eyes to work properly together, including for 3D vision. Strabismus or eye misalignment typically results in double vision in adults, but the developing brain in a child deals with the double vision by suppressing one of the images. Therefore, eye misalignment in childhood blocks normal binocular vision development (as the brain learns to rely on only one image from the fixing eye) resulting in a condition called amblyopia. Amblyopia is decreased vision in a perfectly healthy and well-formed eye which occurs because of a loss of the connection between an eye and the brain during a critical period of vision development from birth to 8 or 9 years of age. Young children with strabismus (eye misalignment) also typically have poor stereo or 3D vision and depth perception.
Strabismus is a common condition among children. About 4 percent of all children in the United States have strabismus 1. However, the prevalence figures for strabismus vary. The most recent screening study in Baltimore, USA, found a prevalence of manifest strabismus of 3.3% in Caucasian and 2.1% in African American children aged 6 to 71 months 2. Other population‐based studies have reported a prevalence of childhood strabismus between 0.01% and 3.1%, indicating that prevalence may vary greatly by ethnicity, age, type of strabismus and definitions used 3.
Strabismus can also occur later in life. Strabismus in adults often results in double vision because the brain has been trained to receive images from both eyes. Adults with strabismus are not at risk of developing amblyopia because the connections between the eye and the brain are already formed and cannot be suppressed.
Infantile esotropia, where the eye turns inward, is a common type of strabismus in infants. Young children with esotropia cannot use their eyes together. Accommodative esotropia is the most common form of esotropia that occurs in children usually 2 years or older. In this type of strabismus, when the child focuses the eyes to see clearly, the eyes turn inward. This crossing may occur when focusing at a distance, up close or both.
Exotropia, or an outward-turning eye, is another common type of strabismus. This occurs most often when a child is focusing on distant objects. The exotropia may occur only from time to time, particularly when a child is daydreaming, ill or tired. Parents often notice that the child squints one eye in bright sunlight.
Strabismus can be primary or it can be a consequence of poor vision in one eye or of refractive errors. Strabismus may run in families; however, many people with strabismus have no relatives with the problem. Less commonly, strabismus can be caused by lesions affecting the oculomotor nerve (the third cranial nerve or cranial nerve III), trochlear nerve (the fourth cranial nerve or cranial nerve IV) or abducens nerve (the sixth cranial nerve or cranial nerve VI) or higher neurological pathways. Strabismus is rarely caused by developmental or traumatic defects of the extraocular muscles. Strabismus is a risk factor for the development of amblyopia during the ‘sensitive period’ of vision development. During this period, neural plasticity is greatest, and it begins to decline around the age of 6 years; clinical interventions are typically offered to children up to the age of 10 years. Screening programmes therefore attempt to identify children with amblyogenic risk factors before the age of 6 years, to allow remedial treatment.
Conditions associated with strabismus include:
- Uncorrected refractive errors
- Poor vision in one eye
- Cerebral palsy
- Down syndrome (20-60% of these patients are affected)
- Hydrocephalus (a congenital disease that results in a buildup of fluid in the brain)
- Brain tumors
- Stroke (the leading cause of strabismus in adults)
- Head injuries, which can damage the area of the brain responsible for control of eye movement, the nerves that control eye movement, and the eye muscles
- Neurological (nervous system) problems
- Graves’ disease (overproduction of thyroid hormone)
A number of different tests can be used to screen for strabismus directly, by measuring the misalignment using corneal or fundus reflex tests; or indirectly, by measuring the level of vision in each eye (visual acuity); or by measuring 3D vision (stereopsis). The reference test to detect strabismus by trained professionals is the cover‒uncover test.
The goal of strabismus treatment is to improve eye alignment which allows for the eyes to better work together (binocular vision). Treatment may involve eye glasses, eye exercises, prism, and/ or eye muscle surgery. Strabismus surgery loosens or tightens eye muscles, changing the alignment of the eyes. Problems associated with strabismus (including amblyopia, ptosis, and cataract) are usually treated prior to eye muscle surgery.
Table 1. Eye muscles anatomy, actions and innervation (see also Figure 6 and 7)
| Extraocular muscle | Primary Action (of the globe, unless otherwise specified) | Secondary Action | Tertiary Action | Innervation |
|---|---|---|---|---|
| Medial rectus | Adduction | none | none | Inferior branch of the oculomotor nerve (cranial nerve III) |
| Lateral rectus | Abduction | none | none | Abducens nerve (cranial nerve VI) |
| Inferior rectus | Depression | Excyclotorsion | Adduction | Inferior branch of cranial nerve III |
| Superior rectus | Elevation | Incyclotorsion | Adduction | Superior branch of cranial nerve III |
| Inferior oblique | Excyclotorsion | Elevation | Abduction | Inferior branch of cranial nerve III |
| Superior oblique | Incyclotorsion | Depression | Abduction | Trochlear nerve (cranial nerve IV) |
| Levator palpebrae superioris | Upper eyelid elevation and retraction | none | none | Superior branch of cranial nerve III |
Figure 1. Cross eyed baby (Esotropia or inward turning of one or both eyes in this baby it’s his left eye)

Figure 2. Strabismus in a child (Exotropia or outward-turning of one or both eyes in this girl it’s her right eye)

Figure 3. Strabismus in adult (Esotropia or inward-turning of one or both eyes in this woman it’s her right eye)

Figure 4. Strabismus in adult (Exotropia or outward-turning of one or both eyes in this woman it’s her left eye)
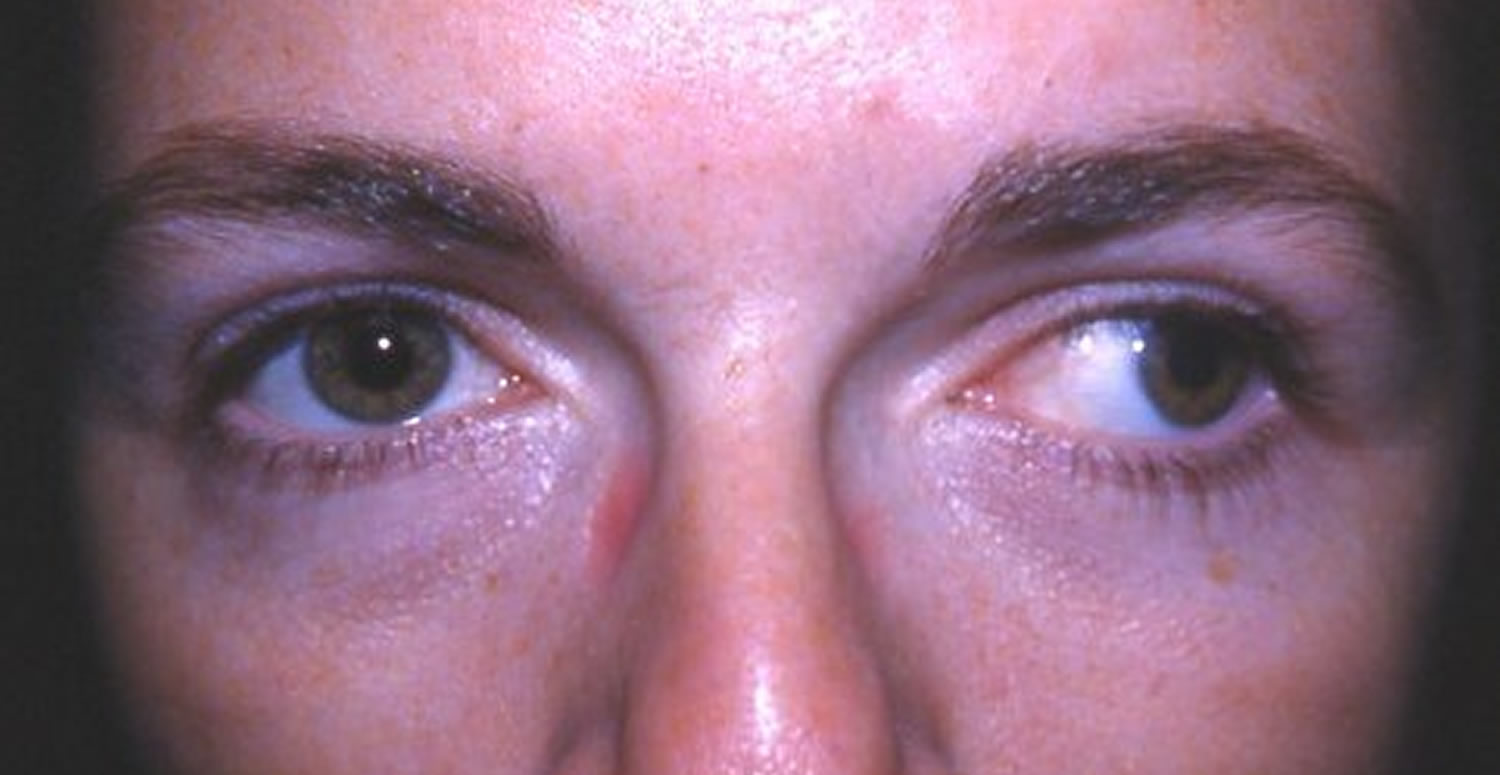
Figure 5. Pseudostrabismus (note a a fold of skin at the inner eyelid that can make eyes appear crossed)

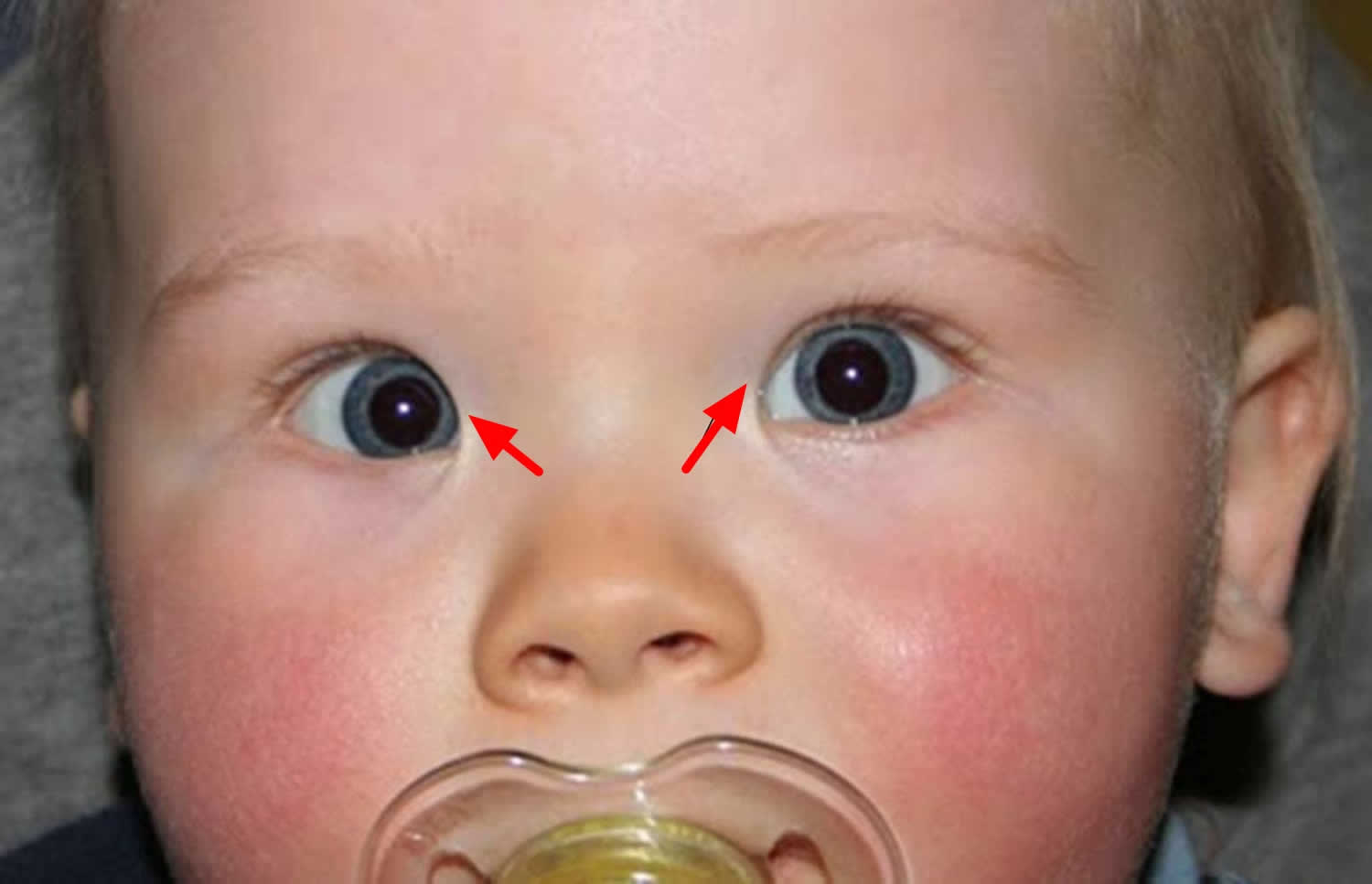
Figure 6. Eye muscles (right eye) and the actions on the eyeball movement are shown by “red” arrows
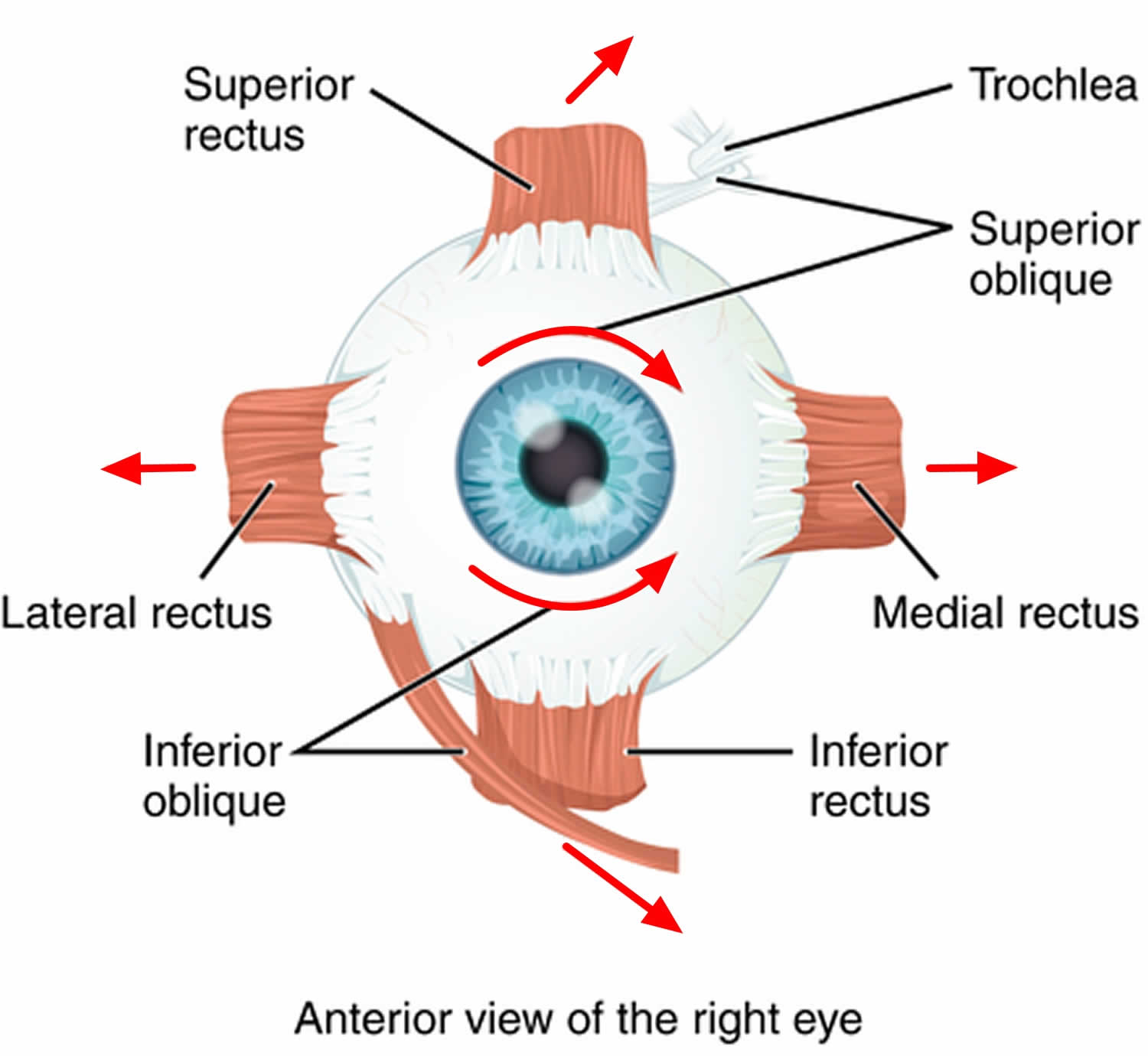
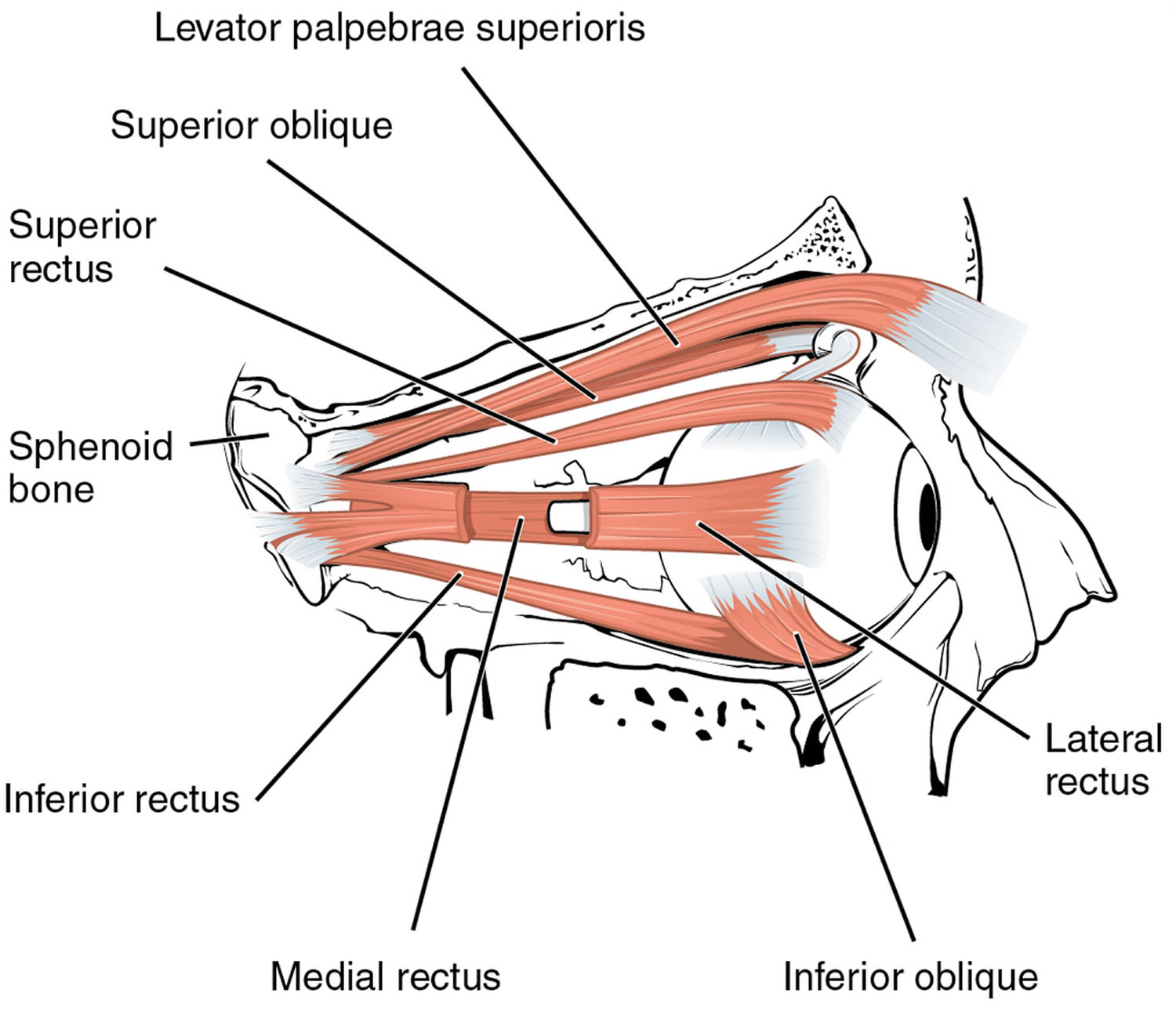
Figure 7. Eye muscles anatomy
Eye misalignment can cause amblyopia in children. When the eyes are oriented in different directions, the brain receives 2 different visual images. The brain may ignore the image from the misaligned eye to avoid double vision, resulting in poor vision development of that eye. Also, an eye that sees poorly may become misaligned.
Who develops strabismus as a child?
Strabismus often occurs in children who are otherwise completely normal. However, disorders that affect the brain such as cerebral palsy, Down syndrome, hydrocephalus and brain tumor are more likely to develop strabismus. Farsightedness may be a contributing factor, often in children. Any other disease that causes vision loss may also cause strabismus.
Strabismus is especially common among children with disorders that may affect the brain, such as:
- Cerebral palsy;
- Down syndrome;
- Hydrocephalus;
- Brain tumors;
- Prematurity;
- Apert syndrome;
- Congenital rubella;
- Hemangioma near the eye during infancy;
- Incontinentia pigmenti syndrome;
- Noonan syndrome;
- Prader-Willi syndrome;
- Retinopathy of prematurity;
- Retinoblastoma;
- Traumatic brain injury;
- Trisomy 18.
A cataract or eye injury that affects vision can also cause strabismus. The vast majority of children with strabismus, however, have none of these problems. Many do have a family history of strabismus.
What adult disorders cause strabismus?
Stroke or vascular problems may cause strabismus in adults. Trauma, neurological problems, and Graves disease (thyroid eye disorders) are other common causes of strabismus.
Strabismus that develops in adults can be caused by:
- Botulism
- Diabetes (causes a condition known as acquired paralytic strabismus)
- Graves disease
- Guillain-Barré syndrome
- Injury to the eye
- Shellfish poisoning
- Stroke
- Traumatic brain injury
- Vision loss from any eye disease or injury
A family history of strabismus is a risk factor. Any other disease that causes vision loss may also cause strabismus.
How does trauma cause strabismus?
Trauma can cause strabismus by 1) brain damage that impairs control of eye movement, 2) damage of the nerves that control eye movement and/or 3) damage of the eye muscles either directly or secondarily from trauma to the eye socket.
When do the symptoms of strabismus appear?
By the age of 3 to 4 months, an infant’s eyes should be able to focus on small objects and the eyes should be straight and well-aligned. A 6-month-old infant should be able to focus on objects both near and far.
Strabismus usually appears in infants and young children, and most often by the time a child is 3 years old. However, older children and even adults can develop strabismus. The sudden appearance of strabismus, especially with double vision, in an older child or adult could indicate a more serious neurologic disorder. If this happens, call your doctor immediately.
A condition called pseudostrabismus (false strabismus) can make it appear that a baby has crossed eyes when in fact the eyes are aiming in the same direction. Pseudostrabismus can be caused by extra skin covering the inner corners of the eyes and/or a flat nasal bridge. As the baby’s face develops and grows, the eyes will no longer appear crossed.
What can happen if strabismus is not treated?
Some believe that children will outgrow strabismus or that it will get better on its own. In truth, it can get worse if it is not treated. In the case of children with strabismus, if the condition is caught in time and properly treated, it can result in excellent vision and depth perception and can protect against loss of vision.
If your eyes are not properly aligned, the following may result:
- Lazy eye (amblyopia) or permanent poor vision in the turned eye. When the eyes are looking in different directions, the brain receives two images. To avoid double vision, the brain may ignore the image from the turned eye, resulting in poor vision development in that eye.
- Blurry vision, which can affect performance in school and at work, and enjoyment of hobbies and leisure activities
- Eye strain
- Fatigue
- Headaches
- Double vision
- Poor 3-dimensional (3-D) vision
- Low self-esteem (from embarrassment about one’s appearance)
It is also possible that by not diagnosing strabismus, a serious problem (such as a brain tumor that is causing the condition) may be overlooked.
Strabismus prognosis
Prognosis of strabismus is excellent if detected and managed early in life. After surgery, the eyes may look straight, but vision problems can remain.
The child may still have reading problems in school. Adults may have a hard time driving. Vision may affect the ability to play sports.
In most cases, the problem can be corrected if identified and treated early. Permanent vision loss in one eye may occur if treatment is delayed. Amblyopia sets in if the strabismus is not appropriately managed before 6-8 years leading to a permanent decrease in the vision. If amblyopia is not treated by about age 11, it is likely to be permanent. About one-third of children with strabismus will develop amblyopia.
Many children will get strabismus or amblyopia again. Therefore, the child will need to be monitored closely.
The importance of strabismus in children
There are many subtypes of strabismus. In the context of childhood vision screening programmes, the most relevant distinction is between manifest and latent strabismus. Manifest strabismus is a risk factor for the development of amblyopia, the commonest vision disorder in children (prevalence 1.6% to 3.6% in Western societies) 5.
Amblyopia is a developmental anomaly of spatial vision, usually associated with strabismus, anisometropia or from deprivation early in life 6. Amblyopes have reduced visual acuity in one or both eyes, reduced contrast sensitivity and reduced contour integration. Clinical definitions of amblyopia are based on visual acuity only, taking into consideration the age of the child and progressive improvement of ‘normal visual acuity’ in the early years. Unilateral amblyopia is often defined as an interocular difference in best‐corrected visual acuity (of 2 logMAR or Snellen chart lines) 2, or best‐corrected visual acuity of 0.30 logMAR or worse in either eye 3. In 3‐year‐old children, bilateral amblyopia is suspected if best‐corrected visual acuity is worse than 0.40 logMAR in one eye and worse than 0.3 logMAR in the other eye in the presence of a bilateral amblyogenic risk factor. In 4‐year‐old children, the thresholds are 0.3 and 0.18 logMAR, respectively 7. Note a LogMAR chart or Snellen chart comprises rows of letters and is used by ophthalmologists, optometrists and vision scientists to estimate visual acuity.
Strabismus has a profound effect on stereopsis or perception of depth. Stereopsis normally develops within the first 3 to 4 months of age and reaches adult levels by the age of 24 to 36 months 8. Two studies reported that stereoacuity continues to develop beyond the age of 3 years, and may not yet be fully mature at 5 years or 12 years of age, respectively 9, 10. Normal adult stereopsis is 50 to 60 seconds of arc; some childhood vision screening programmes have used a threshold of 400 seconds of arc for “suspicion of amblyopia” 3. Reduced stereopsis adversely affects motor skills, particularly fine motor skills 11.
Significant misalignment can affect development (through unilateral reduced acuity, lack of depth perception and limitation of peripheral visual field), social interactions, and emotional well‐being. In children with infantile esotropia (inward turning eye), surgical correction of strabismus leads to improvement in general development as measured by the Bayley scale 12. Scores on anxiety and depression scales such as the National Eye Institute Visual Functioning Questionnaire and the Hospital Anxiety and Depression Scale are significantly different from non‐strabismic children, and improve following surgical strabismus correction 13. Children with strabismus may have significantly greater conduct and externalising problems 14.
Strabismus can also be an indicator of severe eye and health problems. As it can indicate poor vision, it may in rare cases be the first sign of childhood cataract, glaucoma, or tumors of the eye, optic nerve, orbit or brain, such as retinoblastoma, glioma, or rhabdomyosarcoma.
Gross misalignment of the eyes is usually noticed by members of the family or carers. Small angles of deviation are not necessarily apparent. In young children, features such as a broad nasal bridge or certain lid positions and shape (epicanthus) can give rise to pseudostrabismus, i.e. a perception of strabismus when in fact the eyes are straight.
Strabismus symptoms
The main sign of strabismus is an eye that is not straight (misaligned eyes). Sometimes children will squint one eye in bright sunlight or tilt their head to use their eyes together.
Symptoms of strabismus may be present all the time, or may come and go. Symptoms can include:
- Crossed eyes
- Double vision
- Eyes that do not aim in the same direction
- Uncoordinated eye movements (eyes do not move together)
- Loss of vision or depth perception
It is important to note that children may never be aware of double vision. This is because amblyopia can develop quickly.
Adults with strabismus also may notice these other symptoms:
- Weakness in or around the eye, or feeling like something is pulling around your eyes.
- Vision changes, such as double vision (seeing two of one image), blurry vision, trouble reading, or a loss of depth perception.
- Constantly tilting or turning your head to see an image clearly.
Pseudostrabismus
The eyes of infants often appear to be crossed, though actually they are not (see Figure 5). This condition is called pseudostrabismus. Young children often have a wide, flat nose and a fold of skin at the inner eyelid (called epicanthal folds) that can make eyes appear crossed. This appearance of pseudostrabismus may improve as the child grows. Pseudostrabismus does not require treatment and the appearance tends to improve with time as facial grows. On the other hand, a child will not outgrow true strabismus. An ophthalmologist can distinguish true strabismus and pseudostrabismus. It is also important to remember that a baby with pseudostrabismus might develop a real strabismus later in life.
True strabismus in a child can lead to permanent vision loss and is best treated early. If a child is suspected of having strabismus, an ophthalmologist evaluation is important. It may be difficult to tell the difference between true strabismus and pseudostrabismus.
The ophthalmologist has several tests to determine if a real strabismus is present. A simple test is to shine a light onto both eyes and determine where the light reflects on the surface of the eyes. The light should fall on the center of each pupil at the same time. If a true strabismus is present the light reflexes do not fall on the same position of each eye. A more detailed test that is more sensitive to tiny deviations is called a cover test. The eyes are alternately covered while the fixation of each eye is monitored. If either eye has to move to fixate a strabismus is present.
Types of strabismus
There are many different types of strabismus. Strabismus is most commonly described by the direction of the eye misalignment. Common types of strabismus are esotropia (inward turning eye), exotropia (outward turning eye), hypotropia (downward turning eye) and hypertropia (upward turning eye).
Strabismus can also be described by its cause. Three of the twelve cranial nerves (III, IV, VI) are responsible for eye movement can be weak or palsied and cause strabismus. Some examples of this type of strabismus include third nerve (III) palsy and superior oblique (IV) palsy.
Special patterns of strabismus can have unique names such as Brown syndrome, and Duane syndrome.
Horizontal strabismus
Esotropia is inward turning of the eyes (aka “crossed eyes”). Types of esotropia include infantile esotropia, accommodative esotropia (related to farsightedness) and sixth nerve palsy. Exotropia is the term used to describe outward turning of the eyes (aka “wall-eyed”).
Accommodative esotropia
Accommodative esotropia often occurs in cases of uncorrected farsightedness and a genetic predisposition (family history) for the eyes to turn in. Because the ability to focus is linked to where the eyes are pointing, the extra focusing effort needed to keep distant objects in clear focus may cause the eyes to turn inward. Symptoms include double vision, closing or covering one eye when looking at something near, and tilting or turning the head. This type of strabismus typically starts in the first few years of life. Accommodative esotropia is usually treated with glasses, but may also require eye patching and/or surgery on the muscles of one or both eyes.
Infantile esotropia
Infantile esotropia also known as “crossed eyes”, is marked by a large amount of inward turning of one or both eyes in infants that typically starts before six months of age 15. There is usually no significant amount of farsightedness present and glasses do not correct the inward turning of the eyes. The cause of infantile esotropia is unknown 16. Many theories have been postulated regarding the pathogenesis of the disease 17, 18. Inward turning may start on an irregular basis, but soon becomes constant in nature. Infantile esotropia is present when the child is looking far away and up close. The treatment for this type of strabismus is surgery on the muscles of one or both eyes to correct the alignment. Children should be followed closely for amblyopia, even if they achieve good motor alignment. Close follow up is required especially in cross fixating children as amblyopia in one eye can present after surgical alignment 19. The number of children requiring a second operation varies between 15-30% 20. Amblyopia, residual esotropia or consecutive persistent exotropia may develop and should be addressed early to get the best possible visual and fusion potential.
Intermittent exotropia
In intermittent exotropia, one eye will fixate (concentrate) on a target while the other eye is pointing outward. Symptoms may include double vision, headaches, difficulty reading, eyestrain, and closing one eye when viewing far away objects or when in bright light. Patients may have no symptoms while the ocular deviation (difference) may be noticed by others. Intermittent exotropia can happen at any age. Treatment may involve glasses, patching, eye exercises and/or surgery on the muscles of one or both eyes.
Vertical strabismus
The terms hypertropia and hypotropia are used to describe vertical misalignment. Hypertropia is an abnormal eye higher than the normal eye. Hypotropia is when the abnormal eye is lower than the normal eye. The terms can generally be interchanged depending upon which eye is being described.
Brown syndrome
Brown syndrome also known as superior oblique tendon sheath syndrome, is a vertical strabismus syndrome characterized by limited elevation of the eye in an adducted position, most often secondary to mechanical restriction of the superior oblique tendon-trochlea complex 21. Brown syndrome was considered a dysgenesis of the superior oblique muscle’s tendon sheath. More recently, it is thought that the problem is not the sheath, but rather the tendon itself, that undergoes increased tension 21.
Brown syndrome can be congenital or acquired, is unilateral in 90% of patients, and has a slight predilection for females 21. There is thought to be a genetic predisposition to congenital Brown syndrome, however, most cases are sporadic in nature. Recent work suggests that some Brown syndrome cases may be associated with congenital cranial dysinnervation disorders. Secondary causes of Brown syndrome include inflammation, trauma, tendon cysts, previous sinusitis, orbital tumors, and iatrogenic causes such as orbital or strabismus surgery. Abnormalities of the fascial anatomy is considered to be a rare cause.
Management of Brown syndrome depends on symptomatology, cause and the course of the disease.
Observation is often preferred, as symptoms are often intermittent in nature and do not cause permanent damage. Improvement of congenital Brown syndrome has been described in up to 75% of cases. Of note, as patients are most symptomatic on upgaze, normal growth can decrease symptoms as patients grow taller and have less necessity for upgaze position. Acquired Brown syndrome cases may also undergo spontaneous resolution, and thus early surgical intervention is not recommended.
Brown syndrome due to inflammatory disease with associated pain may transiently benefit from injection of steroids to the trochlear area. This may require recurrent treatments for symptomatic relief.
Systemic steroids and non-steroidal anti-inflammatory agents have also been utilized with variable success. Immunosuppressants (i.e. adalimumab) have been used in refractory cases.
Surgery can be considered in the following circumstances:
- Hypotropia in primary position
- Significant abnormal head position
- Significant diplopia
- Significant downshoot on adduction
- Compromised binocularity
- Significant orbital pain or pain with eye movements
The following surgical procedures can be performed:
- A tenotomy or tenectomy to weaken the superior oblique (but beware post-operative iatrogenic superior oblique palsy)
- A superior oblique expansion surgery has been found to have high success rates and can be performed through a variety of techniques, including a silicon expander (e.g. a #240 retinal silicone band), a non-absorbable “Chicken suture”, or a superior oblique split tendon lengthening procedure
- Iatrogenic Brown syndrome secondary to muscle plication may require reversal of the plication
- In case the primary cause is a tendon cyst, removal of the cyst may be indicated
Strabismus or crossed eyes causes
Most strabismus is the result of an abnormality of the neuromuscular (including brain) control of eye movement. Scientists and doctors understanding of these control centers in the brain remains incomplete. Less commonly, a problem with the actual eye muscle may cause strabismus. Strabismus is often inherited, with about 30 percent of children with strabismus having a family member with a similar problem.
Six eye muscles are attached to outside of each eye and work “as a team”, controlling eye movement (see Table 1 and Figure 6 & 7 above). In each eye, one muscle moves in the eye to the right, and one muscle moves the eye to the left. The other four muscles move it up or down and control tilting movements. To focus both eyes on a single target, all 6 eye muscles on each eye must work together with the corresponding muscles of the opposite eye. The brain coordinates these eye muscle movements.
To line up and focus both eyes on a single target, all of the muscles in each eye must be balanced and working together. In order for the eyes to move together, the eye muscles in both eyes must be coordinated. The brain controls these eye muscles.
In someone with strabismus, these eye muscles do not work together. As a result, one eye looks at one object, while the other eye turns in a different direction to focus on another object. Most of the time, the problem has to do with muscle control, and not with muscle strength.
With normal vision, both eyes aim at the same spot. The brain then combines the two pictures into a single, three-dimensional image. This three-dimensional image gives us depth perception.
When one eye is out of alignment, two different pictures are sent to the brain — one from each eye. This confuses the brain. In a young child, the brain learns to ignore (suppress) the image of the misaligned eye –the weaker eye and sees only the image from the straight or better-seeing eye. The child then loses depth perception.
If the strabismus is not treated, the eye that the brain ignores will never see well. This loss of vision is called amblyopia. Another name for amblyopia is “lazy eye.” Sometimes lazy eye is present first, and it causes strabismus.
In most children with strabismus, the cause is unknown. In more than half of these cases, the problem is present at or shortly after birth. This is called congenital strabismus.
Adults who develop strabismus often have double vision because their brains have already learned to receive images from both eyes and cannot ignore the image from the turned eye. A child generally does not see double.
Strabismus is especially common among children with disorders that may affect the brain, such as:
- Cerebral palsy;
- Down syndrome;
- Hydrocephalus;
- Brain tumors;
- Prematurity;
- Apert syndrome;
- Congenital rubella;
- Hemangioma near the eye during infancy;
- Incontinentia pigmenti syndrome;
- Noonan syndrome;
- Prader-Willi syndrome;
- Retinopathy of prematurity;
- Retinoblastoma;
- Traumatic brain injury;
- Trisomy 18.
A cataract or eye injury that affects vision can also cause strabismus. The vast majority of children with strabismus, however, have none of these problems. Many do have a family history of strabismus.
Adults can also experience strabismus. Most commonly, ocular misalignment in adults is due to stroke, but it can also occur from physical trauma or from a childhood strabismus that was not previously treated or has recurred or progressed. Strabismus in adults can be treated in a variety of ways, including observation, patching, prism glasses and/or strabismus surgery.
Strabismus that develops in adults can be caused by:
- Botulism
- Diabetes (causes a condition known as acquired paralytic strabismus)
- Graves disease
- Guillain-Barré syndrome
- Injury to the eye
- Shellfish poisoning
- Stroke
- Traumatic brain injury
- Vision loss from any eye disease or injury
A family history of strabismus is a risk factor. Farsightedness may be a contributing factor, often in children. Any other disease that causes vision loss may also cause strabismus.
Strabismic amblyopia
Good vision develops during childhood when both eyes have normal alignment. Strabismus may cause reduced vision, or amblyopia, in the misaligned eye.
The brain will pay attention to the image of the straight eye and ignore the image of the crossed eye. If the same eye is consistently ignored during early childhood, this misaligned eye may fail to develop good vision, or may even lose vision. Strabismic amblyopia occurs in approximately half of the children who have strabismus.
Amblyopia can be treated by patching or blurring the stronger eye to strengthen and improve vision in the weaker eye. If amblyopia is detected in the first few years of life, treatment is usually successful. If treatment is delayed, amblyopia may become permanent. As a rule, the earlier amblyopia is treated, the better the result for vision.
Risk factors for strabismus
Risk factors for strabismus include:
- Prematurity
- Amblyopia
- Refractive error, particularly anisometropia
- Family history of strabismus
- Craniofacial disorders
- Cranial nerve palsies
- Poor vision in one or both eyes
- Thyroid disease
- Genetic syndromes
- Demyelinating disease
- Central nervous system disorders
- Neuromuscular disorders 22.
Strabismus is more prevalent with certain syndromes like Down syndrome, cerebral palsy, Apert-Crouzon syndrome, premature infants with low birth weight, and in kids with affected parents or siblings 23. All siblings of a strabismic child should be screened at an early age for strabismus as sensorimotor anomalies are common in the pedigrees of strabismic probands. A proband also known as the index case, is a person serving as the starting point for the genetic study of a family.
Strabismus complications
Complications of strabismus include the following:
- Amblyopia (“lazy eye” or a condition in which the eye and brain don’t work together as they should causing poor vision even blindness)
- Reduced stereopsis (depth perception or 3D vision)
- Asthenopia (eyestrain)
- Diplopia (double vision)
- Nystagmus (involuntary eye movement which may cause the eye to rapidly move from side to side, up and down or in a circle, and may slightly blur vision)
- Abnormal head and neck posture
- Impaired social and mental growth
Surgical treatment for strabismus may result in the following:
- Diplopia
- Under/over-correction
- Conjunctival scarring, granuloma, and chronic inflammation
- Corneal Dellen
- Scleral perforation
- Lost muscle
- Endophthalmitis
- Anterior segment ischemia
- Retrobulbar hemorrhage
Srabismus diagnosis
Strabismus can be diagnosed during an eye exam. Your health care provider will do a physical exam. This exam includes a detailed examination of the eyes.
It is recommended that all children between 3 and 3½ years of age have their vision checked by their pediatrician, family practitioner or an individual trained in vision assessment of preschool children. Any child who fails this vision screening should then have a complete eye exam by an ophthalmologist.
If there is a family history of strabismus or amblyopia, or a family history of wearing thick eyeglasses, an ophthalmologist should check vision even earlier than age 3. After a complete eye examination, an ophthalmologist can recommend appropriate treatment.
The following tests will be done to determine how much the eyes are out of alignment.
- Corneal light reflex
- Cover/uncover test
- Retinal exam
- Standard ophthalmic exam
- Visual acuity
A brain and nervous system (neurological) exam will also be done.
How strabismus is measured
Eye misalignment or strabismus can be measured by several different methods. The measurements help guide the surgical and medical management of strabismus. The age, vision, and level of cooperation of the patient determine which method is most accurate and feasible.
Strabismus test
Light reflex test
Light reflex testing also called Hirschberg testing, involves directing a patient to look at a point of light held about three feet from the patient’s face. If the light reflexes are located in the same spot in each pupil, the reflexes are symmetric and the eyes are straight. If the light reflexes fall asymmetrically in the pupils, strabismus may be present. Hirschberg testing estimates the size of the strabismus by determining how far the deviated light reflex is off-center. A more accurate form of light reflex testing is Krimsky testing which involves holding a prism over one eye to center the deviated light reflex until the reflexes are symmetric. The amount of the prism needed to center the deviated light reflex estimates the size of the eye misalignment. Although light reflex testing is not extremely accurate, light reflex testing may be the only means possible in young children and in those with vision too poor to fixate well on a target.
The cover test
The cover test is another method to evaluate strabismus. All cover tests are carried out with the participant fixing on a target presented at distances of 6, 4 or 3 meters, and then at near distances (33 cm or 40 cm). In children, the distance target is often presented at 3 meters. In very young children the cover test is often only carried out at near fixation. While the patient is fixating on the target, one eye is covered. The uncovered eye is observed. If the uncovered eye is well aligned, it will not shift position when the other eye is covered. If the uncovered eye is misaligned, its position will change as the eye shifts to look at the target. For example, if the left eye is turned in, as the right eye is covered, the left eye will move outward to fixate on the target. If an eye is higher and the other eye is covered, the eye makes a downward movement when the other eye is covered.
The cover‒uncover test aims to detect strabismus, but not refractive errors, the other significant group of amblyogenic risk factors. Its accuracy as a standalone amblyopia screening test is therefore limited 7. Conversely, addition of the cover‒uncover test to vision screening tests increases the detection rate of strabismus 24. Vision screening programmes for children between 4 and 6 years traditionally use optotype testing to determine visual acuity (matching or naming letters or pictures), with or without a cover test to detect strabismus. In an effort to screen younger children to identify and treat problems early, these ‘manual’ screening programmes are increasingly supplemented or even replaced by the use of devices such as photorefractors, which also aim to provide information about refractive amblyogenic risk factors. The American Association of Pediatric Ophthalmology and Strabismus recently published updated recommendations for automated screening programmes 25. Screening methods were categorized into refractive and non‐refractive screening instruments. With regards to detection of strabismus, the American Association of Pediatric Ophthalmology and Strabismus recommends that non‐refractive screening devices should detect manifest strabismus greater than 8 prism dioptres in primary position 25. UK recommendations suggest that screening at age 4 to 5 years old provides the most accuracy and allows adequate time to treat 26.
What are prisms?
Prisms are clear, triangular shaped objects that bend light. When held in front of an eye, the prism shifts the pathway of light coming into the eye. The amount the light is shifted is measured in a unit called prism diopters. Prism diopter measurements describe the amount of eye misalignment. A prism bar with stacked increasing prism diopter units may be used instead of individual prisms to improve the speed of measurements.
What is prism and cover testing?
Prism and cover testing are used to determine the amount of strabismus present. A prism is held over the one eye, and the eyes are alternately covered, giving time between alternation for the patient to fixate on a target. When the proper strength of prism is place over the misaligned eye, there is no movement of the eyes when the cover is switched back and forth between the eyes. The eye alignment is measured in different gaze directions, including with head tilts, and at near.
What is positive angle kappa?
A person can look like they have strabismus because of an off-center light reflex and still have straight eyes. This may occur due to a discrepancy between the center of the front surface of the eye and the part of the retina that gives the sharpest vision called the macula. Patients with a positive angle kappa will have normal strabismus measurements and no eye movement on cover testing.
Why is it important to get good strabismus measurements?
Medical and surgical treatment of strabismus is based on the amount of eye misalignment present. Sometimes several office visits are needed to obtain accurate and complete strabismus measurements.
Strabismus treatment
Treatment for strabismus works to straighten the eyes and restore binocular (two-eyed) vision. In some cases of strabismus in children and adults, strabismus treatment consists of glasses, prisms, patching or blurring of one eye, botulinum toxin injections, or a combination of these treatments. Other times, eye muscle surgery is necessary to straighten the eyes or other eye surgery to remove a cataract. Patching or blurring the strong eye to improve amblyopia is often necessary.
Very young children with esotropia usually require surgery to realign the eyes.
For accommodative esotropia, glasses reduce the focusing effort and often straighten the eyes. Sometimes bifocals are needed for close work. If significant crossing of the eyes persists with the glasses, surgery may be required.
With exotropia, though glasses, exercises, patching or prisms may reduce or help control outward-turning of the eye in some children, surgery is often needed.
Strabismus treatment options include the following:
- Eyeglasses or contact lenses: Used in patients with uncorrected refractive errors. With corrective lenses, the eyes will need less focusing effort and may remain straight.
- Prism lenses: Special lenses that can bend light entering the eye and help reduce the amount of turning the eye must do to look at objects.
- Orthoptics (eye exercises): May work on some types of strabismus, especially convergence insufficiency (a form of exotropia).
- Medications: Eye drops or ointments. Also, injections of botulinum toxin type A (such as Botox) can weaken an overactive eye muscle. These treatments may be used with, or in place of, surgery, depending on the patient’s situation.
- Eye patching: To treat amblyopia (lazy eye), if the patient has it at the same time as strabismus. The improvement of vision may also improve control of eye misalignment.
- Eye muscle surgery: Surgery changes the length or position of eye muscles so that the eyes are aligned correctly. This is performed under general anesthesia with dissolvable stitches. Sometimes adults are offered adjustable strabismus surgery, where the eye muscle positions are adjusted after surgery.
Strabismus surgery
During a strabismus surgery the ophthalmologist makes a small incision in the tissue covering the eye to reach the eye muscles. The eye muscles are detached from the wall of the eye and repositioned during the surgery, depending on which direction the eye is turning. Strabismus surgery involves sewing the eye muscle to the wall of the eye after altering the insertion position and/or the length of the muscle. Standard strabismus surgery (no adjustable suture) utilizes a permanent knot. Adjustable suture technique utilizes a bow-knot or slip-knot (temporary knot) in an accessible position. After surgery the eye alignment can be altered by adjusting the temporary knot. The adjustment is typically done while the patient is awake and the operated eye numbed.
It may be necessary to perform surgery on one or both eyes.
Recovery time is rapid. Children are usually able to resume their normal activities within a few days.
After surgery, glasses may still be required. In some cases, more than one surgery may be needed to straighten the eyes.
Preoperative tests for strabismus surgery
Before surgery, a specialized examination called a sensorimotor examination will be performed in the ophthalmologist’s office to assess the alignment of the eyes to determine which muscles are contributing to the strabismus and which muscles need to be altered (weakened, strengthened, or moved) to improve the alignment of the eyes. Prisms are used to measure the degree of the strabismus. These preoperative tests help guide the surgeon in determining the surgical plan. Often both eyes require surgery, even if only one is misaligned. Sometimes the exact surgical plan is determined based on findings at the time of the surgery, especially in reoperations.
Medications and strabismus surgery
Strabismus surgery rarely causes significant bleeding. However, some surgeons may suggest that you stop taking blood thinners, aspirin, aspirin-containing products, ibuprofen or certain nutritional supplements that can affect bleeding for a week before the surgery. Withholding these medications should also be discussed with the prescribing doctor to assess the risk of NOT taking the medication. If a pain medication is necessary during this time, acetaminophen (Tylenol) can be used as a substitute.
Strabismus surgery procedure
Strabismus surgery in children requires general anesthesia. Before surgery, a medication is often given to children to alleviate their anxiety of being separated from their parent. In adults, the procedure can be done with general or local anesthesia. Either way, the patient must fast for about eight hours before the procedure. For this reason, pediatric cases are often scheduled in the early morning.
The eyelids are gently held open with a lid speculum. A small opening is made through the conjunctiva (the mucous membrane surface of the eye) to access the muscle and no skin incisions are made. The surgeon then uses a delicate hook to isolate the eye muscle. The eye muscle is then weakened, strengthened or moved to change its action with dissolvable sutures. Most strabismus surgeries are less than one to two hours; however, the patient will be at the surgery center for several hours including pre-operative and post-operative care.
Adjustable sutures
Strabismus surgery involves sewing the eye muscle to the outer covering of the eye after altering the insertion position and/or the length of the muscle. Standard strabismus surgery without adjustable suture utilizes a permanent knot tied during the surgical procedure. Adjustable suture technique utilizes a bow-knot or slip-knot (temporary knot) on the muscle which can be changed. After surgery, the eye alignment can be altered by adjusting the temporary knot. The adjustment is typically done with the patient awake and the operated eye numbed. Adjustable suture surgery is generally only offered to patients who are able to fully cooperate with the adjustment process. This adjustment may be done in the postoperative room, the next day, or later in the week, depending upon the surgeon’s preference.
After surgery
Any patient that has surgery, whether under general anesthesia or local anesthesia with sedation, needs to be monitored after surgery. Children can return to school after two days. Adults should not drive the day of surgery or the day after and may need up to a week before returning to work. You may have double vision that can last hours to days or a week or more, rarely longer. Exercise caution with activities like driving if you have double vision.
Pain is minimal and usually over-the-counter medicines, such as ibuprofen (Motrin) or acetaminophen (Tylenol), and cool compresses are adequate. Adults and older children may need prescription pain medicine.
The main restriction after strabismus surgery is not swimming for two weeks.
The eye will be red for one to two weeks, rarely longer, especially if it is a reoperation.
After surgery:
- The eye will be red and slightly swollen for a couple of days. It should open fully within 2 days after surgery.
- The eye may be “scratchy” and sore when it moves. Acetaminophen (Tylenol) or a cool, damp washcloth placed gently over the eye can provide comfort.
- You or your child may have some blood-tinged discharge from the eye. The health care provider will prescribe eye ointment or eye drops to use after the surgery to help the eye heal and prevent infection.
- Your eyes or your child’s eye may be sensitive to light. Try dimming the lights, closing curtains or shades, or wearing sunglasses.
Try to avoid rubbing the eyes.
Double vision is common after surgery for adults and for children ages 6 and older. It is less common in younger children. Double vision most often goes away after the surgery. In adults, an adjustment is sometimes made to the position of the eye muscle to refine the results.
You or your child can go back to your normal activities and exercise within a few days after surgery. You can return to work, and your child may go back to school or day care a day or two after surgery.
Children who had the surgery can slowly go back to a regular diet. Many children feel a little sick to their stomach after surgery.
Most people do not have to wear a patch over their eye after this surgery, but some do.
You or your child should have a follow-up visit with the eye surgeon 1 to 2 weeks after the surgery.
When to call your doctor
Call your eye doctor if you or your child has:
- A lasting low-grade fever, or a fever higher than 101°F (38.3°C)
- Increased swelling, pain, drainage, or bleeding from the eye
- An eye that is no longer straight, or is “way out of line.”
Potential risks of strabismus surgery
The chance of any serious complication from strabismus surgery that could affect the sight or well-being of the eye is exceedingly rare. However, surgical treatment for strabismus may result in the following:
- Sore eyes;
- Redness;
- Residual misalignment;
- Under/over-correction;
- Lost muscle;
- Double vision (diplopia);
- Infection;
- Endophthalmitis;
- Bleeding;
- Corneal abrasion;
- Corneal dellen (small saucer-like excavations at the margin of the cornea);
- Conjunctival scarring, granuloma, and chronic inflammation;
- Scleral perforation;
- Anterior segment ischemia;
- Retrobulbar hemorrhage;
- Decreased vision;
- Retinal detachment;
- Anesthesia-related complications.
How successful is strabismus surgery?
Strabismus surgery is a common procedure and most patients will see a large improvement in the alignment of their eyes after surgery. In some cases, you may need additional surgery or prism glasses to optimally align the eyes. Each case of strabismus is unique and should be discussed with your ophthalmologist to understand the goals and expectations of surgery.
How does the surgeon approach the eye muscles?
The eye muscles attach to the sclera (outer covering of the eye). The muscles are covered by a thin layer of transparent tissue called the conjunctiva. The eyelids are held open by a lid speculum. The surgeon incises the conjunctiva to access the eye muscle(s), and uses small instruments to identify the muscle targeted for surgery. No skin incisions are made. The eyeball is NOT removed from the eye socket during strabismus surgery.
What kind of anesthesia is used for strabismus surgery?
The type of anesthesia depends on patient age and health as well as patient preference. Most children undergo general anesthesia. Adults may have general anesthesia, conscious sedation or local anesthesia. The procedure is usually performed as an outpatient (patients come in and go home the same day).
What is an adjustable suture?
Strabismus surgery involves sewing the eye muscle to the wall of the eye after altering the insertion position and/or the length of the muscle. Standard strabismus surgery (no adjustable suture) utilizes a permanent knot. Adjustable suture technique utilizes a bow-knot or slip-knot (temporary knot) in an accessible position. After surgery the eye alignment can be altered by adjusting the temporary knot. The adjustment is typically done with the patient awake and the operated eye numbed, so adjustable suture surgery generally may only be offered to patients who are able to fully cooperate with the adjustment process.
What is a recession?
A recession weakens function by changing the attachment site of the muscle on the eyeball. Once the muscle has been identified, a stitch is placed through the muscle. The muscle is cut from the surface of the eye and stitched back to the eye in a new—weaker location further back from the front of the eye. The muscle is no longer taut, similar to an elastic band that has been released. This effectively reduces the resting tension of the muscle.
What is a resection?
A resection strengthens muscle function by shortening the muscle and then reattaching it to the eyeball at its original position, similar to cutting an elastic band, but still stretching it to the original length. A suture is placed through the muscle at the new intended length. The segment of muscle between the suture and the eyeball is removed or folded over (plication), and the shortened muscle is reattached to the eye.
Are the eyes red after strabismus surgery?
It is normal for the white part of the eyes to be red after surgery. It may take several weeks or occasionally months for the redness to disappear. The eyes are usually scratchy and are sore upon movement. The soreness usually improves after a few days depending upon the exact surgery performed.
Are patches or medicine used after surgery?
A patch is usually placed only if an adjustable suture is used. All surgeons apply antibiotic or antibiotic/steroid drops or ointment at the end of the surgery. Some surgeons will prescribe a similar drop after surgery for a few days as well.
Strabismus surgery in adults
In adults, eye alignment surgery restores normal appearance and is considered reconstructive. There are many other benefits beyond restoring normal appearance: improved depth perception or binocular vision, improved visual fields, eliminating or minimizing double vision and improved social function — as eye contact is hugely important in human communication. It is important to discuss the goals and expectations of the surgery with your ophthalmologist.
During strabismus surgery, one or more of the eye muscles are strengthened, weakened or moved to a different position to improve alignment. Strabismus surgery is usually performed as an outpatient procedure and does not require an overnight hospital stay.
Who treats cross eyed in adults?
An ophthalmologist trained in strabismus is the most qualified specialist to treat adults with misaligned eyes. A specialist can be located in the directory of American Association for Pediatric Ophthalmology and Strabismus (https://secure.aapos.org/aapos/Find-a-Doctor), an organization of eye surgeons with special training in eye muscle problems. Your own eye doctor may also have a recommendation.
Many adults with strabismus wonder, “Why do I go to a pediatric eye specialist? I’m not a child anymore.” The answer is that misaligned eyes are common in children and ophthalmologists who care for children tend to have the most expertise in treating eye muscle conditions.
Does my insurance cover the expense of this surgery?
Eye muscle surgery is reconstructive (not cosmetic). In most cases, insurance will cover strabismus surgery in adults, however, one should check with their medical insurance carrier to determine coverage with their specific plan.
Is eye muscle surgery risky for adults?
Every surgical procedure has some risks. For strabismus surgery, the most common risks are residual misalignment of the eyes and double vision. Most double vision that occurs after strabismus surgery is temporary; however, persistent double vision is possible. Fortunately, the more serious risks are rare. These risks include anesthetic complications, infection, bleeding, retinal detachment, and decreased vision. Health risks vary with the general health of the individual. For those in poor health, surgery under local anesthesia instead of general anesthesia may be considered.
How successful is eye muscle surgery?
Most individuals have significant improvement in eye alignment with one surgery. Occasionally the surgery is only partially successful, or changes in ocular alignment may occur over time after initially successful surgery. Additional surgery may be indicated. Correction of residual double vision may be improved with the use of prism glasses.
How painful is strabismus surgery?
Discomfort after eye muscle surgery is usually not severe. Headache, pulling sensation with eye movement and foreign body sensation in the eye are the most common complaints. These symptoms typically last only several days. Over-the-counter pain medication often reduces the discomfort, although stronger medication is sometimes prescribed. Most patients return to full activity in several days. Some surgeons limit swimming and heavy physical activity for up to several weeks after surgery.
Is hospitalization required for strabismus surgery?
Eye alignment surgery is usually performed as an outpatient procedure although the need for hospitalization varies depending upon general health and surgeon preference. Following surgery, most individuals return to nearly all normal activities within several days.
What age is considered “too old” to have eye muscle surgery?
Eyes can be straightened at any age and should be considered as a treatment option if it is likely to improve symptoms and enhance quality of life. In most cases, eye muscle surgery is a successful, safe, and effective treatment for strabismus in adults of all ages. The good news is that it is never too late for surgery. Even patients in their 90’s have benefited from surgical correction.
I am embarrassed by my misaligned eyes and avoid looking people in the eye. It seems to me that people are distracted by my wandering eye, causing problems with social interaction and difficulty getting the job I want. Can this really be true?
Yes. Recent studies confirm these observations. Misaligned eyes can hinder social interaction, self-confidence and employment opportunities. All individuals deserve straight eyes if possible.
Eye muscle exercises
An ophthalmologist can teach you exercises to help you focus both eyes inward. These exercises can help if you have “convergence insufficiency.” That is when your eyes do not align properly for close tasks, like reading or computer work.
Prism eyeglasses
A prism is a clear, wedge-shaped lens that bends (refracts) light rays. A prism can be attached to eyeglasses or made as part of the lens. Prisms can help some people with mild double vision see one image, not two.
Botulinum toxin (Botox)
In some cases, an injection (shot) of this drug in the eye can help treat strabismus. It paralyzes the muscles that keep your eyes from aligning properly. The effect can last for just a few months, or it could permanently improve eye alignment.
References- What Is Strabismus? https://www.aao.org/eye-health/diseases/what-is-strabismus
- Friedman DS, Repka MX, Katz J, Giordano L, Ibironke J, Hawse P, et al. Prevalence of amblyopia and strabismus in white and African American children aged 6 through 71 months the Baltimore Pediatric Eye Disease Study. Ophthalmology 2009;116(11):2128‐34.
- Traboulsi EI, Cimino H, Mash C, Wilson R, Crowe S, Lewis H. Vision First, a program to detect and treat eye diseases in young children: the first four years. Transactions of the American Ophthalmological Society 2008;106:179‐85.
- Zanganeh T, Legault GL. Extraocular Muscle Management With Orbital and Globe Trauma. [Updated 2021 Nov 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK573075
- Simons K. Preschool vision screening: rationale, methodology and outcome. Survey of Ophthalmology 1996;41(1):3‐30.
- Ciuffreda KJ, Levi DM, Selenow A. Amblyopia: Basic and Clinical Aspects. Boston: Butterworth Heinemann, 1991.
- Schmidt P, Maguire M, Dobson V, Quinn G, Ciner E, Cyert L, et al. Comparison of preschool vision screening tests as administered by licensed eye care professionals in the Vision In Preschoolers Study. Ophthalmology 2004;111(4):637‐50.
- Takai Y, Sato M, Tan R, Hirai T. Development of stereoscopic acuity: longitudinal study using a computer‐based random‐dot stereo test. Japanese Journal of Ophthalmology 2005;49(1):1‐5.
- Simons K. Stereoacuity norms in young children. Archives of Ophthalmology 1981;99(3):439‐45.
- Walraven J, Janzen P. TNO stereopsis test as an aid to the prevention of amblyopia. Ophthalmic & Physiological Optics 1993;13(4):350‐6.
- O’Connor AR, Birch EE, Anderson S, Draper H. The functional significance of stereopsis. Investigative Ophthalmology & Visual Science 2010;51(4):2019‐23.
- Rogers GL, Chazan S, Fellows R, Tsou BH. Strabismus surgery and its effect upon infant development in congenital esotropia. Ophthalmology 1982;89(5):479‐83.
- Chai Y, Shao Y, Lin S, Xiong KY, Chen WS, Li YY, et al. Vision‐related quality of life and emotional impact in children with strabismus: a prospective study. Journal of International Medical Research 2009;37(4):1108‐14.
- Koklanis K, Abel LA, Aroni R. Psychosocial impact of amblyopia and its treatment: a multidisciplinary study. Clinical and Experimental Ophthalmology 2006;34(8):743‐50.
- Costenbader FD. Infantile esotropia. Trans Am Ophthalmol Soc 1961;59:397-429.
- Infantile Esotropia. https://eyewiki.org/Infantile_Esotropia
- Worth C. squint, its causes and treatment. London: Bailliere, Tindall, and Cox, 1903.
- Chavasse FB. Worth’s squint on the binocular reflexes and the treatment of strabismus, 7th ed. Philadelphia: P.Blakiston’s Son & Co, 1939.
- Raab EL. Comitant esotropia. In: Wilson ME, Saunders RA, Trivedi RH. Pediatric ophthalmology: current thoughts and practicle guide. Leipzig. Springer;2009. p. 85-112.
- Elston J. Concomitant strabismus. In: Taylor D. Pediatric ophthalmology. 2nd ed. London: Blackwell science; 1997. p. 925-36.
- Brown syndrome. https://eyewiki.org/Brown_Syndrome
- Chew E, Rernaley N, Tamboli A, Jialiang Z, Podgor M, Klebanoff M. Risk factors for esotropia and exotropia. Arch Ophtahlmol. 10:112, 1994.
- Kanukollu VM, Sood G. Strabismus. [Updated 2021 Aug 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560782
- Vision in Preschoolers Study Group. Does assessing eye alignment along with refractive error or visual acuity increase sensitivity for detection of strabismus in preschool vision screening?. Investigative Ophthalmology & Visual Science 2007;48(7):3115‐25.
- Donahue SP, Arthur B, Neely DE, Arnold RW, Silbert D, Ruben JB, et al. Guidelines for automated preschool vision screening: a 10‐year, evidence‐based update. Journal of AAPOS 2013;17(1):4‐8.
- Solebo AL, Cumebrland PM, Rahi JS. Whole‐population vision screening in children aged 4‐5 years to detect amblyopia. Lancet 2015;385(9984):2308‐19.





{kind=link}