Straddle injury
Straddle injury is when trauma occurs to the groin area between the thighs such as coming down hard on something between your legs, such as a bicycle seat or crossbar, a fence, or playground equipment. Straddle injury can happen from straddling a hard object, or accidents such as falling onto a bicycle crossbar. Straddle injury can cause damage to the outer genitals. In women, this is the vulva. It includes the outer and inner labia and the clitoris. In men, this includes the scrotum, testes, and penis. The groin area will likely be bruised, bleeding, and painful. Straddle injury can also damage the tube that sends urine out of the body (urethra), especially for men. A straddle injury may also hurt the area between the genitals and the anus called the perineum. Severe straddle injury can cause breaks in bones in the pelvis. Falling on a sharp object can cause more severe damage to the area and damage to internal tissues, such as the vagina or rectum.
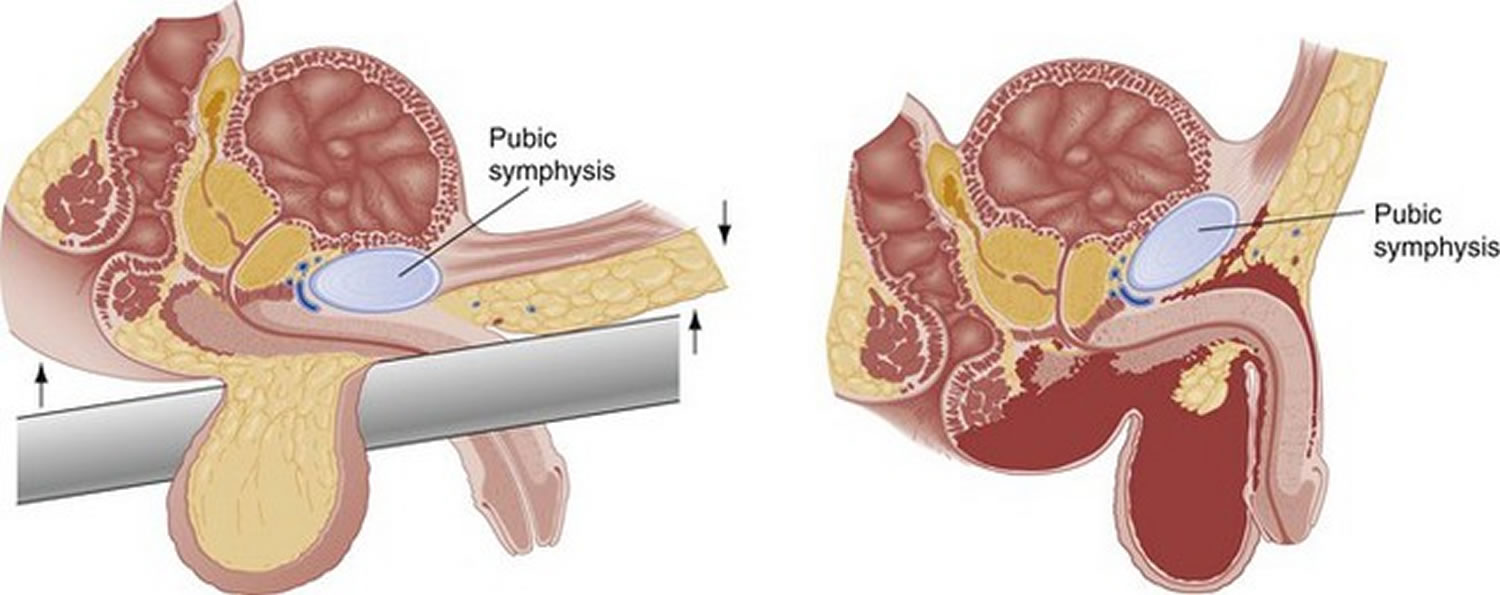
Straddle injuries usually involve only the bulbous urethra in men, which is crushed against the undersurface of the symphysis pubis. In contrast, posterior urethral injuries are distraction injuries accompanied by pelvic fracture injuries 1. If you have blood at the end of the penis or in the urine or can’t pass urine after an injury to the urethral area, you should see a health care provider right away. Your health care provider may try to pass a tube (“catheter”) through your urethra. Not being able to pass a tube into the urethra is the first sign of urethral injury. An x-ray is done after squirting a special dye into the urethra. The dye is used to be seen on an x-ray. X-rays are taken to see if any of the dye leaks out of the urethra inside your body. This would mean there’s an injury. An x-ray of the urethra is often done after a pelvic fracture, because urethral injury is common in these cases (about 1 in 10 cases).
The optimal treatment of bulbous urethral injuries remains controversial 2. Treatment should be aimed at preventing long-term complications, such as stricture, incontinence, and erectile dysfunction. Conventionally, anterior urethral injuries have been managed with initial suprapubic cystostomy and delayed repair if necessary. This approach allows for appropriate urinary drainage until the local edema and associated injuries have subsided 3. However, long-term suprapubic cystostomy is associated with wound infection, urinary tract infection, bladder calculi, patient discomfort, leakage, and dislodgment 4.
See your healthcare provider right away if you have any of these:
- Fever of 100.4°F (38°C) or higher, or as directed
- Pain that gets worse or isn’t better with medicine
- Other symptoms that don’t get better, or get worse
- Trouble urinating
- Blood in your urine
- Other new symptoms
Straddle injury female
Accidental genital trauma is most commonly caused by straddle injuries and is usually treatable by nonoperative management, and most of the injuries have a good prognosis 5. The types of injuries seen in the genital area vary from abrasion to contusion, lacerations, and hematoma. Injuries to the perineum occur in more than 20% of the patients, and injuries to the posterior fourchette and hymenal disruption (which are typically associated with sexual assault) are uncommon. In most of the cases, these straddle injuries are amenable to expectant management but sedation or operative intervention may be needed when complete examination cannot be performed or when the injuries are extensive 6.
Straddle injury female treatment
Straddle injury female treatment depends on the severity and type of injury sustained. Many studies demonstrate that most accidental genital injuries can be managed conservatively because an adequate assessment and examination in the emergency department without surgical management are possible in almost 80% of cases of accidental female genital trauma 7.
Conservative management should enable the patient to void spontaneously. Healing can be achieved by using the recommended conservative measures, including sitz bath and reduction in the physical activity during the critical healing phase, especially in the first 48 to 72 hours 8. Reduction in the activity level helps to ensure that the area is not reinjured before considerable healing has taken place 8.
Straddle injury causes
Straddle injury can happen in many ways, such as a sporting accident or falling while straddling any of these:
- Bicycle crossbar
- Fence or wall
- Gym equipment
- Edge of bathtub
- Arm of a couch or chair
- Diving board
Straddle injury symptoms
Symptoms of straddle injury:
- Pain
- Bruising
- Swelling
- Bleeding
- Trouble urinating, especially for men
- Nausea or vomiting, if testicles are damaged
- Blood blister under the skin called hematoma
Straddle injury complications
Possible complications of straddle injury:
- Infection
- Ongoing problems urinating and need for repair surgery
- Scar tissue.
Straddle injury diagnosis
An exam of the genitals may show injury to the urethra. If the health care provider suspects an injury, you may have the following tests:
- Retrograde urethrogram (an x-ray of the urethra using dye) for injury of urethra
- Retrograde cystogram (imaging of bladder) for injury of bladder
The exam may also show:
- Bladder injury or swollen (distended) bladder
- Other signs of pelvic injury, such as bruising over the penis, scrotum, and perineum
- Signs of hemorrhage or shock, including decreased blood pressure — especially in cases of pelvic fracture
- Tenderness and bladder fullness when touched (caused by urine retention)
- Tender and unstable pelvic bones
- Urine in the abdominal cavity
A catheter may be inserted once an injury of the urethra has been ruled out. This is a tube that drains urine from the body. An x-ray of the bladder using dye to highlight any damage can then be done.
Straddle injury treatment
Straddle injury treatments can include:
- Bandage. Your healthcare provider may put a bandage over any area that’s bleeding. Keep the bandage clean and dry. Change it as often as instructed.
- Cold compress. This is a cloth wet with cold water, or a cold pack from the refrigerator. It can help lessen swelling and pain. Wrap the cold pack with a thin cloth. Don’t put it directly on your skin. Put the cold compress on the area for 15 to 20 minutes, several times a day for 2 to 3 days.
- Sitz bath. This means sitting in a shallow tub of warm water. You can have a sitz bath in a bathtub. Or you can have a sitz bath using a special basin that fits over the rim of a toilet.
- Pain medicine. You may be given medicine to help relieve pain. Or you may be told to take over-the-counter medicine from a drugstore. Take the medicine as instructed.
- Suprapubic cystostomy. This is a thin, flexible tube (catheter) put into your bladder through a small cut in your lower belly. It’s used to drain urine while your urethra heals. A small plastic bag connects to the end of the tube to collect urine. The tube may be left in place for several weeks or more.
- Surgery. In some cases, the healthcare provider needs to make repairs to the area. The provider may stitch cuts in the skin or fix internal areas that are torn. Your provider will give you more information if you need surgery.
The treatment for urethral trauma depends on where and how bad the injury is. Many cases of anterior urethral injury need to be fixed right away with surgery.
Minor of these injuries can be treated with a catheter through the urethra into the bladder. This keeps urine from touching the urethra so it can mend. The catheter is often left in place for 14 to 21 days. After that time, an x-ray is taken to see if the injury has healed. If it has healed, the catheter can be taken out in the doctor’s office. If the x-ray still shows leaks, the catheter is left in longer.
If serious urethral trauma is seen on the x-ray, a tube is used to carry urine away from the injured area to keep it from leaking. Urine leaking inside the body can cause:
- Swelling
- Inflammation
- Infection
- Scarring
The treatment of a posterior urethral injury is very complicated. This is because it’s almost always seen with other severe injuries. Unfortunately, it means that this problem can’t be fixed right away. Most urologists first place a catheter in the bladder at the time of injury and wait for 3 to 6 months. This gives the body time to reabsorb the bleeding from the pelvic fracture. It’s also easier to fix the urethra after swelling in the tissues from a pelvic injury has gone down. Most posterior urethral injuries need an operation to connect the 2 torn edges of the urethra. This is most often done through a cut in the perineum.
If the urethra has completely torn away, urine must be drained. This is done with a tube stuck into the bladder through the skin (“suprapubic”). This Foley catheter goes through the skin just above the pubic bone in the lower belly into the bladder. This is most common after severe injuries. The tube can be put in at the time of abdominal surgery for other repairs. Or it can be done through a small puncture. An x-ray can be used to see that the catheter is in the bladder. Your doctor may suggest a procedure to rejoin the torn urethra over a catheter, which may help it heal.
Surgery
Urethral injury treatments should be designed to reconstruct urethral continuity and thereby to allow patients to void naturally. Also, treatments should prevent complications, such as stricture, impotence, and incontinence 9. Traumatic urethral injuries are often accompanied by multiple organ injuries. Furthermore, the extent and condition of injuries varies greatly 10. In addition, urethral injuries are relatively uncommon; thus, there is limited information on managing this injury and controversy remains with respect to the optimal management strategy 10.
Initial suprapubic cystostomy is the most popular treatment in the management of anterior urethral injuries 11.
However, Hadjizacharia et al. 4 reported that all patients who had long-term suprapubic cystostomy tubes developed strictures. Those authors suggested that the urethra is not adequately repositioned and large distraction may occur, resulting in complicated strictures, which often require a complex flap or graft urethroplasty. In addition, long-term suprapubic diversion can cause problems such as wound infection, urinary tract infection, bladder calculi, leakage and dislodgement, and patient discomfort 12. When patients were treated with immediate primary repair, it was possible to reduce the duration of discomfort and the course of disease 2.
The process of immediate endoscopic realignment of the urethra has rapidly progressed owing to modern endourologic developments. Several studies have reported encouraging results of immediate endoscopic realignment 4. Ying-Hao et al. 13 evaluated 16 men who had bulbar urethral disruption with endoscopic realignment and reported that all cases were successfully treated in a single session without intraoperative or postoperative complications. However, so far, there is controversy regarding postoperative stricture, complications such as impotence and incontinence, and pelvic abscess 14. With attempted urethral “realignment” over a urethral catheter, the rate of stenosis increases from -10 to -65% in incomplete disruption and from -75 to -100% in complete disruption 14.
According to a previous study, immediate primary surgical reconstruction is particularly difficult technically owing to the presence of acutely inflamed tissue, hematoma, and anatomical distortion. As a result, the surgical outcome was poor and complications such as impotence and incontinence occurred more frequently 15. However, there have been few studies on the immediate primary reconstruction of the urethra. The studies that are available involved sample sizes that were too small and were based on data that were too old. Also, the studies dealt with the posterior urethral disruptions associated with major trauma.
References- Mundy AR, Andrich DE. Urethral trauma. Part I: introduction, history, anatomy, pathology, assessment and emergency management. BJU Int. 2011;108:310–327.
- Gong IH, Oh JJ, Choi DK, Hwang J, Kang MH, Lee YT. Comparison of immediate primary repair and delayed urethroplasty in men with bulbous urethral disruption after blunt straddle injury. Korean J Urol. 2012;53(8):569–572. doi:10.4111/kju.2012.53.8.569 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3427843
- Armenakas NA, McAninch JW. Acute anterior urethral injuries: diagnosis and initial management. In: McAninch JW, editor. Traumatic and reconstructive urology. Philadelphia: Saunders; 1996. pp. 543–561.
- Hadjizacharia P, Inaba K, Teixeira PG, Kokorowski P, Demetriades D, Best C. Evaluation of immediate endoscopic realignment as a treatment modality for traumatic urethral injuries. J Trauma. 2008;64:1443–1449.
- Hwang HJ, Lim HW, Han YS, Choi JI, Kim MJ. Hematocolpos as a Result of Delayed Treatment of Acute Straddle Injury in an Adolescent Girl. Case Rep Obstet Gynecol. 2016;2016:1987690. doi:10.1155/2016/1987690 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4779825
- Iqbal C. W., Jrebi N. Y., Zielinski M. D., et al. Patterns of accidental genital trauma in young girls and indications for operative management. Journal of Pediatric Surgery. 2010;45(5):930–933. doi: 10.1016/j.jpedsurg.2010.02.024
- Spitzer R. F., Kives S., Caccia N., Ornstein M., Goia C., Allen L. M. Retrospective review of unintentional female genital trauma at a pediatric referral center. Pediatric Emergency Care. 2008;24(12):831–835. doi: 10.1097/PEC.0b013e31818ea064
- Deligeoroglou E., Iavazzo C., Sofoudis C., Kalampokas T., Creatsas G. Management of hematocolpos in adolescents with transverse vaginal septum. Archives of Gynecology and Obstetrics. 2012;285(4):1083–1087. doi: 10.1007/s00404-011-2114-4
- Koraitim MM. Pelvic fracture urethral injuries: the unresolved controversy. J Urol. 1999;161:1433–1441.
- Martinez-Pineiro L, Djakovic N, Plas E, Mor Y, Santucci RA, Serafetinidis E, et al. EAU Guidelines on Urethral Trauma. Eur Urol. 2010;57:791–803.
- Hernandez J, Morey AF. Anterior urethral injury. World J Urol. 1999;17:96–100.
- Ku JH, Kim ME, Jeon YS, Lee NK, Park YH. Management of bulbous urethral disruption by blunt external trauma: the sooner, the better? Urology. 2002;60:579–583.
- Ying-Hao S, Chuan-Liang X, Xu G, Guo-Qiang L, Jian-Guo H. Urethroscopic realignment of ruptured bulbar urethra. J Urol. 2000;164:1543–1545.
- Park S, McAninch JW. Straddle injuries to the bulbar urethra: management and outcomes in 78 patients. J Urol. 2004;171(2 Pt 1):722–725.
- Chapple C, Barbagli G, Jordan G, Mundy AR, Rodrigues-Netto N, Pansadoro V, et al. Consensus statement on urethral trauma. BJU Int. 2004;93:1195–1202.





{kind=link}