
What are thiazide diuretics
Thiazide diuretics are the most commonly used oral diuretics (drug that increases urine flow) and are widely used in the therapy of hypertension and congestive heart failure, as well as the treatment of edema due to local, renal and hepatic causes.
Thiazide diuretics act directly on your kidneys and promote diuresis (urine flow) by inhibiting the sodium/chloride cotransporter located in the distal convoluted tubule of a nephron (the functional unit of a kidney). Thiazides decrease sodium reabsorption which increases fluid loss in urine, which in turn decreases extracellular fluid and plasma volume. This reduces cardiac output (how hard the heart has to work to pump blood around the body) and lowers blood pressure. Thiazides also work in other ways to lower blood pressure. Thiazides also cause potassium loss while retaining calcium.
Thiazides are usually used for their blood pressure lowering effects because their diuretic activity is relatively weak compared to some other types of diuretic (such as loop diuretics).
The thiazide diuretics are grouped together based upon shared chemical, sulfonamide-like, structure. More recently non-benzothiazide drugs with a similar mechanism of action have been developed (metolazone, indapamide), which are referred to as thiazide-like diuretics. The thiazide and thiazide-like diuretics are all available generically and differ largely in their pharmacokinetic properties of oral availability, relative potency, serum and effective half-life and route of elimination. The general indications for the thiazide diuretics are treatment of hypertension and edema.
Thiazide diuretics are available in multiple forms and all are available generically.
Common side effects of the thiazide and thiazide-like diuretics include nausea, dizziness, headache, polyuria, dehydration, hyponatremia, hypokalemia and hypomagnesia. Chronic therapy may be associated with hyperuricemia and gout, and possibly an increased risk of cholecystitis. Many of the thiazide diuretics are also available in fixed dose combination with other antihypertensive medications or with potassium-sparing diuretics.
Thiazide diuretics list
Bendroflumethiazide is available in tablets of 2.5 mg in generic forms; recommended oral doses in adults are 2.5 to 10 mg in two divided doses. It is also available in a fixed dose with nadolol generically and under the brand name Corzide.
Chlorothiazide is available in tablets of 250 and 500 mg generically and under the trade name of Diuril; recommended oral doses in adults are 500 to 1000 mg once or twice daily.
Chlorthalidone is available in tablets of 25 and 50 mg generically and under the brand name of Thalitone; recommended oral doses in adults are 25 to 100 mg once daily or 100 mg every other day.
Hydrochlorothiazide is available in tablets of 25 and 50 mg and as capsules of 12.5 mg generically and under the trade names of Hydrodiuril, Microzide and Esidrix; recommended oral doses in adults are 12.5 to 50 mg daily given in one or two divided doses.
Methyclothiazide is available in tablets of 2.5 and 5 mg generically and under the trade name of Enduron; recommended oral doses in adults are 2.5 to 5 mg once daily.
Polythiazide is available in tablets of 1, 2 and 4 mg generically and under the trade name of Renese; typical oral doses in adults are 2 to 4 mg in one or two divided doses daily.
Metolazone is a thiazide-like diuretic that is available as tablets of 2.5 and 5 mg generically and under the trade name of Zaroxolyn; recommended oral doses in adults are 2.5 to 20 mg once daily.
Indapamide is a thiazide-like diuretic that is available as tablets of 1.25 and 2.5 mg generically and under the trade name of Lozol; recommended oral doses in adults are 1.25 to 5 mg once daily.
Thiazide diuretics mechanism of action
Thiazides achieve their diuretic action via inhibition of the Na+/Cl− cotransporter in the renal distal convoluted tubule 1. As a result, there is increased excretion of sodium and water and an associated loss of potassium. Chronic thiazide diuretics therapy may also result in increase calcium and magnesium loss. The Na+/Cl− cotransporter facilitates the absorption of sodium from the distal tubules back to the interstitium and accounts for approximately 7% of total sodium reabsorption 2. By decreasing sodium reabsorption, thiazide use acutely results in an increase in fluid loss to urine, which leads to decreased extracellular fluid (ECF) and plasma volume. This volume loss results in diminished venous return, increased renin release, reduced cardiac output and decreased blood pressure 3. Within days, the reduction in cardiac output increases total peripheral resistance, which stems mostly from activation of the sympathetic nervous system and renin–angiotensin–aldosterone system (RAAS) 4. This acute effect is evidenced by the fact that an infusion of dextran, a volume expander, during the acute thiazide treatment phase restores blood pressure to pretreatment levels 5.
Thiazide diuretics mechanism of action
Diuretic
- Thiazides are sulfonamide related organic acids that are secreted into the proximal tubule by an organic secretory mechanism. (Thiazides compete for the same secretory process by which uric acid is secreted into the proximal tubule).
- From within the lumen they act to increase the excretion of sodium (Na) and chloride (Cl) by inhibiting the Na/Cl symporter in the distal convoluted tubule. Natriuresis may be accompanied by some loss of potassium and bicarbonate.
- Thiazides enhance calcium (Ca) reabsorption in the distal convoluted tubule, by increasing Na/Ca exchange (which makes thiazides useful in treating the calcium-subtype of kidney stones).
- Thiazide diuretics also reduce the urinary excretion of calcium (Ca) and therefore are employed to treat kidney stones & may be useful for treating osteoporosis.
Antihypertensive effects
- The mechanism for the antihypertensive effects of thiazides is poorly understood. One hypothesis proposed is that thiazides produce a smooth muscle vasodilator effect initiated by a reduction in plasma Na levels, which thereby reduce intracellular Ca levels in vascular smooth muscle via Na/Ca exchange 6. However, other reasonable hypotheses have also been proposed 7.
Figure 1. Thiazide mechanism of action
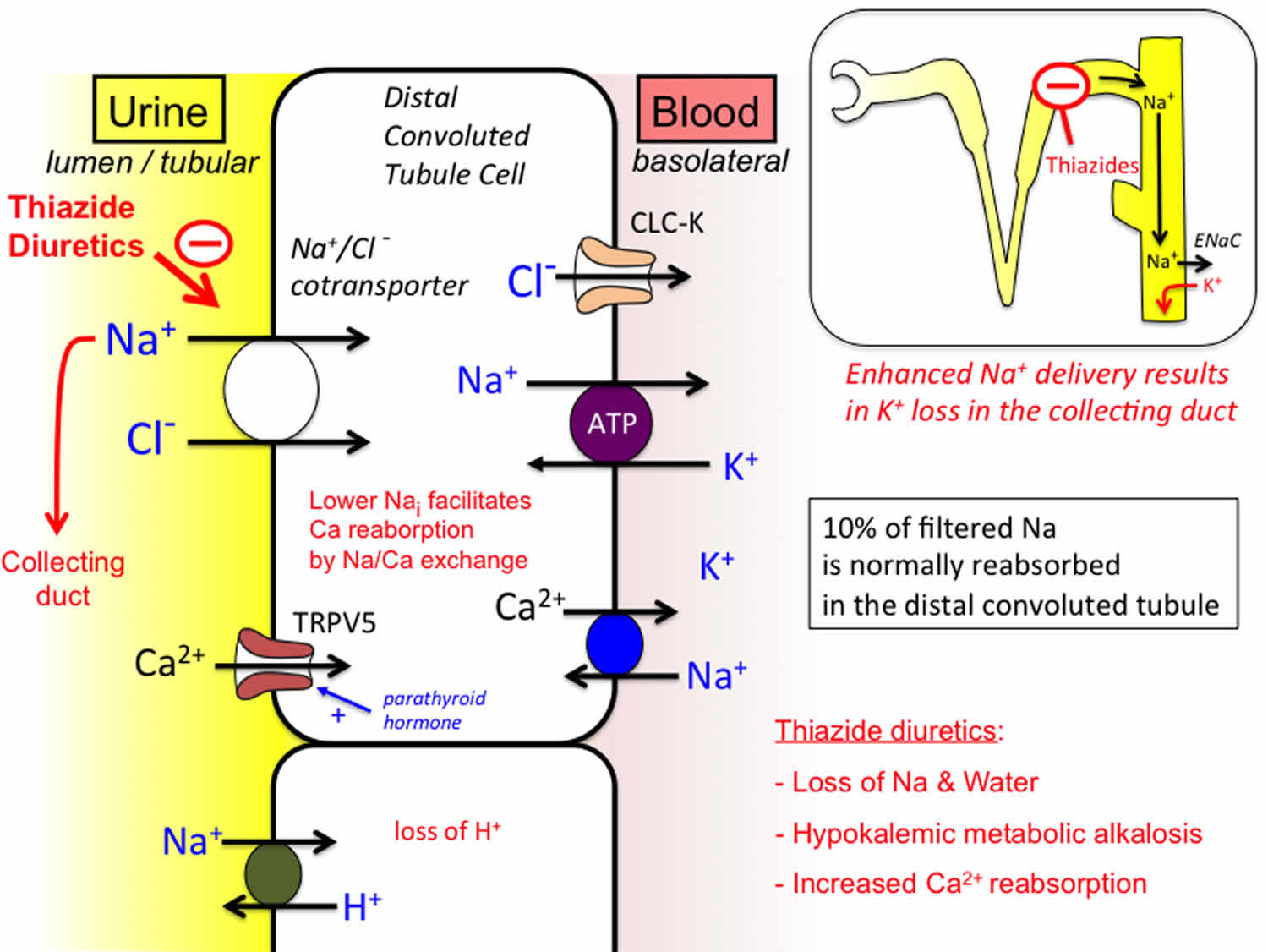
Footnote: Thiazide diuretics compete for the chloride binding site on the Na/Cl cotransporter that is selectively expressed in the distal convoluted tubule, inhibiting its ability to transport ions (Tran et al, 1990; Brater, 2015). Inhibition of this cotransporter lowers intracellular Na, which in turn results in a lowering of intracellular calcium mediated by Na/Ca exchange expressed on the basolateral membrane. This facilitates the diffusion of calcium through calcium ion channels expressed on the lumen membrane. The inhibition of Na transport in this segment results in greater delivery of sodium to the collecting duct (see inset), where enhanced Na influx through epithelial Na channels stimulates potassium efflux, which can result in the development of hypokalemia. CLC-K: Voltage-gated chloride channel; TRPV5: Transient receptor potential cation channel subfamily 5 (a calcium selective channel).
[Source 8 ]Chronically, however, thiazides must lower blood pressure via some other mechanism. Plasma and extracellular fluid (ECF) volumes almost fully recover within 4–6 weeks of thiazide initiation, yet blood pressure reduction is maintained 4. After chronic administration, discontinuation of thiazides result in a decrease in renin levels and rapid volume replenishment, although the rise in blood pressure is much slower 9. In addition, when given a dextran infusion, patients taking thiazides over longer periods of time (>2 months) experience an expansion of body fluid volume but blood pressure does not increase to baseline 9. In addition, if diuretics simply lowered blood pressure by reducing plasma volume, then one would expect loop diuretics (such as furosemide, torsemide and bumetanide), which are superior diuretics to thiazides, to be superior antihypertensives. However, loop diuretics do not lower blood pressure to the degree thiazides do (although some difficulty exists in establishing equivalent doses) 10. The aforementioned evidence indicates that the chronic thiazide antihypertensive effect is not exclusively due to a loss of blood volume.
Research has shown for decades that a decrease in total peripheral resistance plays an important role in the antihypertensive effect of thiazide diuretics over the long term 3. However, the mechanism of this decrease in total peripheral resistance has not been fully elucidated. Many hypotheses exist to describe this mechanism, with varying amounts of evidence to support them 11.
Despite decades of use and study, much of the data regarding thiazide mechanisms of action are in conflict. Most of the blood pressure-lowering mechanistic studies are small, in vitro projects using animal rather than human tissue, and many are more than 20 years old. In many of these older studies, the diuretic doses (or equivalent in vitro concentrations) used were 50 mg of hydrochlorothiazide or more 11. Current guidelines recommend 50 mg as the maximum dose of hydrochlorothiazide for the treatment of hypertension [2], and today clinicians do not often prescribe doses greater than 25 mg of hydrochlorothiazide or its equivalent for hypertension. It is uncertain whether many noted effects witnessed in these older studies would be observed using lower doses 11.
Recently, there has been controversy over the long-held notion that all thiazides act similarly. The theory that all thiazides do not have a similar efficacy or mechanism of action would help explain the conflicting findings in many studies investigating their blood pressure-lowering and metabolic effects, and has been addressed previously by others 12. Evidence already exists documenting the differences between chlorthalidone and hydrochlorothiazide, although whether they exhibit differential effects on clinical outcomes is unclear 13. Regardless, the mechanisms by which thiazides exert blood pressure-lowering and metabolic effects remain incompletely understood. From the current evidence, thiazides appear to exert their effects via multiple complex and interacting mechanisms.
Thiazide diuretics drug interactions
Major drug interactions:
- Since thiazides must be secreted into the tubular lumen to inhibit the Na/Cl symporter, their action can be reduced by drugs such as probenecid which compete for transport into the proximal tubule.
- Hypokalemia caused by thiazide & loop diuretics can increase the likelihood of potentially fatal polymorphic ventricular tachycardia (torsade de pointes) if coadministered with other drugs that prolong the QT interval (e.g. Class III antiarrhythmic, or quinidine-like drugs).
- Alcohol, barbiturates & narcotics may potentiate orthostatic hypotension
- Additive effects occur when combined with other antihypertensives
- Decreased response to pressor amines
- Dosage adjustment of antidiabetic drugs may be necessary.
Using chlorothiazide with other drugs that make you dizzy can worsen this effect. Ask your doctor before using opioid medication, a sleeping pill, a muscle relaxer, or medicine for anxiety or seizures.
Tell your doctor about all your other medicines, especially:
- other blood pressure medications;
- cholestyramine or colestipol;
- lithium;
- insulin or oral diabetes medicine;
- steroid medicine; or
- NSAIDs (nonsteroidal anti-inflammatory drugs)–aspirin, ibuprofen (Advil, Motrin), naproxen (Aleve), celecoxib, diclofenac, indomethacin, meloxicam, and others.
This list is not complete. Other drugs may affect chlorothiazide, including prescription and over-the-counter medicines, vitamins, and herbal products. Not all possible drug interactions are listed here.
Thiazide diuretics side effects
Common side effects may include:
- dizziness, spinning sensation;
- numbness or tingling;
- diarrhea, constipation, stomach cramps;
- blurred vision;
- muscle spasm; or
- impotence, sexual problems.
This is not a complete list of side effects and others may occur. Call your doctor for medical advice about side effects.
Get emergency medical help if you have signs of an allergic reaction (hives, difficult breathing, swelling in your face or throat) or a severe skin reaction (fever, sore throat, burning eyes, skin pain, red or purple skin rash with blistering and peeling).
Call your doctor at once if you have:
- a light-headed feeling, like you might pass out;
- little or no urination;
- severe pain in your upper stomach spreading to your back;
- low blood cell counts–pale or yellowed skin, dark colored urine, fever, easy bruising or bleeding; or
- signs of an electrolyte imbalance–dry mouth, increased thirst or urination, confusion, vomiting, constipation, muscle pain or weakness, leg cramps, dizziness, drowsiness, lack of energy, feeling restless, fast heartbeats, tingly feeling.
Symptoms of a thiazide overdose include:
- Confusion
- Dizziness, fainting
- Drowsiness
- Dry mouth
- Fever
- Frequent urination, pale-colored urine
- Heart rhythm problems
- Low blood pressure
- Muscle cramps and twitching
- Nausea, vomiting
- Rash
- Seizures
- Skin sensitive to sunlight, yellow skin
- Slow breathing
- Vision problems (things you see look yellow)
- Weakness
- Coma (unresponsiveness)
Metabolic
Dose related metabolic changes (primarily observed with doses higher than used in the current standard of care):
- Hypokalemic metabolic alkalosis: with the low doses commonly used <25% of patients develop hypokalemia & most cases are not severe 14.
- Hyperuricemia can be aggrevated by treatment with thiazide diuretics, potentially leading to the development of gout 15. Both thiazide and loop diuretics interfere with different transporters involved in urate secretion (see Figure 6 in the module on Gout.
- Hyperglycemia: Thiazides have a mild effect to impaire glucose tolerance. This is normally of little clinical significance at therapeutic doses – but may increase hyperglycemia in a type 2 diabetic. There is evidence that the hyperglycemia may be related to loss of body potassium, which may affect the ability of pancreatic beta cells to regulate the release of insulin via ATP-sensitive K channels. Appropriate correction of hypokalemia can typically reverse thiazide-induced hyperglycemia 16.
- Hyperlipidemia: Dyslipidemia can by produced by high doses of thiazides (not typically used). The mechanism by which thiazides and some beta blockers affect lipid levels is still poorly understood.
- Hyponatremia
Cardiovascular
Cardiovascular complications of diuretic therapy include orthostatic hypotension secondary to intravascular volume depletion. This has resulted in syncope and, in some patients with glaucoma, temporary loss of vision. Rare cases of cerebrovascular accident associated with thiazide-induced diuresis have been reported.
Hypersensitivity
Thiazides may induce allergic reactions in patients who are allergic to sulfonamides.
Hypersensitivity reactions usually involve the skin (cutaneous vasculitis, urticaria, rash, purpura), but may involve the gastrointestinal system (nausea, vomiting, or diarrhea), the genitourinary system (interstitial nephritis), and the respiratory system (acute noncardiogenic pulmonary edema, pneumonitis). Thiazide diuretics may induce phototoxic dermatitis.
Dermatologic
Dermatologic reactions may indicate hypersensitivity to the drug. Erythema multiforme, Stevens-Johnson syndrome, exfoliative dermatitis (including toxic epidermal necrolysis), and alopecia have been reported in rare cases.
Gastrointestinal
Gastrointestinal problems include diarrhea, vomiting, constipation or abdominal pain in approximately 5% of patients. Thiazide diuretics have been associated with acute cholecystitis and rare cases of pancreatitis.
A retrospective case-control drug surveillance study has revealed the relative risk of acute cholecystitis associated with the use of a thiazide diuretic is 2.0. The suspected explanation for this association is the potentially deleterious effect thiazides have on the serum lipid profile. Chlorothiazide-induced hypercholesterolemia or hypertriglyceridemia may enhance the formation of some types of gallstones.
Renal
Renal side effects including new or worsened renal insufficiency associated with chlorothiazide therapy is a probable sign of intravascular volume depletion, and serves as a signal to reduce or withhold therapy. Rare cases of allergic interstitial nephritis have been associated with chlorothiazide.
Endocrine
Endocrinologic changes associated with chlorothiazide, as with other thiazide diuretic agents, include decreased glucose tolerance and a potentially deleterious effect on the lipid profile. This may be important in some patients with or who are at risk for diabetes or coronary artery disease.
Hematologic
Hematologic side effects are rare. Rare cases of immune-complex hemolytic anemia, aplastic anemia, and thrombocytopenia have been associated with thiazide diuretics.
Musculoskeletal
Musculoskeletal cramping or spasms have occasionally been reported during chlorothiazide diuresis.
Genitourinary
Genitourinary problems have been limited to rare complaints of impotence among male patients.
References- Mechanisms for blood pressure lowering and metabolic effects of thiazide and thiazide-like diuretics. Expert Rev Cardiovasc Ther. 2010 Jun; 8(6): 793–802. doi: 10.1586/erc.10.27 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2904515/
- Sodium and potassium in the pathogenesis of hypertension. Adrogué HJ, Madias NE. N Engl J Med. 2007 May 10; 356(19):1966-78.
- Hemodynamic and hypotensive effects of long-term therapy with chlorothiazide. CONWAY J, LAUWERS P. Circulation. 1960 Jan; 21():21-7.
- Hemodynamic changes during long-term thiazide treatment of essential hypertension in responders and nonresponders. van Brummelen P, Man in ‘t Veld AJ, Schalekamp MA. Clin Pharmacol Ther. 1980 Mar; 27(3):328-36.
- Relationship between plasma and extracellular fluid volume depletion and the antihypertensive effect of chlorothiazide. WILSON IM, FREIS ED. Circulation. 1959 Dec; 20():1028-36.
- Adrogue HJ, Madias NE (2007): Sodium and potassium in the pathogenesis of hypertension. N Eng J Med 356:1966-1978.
- Ernst ME, Moser M (2009): Use of diuretics in patients with hypertension. N Engl J Med 361:2153-2164.
- Thiazide Diuretics. http://tmedweb.tulane.edu/pharmwiki/doku.php/thiazides
- The antihypertensive actions of benzothiadiazines. WINER BM. Circulation. 1961 Feb; 23():211-8.
- A comparison of the effects of hydrochlorothiazide and of frusemide in the treatment of hypertensive patients. Anderson J, Godfrey BE, Hill DM, Munro-Faure AD, Sheldon J. Q J Med. 1971 Oct; 40(160):541-60.
- Duarte JD, Cooper-DeHoff RM. Mechanisms for blood pressure lowering and metabolic effects of thiazide and thiazide-like diuretics. Expert Rev Cardiovasc Ther. 2010;8(6):793-802. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2904515/
- How do thiazide and thiazide-like diuretics lower blood pressure? Hughes AD. J Renin Angiotensin Aldosterone Syst. 2004 Dec; 5(4):155-60.
- Hydrochlorothiazide versus chlorthalidone: evidence supporting their interchangeability. Carter BL, Ernst ME, Cohen JD. Hypertension. 2004 Jan; 43(1):4-9.
- Saseen JJ (2009): Essential Hypertension. In: Applied Therapeutics. The Clinical Use of Drugs. 9th Edition. Lippincott Williams & Wilkins. Koda-Kimble MA et al (Editors). Baltimore MD. pg 13-21.
- Becker MA (2016): Diuretic-induced hyperuricemia and gout. In UpToDate, Basow, DS (Ed), Waltham, MA.
- Zillich AJ, et al (2006): Thiazide diuretics, potassium, and the development of diabetes: a quantitative review. Hypertension 48:219-224.





{kind=link}