What is a tonic clonic seizure
Generalized tonic-clonic seizure previously known as ‘grand mal seizure’, is a that seizure begins with a sudden loss of consciousness, the body then becomes stiff followed by jerking of the muscles. Turning red or blue, tongue-biting and loss of bladder control are common. Confusion, drowsiness, memory loss, headache and agitation can occur on regaining consciousness.
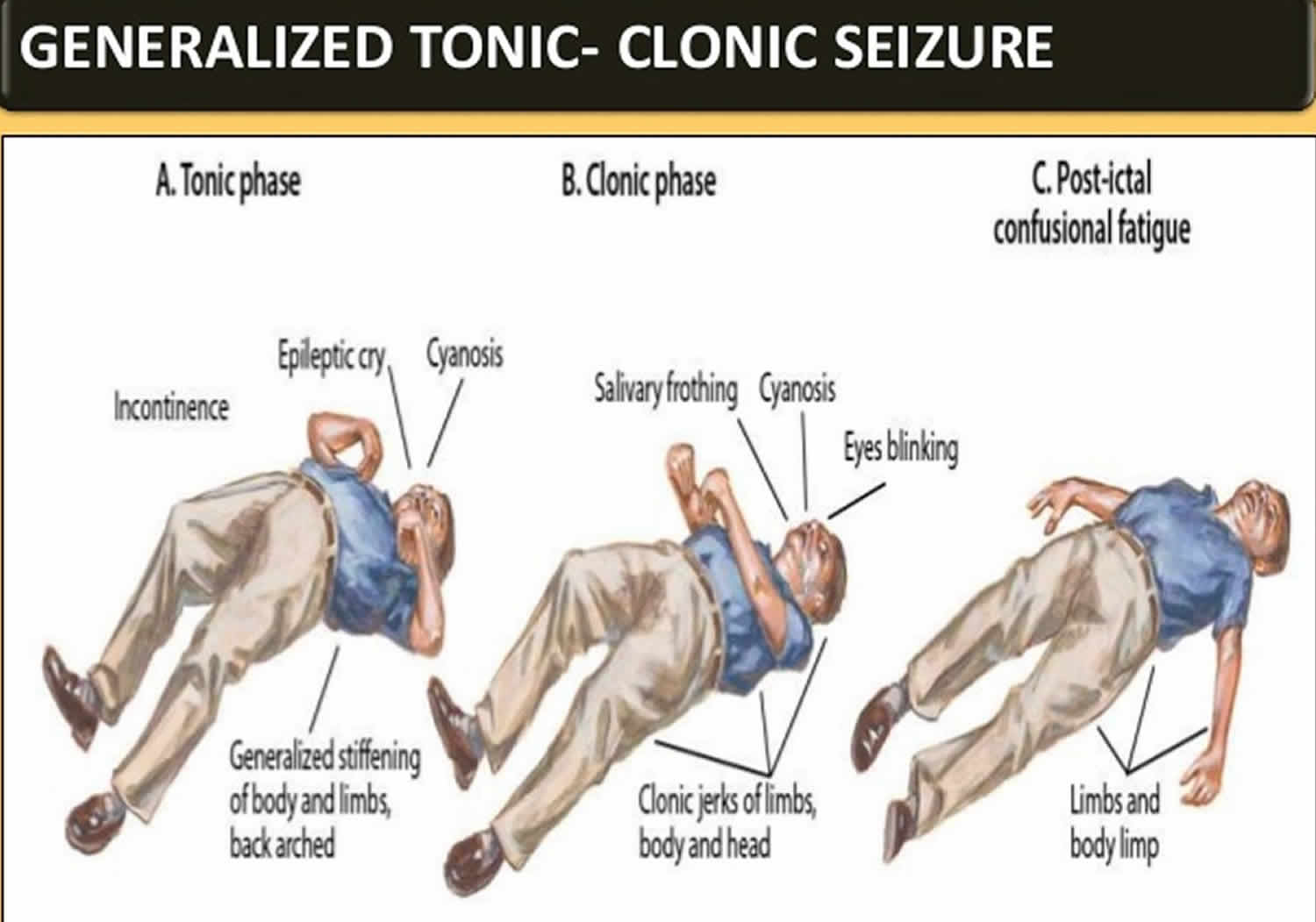
At the start of a generalized tonic clonic seizure:
- the person becomes unconscious
- their body goes stiff and if they are standing up they usually fall backwards
- they may cry out
- they may bite their tongue or cheek.
During a generalized tonic clonic seizure:
- they jerk and shake (convulse) as their muscles relax and tighten rhythmically
- their breathing might be affected and become difficult or sound noisy
- their skin may change colour and become very pale or bluish
- they may wet themselves.
After a generalized tonic clonic seizure (once the jerking stops):
- their breathing and colour return to normal
- they may feel tired, confused, have a headache or want to sleep.
Tonic clonic seizure what to do?
If you see someone having a seizure or fit, there are some simple things you can do to help. You should call an ambulance if you know it’s their first seizure or it’s lasting longer than 5 minutes.
It might be scary to witness, but don’t panic.
- Do not try to restrain the person or stop the jerking.
- Don’t try to move them. Only move them if they’re in danger – such as near a busy road or hot cooker.
- Don’t put anything in their mouth, including your fingers. They shouldn’t have any food or drink until they fully recover.
- Protect the patient from harming themselves.
- Put something soft under their head.
- Loosen any tight clothing around their neck – such as a collar or tie to – aid breathing
- Time the seizure.
- Put them on their side in the recovery position as soon as the jerking stops, or immediately if they have vomited or have food or fluid in their mouth.
- Don’t wake them up, but do check their breathing.
- Look after any injuries they may have.
If they’re in a wheelchair, put the brakes on and leave any seatbelt or harness on. Support them gently and cushion their head, but don’t try to move them.
Call your local emergency services number if:
- the seizure continues for more than 5 minutes or a second seizure quickly follows
- the patient remains unresponsive for more than 5 minutes after a seizure stops
- the patient has been injured
- the patient has diabetes or is pregnant
- you know, or believe it to be the patient’s first seizure.
People with epilepsy don’t always need to go to hospital every time they have a seizure.
Some people with epilepsy wear a special bracelet or carry a card to let medical professionals and anyone witnessing a seizure know they have epilepsy.
Figure 1. Recovery position

Tonic vs Clonic seizure
Tonic seizure causes stiffening of muscles of the body, generally those in the back, legs, and arms.
Clonic seizure causes repeated jerking movements of muscles on both sides of the body.
Both tonic and clonic seizures are part of generalized seizure, which are a result of abnormal neuronal activity that rapidly emerges on both sides of the brain. These seizures may cause loss of consciousness, falls, or a muscle’s massive contractions.
Not all seizures can be easily defined as either focal or generalized. Some people have seizures that begin as focal seizures but then spread to the entire brain. Other people may have both types of seizures but with no clear pattern.
Some people recover immediately after a seizure, while others may take minutes to hours to feel as they did before the seizure. During this time, they may feel tired, sleepy, weak, or confused. Following focal seizures or seizures that started from a focus, there may be local symptoms related to the function of that focus. Certain characteristics of the post-seizure (or post-ictal) state may help locate the region of the brain where the seizure occurred. A classic example is called Todd’s paralysis, a temporary weakness in the part of the body that was affected depending on where in the brain the focal seizure occurred. If the focus is in the temporal lobe, post-ictal symptoms may include language or behavioral disturbances, even psychosis. After a seizure, some people may experience headache or pain in muscles that contracted.
Tonic clonic seizure causes
Nerve cells (neurons) in your brain create, send and receive electrical impulses to each other, which allow your brain’s nerve cells to communicate and controls the way you function. Anything that disrupts these communication pathways can lead to a seizure. During a seizure these electrical signals are disrupted and this affects how you feel or what you do while the seizure is happening.
Sometimes there is a clear cause for seizures, for example, if someone has damage to their brain from a difficult birth, or an infection such as meningitis, a stroke or a head injury.
The likelihood of someone having seizures can also be partly genetic. This is sometimes inherited from one or both parents, but in some cases it may be from a change that happens only in the person’s own genes. So even if someone has a genetic tendency to having seizures, in many cases epilepsy is not inherited.
Genetic – information in the DNA in our cells that controls our characteristics, for example hair color, sex and height. Part of the genetic likelihood of developing seizures is called a seizure threshold. This is your individual level of resistance to seizures. Any of us could have a seizure under certain circumstances, but for most people, their natural resistance to having seizures is high enough to stop that happening. Your seizure threshold is one part of your genetic make-up which can be passed from parent to child. So the chance of you having seizures may depend partly on whether either or both of your parents has epilepsy. If you have a low seizure threshold, your brain is less resistant to seizures. So you are more likely to suddenly start having seizures for no obvious reason than someone with a high seizure threshold.
Your doctors may be able to tell you what has caused your seizures to start, but this is not always possible. Research continues into understanding more about why seizures happen in some people and not in others.
Your doctor or neurologist may be able to tell you what has caused your epilepsy, but this is not always possible. Research continues into understanding more about why seizures happen in some people and not in others.
Causes of seizures can sometimes be difficult to find. Some known causes of seizures include the following:
- Epilepsy. The most common cause of seizures is epilepsy. But not every person who has a seizure has epilepsy.
- Illegal (recreational) drugs
- Alcohol
- Extremely low blood sugar
- High fever
- Head injury
- Infection. The most common cause of epilepsy in developing countries and overall worldwide is infectious. Infections can cause both acute seizures and epilepsy. Tuberculosis, neurocysticercosis, cerebral toxoplasmosis, HIV, cerebral malaria, subacute sclerosing panencephalitis (SSPE), and bacterial and viral meningoencephalitis are some infections known to cause seizures.
- Brain tumors or other medical problems, including stroke.
- Developmental abnormalities
- Vascular lesions/AV malformations
- Meningitis/focal encephalitis
- Hypoxic brain injury
- Postsurgical changes
- Electrolyte imbalance like hyponatremia or hypocalcemia
- Endocrine disorders
- Metabolic: Several inherited enzymatic disorders like GLUT-1 deficiency, cerebral folate deficiency, among others can cause seizures.
- Medications and toxins
- Genetic/chromosomal abnormalities: Several chromosomal disorders (e.g., AKT3, Fragile X syndrome) and gene defects (e.g., Down’s syndrome, Klinefelter’s syndrome, Angelman syndrome) have been associated with epilepsy.
The cause cannot be determined in more than half of all individuals with epilepsy. Congenital anomaly is the most common known cause in children, and head trauma in young adults. In people, age 35 to 64 years, head trauma, tumors, and vascular disorders are common causes. In people age 65 years or more, cerebrovascular disease, and degenerative disorders are most common known causes.
Seizures can be brought on by certain situations or triggers. Some common triggers include tiredness and lack of sleep, stress, alcohol, fever, acute medical illness, substance abuse, hormonal changes and medication noncompliance 1 . The triggers should be avoided wherever possible.
Common triggers include:
- flashing or flickering lights
- lack of sleep
- stress
- alcohol
- missed medication taken for seizures.
A common cause of seizures in childhood is a perinatal hypoxic brain injury. In adolescents, seizures are most commonly caused by head trauma and encephalitis. Brain tumors are the most common cause of seizures in middle-aged adults, and vascular dementia and encephalopathies are the most common etiology in older adults 2.
Important: Anyone taking prescribed medicines for seizures should always take the correct dosage and make sure they do not miss a dose.
Genetics
Genetic mutations may play a key role in the development of certain epilepsies. Many types of epilepsy affect multiple blood-related family members, pointing to a strong inherited genetic component. In other cases, gene mutations may occur spontaneously and contribute to development of epilepsy in people with no family history of the disorder (called “de novo” mutations). Overall, researchers estimate that hundreds of genes could play a role in the disorders.
Several types of epilepsy have been linked to mutations in genes that provide instructions for ion channels, the “gates” that control the flow of ions in and out of cells to help regulate neuronal signaling. For example, most infants with Dravet syndrome, a type of epilepsy associated with seizures that begin before the age of one year, carry a mutation in the SCN1A gene that causes seizures by affecting sodium ion channels.
Genetic mutations also have been linked to disorders known as the progressive myoclonic epilepsies, which are characterized by ultra-quick muscle contractions (myoclonus) and seizures over time. For example, Lafora disease, a severe, progressive form of myoclonic epilepsy that begins in childhood, has been linked to a gene that helps to break down carbohydrates in brain cells.
Mutations in genes that control neuronal migration – a critical step in brain development – can lead to areas of misplaced or abnormally formed neurons, called cortical dysplasia, in the brain that can cause these mis-wired neurons to misfire and lead to epilepsy.
Other genetic mutations may not cause epilepsy, but may influence the disorder in other ways. For example, one study showed that many people with certain forms of epilepsy have an abnormally active version of a gene that results in resistance to anti-seizure drugs. Genes also may control a person’s susceptibility to seizures, or seizure threshold, by affecting brain development.
Other Disorders
Epilepsies may develop as a result of brain damage associated with many types of conditions that disrupt normal brain activity. Seizures may stop once these conditions are treated and resolved. However, the chances of becoming seizure-free after the primary disorder is treated are uncertain and vary depending on the type of disorder, the brain region that is affected, and how much brain damage occurred prior to treatment. Examples of conditions that can lead to epilepsy include:
- Brain tumors, including those associated with neurofibromatosis or tuberous sclerosis complex, two inherited conditions that cause benign tumors called hamartomas to grow in the brain
- Head trauma
- Alcoholism or alcohol withdrawal
- Alzheimer’s disease
- Strokes, heart attacks, and other conditions that deprive the brain of oxygen (a significant portion of new-onset epilepsy in elderly people is due to stroke or other cerebrovascular disease)
- Abnormal blood vessel formation (arteriovenous malformations) or bleeding in the brain (hemorrhage)
- Inflammation of the brain
- Infections such as meningitis, HIV, and viral encephalitis
Cerebral palsy or other developmental neurological abnormalities may also be associated with epilepsy. About 20 percent of seizures in children can be attributed to developmental neurological conditions. Epilepsies often co-occur in people with abnormalities of brain development or other neurodevelopmental disorders. Seizures are more common, for example, among individuals with autism spectrum disorder or intellectual impairment. In one study, fully a third of children with autism spectrum disorder had treatment-resistant epilepsy.
Seizure Triggers
Seizure triggers do not cause epilepsy but can provoke first seizures in those who are susceptible or can cause seizures in people with epilepsy who otherwise experience good seizure control with their medication. Seizure triggers include alcohol consumption or alcohol withdrawal, dehydration or missing meals, stress, and hormonal changes associated with the menstrual cycle. In surveys of people with epilepsy, stress is the most commonly reported seizure trigger. Exposure to toxins or poisons such as lead or carbon monoxide, street drugs, or even excessively large doses of antidepressants or other prescribed medications also can trigger seizures.
Sleep deprivation is a powerful trigger of seizures. Sleep disorders are common among people with the epilepsies and appropriate treatment of co-existing sleep disorders can often lead to improved control of seizures. Certain types of seizures tend to occur during sleep, while others are more common during times of wakefulness, suggesting to physicians how to best adjust a person’s medication.
For some people, visual stimulation can trigger seizures in a condition known as photosensitive epilepsy. Stimulation can include such things as flashing lights or moving patterns.
Tonic clonic seizure symptoms
Tonic-clonic seizures, previously known as grand mal seizures, are the most dramatic type of epileptic seizure and can cause an abrupt loss of consciousness, body stiffening and shaking, and sometimes loss of bladder control or biting your tongue.
At the start of a generalized tonic clonic seizure:
- the person becomes unconscious
- their body goes stiff and if they are standing up they usually fall backwards
- they may cry out
- they may bite their tongue or cheek.
During a generalized tonic clonic seizure:
- they jerk and shake (convulse) as their muscles relax and tighten rhythmically
- their breathing might be affected and become difficult or sound noisy
- their skin may change colour and become very pale or bluish
- they may wet themselves.
After a generalized tonic clonic seizure (once the jerking stops):
- their breathing and colour return to normal
- they may feel tired, confused, have a headache or want to sleep.
Warning signs
Some people who have seizures may get warning signs, such as a change in body temperature, visual problems or a strange taste in their mouth for example. These signs are also called ‘auras’. If these warnings occur, try to get to a safe place or position if possible.
Sometimes, other people can tell if someone they know is about to have a seizure. They may look different, their pupils may change size or they may act out of character. Again, if this happens, try to guide the person to a safe location.
People who have seizures should take precautions when swimming, driving or bathing.
Tonic clonic seizure diagnosis
After a seizure, your doctor will thoroughly review your symptoms and medical history. Your doctor may order several tests to determine the cause of your seizure and evaluate how likely it is that you’ll have another one.
Tests may include:
- A neurological exam. Your doctor may test your behavior, motor abilities and mental function to determine if you have a problem with your brain and nervous system.
- Blood tests. Your doctor may take a blood sample to check for signs of infections, genetic conditions, blood sugar levels or electrolyte imbalances.
- Lumbar puncture. If your doctor suspects an infection as the cause of a seizure, you may need to have a sample of cerebrospinal fluid removed for testing.
- An electroencephalogram (EEG). In this test, doctors attach electrodes to your scalp with a paste-like substance. The electrodes record the electrical activity of your brain, which shows up as wavy lines on an EEG recording. The EEG may reveal a pattern that tells doctors whether a seizure is likely to occur again. EEG testing may also help your doctor exclude other conditions that mimic epilepsy as a reason for your seizure. Depending on the details of your seizures, this test may be done as an outpatient in the clinic, overnight at home with an ambulatory device or over a few nights in the hospital.
- Computerized tomography (CT). A CT scan uses X-rays to obtain cross-sectional images of your brain. CT scans can reveal abnormalities in your brain that might cause a seizure, such as tumors, bleeding and cysts.
- Magnetic resonance imaging (MRI). An MRI scan uses powerful magnets and radio waves to create a detailed view of your brain. Your doctor may be able to detect lesions or abnormalities in your brain that could lead to seizures.
- Positron emission tomography (PET). A PET scan uses a small amount of low-dose radioactive material that’s injected into a vein to help visualize active areas of the brain and detect abnormalities.
- Single-photon emission computerized tomography (SPECT). A SPECT test uses a small amount of low-dose radioactive material that’s injected into a vein to create a detailed, 3-D map of the blood flow activity in your brain that happens during a seizure. Doctors also may conduct a form of a SPECT test called subtraction ictal SPECT coregistered to MRI (SISCOM), which may provide even more-detailed results. This test is usually done in a hospital with overnight EEG recording.
Imaging and Monitoring
An electroencephalogram, or EEG, can assess whether there are any detectable abnormalities in the person’s brain waves and may help to determine if antiseizure drugs would be of benefit. This most common diagnostic test for epilepsy records electrical activity detected by electrodes placed on the scalp. Some people who are diagnosed with a specific syndrome may have abnormalities in brain activity, even when they are not experiencing a seizure. However, some people continue to show normal electrical activity patterns even after they have experienced a seizure. These occur if the abnormal activity is generated deep in the brain where the EEG is unable to detect it. Many people who do not have epilepsy also show some unusual brain activity on an EEG. Whenever possible, an EEG should be performed within 24 hours of an individual’s first seizure. Ideally, EEGs should be performed while the person is drowsy as well as when he or she is awake because brain activity during sleep and drowsiness is often more revealing of activity resembling epilepsy. Video monitoring may be used in conjunction with EEG to determine the nature of a person’s seizures and to rule out other disorders such as psychogenic non-epileptic seizures, cardiac arrhythmia, or narcolepsy that may look like epilepsy.
A magnetoencephalogram (MEG) detects the magnetic signals generated by neurons to help detect surface abnormalities in brain activity. MEG can be used in planning a surgical strategy to remove focal areas involved in seizures while minimizing interference with brain function.
The most commonly used brain scans include CT (computed tomography), PET (positron emission tomography) and MRI (magnetic resonance imaging). CT and MRI scans reveal structural abnormalities of the brain such as tumors and cysts, which may cause seizures. A type of MRI called functional MRI (fMRI) can be used to localize normal brain activity and detect abnormalities in functioning. SPECT (single photon emission computed tomography) is sometimes used to locate seizure foci in the brain. A modification of SPECT, called ictal SPECT, can be very helpful in localizing the brain area generating seizures. In a person admitted to the hospital for epilepsy monitoring, the SPECT blood flow tracer is injected within 30 seconds of a seizure, then the images of brain blood flow at the time of the seizure are compared with blood flow images taken in between seizures. The seizure onset area shows a high blood flow region on the scan. PET scans can be used to identify brain regions with lower than normal metabolism, a feature of the epileptic focus after the seizure has stopped.
Medical History
Taking a detailed medical history, including symptoms and duration of the seizures, is still one of the best methods available to determine what kind of seizures a person has had and to determine any form of epilepsy. The medical history should include details about any past illnesses or other symptoms a person may have had, as well as any family history of seizures. Since people who have suffered a seizure often do not remember what happened, caregiver or other accounts of seizures are vital to this evaluation. The person who experienced the seizure is asked about any warning experiences. The observers will be asked to provide a detailed description of events in the timeline they occurred.
Blood Tests
Blood samples may be taken to screen for metabolic or genetic disorders that may be associated with the seizures. They also may be used to check for underlying health conditions such as infections, lead poisoning, anemia, and diabetes that may be causing or triggering the seizures. In the emergency department it is standard procedure to screen for exposure to recreational drugs in anyone with a first seizure.
Developmental, Neurological, and Behavioral Tests
Tests devised to measure motor abilities, behavior, and intellectual ability are often used as a way to determine how epilepsy is affecting an individual. These tests also can provide clues about what kind of epilepsy the person has.
Tonic clonic seizure treatment
Not everyone who has one seizure will have another one, and because a seizure can be an isolated incident, your doctor may not decide to start treatment until you’ve had more than one.
The optimal goal in seizure treatment is to find the best possible therapy to stop seizures, with the fewest side effects.
Tonic clonic seizure medication
More than 20 different antiseizure medications are available today, all with different benefits and side effects. Most seizures can be controlled with one drug (called monotherapy). Deciding on which drug to prescribe, and at what dosage, depends on many different factors, including seizure type, lifestyle and age, seizure frequency, drug side effects, medicines for other conditions, and, for a woman, whether she is pregnant or will become pregnant. It may take several months to determine the best drug and dosage. If one treatment is unsuccessful, another may work better. Benzodiazepines such as diazepam, midazolam, or lorazepam are accepted as the first line medications for continuing seizures.
Many medications are used in the treatment of epilepsy as first-line or add-on. They can be grouped based on their mechanism of action. Sodium channel blockers (carbamazepine, oxcarbazepine, eslicarbazepine, phenytoin, fosphenytoin, lamotrigine, lacosamide, and zonisamide), potassium channel opener (ezogabine), agonist of GABA receptor (benzodiazepine and barbiturates), GABA reuptake inhibitors (tiagabine), inhibitors of GABA-transaminase (vigabatrin), multiple mechanisms (gabapentin, pregabalin, valproic acid), glutamate antagonists (topiramate, felbamate, perampanel), and binding to synaptic vesicle 2A protein (levetiracetam, brivaracetam).
If the patient has noncompliance with a medical regimen and has returned to normal mental status, medications may be resumed. Testing for medication levels may be appropriate if available for the particular medication.
Table 1. Seizure medications
| Generic | Brand Name (United States) |
|---|---|
| Carbamazepine | Carbatrol, Tegretol |
| Clobazam | Frisium, Onfi |
| Clonazepam | Klonopin |
| Diazepam | Diastat, Diazepam, Valium |
| Divalproex Sodium | Depakote, Depakote ER |
| Eslicarbazepine Acetate | Aptiom |
| Ezogabine | Potiga |
| Felbamate | Felbatol |
| Gabapentin | Neurontin |
| Lacosimide | Vimpat |
| Lamotrigine | Lamictal |
| Levetiracetam | Keppra, Keppra XR |
| Lorazepam | Ativan |
| Oxcarbazepine | Oxtellar, Oxtellar XR, Trileptal |
| Perampanel | Fycompa |
| Phenobarbital | |
| Phenytoin | Dilantin, Phenytek, |
| Pregabalin | Lyrica |
| Primidone | Mysoline |
| Rufinamide | Banzel |
| Tiagabine Hydrochloride | Gabitril |
| Topiramate | Topamax, Topamax XR |
| Valproic Acid | Depakene |
| Vigabatrin | Sabril |
In June 2018 the U.S. Food and Drug Administration approved cannabidiol (Epidolex, derived from marijuana) for the treatment of seizures associated with Lennox-Gastaut syndrome and Dravet syndrome for children age 2 and older. The drug contains only small amount of the psychoactive element in marijuana and does not induce euphoria associated with the drug.
For many people with epilepsy, seizures can be controlled with monotherapy at the optimal dosage. Combining medications may amplify side effects such as fatigue and dizziness, so doctors usually prescribe just one drug whenever possible. Combinations of drugs, however, are still sometimes necessary for some forms of epilepsy that do not respond to monotherapy.
When starting any new antiseizure medication, a low dosage will usually be prescribed initially followed by incrementally higher dosages, sometimes with blood-level monitoring, to determine when the optimal dosage has been reached. It may take time for the dosage to achieve optimal seizure control while minimizing side effects. The latter are usually worse when first starting a new medicine.
Most side effects of antiseizure drugs are relatively minor, such as fatigue, dizziness, or weight gain. Antiseizure medications have differing effects on mood: some may worsen depression, where others may improve depression or stabilize mood. However, severe and life-threatening reactions such as allergic reactions or damage to the liver or bone marrow can occur. Antiseizure medications can interact with many other drugs in potentially harmful ways. Some antiseizure drugs can cause the liver to speed the metabolism of other drugs and make the other drugs less effective, as may be the case with oral contraceptives. Since people can become more sensitive to medications as they age, blood levels of medication may need to be checked occasionally to see if dosage adjustments are necessary. The effectiveness of a medication can diminish over time, which can increase the risk of seizures. Some citrus fruit and products, in particular grapefruit juice, may interfere with the breakdown of many drugs, including antiseizure medications – causing them to build up in the body, which can worsen side effects.
Some people with epilepsy may be advised to discontinue their antiseizure drugs after 2-3 years have passed without a seizure. Others may be advised to wait for 4 to 5 years. Discontinuing medication should always be done with supervision of a health care professional. It is very important to continue taking antiseizure medication for as long as it is prescribed. Discontinuing medication too early is one of the major reasons people who have been seizure-free start having new seizures and can lead to status epilepticus. Some evidence also suggests that uncontrolled seizures may trigger changes in the brain that will make it more difficult to treat the seizures in the future.
The chance that a person will eventually be able to discontinue medication varies depending on the person’s age and his or her type of epilepsy. More than half of children who go into remission with medication can eventually stop their medication without having new seizures. One study showed that 68 percent of adults who had been seizure-free for 2 years before stopping medication were able to do so without having more seizures and 75 percent could successfully discontinue medication if they had been seizure-free for 3 years. However, the odds of successfully stopping medication are not as good for people with a family history of epilepsy, those who need multiple medications, those with focal seizures, and those who continue to have abnormal EEG results while on medication.
There are specific syndromes in which certain antiseizure medications should not be used because they may make the seizures worse. For example, carbamazepine can worsen epilepsy in children diagnosed with Dravet syndrome.
Contraception and anti-seizure medications
Some anti-seizure medications can alter the effectiveness of birth control (oral contraceptive) medication. If contraception is a high priority, check with your doctor to evaluate whether your medication interacts with your oral contraceptive, and if other forms of contraception need to be considered.
Ketogenic diet
Dietary approaches and other treatments may be more appropriate depending on the age of the individual and the type of epilepsy. A high-fat, very low carbohydrate ketogenic diet is often used to treat medication-resistant epilepsies. The diet induces a state known as ketosis, which means that the body shifts to breaking down fats instead of carbohydrates to survive. A ketogenic diet effectively reduces seizures for some people, especially children with certain forms of epilepsy. Studies have shown that more than 50 percent of people who try the ketogenic diet have a greater than 50 percent improvement in seizure control and 10 percent experience seizure freedom. Some children are able to discontinue the ketogenic diet after several years and remain seizure-free, but this is done with strict supervision and monitoring by a physician.
The ketogenic diet is not easy to maintain, as it requires strict adherence to a limited range of foods. Possible side effects include impaired growth due to nutritional deficiency and a buildup of uric acid in the blood, which can lead to kidney stones.
Researchers are looking at modified versions of and alternatives to the ketogenic diet. For example, studies show promising results for a modified Atkins diet and for a low-glycemic-index treatment, both of which are less restrictive and easier to follow than the ketogenic diet, but well-controlled randomized controlled trials have yet to assess these approaches.
Surgery
Evaluation of persons for surgery is generally recommended only after focal seizures persist despite the person having tried at least two appropriately chosen and well-tolerated medications, or if there is an identifiable brain lesion (a dysfunctional part of the brain) believed to cause the seizures. When someone is considered to be a good candidate for surgery experts generally agree that it should be performed as early as possible.
Surgical evaluation takes into account the seizure type, the brain region involved, and the importance of the area of the brain where seizures originate (called the focus) for everyday behavior. Prior to surgery, individuals with epilepsy are monitored intensively in order to pinpoint the exact location in the brain where seizures begin. Implanted electrodes may be used to record activity from the surface of the brain, which yields more detailed information than an external scalp EEG. Surgeons usually avoid operating in areas of the brain that are necessary for speech, movement, sensation, memory and thinking, or other important abilities. fMRI can be used to locate such “eloquent” brain areas involved in an individual.
While surgery can significantly reduce or even halt seizures for many people, any kind of surgery involves some level of risk. Surgery for epilepsy does not always successfully reduce seizures and it can result in cognitive or personality changes as well as physical disability, even in people who are excellent candidates for it. Nonetheless, when medications fail, several studies have shown that surgery is much more likely to make someone seizure-free compared to attempts to use other medications. Anyone thinking about surgery for epilepsy should be assessed at an epilepsy center experienced in surgical techniques and should discuss with the epilepsy specialists the balance between the risks of surgery and desire to become seizure-free.
Even when surgery completely ends a person’s seizures, it is important to continue taking antiseizure medication for some time. Doctors generally recommend continuing medication for at least two years after a successful operation to avoid recurrence of seizures.
Surgical procedures for treating epilepsy disorders include:
- Surgery to remove a seizure focus involves removing the defined area of the brain where seizures originate. It is the most common type of surgery for epilepsy, which doctors may refer to as a lobectomy or lesionectomy, and is appropriate only for focal seizures that originate in just one area of the brain. In general, people have a better chance of becoming seizure-free after surgery if they have a small, well-defined seizure focus. The most common type of lobectomy is a temporal lobe resection, which is performed for people with medial temporal lobe epilepsy. In such individuals one hippocampus (there are two, one on each side of the brain) is seen to be shrunken and scarred on an MRI scan.
- Multiple subpial transection may be performed when seizures originate in part of the brain that cannot be removed. It involves making a series of cuts that are designed to prevent seizures from spreading into other parts of the brain while leaving the person’s normal abilities intact.
- Corpus callosotomy or severing the network of neural connections between the right and left halves (hemispheres) of the brain, is done primarily in children with severe seizures that start in one half of the brain and spread to the other side. Corpus callosotomy can end drop attacks and other generalized seizures. However, the procedure does not stop seizures in the side of the brain where they originate, and these focal seizures may even worsen after surgery.
- Hemispherectomy and hemispherotomy involve removing half of the brain’s cortex, or outer layer. These procedures are used predominantly in children who have seizures that do not respond to medication because of damage that involves only half the brain, as occurs with conditions such as Rasmussen’s encephalitis. While this type of surgery is very excessive and is performed only when other therapies have failed, with intense rehabilitation, children can recover many abilities.
Devices
Electrical stimulation of the brain remains a therapeutic strategy of interest for people with medication-resistant forms of epilepsy who are not candidates for surgery.
The vagus nerve stimulation device for the treatment of epilepsy was approved by the U.S. Food and Drug Administration (FDA) in 1997. The vagus nerve stimulator is surgically implanted under the skin of the chest and is attached to the vagus nerve in the lower neck. The device delivers short bursts of electrical energy to the brain via the vagus nerve. On average, this stimulation reduces seizures by about 20 – 40 percent. Individuals usually cannot stop taking epilepsy medication because of the stimulator, but they often experience fewer seizures and they may be able to reduce the dosage of their medication.
Responsive stimulation involves the use of an implanted device that analyzes brain activity patterns to detect a forthcoming seizure. Once detected, the device administers an intervention, such as electrical stimulation or a fast-acting drug to prevent the seizure from occurring. These devices also are known as closed-loop systems. NeuroPace, one of the first responsive stimulation, closed-loop devices, received premarket approval by the FDA in late 2013 and is available for adults with refractory epilepsy (hard to treat epilepsy that does not respond well to trials of at least two medicines).
Experimental devices: not approved by the FDA for use in the United States (as of March 2015)
- Deep brain stimulation using mild electrical impulses has been tried as a treatment for epilepsy in several different brain regions. It involves surgically implanting an electrode connected to an implanted pulse generator – similar to a heart pacemaker – to deliver electrical stimulation to specific areas in the brain to regulate electrical signals in neural circuits. Stimulation of an area called the anterior thalamic nucleus has been particularly helpful in providing at least partial relief from seizures in people who had medication-resistant forms of the disorder.
- A report on trigeminal nerve stimulation (using electrical signals to stimulate parts of the trigeminal nerve and affected brain regions) showed efficacy rates similar to those for vagal nerve stimulation, with responder rates hovering around 50 percent. (A responder is defined as someone having greater than a 50 percent reduction in seizure frequency.) Freedom from seizures, although reported, remains rare for both methods. At the time of this writing, a trigeminal nerve stimulation device was available for use in Europe, but it had not yet been approved in the United States.
- Transcutaneous magnetic stimulation involves a device being placed outside the head to produce a magnetic field to induce an electrical current in nearby areas of the brain. It has been shown to reduce cortical activity associated with specific epilepsy syndromes.
Pregnancy and seizures
Women who’ve had previous seizures typically are able to have healthy pregnancies. Birth defects related to certain medications can sometimes occur.
In particular, valproic acid — one possible medication for generalized seizures — has been associated with cognitive deficits and neural tube defects, such as spina bifida. The American Academy of Neurology recommends that women avoid using valproic acid during pregnancy because of risks to the baby. Discuss these risks with your doctor. Because of the risk of birth defects and because pregnancy can alter medication levels, preconception planning is particularly important for women who’ve had seizures.
In some cases, it may be appropriate to change the dose of seizure medication before or during pregnancy. Medications may be switched in rare cases.
Lifestyle and home remedies
Here are some steps you can take to help with seizure control:
- Take medication correctly. Don’t adjust the dosage before talking to your doctor. If you feel your medication should be changed, discuss it with your doctor.
- Get enough sleep. Lack of sleep can trigger seizures. Be sure to get adequate rest every night.
- Wear a medical alert bracelet. This will help emergency personnel know how to treat you correctly if you have another seizure.
- Be active. Exercising and being active may help keep you physically healthy and reduce depression. Make sure to drink enough water and rest if you get tired during exercise.
- Make healthy life choices. Managing stress, limiting alcoholic beverages and avoiding cigarettes all factor in to a healthy lifestyle.
Personal safety
Seizures don’t usually result in serious injury, but if you have recurrent seizures, injury is a possibility. These steps can help you avoid injury during a seizure:
- Take care near water. Don’t swim alone or relax in a boat without someone nearby.
- Wear a helmet for protection during activities such as bike riding or sports participation.
- Take showers instead of baths, unless someone is near you.
- Modify your furnishings. Pad sharp corners, buy furniture with rounded edges and choose chairs that have arms to keep you from falling off the chair.
- Consider carpet with thick padding to protect you if you do fall.
- Display seizure first-aid tips in a place where people can easily see them. Include any important phone numbers there, too.
Coping and support
If you’re living with a seizure disorder, you may feel anxious or stressed about what your future holds. Stress can affect your mental health, so it’s important to talk with your health care professional about your feelings and seek ways you can find help.
At home
Your family can provide much-needed support. Tell them what you know about your seizure disorder. Let them know they can ask you questions, and be open to conversations about their worries. Help them understand your condition by sharing any educational materials or other resources that your health care professional has given you.
At work
Meet with your supervisor and talk about your seizure disorder and how it affects you. Discuss what you need from your supervisor or co-workers if a seizure happens while at work. Consider talking with your co-workers about seizure disorders — you can widen your support system and bring about acceptance and understanding.
You’re not alone
Remember, you don’t have to go it alone. Reach out to family and friends. Ask your health care professional about local support groups or join an online support community. Don’t be afraid to ask for help. Having a strong support system is important to living with any medical condition.
References- Salpekar J. Seizures, Nonepileptic Events, Trauma, Anxiety, or All of the Above. Epilepsy Curr. 2019 Jan;19(1):29-30.
- Vasudevan C, Levene M. Epidemiology and aetiology of neonatal seizures. Semin Fetal Neonatal Med. 2013 Aug;18(4):185-91
- The Epilepsies and Seizures: Hope Through Research. https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Hope-Through-Research/Epilepsies-and-Seizures-Hope-Through





{kind=link}