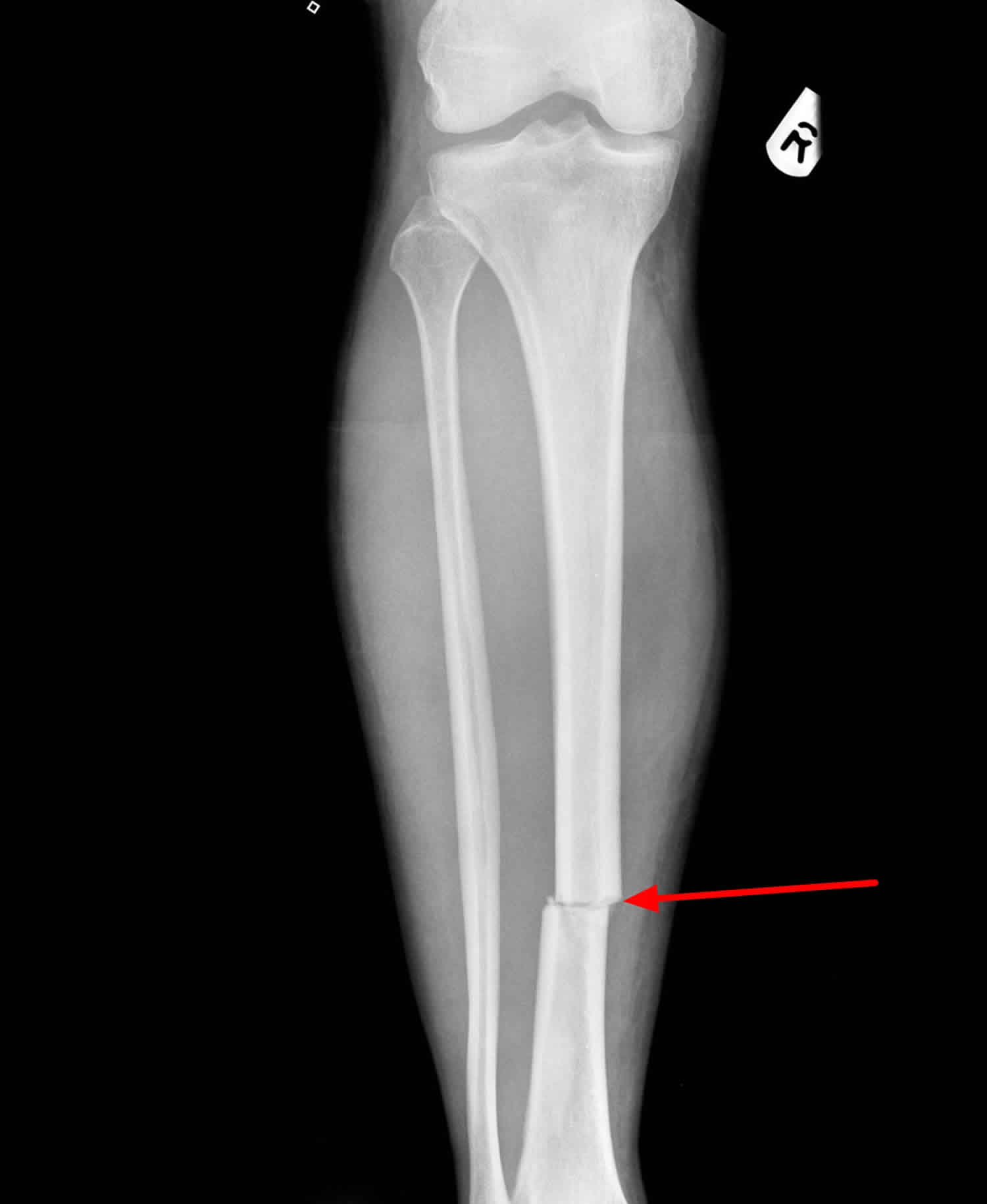
What is a transverse fracture
Transverse fracture is a complete fracture that traverse the bone perpendicular to the axis of the bone. Transverse fracture involves the cortex circumferentially and there may be displacement. The term is predominantly used in the context of fractures of long bones although other types of bones may have transverse fractures, e.g. transverse fracture of the temporal bone.
Transverse fractures of long bones are at risk of displacement, like any other long bone fracture.
Transverse fracture causes
Transverse fracture in young people are frequently due to some type of high-energy collision. The most common cause of femoral shaft fracture is a motor vehicle or motorcycle crash. Being hit by a car while walking is another common cause, as are falls from heights and gunshot wounds. A lower-force incident, such as a fall from standing, may cause a femoral shaft fracture in an older person who has weaker bones.
Transverse fractures are usually associated with blows to the frontal bone or occipital bone. These fractures normally cross the fallopian canal (of the facial nerve) and otic capsule.
Transverse fracture complications
Femoral shaft fractures can cause further injury and complications
- The ends of broken bones are often sharp and can cut or tear surrounding blood vessels or nerves, though this is very rare.
- Acute compartment syndrome may develop. This is a painful condition that occurs when pressure within the muscles builds to dangerous levels. This pressure can decrease blood flow, which prevents nourishment and oxygen from reaching nerve and muscle cells. Unless the pressure is relieved quickly, permanent disability may result. This is a surgical emergency. During the procedure, your surgeon makes incisions in your skin and the muscle coverings to relieve the pressure.
- Open fractures expose the bone to the outside environment. Even with good surgical cleaning of the bone and muscle, the bone can become infected. Bone infection is difficult to treat and often requires multiple surgeries and long-term antibiotics.
- Occasionally, the ligaments around the knee can be injured during a femoral shaft fracture. If you have knee pain after surgery, tell your doctor.
Transverse fracture of the temporal bone complications
- >30% have facial nerve palsies (disruption of fallopian canal containing the facial nerve)
- sensorineural hearing loss (disruption of vestibulocochlear nerve)
- vertigo
- internal carotid artery injury
- jugular vein injury
- fracture through the tegmen tympani results in CSF otorrhea
Transverse fracture treatment
Nonsurgical treatment
Most femoral shaft fractures require surgery to heal. It is unusual for femoral shaft fractures to be treated without surgery. Very young children are sometimes treated with a cast.
Surgical treatment
Timing of surgery. Most femur fractures are fixed within 24 to 48 hours. On occasion, fixation will be delayed until other life-threatening injuries or unstable medical conditions are stabilized. To reduce the risk of infection, open fractures are treated with antibiotics as soon as you arrive at the hospital. The open wound, tissues, and bone will be cleaned during surgery.
For the time between initial emergency care and your surgery, your doctor may place your leg either in a long-leg splint or in traction. This is to keep your broken bones as aligned as possible and to maintain the length of your leg.
Skeletal traction is a pulley system of weights and counterweights that holds the broken pieces of bone together. It keeps your leg straight and often helps to relieve pain.
External fixation
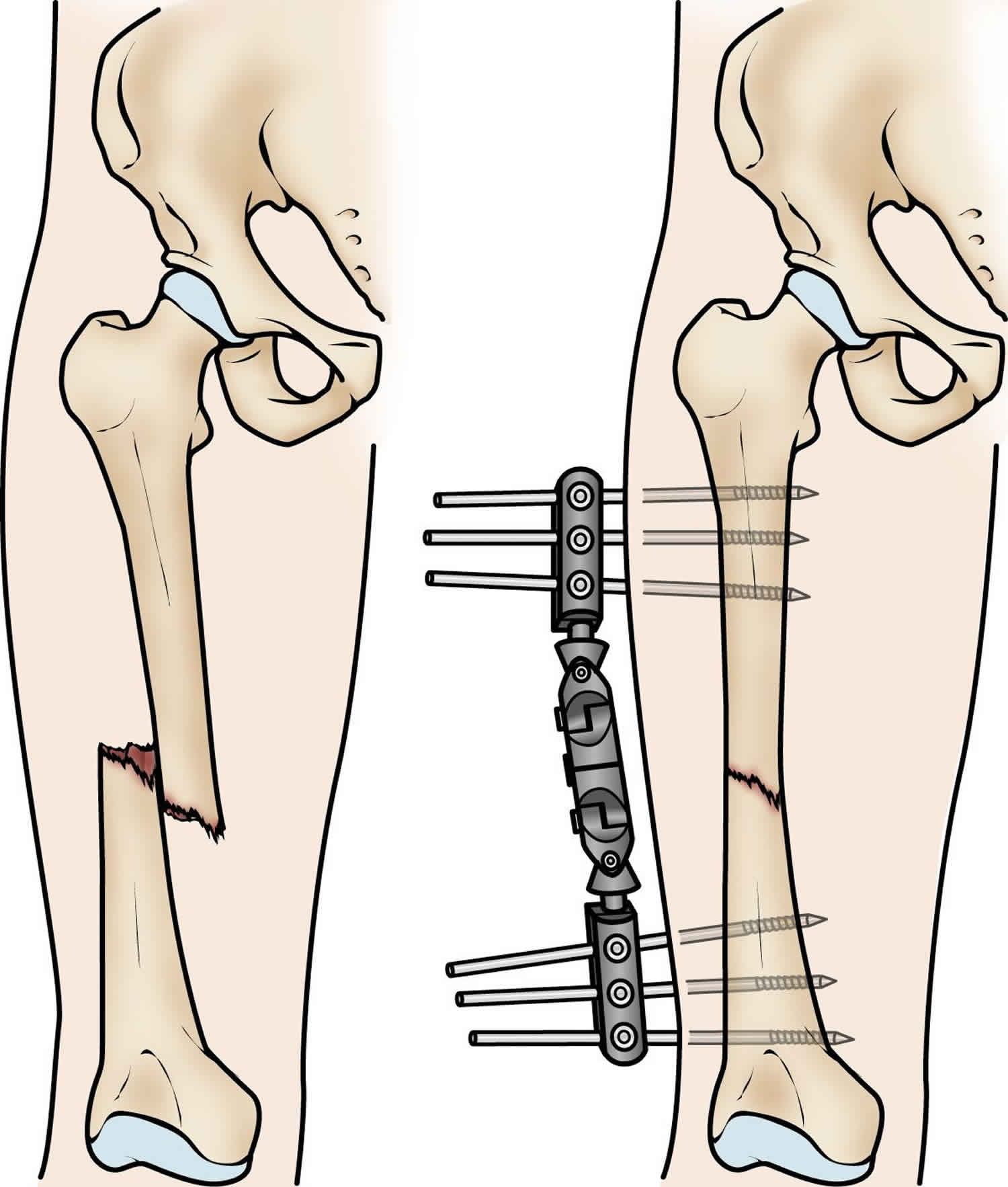
In this type of operation, metal pins or screws are placed into the bone above and below the fracture site. The pins and screws are attached to a bar outside the skin. This device is a stabilizing frame that holds the bones in the proper position. External fixation is usually a temporary treatment for femur fractures. Because they are easily applied, external fixators are often put on when a patient has multiple injuries and is not yet ready for a longer surgery to fix the fracture. An external fixator provides good, temporary stability until the patient is healthy enough for the final surgery. In some cases, an external fixator is left on until the femur is fully healed, but this is not common.
Figure 1. External fixation for transverse fracture of femur (external fixation is often used to hold the bones together temporarily when the skin and muscles have been injured.)
Intramedullary nailing
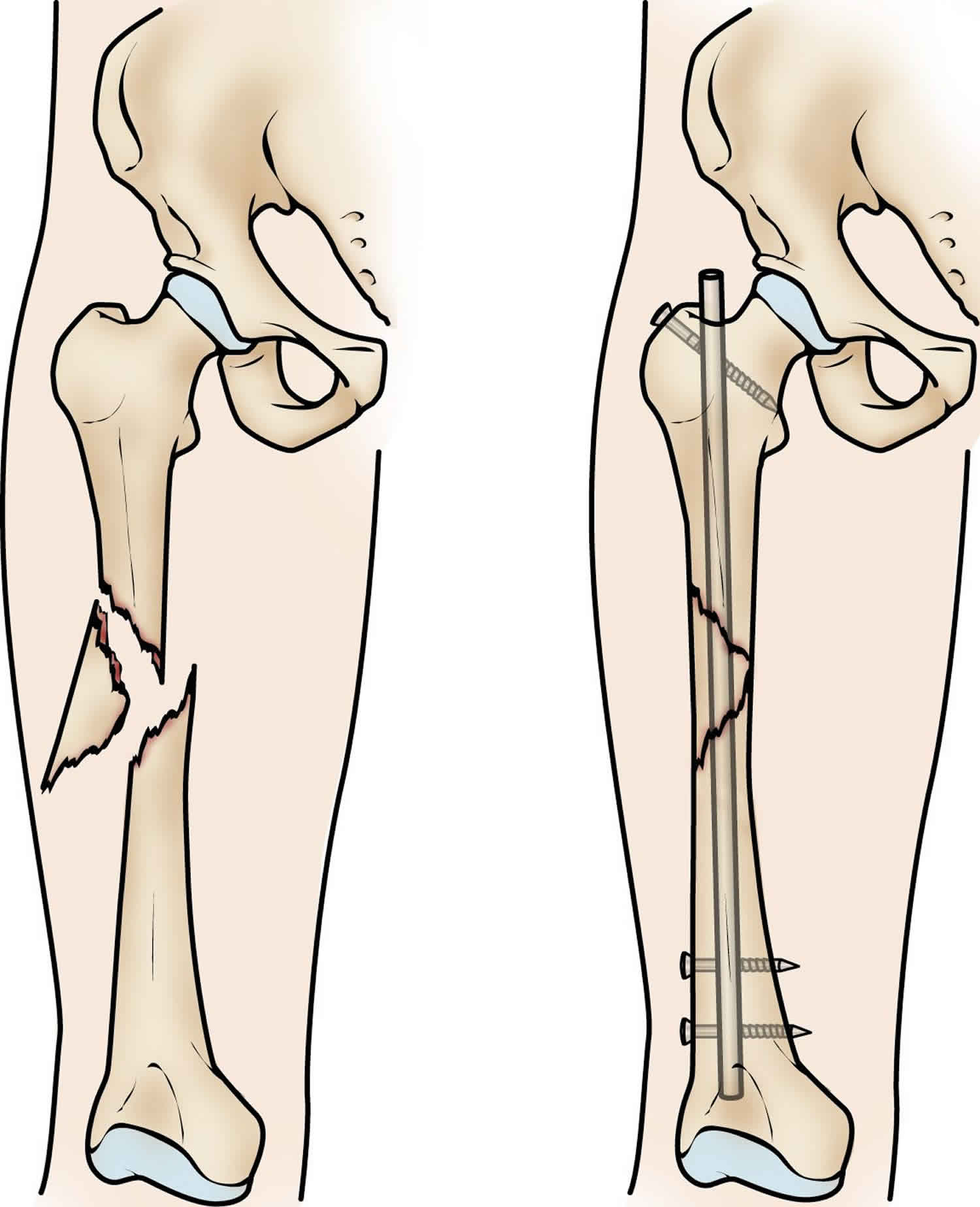
Currently, the method most surgeons use for treating femoral shaft fractures is intramedullary nailing. During this procedure, a specially designed metal rod is inserted into the canal of the femur. The rod passes across the fracture to keep it in position.
An intramedullary nail can be inserted into the canal either at the hip or the knee. Screws are placed above and below the fracture to hold the leg in correct alignment while the bone heals.
Intramedullary nails are usually made of titanium. They come in various lengths and diameters to fit most femur bones.
Figure 2. Intramedullary nailing for transverse fracture of femur (intramedullary nailing provides strong, stable, full-length fixation)
Plates and screws
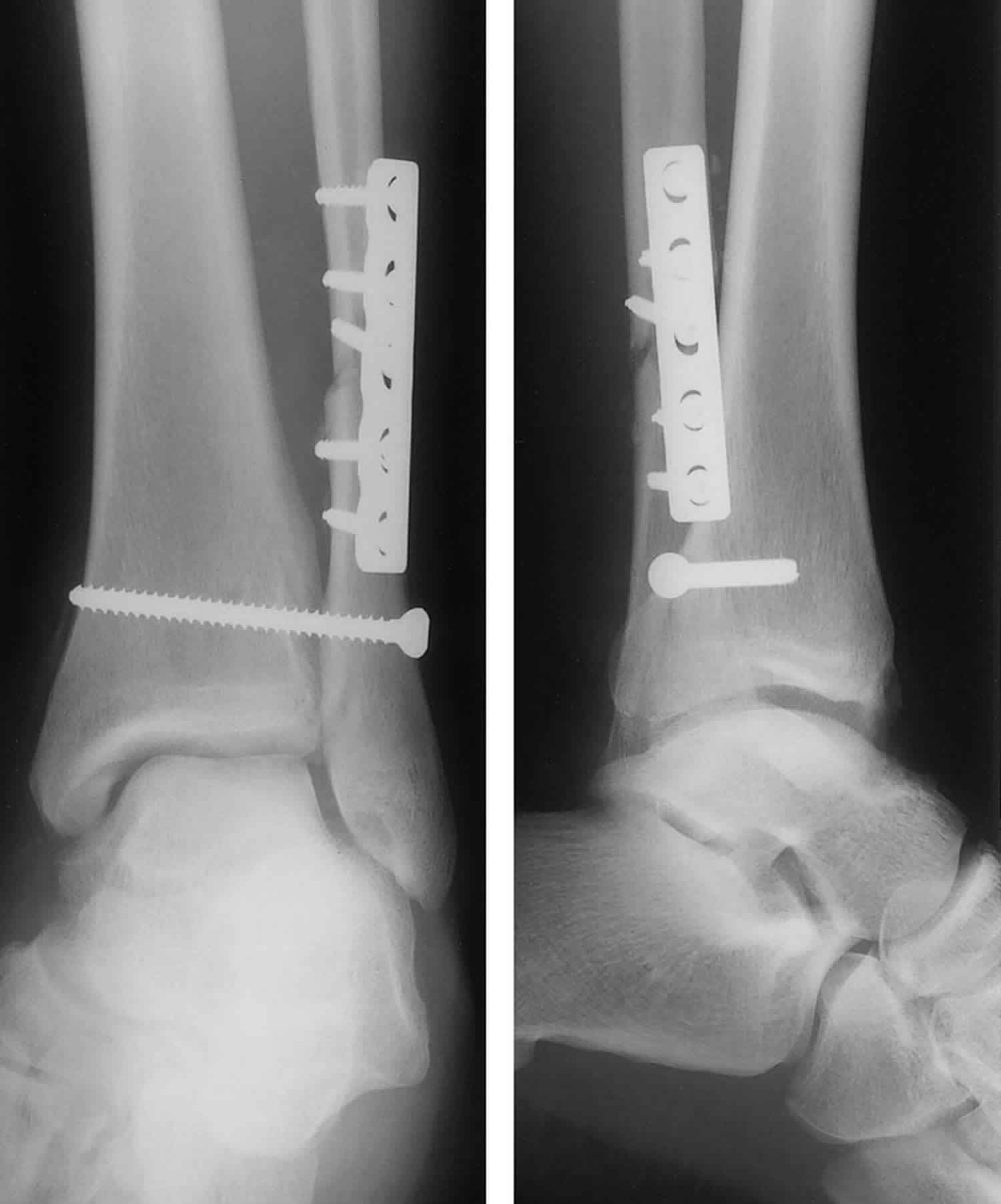
During this operation, the bone fragments are first repositioned (reduced) into their normal alignment. They are held together with screws and metal plates attached to the outer surface of the bone.
Plates and screws are often used when intramedullary nailing may not be possible, such as for fractures that extend into either the hip or knee joints.
Figure 3. Plates and screws for transverse fracture
Complications from surgery
In addition to the risks of surgery in general, such as blood loss or problems related to anesthesia, complications of surgery may include:
- Infection
- Injury to nerves and blood vessels
- Blood clots
- Fat embolism (bone marrow enters the blood stream and can travel to the lungs; this can also happen from the fracture itself without surgery)
- Malalignment or the inability to correctly position the broken bone fragments
- Delayed union or nonunion (when the fracture heals slower than usual or not at all)
- Hardware irritation (sometimes the end of the nail or the screw can irritate the overlying muscles and tendons)
Transverse fracture recovery
Most femoral shaft fractures take 3 to 6 months to completely heal. Some take even longer, especially if the fracture was open or broken into several pieces or if the patient uses tobacco products.
Pain Management
Pain after an injury or surgery is a natural part of the healing process. Your doctor and nurses will work to reduce your pain, which can help you recover faster.
Medications are often prescribed for short-term pain relief after surgery or an injury. Many types of medications are available to help manage pain. These include acetaminophen, nonsteroidal anti-inflammatory drugs (NSAIDs), gabapentinoids, muscle relaxants, opioids, and topical pain medications. Your doctor may use a combination of these medications to improve pain relief, as well as minimize the need for opioids. Some pain medications may have side effects that can impact your ability to drive and do other activities. Your doctor will talk to you about the side effects of your pain medications.
Be aware that although opioids help relieve pain after surgery or an injury, they are a narcotic and can be addictive. Opioid dependency and overdose has become a critical public health issue in the U.S. It is important to use opioids only as directed by your doctor. As soon as your pain begins to improve, stop taking opioids. Talk to your doctor if your pain has not begun to improve within a few days of your treatment.
Weightbearing
Many doctors encourage leg motion early on in the recovery period. It is very important to follow your doctor’s instructions for putting weight on your injured leg to avoid problems.
In some cases, doctors will allow patients to put as much weight as possible on the leg right after surgery. However, you may not be able to put full weight on your leg until the fracture has started to heal. Be sure to follow your doctor’s instructions carefully.
When you begin walking, you will probably need to use crutches or a walker for support.
Physical Therapy
Because you will most likely lose muscle strength in the injured area, exercises during the healing process are important. Physical therapy will help to restore normal muscle strength, joint motion, and flexibility. It can also help you manage your pain after surgery.
A physical therapist will most likely begin teaching you specific exercises while you are still in the hospital. The therapist will also help you learn how to use crutches or a walker.
Transverse process fracture
Transverse process fracture is a rare injury in sport, most often associated with either direct trauma or violent muscular contraction 1. Transverse process fracture in the general population has been reported relatively widely in the literature 2. Conversely, coverage of transverse process fracture in the context of sport is sparse, especially with respect to the factors informing the sports physician in practice, namely mechanism of injury, treatment and recovery times. Currently, there is a paucity of research in sport-related transverse process fracture with the existing literature taking the form of epidemiological studies or case reports.
Transverse process fracture in the general population is more commonly complicated with visceral injury with or without nerve root injury 1. While transverse process fracture can occur in the athlete, it is probably associated with a lower energy mechanism of injury, rarely complicated and commonly associated with a relatively swift recovery 3.
Figure 4. Transverse process fracture

Footnote: X-ray lumbar spine antero-posterior view showing the fractures of the left L2 and L3 transverse processes (arrows)
Transverse process fracture causes
Transverse process fracture has traditionally been associated with high-energy direct trauma or violent muscular contraction, often from direct blunt trauma as in motor vehicle accidents, a fall from height 4, violent lateral flexion-extension forces (as in sports particularly football), avulsion of the psoas muscle or Malgaigne fractures of the pelvis 5. Fractures of the transverse processes of the lumbar vertebrae usually occur as the result of major forces and a statistically significant association between transverse process fractures and abdominal injury has been reported 6. Although transverse fracture of the lumbar vertebra can be a marker of associated visceral injuries including trauma to the abdominal viscera, retroperitoneum, spine, long bones and cranium 7, the fractures of the transverse processes of the lumbar spine can occur in the absence of other vertebral and visceral damage 8.
Transverse process fracture diagnosis
In literature, in patients with isolated transverse fractures, the detailed investigations are recommended to exclude the possible associated visceral injuries. Classically, the conventional lumbar radiographs are used for evaluation of patients who are at risk of injury from blunt trauma; however, it is relatively insensitive in detecting the fractures as well as associated visceral injuries 9. This insensitivity of conventional radiographs, especially in the setting of acute trauma can be due to the presence of overlying bowel gas, hence the full assessment and extent of fractures and associated injuries is not possible 6. With the widespread use of whole-body CT scanning in trauma patients, the isolated transverse process fractures has been increasingly recognized and apart form this, the CT scan can detect the associated injuries in detail 10. The detailed radiological investigations should be performed wherever facilities and resources permit. In a large retrospective review at Level I trauma center, it was found that where no other vertebral fracture is seen on an adequate screening CT scan, investigation may reasonably end. Also further imaging and consultations can lead to prolonged log-roll precautions, which delay the mobilization and can be potentially deleterious to overall patient care 11. This can be followed in a setting with limited resources (either the resources are not available, e.g. CT scan or inability to perform recommended investigation in all the cases, e.g. financial constraints and poor affordability) and clinically stable patients can be carefully observed over an extended period.
Transverse process fracture treatment
Lumbar transverse process fractures, not associated with neurological deficits or structural instability, can be managed conservatively without neurosurgical or orthopedic intervention 10. Dutson 12 outlined a case of transverse process fracture of L1 in a trainee association footballer, associated with direct blunt trauma to the players back from a goalkeeper’s knee. The fracture was complicated by traumatic transverse colon rupture requiring a stay in intensive care and colostomy. This was reversed 12 weeks post-trauma. Return to play data were not specified.
Brynin and Gardiner 13 detailed a single case of lumbar transverse process fracture at L2 and L3, confirmed on CT. The injury was precipitated by a ‘spear’ in the back during an American football game. The player was precluded from contact sport with a return to play of 4 weeks without an adverse event.
Bali et al. 14 reported a case of multiple displaced lumbar transverse process fracture (L1–5) in a cricket bowler. The player presented with chronic lower back pain with no obvious precipitant. The authors hypothesized that the fractures occurred after repeated small stresses on the spine associated with fast-bowling.
Gertzbein et al. 15 conducted a retrospective epidemiological study of thoracic and lumbar fractures in skiers and snowboarders over a 5-year period and found 43 instances of isolated transverse process fracture accounting for 29% of all fractures reported. The authors postulated that these occurred secondary to avulsion forces from intense muscle spasm on impact from a fall. Recovery time data were not provided.
Finally, Tewes et al. 3 reviewed 29 cases of lumbar transverse process fracture in the American NFL (national football league) and found an average return to play time of 3.5 weeks. Rest was the most common management approach. Average return to play was further broken down based on the total number of fractures and was 16 days with 1 transverse process fracture, 19 days with 2 transverse process fractures and 36 days with 3 transverse process fractures. However, this trend was not statistically significant. Upon return to play, most players wore flak jackets/padded wrap. The single re-injury reported occurred in a player wearing a flak jacket. The cause of injury was identified as ‘impact’ in 93% and ‘torsion’ in 7% of players. In terms of complications, five players suffered back spasms. Additionally, one player sustained a visceral injury in the form of a kidney contusion.
References- Gray M, Catterson P. Multilevel lumbar transverse process fractures in a professional association football player: a case report. Oxf Med Case Reports. 2015;2015(5):288–291. Published 2015 May 15. doi:10.1093/omcr/omv037 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4434575
- Chang CH, Holmes JF, Mower WR, Panacek EA. Distracting injuries in patients with vertebral injuries. J Emerg Med 2005;28:147–52
- Tewes DP, Fischer DA, Quick DC, Zamberletti F, Powell J. Lumbar transverse process fractures in professional football players. Am J Sports Med 1995;23:507–9
- Agrawal A, Srivastava S, Kakani A. Isolated transverse process fracture of the lumbar vertebrae. J Emerg Trauma Shock. 2009;2(3):217–218. doi:10.4103/0974-2700.55350 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2776377
- Brynin R, Gardiner L. Missed lumbar transverse process fractures in a high school football player. J Manipulative Physiol Ther. 2001;24:123–6.
- Patten RM, Gunberg SR, Brandenburger DK. Frequency and importance of transverse process fractures in the lumbar vertebrae at helical abdominal CT in patients with trauma. Radiology. 2000;215:831–4
- Krueger MA, Green DA, Hoyt D, Garfin SR. Overlooked spine injuries associated with lumbar transverse process fractures. Clin Orthop Relat Res. 1996;327:191–5
- Epstein BS. The spine: A radiological text and atlas. 4th ed. Philadelphia: Lea and Febiger; 1976. p. 572
- Gestring ML, Gracias VH, Feliciano MA, Reilly PM, Shapiro MB, Johnson JW, et al. Evaluation of the lower spine after blunt trauma using abdominal computed tomographic scanning supplemented with lateral scanograms. J Trauma. 2002;53:9–14
- Bradley LH, Paullus WC, Howe J, Litofsky NS. Isolated transverse process fractures: spine service management not needed. J Trauma. 2008;65:832–6
- Homnick A, Lavery R, Nicastro O, Livingston DH, Hauser CJ. Isolated thoracolumbar transverse process fractures: Call physical therapy, not spine. J Trauma. 2007;63:1292–5
- Dutson SCM. Transverse colon rupture in a young footballer. Br J Sports Med 2006;40:e6.
- Brynin R, Gardiner L. Missed lumbar transverse process fractures in a high school football player. J Manipulative Physiol Ther 2001;24:123–6
- Bali K, Kumar V, Krishnan V, Meena D, Rawall S. Multiple lumbar transverse process stress fractures as a cause of chronic low back ache in a young fast bowler—a case report. SMARTT 2011;3:8
- Gertzbein SD, Khoury D, Bullington A, St John TA, Larson AI. Thoracic and lumbar fractures associated with skiing and snowboarding injuries according to the AO Comprehensive Classification. Am J Sports Med 2012;40:1750–4





{kind=link}