What is Troponin
Troponin is a protein complex found in skeletal and heart (cardiac) muscle fibers that regulate the excitation and muscular contraction. Troponin tests measure the level of cardiac-specific troponin in the blood to help detect heart injury. Troponin levels may remain high for 1 to 2 weeks after a heart attack. Because troponin tests measure cardiac muscle-specific troponin, the troponin test is not affected by damage to skeletal muscles, so injections, accidents, and drugs that can damage muscle do not affect cardiac troponin levels. Very rarely, people who have a heart attack will have normal troponin levels, and some people with increased troponin levels have no apparent heart injury. Other conditions that can contribute to elevated troponin levels include renal failure and pulmonary embolism.
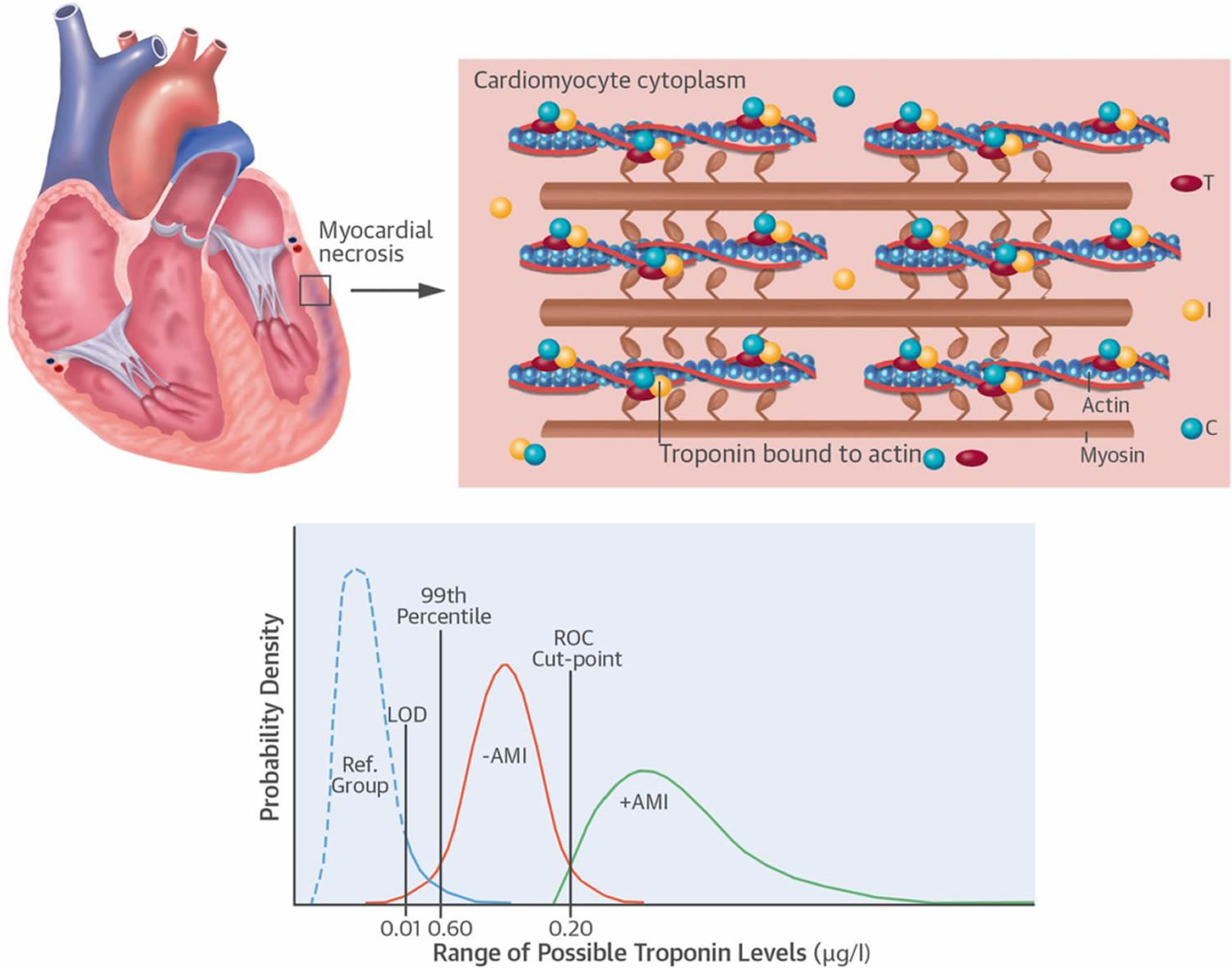
There are three types of troponin proteins each of which has different functions and are encoded by separate genes 1:
- Troponin C: Troponin C initiates contraction by binding calcium and moves troponin I so that the two proteins that pull the muscle fiber shorter can interact. There is little or no difference in troponin C between skeletal and cardiac muscle, but the forms of troponin I and troponin T are different.
- Troponin T: Troponin T anchors the troponin complex to the muscle fiber structure. Troponin T binds the troponin complex to tropomyosin. Troponin T is a myofibrillar protein found in striated musculature. There are 2 types of myofilament: a thick filament containing myosin and a thin filament consisting of 3 different proteins, namely actin, tropomyosin, and troponin. Troponin T is found in free cytosol and structurally bound protein. The unbound pool of troponin T is the source of early protein release in myocardial damage. Troponin T is released from the structural elements at a later stage, corresponding to the degradation of myofibrils that occurs in irreversible myocardial damage. Troponin T becomes elevated 2 to 4 hours after the onset of myocardial necrosis and can remain elevated for up to 14 days, or even longer on occasion.
- Troponin I: Troponin I is an inhibitory protein – troponin T binds the troponin complex to tropomyosin and exhibits in 3 isoforms: cardiac muscle, slow-twitch skeletal muscle, and fast-twitch skeletal muscle. The cardiac form of troponin I has 31 amino acid residues on its N-terminal, not present in the skeletal forms, which allow for specific polyclonal and monoclonal antibody development. The cardiac specificity of this isoform improves the accuracy of diagnosis in patients with acute or chronic skeletal muscle injury and possible concomitant myocardial injury. Troponin I is the only troponin isotope present in the myocardium and is not expressed during any developmental stage in skeletal muscle. Troponin I is released into the bloodstream within hours of the onset of symptoms of myocardial infarction or ischemic damage. It can be detected at 3 to 6 hours following onset of chest pain with peak concentrations at 12 to 16 hours, and remains elevated for 5 to 9 days.
Figure 1. Troponin
Troponin I and troponin T have amino acid sequences specific to cardiac tissue, making these molecules ideal biological markers 3. In the late 1980s, investigators developed immunoassays for troponin I and troponin T 4. Refinements in the antibodies, reagents, and automation have made the current commercial troponin assays exquisitely sensitive and precise 3. The newest, most sensitive assays are able to detect troponin in the bloodstream of patients without myocardial damage, perhaps due to normal myocardial cell turnover or formation of exosomes that release small amounts of free troponin into the bloodstream 5.
Measuring the amount of cardiac-specific troponin T or troponin I in the blood can help identify individuals who have experienced damage to their heart. When a person has a heart attack, levels of cardiac-specific troponins I and T can become elevated in the blood within 3 or 4 hours after injury and may remain elevated for 10 to 14 days.
Normally, troponin is present in very small to undetectable quantities in the blood. When there is damage to heart muscle cells, troponin is released into the blood. The more damage there is, the greater the concentration in the blood. Primarily, troponin tests are used to help determine if an individual has suffered a heart attack. They may also be helpful in evaluating someone for other forms of heart injury.
The 2014 American Heart Association/American College of Cardiology Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes document states that troponin is the preferred biomarker for diagnosing acute myocardial infarction (heart attack) 6. This recommendation acknowledges the fact that laboratory methods for troponin testing have markedly improved over the past 2 decades, resulting in lower limits of detection and improved assay precision 7. The laboratory advances in troponin testing have been extraordinary, but the optimal use of the test also requires good clinical reasoning by practitioners who use troponin testing in clinical practice.
There are 3 critical elements necessary for optimal use of troponin testing in clinical care, as follows: 1) the analytical performance of the assay; 2) the clinical sensitivity and specificity of the test result; and 3) the clinical reasoning for ordering and the proper clinical context for interpreting the test result. All 3 elements are integral to foster optimal clinical utility. Most clinicians rely on their clinical laboratories to address the analytical performance of the assay and are unfamiliar with the laboratory science of troponin testing. The clinical sensitivity and specificity of troponin testing have been a source of confusion for clinicians because definitions have changed as the test has evolved and because there are many different assays available. Additionally, for clinical reasoning, there is generally little attention as to how to integrate these test results with other clinical information. Excellent review papers have explained the operating characteristics and proper use of troponin testing 8, but further explanation may be beneficial.
Many laboratories in the U.S. use high-sensitivity troponin tests since the Food and Drug Administration (FDA) approved them in 2017. Because this version of the test is more sensitive than previous, older versions, it becomes positive sooner and may help detect heart injury and acute coronary syndrome earlier. The high-sensitivity-troponin test may also be positive in people with stable angina and even in people with no symptoms. Angina is chest pain thought to be from a part of your heart not getting enough blood flow. When it is elevated in these individuals, it indicates an increased risk of future heart events such as heart attacks.
What does heart attack mean?
Heart attack (myocardial infarction) means that some of the muscle tissue in your heart is severely injured or has died. The medical term for the death of cardiac muscle is myocardial infarction. Because it is not always possible to determine whether there is only serious injury or there is infarction, the general term for the condition is acute coronary syndrome (ACS).
Most commonly, a heart attack starts with a sensation of heavy pressure or pain in the chest, often extending into the neck or left arm. You may have trouble catching your breath or you may feel weak and break into a cold sweat.
A heart attack usually occurs because one of the blood vessels (called coronary arteries) that brings blood to your heart muscle is blocked. This usually happens when a blood clot forms in a blood vessel that is already partially closed. The partial closure is usually due to atherosclerosis (often called hardening of the arteries). Obstruction occurs gradually over many years as lipid plaques are deposited along the walls of the blood vessels. These plaques narrow and stiffen the arteries and can rupture unexpectedly, totally blocking off the affected artery.
If I have chest pain, does that mean I am having a heart attack?
Many other problems can cause chest pain, and it is not possible to tell from the type of chest pain whether or not you are having a heart attack. Many people have chest pain from straining the muscles in their chest, from heartburn or other problems involving the stomach and esophagus, from emotional stress, and with some lung problems. Chest pain that occurs during exercise, hard work, or at times of stress, lasts for a few minutes, and goes away with rest is often caused by angina. A relatively rare form of chest pain may be due to temporary heart spasms called variant angina. These spasms usually occur at night when a person is resting and can cause severe but temporary pain.
If chest pain lasts longer than just a few minutes, especially if it occurs when you are resting, seek immediate medical attention.
What if I am not sure if I am having a heart attack?
Many people are not sure if they are experiencing a heart attack. If you are unsure, don’t wait, but get help. Getting help right away can help you survive and treatments given soon after a heart attack can help limit the damage to your heart.
Note that not everyone will experience chest pain, and women are more likely than men to have signs and symptoms that are not typical. In women, symptoms are often less dramatic and more likely to be misinterpreted as due to another cause than in men. Some heart attacks are sudden while other heart attacks start slowly. The pain and other symptoms may come and go. Signs and symptoms may include:
- Chest pain, discomfort and/or pressure (most common)
- Rapid heart rate, skipping a beat
- Nausea and vomiting or stomach pain
- Sweating
- Sudden onset of shortness of breath
- Difficulty breathing
- Feeling lightheaded
- Change in blood pressure
- Fatigue
- Pain on other places such as the back, one or both arms, jaw or neck
Troponin test
A troponin test measures the levels of troponin T or troponin I proteins in the blood. These proteins are released when the heart muscle has been damaged, such as occurs with a heart attack. The more damage there is to the heart, the greater the amount of troponin T and I there will be in the blood. Your health care provider will order this test if you have chest pain and other signs of a heart attack. Troponin test is usually repeated two more times over the next 6 to 24 hours.
High-sensitivity troponin tests are primarily ordered to help diagnose a heart attack and rule out other conditions with similar signs and symptoms. Either a troponin I or troponin T test can be performed; usually a laboratory will offer one test or the other. The concentrations are different, but they basically provide the same information.
The most common reason to perform troponin test is to see if a heart attack has occurred. Troponin tests are also sometimes used to evaluate people for heart injury due to causes other than a heart attack or to distinguish signs and symptoms such as chest pain that may be due to other causes. Testing may also be done to evaluate people with angina if their signs and symptoms worsen.
Your doctor may also order troponin test if you have angina that is getting worse, but no other signs of a heart attack. Angina is chest pain thought to be from a part of your heart not getting enough blood flow.
The troponin test may also be done to help detect and evaluate other causes of heart injury.
Troponin tests are sometimes ordered along with other cardiac biomarkers, such as CK–MB (CPK isoenzymes) or myoglobin. However, troponin is the preferred test for a suspected heart attack because it is more specific for heart injury than other tests (which may be elevated in the blood with skeletal muscle injury) and remain elevated for a longer period of time. However, there have been some reports of increased troponin in people with skeletal muscle disease. Also, troponin may rise following strenuous exercise, although in the absence of signs and symptoms of heart disease, it is usually of no medical significance.
When is troponin test ordered?
A troponin test will usually be ordered when a person with a suspected heart attack first comes into the emergency room, followed by a series of troponin tests performed over several hours.
A heart attack may be suspected and testing done when a person has signs and symptoms such as those listed below. Note that not everyone will experience chest pain, and women are more likely than men to have sign and symptoms that are not typical.
- Chest pain, discomfort and/or pressure (most common)
- Rapid heart rate, skipping a beat
- Shortness of breath and/or difficulty breathing
- Fatigue
- Nausea, vomiting
- Cold sweat
- Lightheaded
- Undue fatigue
- Pain in other places: back, arm, jaw, neck, or stomach
In people with stable angina, a troponin test may be ordered when:
- Symptoms worsen
- Symptoms occur when a person is at rest
- Symptoms are no longer eased with treatment
These are all signs that the angina is becoming unstable, which increases the risk of a heart attack or other serious heart problem in the near future.
Normal troponin levels
Cardiac troponin levels are normally so low they cannot be detected with most blood tests.
Having normal troponin levels 12 hours after chest pain has started means a heart attack is unlikely.
A normal value range may vary slightly among different laboratories. Some labs use different measurements (for example, “high sensitivity troponin test”) or test different samples. Also, some labs have different cutoff points for “normal” and “probable myocardial infarction.” Talk to your doctor about the meaning of your specific test results.
Troponin I normal levels: < or =0.04 ng/mL
Reference values have not been established for patients <17 years of age.
Troponin T normal levels
- Males: < or =15 ng/L
- Females: < or =10 ng/L
Values for healthy adults, based upon available literature and clinical guidelines, are 10 ng/L or less for women and 15 ng/L or less for men.
What is considered a high troponin level?
For patients who present with suspected acute coronary syndromes, troponin T values greater than the reference interval with a rising (> or =10 ng/L over 2 hours or > or =12 ng/L over 6 hours) pattern are highly suggestive of acute cardiac injury. Decreasing values are indicative of recent cardiac injury. Serial measurement is highly recommended for the diagnosis or exclusion of acute coronary syndromes.
Troponin T values greater than the reference interval are associated with adverse events in patients with ischemic heart disease and many other clinical situations. Clinical judgment is necessary to distinguish patients who have ischemic heart disease from those who do not.
Elevated troponin causes
A high troponin and even slight increase in the troponin level may indicate some degree of damage to the heart. Very high levels of troponin are a sign that a heart attack has occurred. When a person has significantly elevated troponin levels and, in particular, a rise and/or fall in the results from a series of tests done over several hours, then it is likely that the person has had a heart attack or some other form of damage to the heart. Levels of troponin can become elevated in the blood within 3 to 6 hours after heart injury and may remain elevated for 10 to 14 days.
Most patients who have had a heart attack have increased troponin levels within 6 hours. After 12 hours, almost everyone who has had a heart attack will have raised levels.
Increased troponin levels are not be used by themselves to diagnose or rule out a heart attack. A physical exam, clinical history, and ECG are also important. Your healthcare practitioner may also need to see whether the troponin levels from a series of tests are stably elevated or show a rise and/or fall over several hours.
In people with angina, an elevated troponin may indicate that their condition is worsening and they are at increased risk of a heart attack.
Troponin levels may also be elevated with other heart conditions such as myocarditis (heart inflammation), weakening of the heart (cardiomyopathy), or congestive heart failure, and with conditions unrelated to the heart, such as severe infections and kidney disease.
Normal troponin values in a series of measurements over several hours means that it is unlikely that a person’s heart has been injured. Signs and symptoms may be due to a cause unrelated to the heart.
Increased troponin levels may also be due to:
- Abnormally fast heartbeat
- High blood pressure in lung arteries (pulmonary hypertension)
- Blockage of a lung artery by a blood clot, fat, or tumor cells (pulmonary embolus)
- Congestive heart failure
- Coronary artery spasm
- Inflammation of the heart muscle usually due to a virus (myocarditis)
- Prolonged exercise (for example, due to marathons or triathlons)
- Trauma that injures the heart, such as a car accident
- Weakening of the heart muscle (cardiomyopathy)
- Long-term kidney disease
Increased troponin levels may also result from certain medical procedures such as:
- Cardiac angioplasty/stenting
- Heart defibrillation or electrical cardioversion (purposeful shocking of the heart by medical personnel to correct an abnormal heart rhythm)
- Open heart surgery
- Radiofrequency ablation of the heart
Troponin I is the only troponin isotope present in the myocardium and is not expressed during any developmental stage in skeletal muscle. Troponin I is released into the bloodstream within hours of the onset of symptoms of myocardial infarction or ischemic damage. It can be detected at 3 to 6 hours following onset of chest pain with peak concentrations at 12 to 16 hours, and remains elevated for 5 to 9 days.
The most common cause of cardiac injury is myocardial ischemia, ie, acute myocardial infarction (heart attack). These patients are known to have an adverse short- and long-term prognosis compared to patients with unstable angina and no elevation of troponin T. Many of these patients, especially those with troponin T elevations above 30 ng/L, benefit from an aggressive strategy with anticoagulation and an invasive interventional strategy.
There are, on occasions, elevations of cardiac troponin T can be due to skeletal muscle disease. One way to unmask such elevations is to measure cardiac troponin I, which will be normal in that circumstance. In addition, at times there are interferences that can cause spurious increases or decreases in cardiac troponin T values. Conceptually, these same interferences can occur with cardiac troponin I but in any given case, the likelihood of having both assays be confounded in that way is highly unusual. Thus, potential false-positives would be unmasked by a normal cardiac troponin I and false-negatives by an elevated value.
Cautions
A positive troponin result is not always indicative of myocardial infarction. Other conditions resulting in myocardial cell damage can contribute to elevated cardiac troponin I levels. These conditions include, but are not limited to, myocarditis, cardiac surgery, angina, unstable angina, congestive heart failure, and noncardiac-related causes, such as, renal failure and pulmonary embolism.
As with all markers of cardiac injury, elevations of cardiac troponin T do not in and of themselves indicate the presence of an ischemic mechanism. Many other disease states can be associated with elevations of cardiac troponin T via mechanisms different from those that cause injury in patients with acute coronary syndromes. These include: trauma including contusion, ablation, pacing; congestive heart failure; pulmonary embolism; renal failure; and myocarditis.
References- Jarolim P. 2015 High sensitivity cardiac troponin assays in the clinical laboratories. Clin Chem Lab Med 53:635–652.
- John E. Brush, Sanjay Kaul, Harlan M. Krumholz. Troponin Testing for Clinicians. Journal of the American College of Cardiology Nov 2016, 68 (21) 2365-2375; DOI: 10.1016/j.jacc.2016.08.066 http://www.onlinejacc.org/content/68/21/2365
- Apple F.S., Collinson P.O., for the IFCC Task Force on Clinical Applications of Cardiac Biomarkers. 2012 Analytical characteristics of high-sensitivity cardiac troponin assays. Clin Chem 58:54–61.
- Katus H.A., Remppis A., Neumann F.J., et al. 1991 Diagnostic efficiency of troponin T measurements in acute myocardial infarction. Circulation 83:902–912.
- Jarolim P. 2015 High sensitivity cardiac troponin assays in the clinical laboratories. Clin Chem Lab Med 53:635–652
- Amsterdam E.A., Wenger N.K., Brindis R.G., et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 64:e139–e228.
- Apple F.S., Collinson P.O., for IFCC Task Force on Clinical Applications of Cardiac Biomarkers. 2012 Analytical characteristics of high-sensitivity cardiac troponin assays. Clin Chem 58:54–61
- Newby L.K., Jesse R.L., Babb J.D., et al. ACCF 2012 expert consensus document on practical clinical considerations in the interpretation of troponin elevations: a report of the American College of Cardiology Foundation task force on Clinical Expert Consensus Documents. J Am Coll Cardiol 60:2427–2463





{kind=link}