What is a tubercle
Tubercle is a small rounded projection or process of a bone, for example greater tubercle of humerus, tibial tubercle, conoid tubercle of clavicle and adductor tubercle of the distal femur.
Tubercle also refers to a nodule attached to bone, mucous membrane (moist layer lining parts of the body), or skin.
The term tubercle is less commonly used to refer to skin irritation resulting from a tuberculosis (TB) infection.
Darwin’s tubercle is a blunt point projecting from the upper part of the helix of the ear.
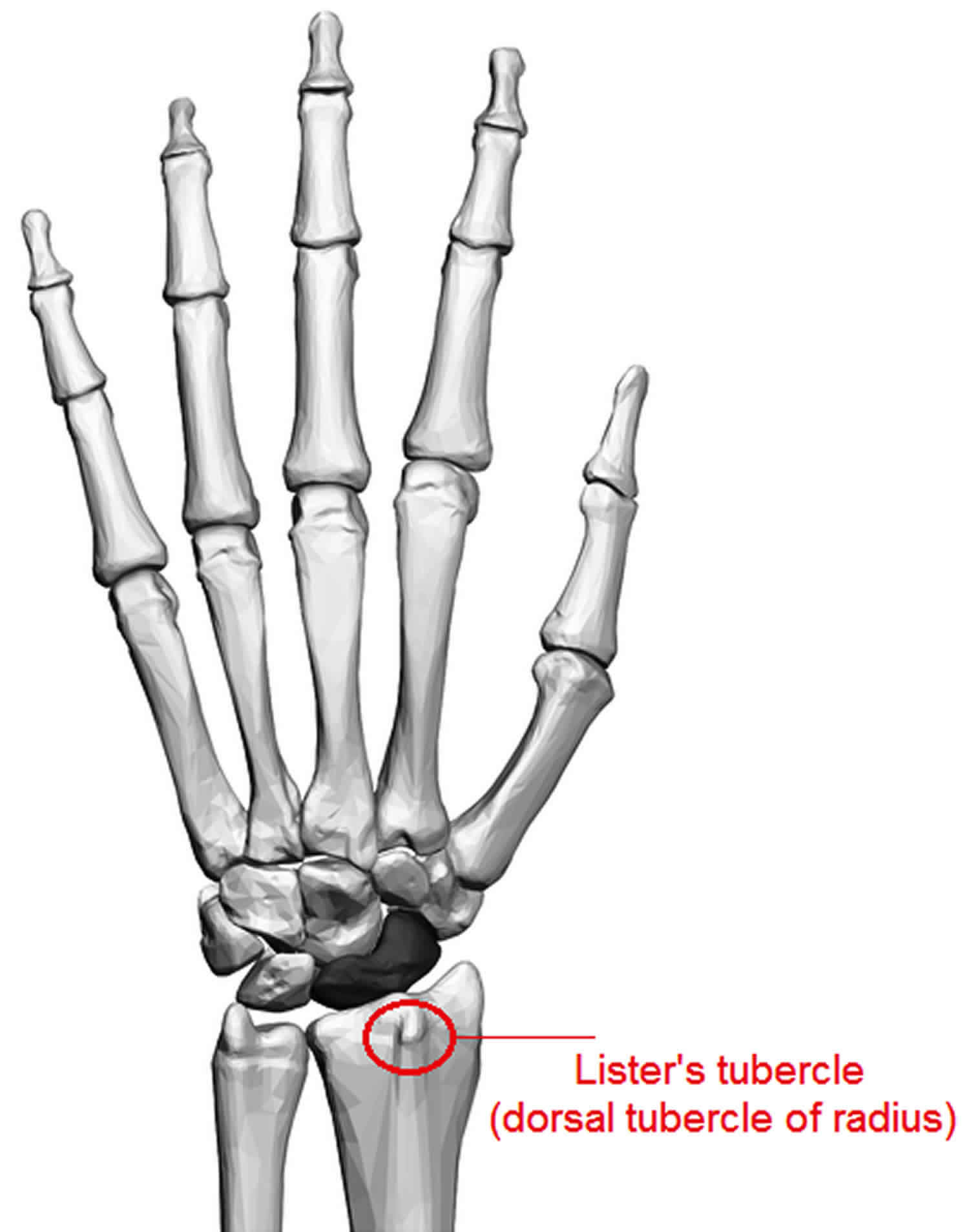
Lister’s tubercle
Lister’s tubercle is an old term for prominent bony tubercle over the dorsal aspect of the distal radius 1, which functions as a pulley for the extensor pollicis longus tendon before the tendon pivots and turns obliquely to insert onto the distal phalanx of the thumb 2. As a palpable structure, Lister’s tubercle has been used as an anatomical landmark for localizing the first dorsal extensor compartment 3, posterior interosseous nerve 4, superficial branch of the radial nerve 5 and dorsal radiotriquetral ligament 6. Lister’s tubercle is also used as a surgical landmark in wrist arthrography injections, wrist arthroscopy and wrist joint injectionsy 7, dorsal wrist capsulotomy 8, hand microsurgery 9, radioscapholunate arthrodesis 10, Kirschner wire placement, and internal fixation of Colles fractures 11.
Besides being an anatomic landmark during surgery, there is also some clinical importance to the anatomical localization of Lister’s tubercle. For instance during volar plate fixation for distal radius fractures, when the screws are applied in unsuitable orientation and length, they may irritate the extensor pollicis longus tendon which lies in the groove medial to the dorsal tubercle. Over a long period this may cause extensor pollicis longus tendon ruptures 6.
Because of its proximity to carpal structures and overlapping bony densities, conventional radiology does not provide a detailed outline of Lister’s tubercle or its relationship to the adjacent tendon structures.
Despite the importance of Lister’s tubercle in modern surgical procedures and its close spatial relationship with the extensor pollicis longus tendon, few reports have described the variations of Lister’s tubercle and its relationship with the extensor pollicis longus tendon. Pichler et al. 12 reported the height variations of Lister’s tubercle on computed tomography (CT) and Ağır et al. 13 described its variable location along the dorsal radius using cadaveric radii. To our best knowledge, currently, there is no literature describing variations in anatomical morphology of Lister’s tubercle and its relationship with the course of the extensor pollicis longus tendon in the third dorsal extensor compartment.
Figure 1. Lister’s tubercle
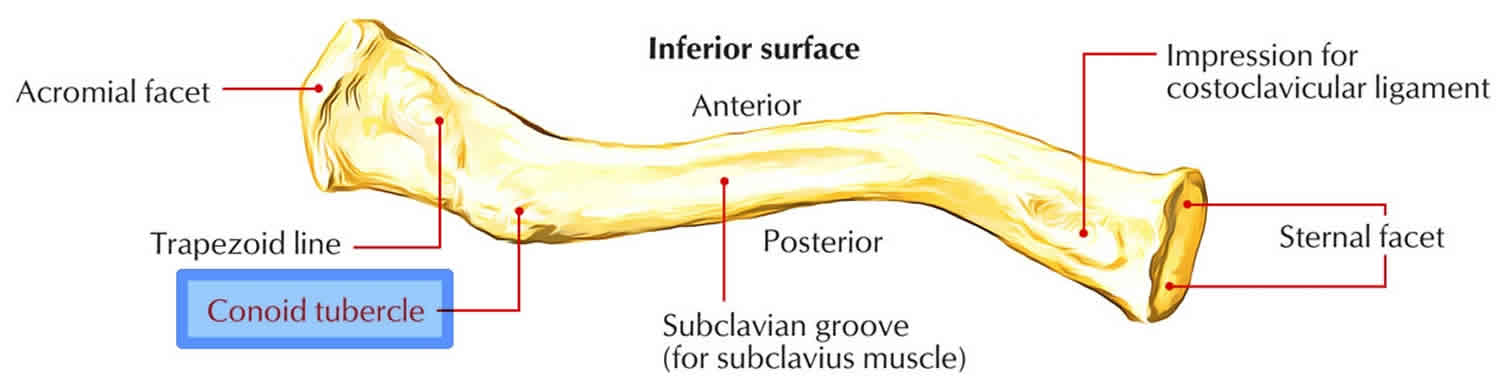
Conoid tubercle
Conoid tubercle is located near the posterior border on the junction of the lateral one-fourth along with medial three-fourth of the clavicle on the inferior surface. The trapezoid ridge spreads forwards as well as laterally through conoid tubercle.
The conoid tubercle gives the attachment for the conoid ligament and is situated on the posterior inferior surface of the lateral curvature of the clavicle.
- The attachment of the trapezoid ligament is indicated by the trapezoid line that spreads out laterally from the conoid tubercle.
- A groove that extends over the central one-third of the inferior surface of the clavicle is medial to the conoid tubercle.
- The acromial end has a rough inferior surface that bears a ridge, the trapezoid line, and a slight rounded projection, the conoid tubercle above the coracoid process.
Figure 2. Conoid tubercle
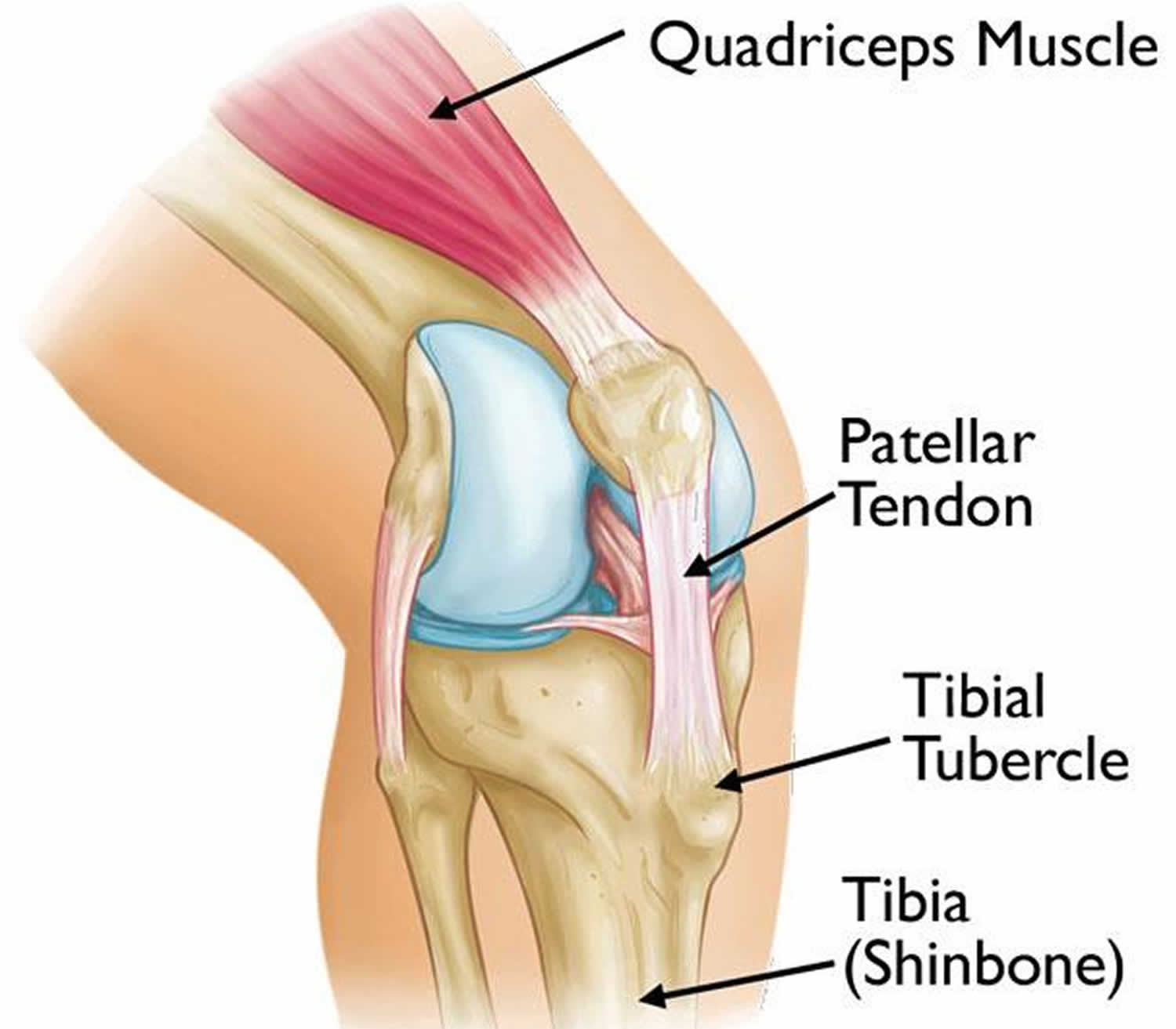
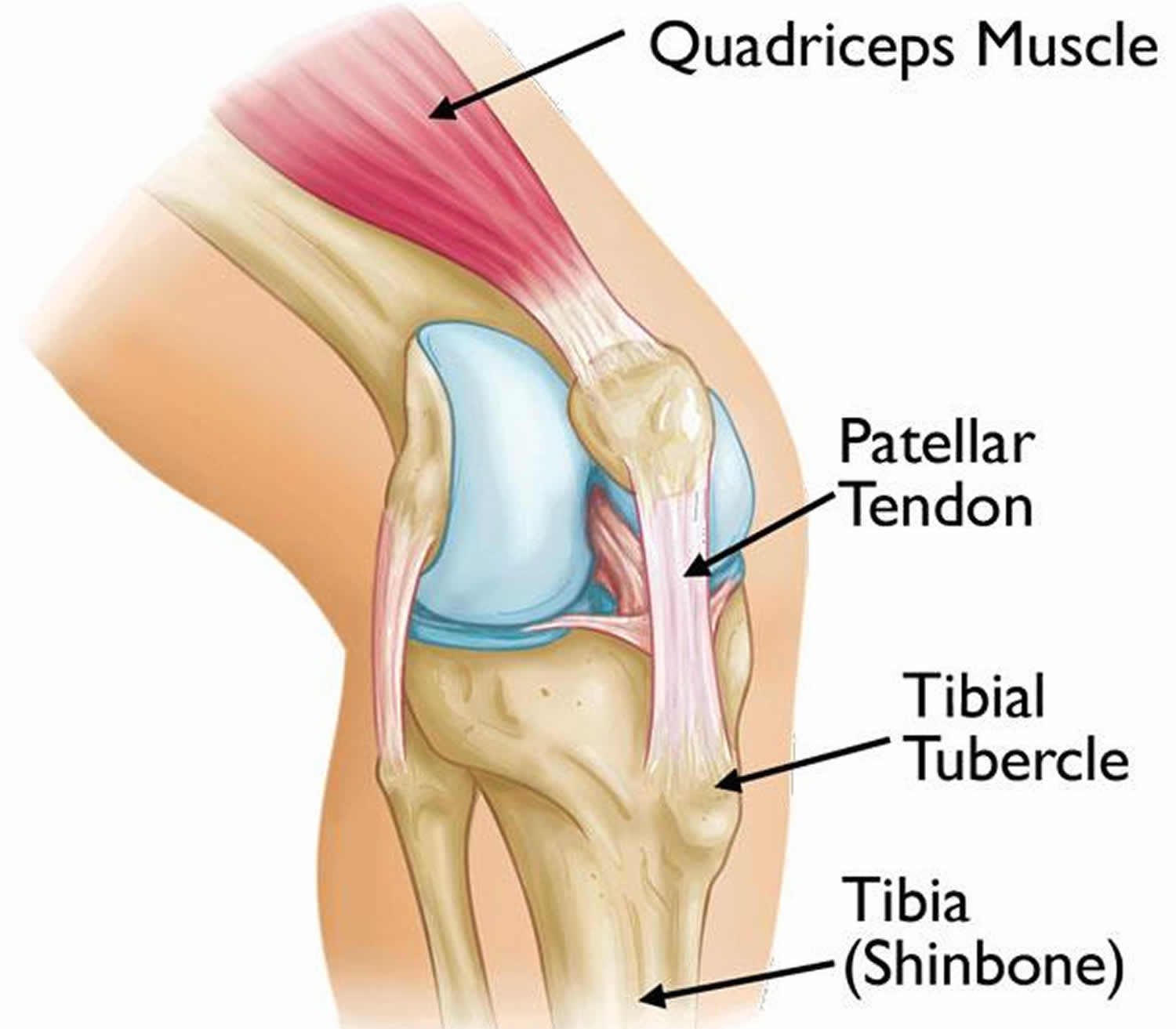
Tibial tubercle
Tibial tubercle is the bony bump where the patellar tendon attaches to the tibia (shinbone).
Figure 3. Tibial tubercle
Tibial tubercle pain
Osgood-Schlatter disease also known as osteochondrosis or traction apophysitis of the tibial tubercle. Osgood-Schlatter disease is an inflammation of the area just below the knee where the tendon from the kneecap (patellar tendon) attaches to the shinbone (tibia). Osgood-Schlatter disease causes tibial tubercle pain. Osgood-Schlatter disease is a common cause of knee pain in growing adolescents 14. Osgood Schlatter’s disease is one of the most common causes of knee pain in the skeletally immature, adolescent athlete. Onset coincides with adolescent growth spurts between ages 10 to 15 years for males and 8 to 13 years for females. The condition is more common in males and occurs more frequently in athletes that participate in sports that involve running and jumping. In adolescents, age 12 to 15, the prevalence of Osgood Schlatter disease is 9.8% (11.4% in males, 8.3% in females). Symptoms present bilaterally in 20% to 30% of patients 15.
Common sports seen in association with traction apophysitis of the tibial tubercle or Osgood-Schlatter disease include:
- Basketball
- Volleyball
- Sprinters
- Gymnastics
- Football
Clinical presentation classically associates atraumatic, insidious onset of anterior knee pain, with tenderness at the patellar tendon insertion site at the tibial tuberosity. The condition is self-limited and occurs secondary to repetitive extensor mechanism stress activities such as jumping and sprinting. Pain level dictates overall treatment, and management includes symptomatic treatment with ice and NSAIDs, as well as activity modification and relative rest from inciting activities in association with lower extremities stretching regimen to correct underlying predisposing biomechanical factors.[1][2][3][4]
The bones of children and adolescents possess a special area where the bone is growing called the growth plate. Growth plates are areas of cartilage located near the ends of bones. When a child is fully grown, the growth plates harden into solid bone.
Some growth plates serve as attachment sites for tendons, the strong tissues that connect muscles to bones. A bony bump called the tibial tubercle covers the growth plate at the end of the tibia. The group of muscles in the front of the thigh (called the quadriceps) attaches to the tibial tubercle.
When a child is active, the quadriceps muscles pull on the patellar tendon which in turn, pulls on the tibial tubercle. In some children, this repetitive traction on the tubercle leads to inflammation of the growth plate. The prominence, or bump, of the tibial tubercle may become very pronounced.
Osgood-Schlatter disease most often occurs during growth spurts, when bones, muscles, tendons, and other structures are changing rapidly. Because physical activity puts additional stress on bones and muscles, children who participate in athletics — especially running and jumping sports – are at an increased risk for this condition. However, less active adolescents may also experience this problem.
In most cases of Osgood-Schlatter disease, simple measures like rest, over-the-counter medication, and stretching and strengthening exercises will relieve pain and allow a return to daily activities.
Osgood-Schlatter disease causes
Osgood Schlatter’s disease is an overuse injury that occurs in active adolescent patients. It occurs secondary to repetitive strain and microtrauma from the force applied by the strong patellar tendon at its insertion into the relatively soft apophysis of the tibial tubercle. This force results in irritation and severe cases partial avulsion of the tibial tubercle apophysis. Force is increased with higher levels of activity and especially after periods of rapid growth. Rarely trauma may lead to full avulsion fracture. Predisposing factors include poor flexibility of quadriceps and hamstrings or other evidence of extensor mechanism misalignment 16.
Osgood-Schlatter disease pathophysiology
The tibial tubercle develops as a secondary ossification center that provides attachment for the patellar tendon. Bone growth exceeds the ability of the muscle-tendon unit to stretch sufficiently to maintain previous flexibility leading to increased tension across the apophysis. The physis is the weakest point in the muscle-tendon-bone-attachment (as opposed to the tendon in an adult) and therefore, at risk of injury from repetitive stress. With repeated contraction of the quadriceps muscle mass, especially with repeated forced knee extension as seen in sports requiring running and jumping (basketball, football, gymnastics), softening and partial avulsion of the apophyseal ossification center may occur with a resulting osteochondritis 17.
The appearance and closure/fusion of the tibial tubercle occurs in the following sequence pattern:
- Tibial tubercle is entirely cartilagenous (age < 11 years)
- Apophysis forms (age 11 to 14 years)
- Apophysis fuses with the proximal tibial epiphysis (age 14 to 18 years)
- The proximal tibial epiphysis and tibial tubercle apophysis fuses with the rest of the proximal tibia (age > 18 years) 18
Osgood-Schlatter disease symptoms
Painful symptoms are often brought on by running, jumping, and other sports-related activities. In some cases, both knees have symptoms, although one knee may be worse than the other.
- Knee pain and tenderness at the tibial tubercle
- Swelling at the tibial tubercle
- Tight muscles in the front or back of the thigh
Osgood-Schlatter disease diagnosis
During the appointment, your doctor will discuss your child’s symptoms and general health. He or she will conduct a thorough examination of the knee to determine the cause of the pain. This will include applying pressure to the tibial tubercle, which should be tender or painful for a child with Osgood-Schlatter disease. In addition, your doctor may also ask your child to walk, run, jump, or kneel to see if the movements bring on painful symptoms.
Your doctor may also order an x-ray image of your child’s knee to help confirm the diagnosis or rule out any other problems. Classic radiographic findings in Osgood-Schlatter disease include an elevated tibial tubercle with soft tissue swelling, fragmentation of the apophysis, or calcification in the distal patellar tendon. It is worth noting that these findings can also be seen as normal variants and do not always represent pathology, so clinical correlation is of utmost importance. If ordering radiographs consider comparing bilateral images to delineate normal versus abnormal in the individual patient 19.
Osgood-Schlatter disease treatment
Ultimately, Osgood-Schlatter disease is self-limiting but may persist for up to 2 years until the apophysis fuses. Treatment for Osgood-Schlatter disease focuses on reducing pain and swelling. This typically requires limiting exercise activity until your child can enjoy activity without discomfort or significant pain afterwards. In some cases, rest from activity is required for several months, followed by a strength conditioning program. However, if your child does not have a large amount of pain or a limp, participation in sports may be safe to continue. There is no evidence to suggest that rest speeds up recovery, but activity restriction is effective in reducing pain 14.
Your doctor may recommend additional treatment methods, including:
- Stretching exercises. Stretches for the front and back of the thigh (quadriceps and hamstring muscles) may help relieve pain and prevent the disease from returning.
- Non-steroidal anti-inflammatory medication. Drugs like ibuprofen and naproxen reduce pain and swelling.
In severe, prolonged cases a short period of knee immobilization may be considered. There is no evidence to recommend injection therapy or surgical intervention for Osgood-Schlatter disease. Symptoms typically are self-limiting with a resolution of pain upon closure of the apophysis. Long-term sequelae may include a thickened or prominent tibial tubercle, but this is asymptomatic in the vast majority of cases 20.
In up to 10% of cases, symptoms may persist >1-2 years beyond skeletal maturity. In skeletally mature patients with persistent symptoms, tibial tubercle osteotomy may be performed.
Osgood-Schlatter disease prognosis
Most symptoms will completely disappear when a child completes the adolescent growth spurt, around age 14 for girls and age 16 for boys. For this reason, surgery is rarely recommended. However, the prominence of the tubercle will persist.
Tibial tubercle fracture
Isolated tibial tubercle fractures or patellar tendon ruptures are common injuries in adolescents through a mechanism involving eccentric contraction of the patellar tendon when the proximal tibial physis is closing 21.
Tibial tubercle fracture will need anatomical reduction to ensure restoration of knee function 22. Methods for treatment of tibial tuberosity fracture include use of tension band wire, independent cortical lag screws or screws placed through a plate, which serve to increase the surface area covered by the screws 23. The choice of treatment should be guided by the morphology of tibial tuberosity fracture and the characteristics of the tibial plateau fracture. When the tibial tubercle fracture is a single large noncomminuted fragment, use of tension band wire or fixation of the tubercle to the posterior tibial cortex with one or more lag screw is the traditionally preferred surgical option 24. In cases where comminution of the tibial tubercle fracture or posterior tibial cortex is present, the cortex of the posterior tibia does not always offer good purchase for screw fixation; plate and screws are preferred in such cases 23. The plate in effect serves to resist the pull of the extensor mechanism on the tibial tubercle. This allows rigid fixation of the tubercle fragment. In this study, the treating surgeon selected screw to fix the fracture.
Maroto et al 23 suggested the tibial tubercle should also be conformed and treated when a suspected or incomplete fracture exists, so as to avoid displacement or malunion in the postoperative period with early mobilization of the knee. As the tibial tubercle has relatively sparse overlying soft tissue, care must be taken to protect the soft tissue envelope during exposure and fixation. Further, it may be necessary to remove the fixation device after bony union has occurred.
References- Chan WY, Chong LR. Anatomical Variants of Lister’s Tubercle: A New Morphological Classification Based on Magnetic Resonance Imaging. Korean J Radiol. 2017;18(6):957–963. doi:10.3348/kjr.2017.18.6.957 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5639161
- [Secondary repair of the extensor pollicis longus]. Saffar P, Fakhoury B. Ann Chir Main. 1987; 6(3):225-9.
- Anatomic landmarks for the first dorsal compartment. Hazani R, Engineer NJ, Cooney D, Wilhelmi BJ. Eplasty. 2008; 8():e53.
- Sonographic appearance of the posterior interosseous nerve at the wrist. Smith J, Rizzo M, Finnoff JT, Sayeed YA, Michaud J, Martinoli C. J Ultrasound Med. 2011 Sep; 30(9):1233-9.
- Anatomic characteristics and clinical importance of the superficial branch of the radial nerve. Ikiz ZA, Uçerler H. Surg Radiol Anat. 2004 Dec; 26(6):453-8.
- Dorsal carpal ligaments of the wrist: normal appearance on multiplanar reconstructions of three-dimensional Fourier transform MR imaging. Smith DK. AJR Am J Roentgenol. 1993 Jul; 161(1):119-25.
- Ağır I, Aytekin MN, Küçükdurmaz F, Gökhan S, Cavuş UY. Anatomical Localization of Lister’s Tubercle and its Clinical and Surgical Importance. Open Orthop J. 2014;8:74–77. Published 2014 Apr 4. doi:10.2174/1874325001408010074 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4023390
- A method of defining palpable landmarks for the ligament-splitting dorsal wrist capsulotomy. Berger RA. J Hand Surg Am. 2007 Oct; 32(8):1291-5.
- Anatomical relations of the superficial sensory branches of the radial nerve: a cadaveric study with clinical implications. Samarakoon LB, Lakmal KC, Thillainathan S, Bataduwaarachchi VR, Anthony DJ, Jayasekara RW. Patient Saf Surg. 2011 Nov 4; 5(1):28.
- Radioscapholunate arthrodesis using low-profile dorsal pi plate. Galvis EJ, Kumar KK, Özyurekoglu T. Tech Hand Up Extrem Surg. 2013 Jun; 17(2):80-3.
- [Fixation of fractures of the distal radius using the “nail-plate”]. Espen D. Oper Orthop Traumatol. 2009 Nov; 21(4-5):459-71.
- Computer tomography aided 3D analysis of the distal dorsal radius surface and the effects on volar plate osteosynthesis. Pichler W, Windisch G, Schaffler G, Rienmüller R, Grechenig W. J Hand Surg Eur Vol. 2009 Oct; 34(5):598-602.
- Anatomical Localization of Lister’s Tubercle and its Clinical and Surgical Importance. Ağır I, Aytekin MN, Küçükdurmaz F, Gökhan S, Cavuş UY. Open Orthop J. 2014; 8():74-7.
- Smith JM, Varacallo M. Osgood Schlatter’s Disease (Tibial Tubercle Apophysitis) [Updated 2019 May 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441995
- Indiran V, Jagannathan D. Osgood-Schlatter Disease. N. Engl. J. Med. 2018 Mar 15;378(11):e15
- Hart E, Meehan WP, Bae DS, d’Hemecourt P, Stracciolini A. The Young Injured Gymnast: A Literature Review and Discussion. Curr Sports Med Rep. 2018 Nov;17(11):366-375.
- Seyfettinoğlu F, Köse Ö, Oğur HU, Tuhanioğlu Ü, Çiçek H, Acar B. Is There a Relationship between Patellofemoral Alignment and Osgood-Schlatter Disease? A Case-Control Study. J Knee Surg. 2018 Dec 21
- Watanabe H, Fujii M, Yoshimoto M, Abe H, Toda N, Higashiyama R, Takahira N. Pathogenic Factors Associated With Osgood-Schlatter Disease in Adolescent Male Soccer Players: A Prospective Cohort Study. Orthop J Sports Med. 2018 Aug;6(8):2325967118792192
- Rathleff MS, Straszek CL, Blønd L, Thomsen JL. [Knee pain in children and adolescents]. Ugeskr. Laeg. 2019 Mar 25;181, 13
- Itoh G, Ishii H, Kato H, Nagano Y, Hayashi H, Funasaki H. Risk assessment of the onset of Osgood-Schlatter disease using kinetic analysis of various motions in sports. PLoS ONE. 2018;13(1):e0190503
- Pascarella F, Ziranu A, Maccauro G. Tibial tubercle fracture in a 14-year-old athlete with bilateral lower pole bipartite patella and osgood-schlatter disease. Case Rep Orthop. 2015;2015:815061. doi:10.1155/2015/815061 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4345235
- Mckoy BE, Stanitski CL. Acute tibial tubercle avulsion fractures. Orthop Clin North Am 2004;24:181
- Maroto MD, Scolaro JA, Henley MB, et al. Management and incidence of tibial tubercle fractures in bicondylar fractures of the tibial plateau. Bone Joint J 2013;95-B:1697–702
- Aterkar VM, Mahajan UD, Somani AM. Tibial tuberosity avulsion fracture in an adult—a rare case report. Int J Med Res Health Sci 2014;3:1016





{kind=link}