
What is unstable angina
Unstable angina also called acute coronary syndrome, is a medical emergency where your heart doesn’t get enough blood flow and oxygen. Unstable angina causes unexpected chest pain, and usually occurs while resting. The most common cause of unstable angina is reduced blood flow to the heart muscle because the coronary arteries that are narrowed by fatty buildups (atherosclerosis) suddenly rupture causing injury to the coronary blood vessel resulting in blood clotting which blocks the flow of blood to the heart muscle. Unstable angina can also be caused by blood clots that block or partially block your heart’s coronary arteries. Unstable angina is a sign of more severe heart disease and unstable angina may lead to a heart attack.
Unstable angina should be treated as an emergency. If you have new, worsening or persistent chest discomfort, you need to go to the emergency room. You could be having a heart attack which puts you at increased risk for severe cardiac arrhythmias or cardiac arrest, which could lead to sudden death.
Symptoms of angina may include:
- Chest pain that you may also feel in the shoulder, arm, jaw, neck, back, or other area
- Discomfort that feels like tightness, squeezing, crushing, burning, choking, or aching
- Discomfort that occurs at rest and does not easily go away when you take medicine
- Shortness of breath
- Sweating
- Chest pain is triggered by physical exertion or stress
- Chest pain stops within a few minutes of resting
Unstable angina is chest pain that is sudden and often gets worse over a short period of time.
You may be developing unstable angina if your:
- Chest pain starts to feel different, is more severe, comes more often, or occurs with less activity or while you are at rest
- Chest pain lasts longer than 15 to 20 minutes
- Chest pain occurs without cause (for example, while you are asleep or sitting quietly)
- Chest pain does not respond well to a medicine called nitroglycerin (especially if this medicine worked to relieve chest pain in the past)
- Chest pain occurs with a drop in blood pressure or shortness of breath
Unstable angina is a warning sign that a heart attack may happen soon and needs to be treated right away. See your health care provider if you have any type of chest pain.
You may need to check into the hospital to get some rest, have more tests, and prevent complications.
Blood thinners (antiplatelet drugs) are used to treat and prevent unstable angina. You will receive these drugs as soon as possible if you can take them safely. Medicines include aspirin and the prescription drug clopidogrel or something similar (ticagrelor, prasugrel). These medicines may be able to reduce the chance of a heart attack or the severity of a heart attack that occurs.
During an unstable angina event:
- You may get heparin (or another blood thinner) and nitroglycerin (under the tongue or through an IV).
- Other treatments may include medicines to control blood pressure, anxiety, abnormal heart rhythms, and cholesterol (such as a statin drug).
A procedure called angioplasty and stenting can often be done to open a blocked or narrowed artery:
- Angioplasty is a procedure to open narrowed or blocked blood vessels that supply blood to the heart.
- A coronary artery stent is a small, metal mesh tube that opens up (expands) inside a coronary artery. A stent is often placed after angioplasty. It helps prevent the artery from closing up again. A drug-eluting stent has medicine in it that helps prevent the artery from closing over time.
Heart bypass surgery may be done for some people. The decision to have this surgery depends on:
- Which arteries are blocked
- How many arteries are involved
- Which parts of the coronary arteries are narrowed
- How severe the narrowings are
How well you do depends on many different things, including:
- How many and which arteries in your heart are blocked, and how severe the blockage is
- If you have ever had a heart attack
- How well your heart muscle is able to pump blood out to your body
Abnormal heart rhythms and heart attacks can cause sudden death.
Unstable angina or acute coronary syndrome is a medical emergency.
If you have unstable angina symptoms, call your local emergency number quickly.
DO NOT:
- Try to drive yourself to the hospital.
- WAIT. If you are having a heart attack, you are at greatest risk of sudden death in the early hours.
Call your local emergency services number if your angina pain:
- Is not better 5 minutes after you take nitroglycerin (your provider may tell you to take 3 total doses)
- Does not go away after 3 doses of nitroglycerin
- Is getting worse
- Returns after the nitroglycerin helped at first
See your doctor if:
- You are having angina symptoms more often
- You are having angina when you are sitting (rest angina)
- You are feeling tired more often
- You are feeling faint or lightheaded, or you pass out
- Your heart is beating very slowly (less than 60 beats a minute) or very fast (more than 120 beats a minute), or it is not steady
- You are having trouble taking your heart medicines
- You have any other unusual symptoms
If you think you are having a heart attack, call your local emergency services number for an ambulance right away.
Figure 1. Coronary Arteries supplying blood, oxygen & nutrients to your heart
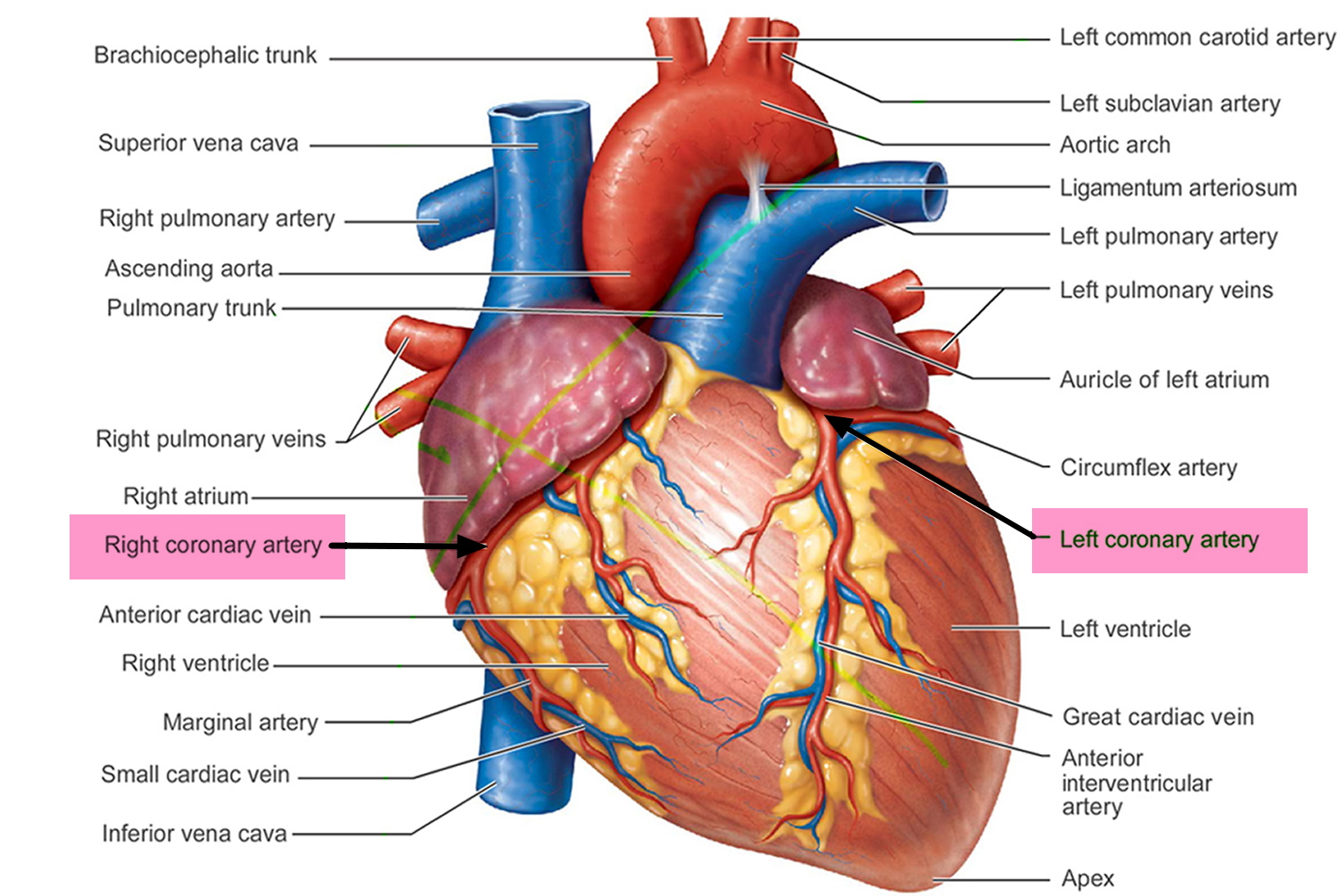
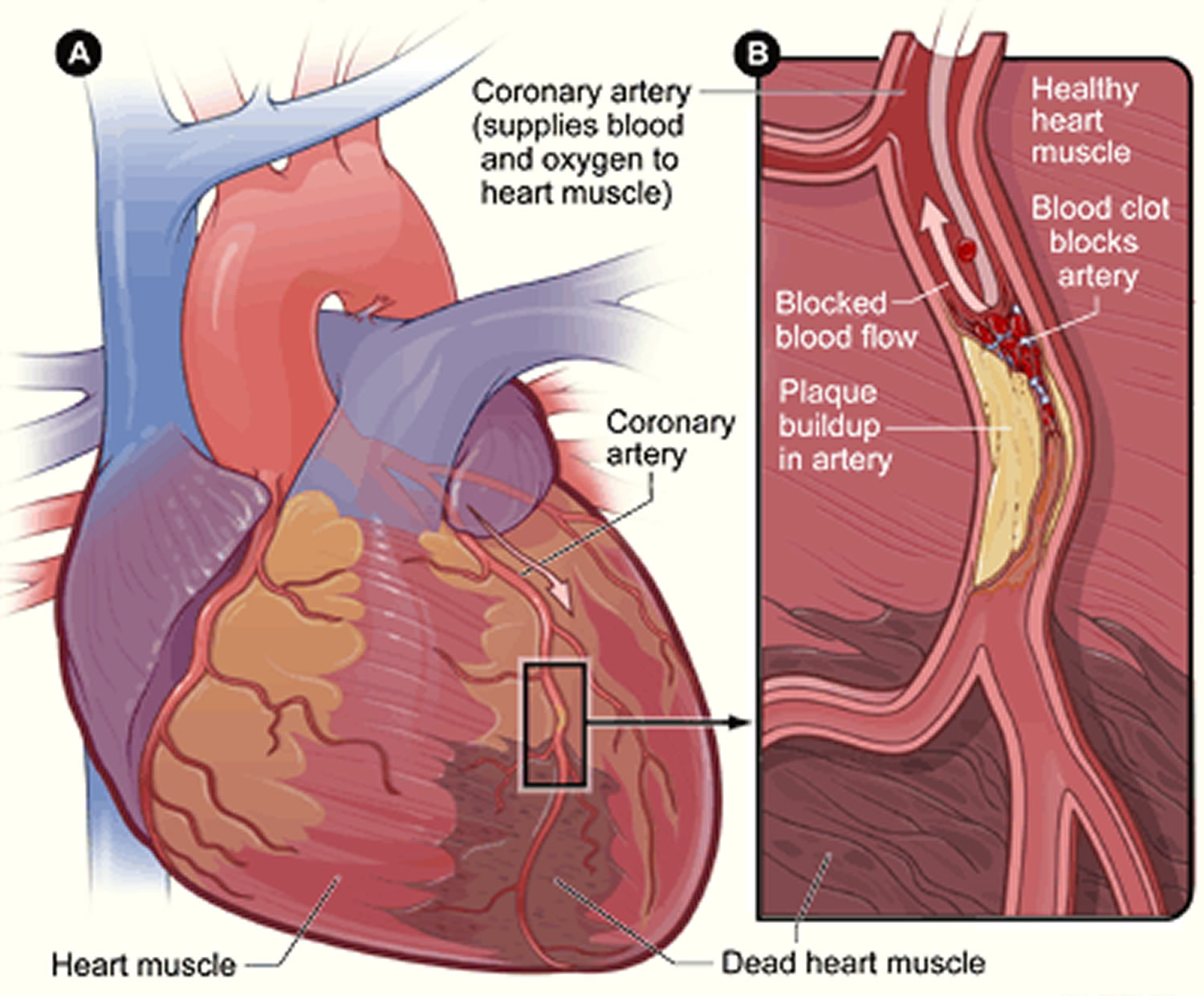
Figure 2. Heart With Muscle Damage and a Blocked Left Coronary Artery
Stable vs Unstable angina
Angina is chest pain caused by reduced blood flow to the heart muscles. Angina is not usually life threatening, but it’s a warning sign that you could be at risk of a heart attack or stroke.
With treatment and healthy lifestyle changes, it’s possible to control angina and reduce the risk of these more serious problems.
The main symptom of angina is chest pain. With stable angina, the chest pain or other symptoms only occur with a certain amount of activity or stress. The pain does not occur more often or get worse over time.
Characteristics of stable angina
- Develops when your heart works harder, such as when you exercise or climb stairs
- Can usually be predicted and the pain is usually similar to previous types of chest pain you’ve had
- Lasts a short time, perhaps five minutes or less
- Disappears sooner if you rest or use your angina medication
The severity, duration and type of angina can vary. New or different symptoms may signal a more dangerous form of angina (unstable angina) or a heart attack.
Characteristics of unstable angina (a medical emergency)
- Occurs even at rest
- Is a change in your usual pattern of angina
- Is unexpected
- Is usually more severe and lasts longer than stable angina, maybe 30 minutes or longer
- May not disappear with rest or use of angina medication
- Might signal a heart attack
Unstable angina is more serious – the attacks are more unpredictable. There may not be an obvious trigger for attacks and can continue despite resting. Medication might not help. Some people develop unstable angina after having stable angina.
There’s another type of angina, called variant angina or Prinzmetal’s angina. This type of angina is rarer. It’s caused by a spasm in your heart’s arteries that temporarily reduces blood flow.
Characteristics of variant angina (Prinzmetal’s angina)
- Usually happens when you’re resting, usually between midnight and early morning. These attacks can be very painful.
- Is often severe
- Prinzmetal’s angina is rare, representing about two out of 100 cases of angina, and usually occurs in younger patients than those who have other kinds of angina.
- Causes of variant angina (Prinzmetal’s Angina) is a spasm in the coronary arteries (which supply blood to the heart muscle). Prinzmetal Angina is not due to atherosclerosis but rather to spasmodic contraction of the coronary arteries.
- May be relieved by angina medication
Unstable angina causes
Coronary artery disease due to atherosclerosis is the most common cause of unstable angina. Atherosclerosis is the buildup of fatty material, called plaque, along the walls of the arteries. This causes arteries to become narrowed and less flexible. The narrowing can reduce blood flow to the heart, causing chest pain. Blood clots that block an coronary artery partially or totally are what causes unstable angina. Blood clots may form, partially dissolve, and later form again and angina can occur each time a clot blocks blood flow in a coronary artery.
People with unstable angina are at higher risk of having a heart attack.
Rare causes of angina are:
- Abnormal function of tiny branch arteries without narrowing of larger arteries (called microvascular dysfunction or Syndrome X)
- Coronary artery spasm
Risk factors for coronary artery disease include:
- Diabetes
- Family history of early coronary heart disease (a close relative such as a sibling or parent had heart disease before age 55 in a man or before age 65 in a woman)
- High blood pressure (hypertension). High blood pressure promotes artery damage which may initiate or exacerbate atherosclerosis causing plaque rupture. It should be noted that hypertension also worsens myocardial ischaemia (heart attack) through the adaptive changes it causes in the left ventricle. In hypertension the heart has to work harder to pump blood and as a consequence the left ventricle becomes hypertrophied (increased muscle bulk). This bulkier muscle then has higher blood requirements. This is theoretically independent of vessel narrowing.
- High LDL “bad” cholesterol
- Low HDL “good” cholesterol
- Male gender
- Sedentary lifestyle (not getting enough exercise)
- Obesity
- Older age
- Smoking
- Stress/anxious personality.
- Alcohol consumption.
Unstable angina prevention
Some studies have shown that making a few lifestyle changes can prevent blockages from getting worse and may actually improve them. Lifestyle changes can also help prevent some angina attacks. Your provider may tell you to:
- Lose weight if you are overweight
- Stop smoking
- Exercise regularly
- Drink alcohol in moderation only
- Eat a healthy diet that is high in vegetables, fruits, whole grains, fish, and lean meats
Your provider will also recommend that you keep other health conditions such as high blood pressure, diabetes, and high cholesterol levels under control.
If you have one or more risk factors for heart disease, talk to your provider about taking aspirin or other medicines to help prevent a heart attack. Aspirin therapy (75 to 325 mg a day) or drugs such as clopidogrel, ticagrelor or prasugrel may help prevent heart attacks in some people. Aspirin and other blood thinning therapies are recommended if the benefit is likely to outweigh the risk of side effects.
Unstable angina signs and symptoms
Unstable angina chest pain or discomfort:
- Often occurs while you may be resting, sleeping, or with little physical exertion
- Comes as a surprise
- May last longer than stable angina
- Rest or medicine usually do not help relieve it
- May get worse over time
- Can lead to a heart attack
Angina in women
A woman’s angina symptoms can be different from the classic angina symptoms. These differences may lead to delays in seeking treatment. For example, chest pain is a common symptom in women with angina, but it may not be the only symptom or the most prevalent symptom for women. Women may also experience symptoms such as:
- Nausea
- Shortness of breath
- Abdominal pain
- Discomfort in the neck, jaw or back
- Stabbing pain instead of chest pressure
Unstable angina possible complications
Unstable angina may lead to:
- Abnormal heart rhythms (arrhythmias)
- A heart attack
- Heart failure
Unstable angina diagnosis
Your doctor will do a physical exam and check your blood pressure. Your doctor may hear abnormal sounds, such as a heart murmur or irregular heartbeat, when listening to your chest with a stethoscope.
Tests for angina include:
- Blood tests to show if you have heart tissue damage or are at a high risk for heart attack, including troponin I and T-00745, creatine phosphokinase (CPK), and myoglobin.
- ECG (electrocardiogram).
- Echocardiography.
- Stress tests, such as exercise tolerance test (stress test or treadmill test), nuclear stress test, or stress echocardiogram.
- Coronary angiography. This test involves taking pictures of the heart arteries using x-rays and dye. It is the most direct test to diagnose heart artery narrowing and find clots.
Unstable angina treatment
Immediate treatment goals are to relieve pain and distress, improve blood flow, and restore heart function as quickly and as best as possible. Long-term treatment goals are to improve overall heart function, manage risk factors and lower the risk of a heart attack. A combination of drugs and surgical procedures may be used to meet these goals.
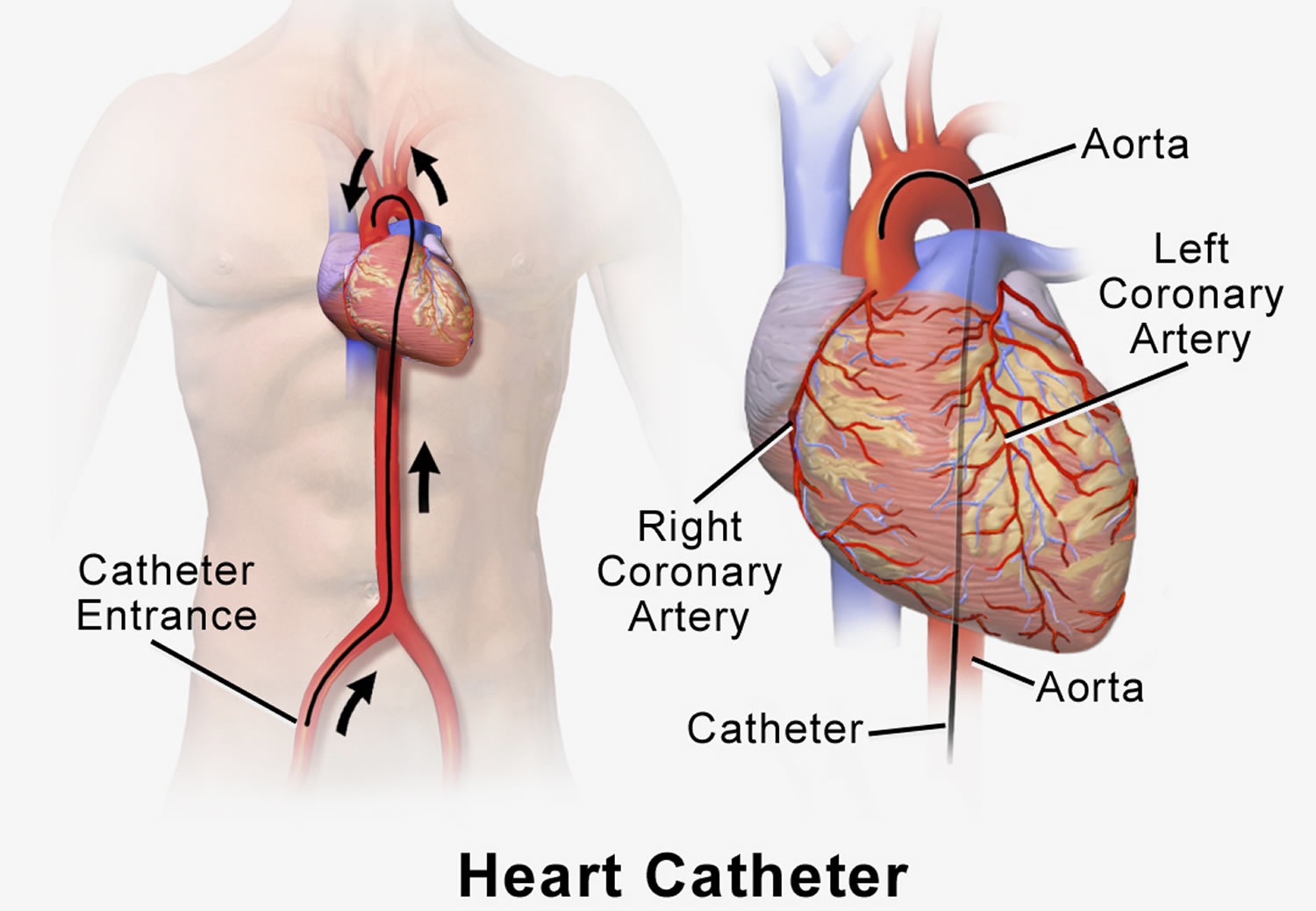
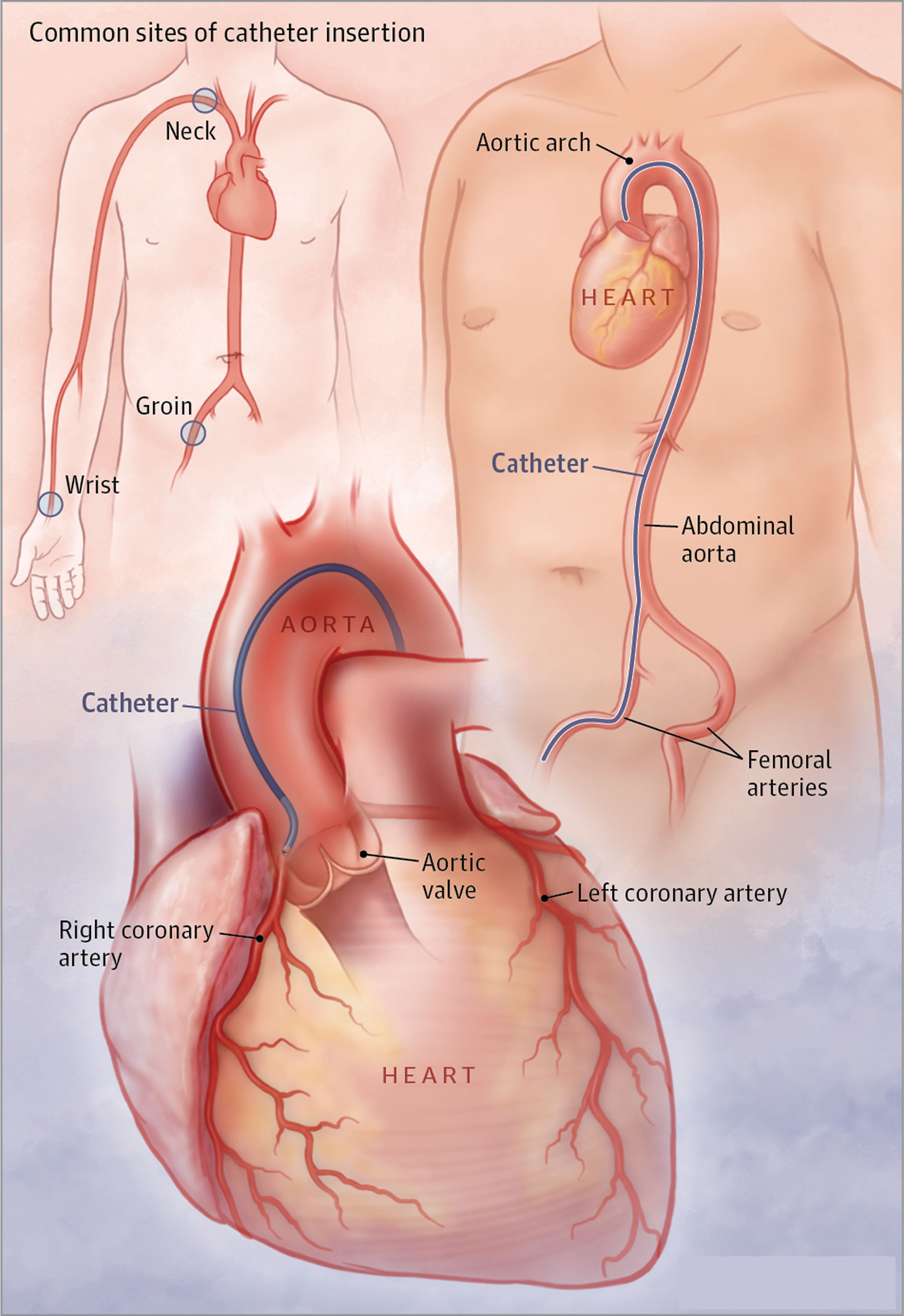
First, your healthcare provider will need to find the blocked part or parts of the coronary arteries by performing a cardiac catheterization. In this procedure, a catheter is guided through an artery in the arm or leg and into the coronary arteries, then injected with a liquid dye through the catheter. High-speed X-ray movies record the course of the dye as it flows through the arteries, and doctors can identify blockages by tracing the flow. An evaluation of how well your heart is working also can be done during cardiac catheterization.
Figure 3. Cardiac catheterization
Next, based on the extent of the coronary artery blockage(s) your doctor will discuss with you the following treatment options:
- Percutaneous coronary intervention may be required to open a blocked coronary artery. Briefly, this procedure involves undergoing cardiac catheterization followed by using a catheter with a small inflatable balloon at the tip. The balloon is inflated, squeezing open the fatty plaque deposit located on the inner lining of the coronary artery. Then the balloon is deflated and the catheter is withdrawn. This procedure is often followed by insertion of a stent to then keep the coronary artery vessel propped open to allow for improved blood flow to the heart muscle.
- Coronary artery bypass graft (CABG) surgery may be indicated depending on the extent of coronary artery blockages and medical history. Coronary artery bypass graft (CABG) is a surgical procedure where a donor blood vessel from another site in the body is used to bypass area of stenosis. Coronary artery bypass graft (CABG) confers significant symptomatic and prognostic benefits in patients with severe triple coronary arteries disease (areas of stenosis in all three coronary arteries). Wherever possible the left internal mammary artery (LIMA) is used to supply blood to the coronary circulation downstream from the stenosis. Grafts using the saphenous vein (from the leg) are still frequently used. Newer minimally invasive techniques using laparoscopic (keyhole) technology are currently being developed.
Before any of these procedures, a doctor must find the blocked part or parts of the coronary arteries. He or she will guide a catheter through an artery in the arm or leg and into the coronary arteries, then inject a liquid dye through the catheter. High-speed X-ray movies record the course of the dye as it flows through the arteries, and doctors can identify blockages by tracing the flow. An evaluation of how the heart works also can be done during cardiac catheterization.
Unstable angina guidelines
The goals of the American College of Cardiology and the American Heart Association have collaborated with the National Heart, Lung, and Blood Institute to develop clinical practice guidelines for assessment of cardiovascular risk, lifestyle modifications to reduce cardiovascular risk, management of blood cholesterol in adults, and management of overweight and obesity in adults 1.
These guidelines are meant to define practices that meet the needs of patients in most circumstances and are not a replacement for clinical judgment. The ultimate decision about care of a particular patient must be made by the healthcare provider and patient in light of the circumstances presented by that patient. As a result, situations might arise in which deviations from these guidelines may be appropriate. These considerations notwithstanding, in caring for most patients, clinicians can employ the recommendations confidently to reduce the risks of atherosclerotic cardiovascular disease (CVD) events.
Diet Recommendations for LDL-C “bad cholesterol” Lowering
Advise adults who would benefit from LDL-C “bad cholesterol” lowering to:
- Consume a dietary pattern that emphasizes intake of vegetables, fruits, and whole grains; includes low-fat dairy products, poultry, fish, legumes, nontropical vegetable oils, and nuts; and limits intake of sweets, sugar-sweetened beverages, and red meats.
- Adapt this dietary pattern to appropriate calorie requirements, personal and cultural food preferences, and nutrition therapy for other medical conditions (including diabetes).
- Achieve this pattern by following plans such as the DASH dietary pattern, the US Department of Agriculture (USDA) Food Pattern, or the American Heart Association (AHA) Diet.
- Aim for a dietary pattern that achieves 5% to 6% of calories from saturated fat.
Sodium and Blood Pressure
Diet Recommendations for Blood Pressure Lowering
1. Advise adults who would benefit from blood pressure (BP) lowering to:
- a. Consume a dietary pattern that emphasizes intake of vegetables, fruits, and whole grains; includes low-fat dairy products, poultry, fish, legumes, nontropical vegetable oils, and nuts; and limits intake of sweets, sugar-sweetened beverages, and red meats.
- i. Adapt this dietary pattern to appropriate calorie requirements, personal and cultural food preferences, and nutrition therapy for other medical conditions (including diabetes).
- ii. Achieve this pattern by following plans such as the DASH dietary pattern, the USDA Food Pattern, or the AHA Diet.
2. Advise adults who would benefit from blood pressure lowering to:
- a. Consume no more than 2400 mg of sodium/day;
- b. Further reduction of sodium intake to 1500 mg/day can result in even greater reduction in BP;
- c. Even without achieving these goals, reducing sodium intake by at least 1000 mg/day lowers BP.
- d. Combine the DASH dietary pattern with lower sodium intake.
Physical Activity: Lipids and Blood Pressure
Physical Activity Recommendations
Most health benefits occur with at least 150 minutes (2 hours and 30 minutes) a week of moderate-intensity physical activity, such as brisk walking. Additional benefits occur with more physical activity 2.
- In general, advise adults to engage in aerobic physical activity to reduce LDL “bad” cholesterol and non–HDL-cholesterol: 3 to 4 sessions per week, lasting on average 40 minutes per session, and involving moderate- to vigorous-intensity physical activity.
- In general, advise adults to engage in aerobic physical activity to lower blood pressure (BP): 3 to 4 sessions per week, lasting on average 40 minutes per session, and involving moderate- to vigorous-intensity physical activity.
- 2013 AHA/ACC Guideline on Lifestyle Management to Reduce Cardiovascular Risk. A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. http://circ.ahajournals.org/content/129/25_suppl_2/S76.long
- Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Report, 2008. Washington, DC: US Department of Health and Human Services; 2008:1–683





{kind=link}