Vitamin B6 deficiency
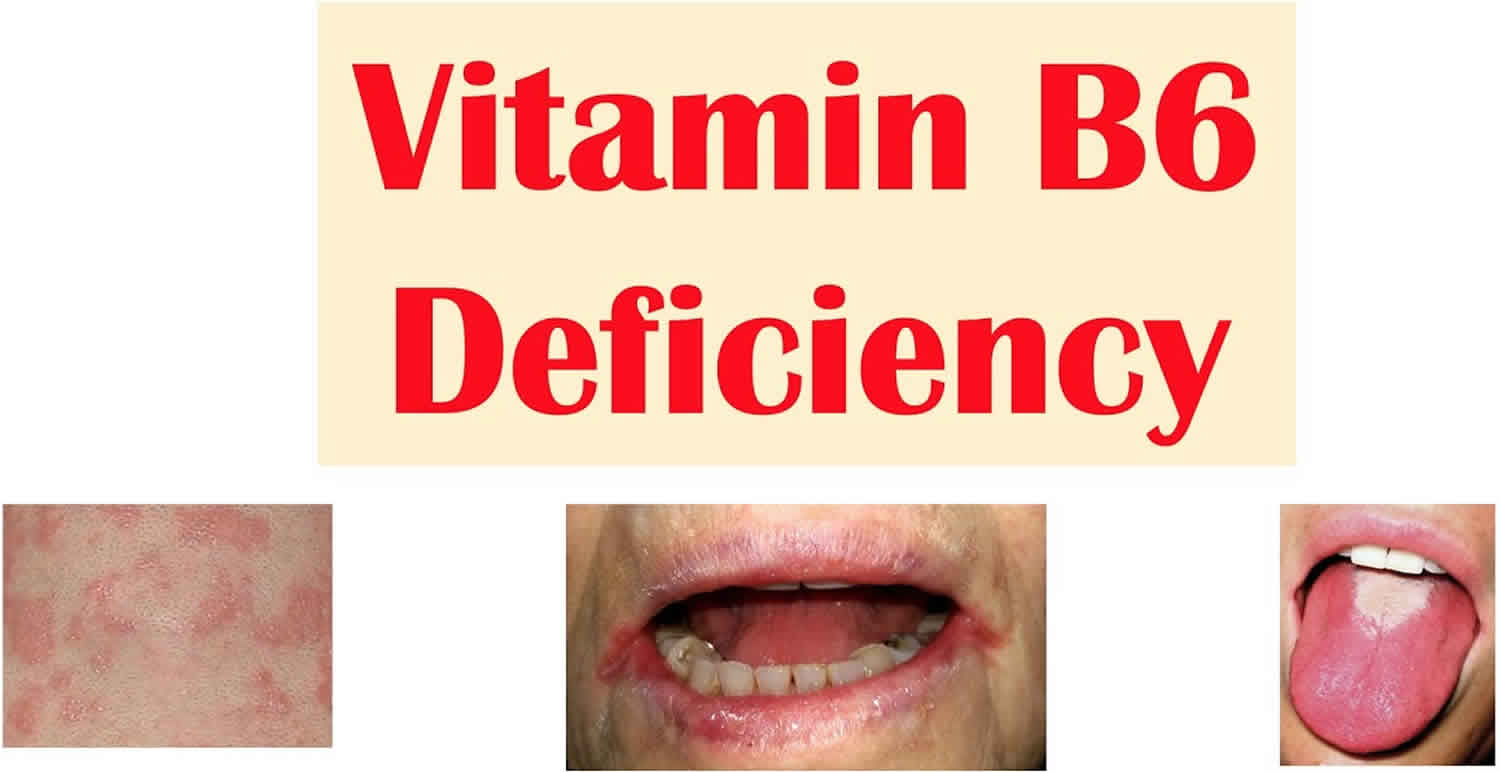
Isolated vitamin B6 deficiency, also known as pyridoxine deficiency, is very rare in the United States; inadequate vitamin B6 status is usually associated with low concentrations of other B-complex vitamins, such as vitamin B12 and folic acid 1, 2, 3. Vitamin B6 deficiency causes biochemical changes that become more obvious as the deficiency progresses 2, 4. Vitamin B6 deficiency is associated with microcytic anemia, peripheral neuropathy, mental status changes, electroencephalographic abnormalities, seborrhoeic dermatitis, angular cheilitis (scaling on the lips and cracks at the corners of the mouth) and glossitis (inflammation of the tongue), depression and confusion, and weakened immune function 1, 5, 2, 6. Individuals with borderline vitamin B6 concentrations or mild deficiency might have no deficiency signs or symptoms for months or even years. Fetal brain development requires adequate vitamin B6, and this continues throughout infancy. In infants, vitamin B6 deficiency causes irritability, abnormally acute hearing, and convulsive seizures 2, 7.
Vitamin B6 is one of the vital micronutrients involved in one-carbon metabolism along with folate and vitamin B12 8. Pyridoxal 5-phosphate (PLP), the active form of vitamin B6, acts as a cofactor in more than 100 enzymatic reactions in carbohydrate, amino acids and lipid metabolism 9 . It has also been shown to have antioxidant 10, anti-inflammatory properties 11, cognitive functions 12, 13, 14, 15 and a role in the immune response 16, 17.
Vitamin B6 deficiency is uncommon in the United States 18. Most people in the United States get enough vitamin B6 from the foods they eat 19, 20. However, these groups of people are more likely than others to have trouble getting enough vitamin B6 18, 1:
- People whose kidneys do not work properly, including people who are on kidney dialysis (hemodialysis or peritoneal dialysis) and those who have had a kidney transplant.
- People with autoimmune disorders, which cause their immune system to mistakenly attack their own healthy tissues. For example, people with rheumatoid arthritis, celiac disease, Crohn’s disease, ulcerative colitis, or inflammatory bowel disease sometimes have low vitamin B6 levels.
- People with protein-energy malnutrition.
- States of decreased consumption and/or absorption. For example, pregnancy, chronic alcohol dependence and post-weight loss surgery.
End-stage renal diseases, chronic renal insufficiency, and other kidney diseases can cause vitamin B6 deficiency 21. In addition, vitamin B6 deficiency can result from malabsorption syndromes, such as celiac disease, Crohn’s disease, and ulcerative colitis. Certain genetic diseases, such as homocystinuria, can also cause vitamin B6 deficiency 2. Some medications, such as antiepileptic drugs, can lead to vitamin B6 deficiency over time.
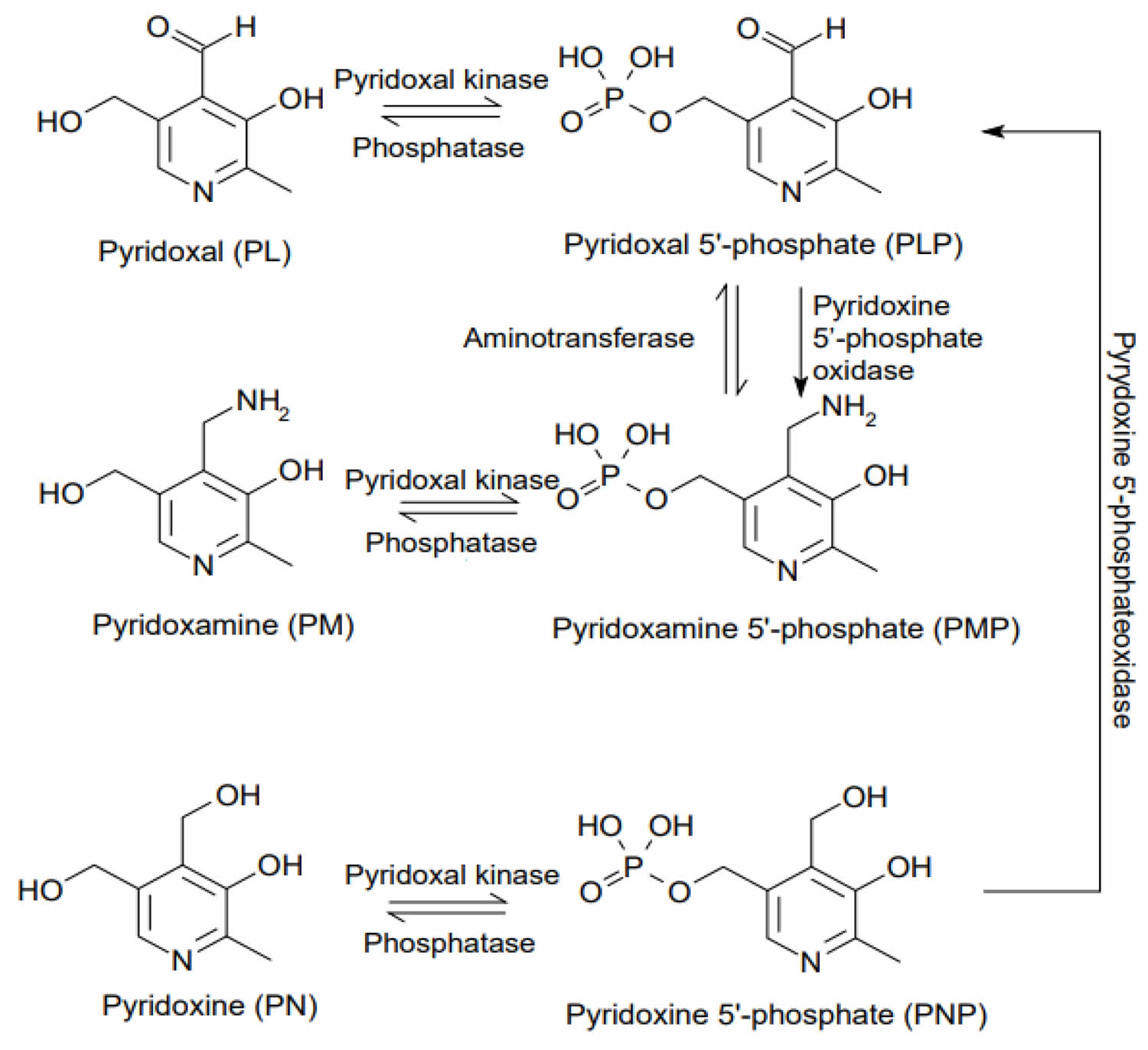
Vitamin B6 concentrations can be measured directly by assessing concentrations of pyridoxal 5’ phosphate (PLP); other vitamers; or total vitamin B6 in plasma, red blood cells, or urine 22. Vitamin B6 concentrations can also be measured indirectly by assessing either red blood cell aminotransferase saturation by pyridoxal 5’ phosphate (PLP) or tryptophan metabolites. Plasma pyridoxal 5’ phosphate (PLP) is the most common measure of vitamin B6 status 23.
Pyridoxal 5’ phosphate (PLP) concentrations of more than 30 nanomole per liter [nmol/L] have been traditional indicators of adequate vitamin B6 status in adults 21. However, the Food and Nutrition Board at the Institute of Medicine of the National Academies used a plasma pyridoxal 5’ phosphate (PLP) level of 20 nmol/L as the major indicator of adequacy to calculate the Recommended Dietary Allowances (RDAs) for adults 22, 21. Plasma Pyridoxal 5’ phosphate (PLP) of less than 20 nmol/L is considered vitamin B6 deficiency 24.
What is Vitamin B6?
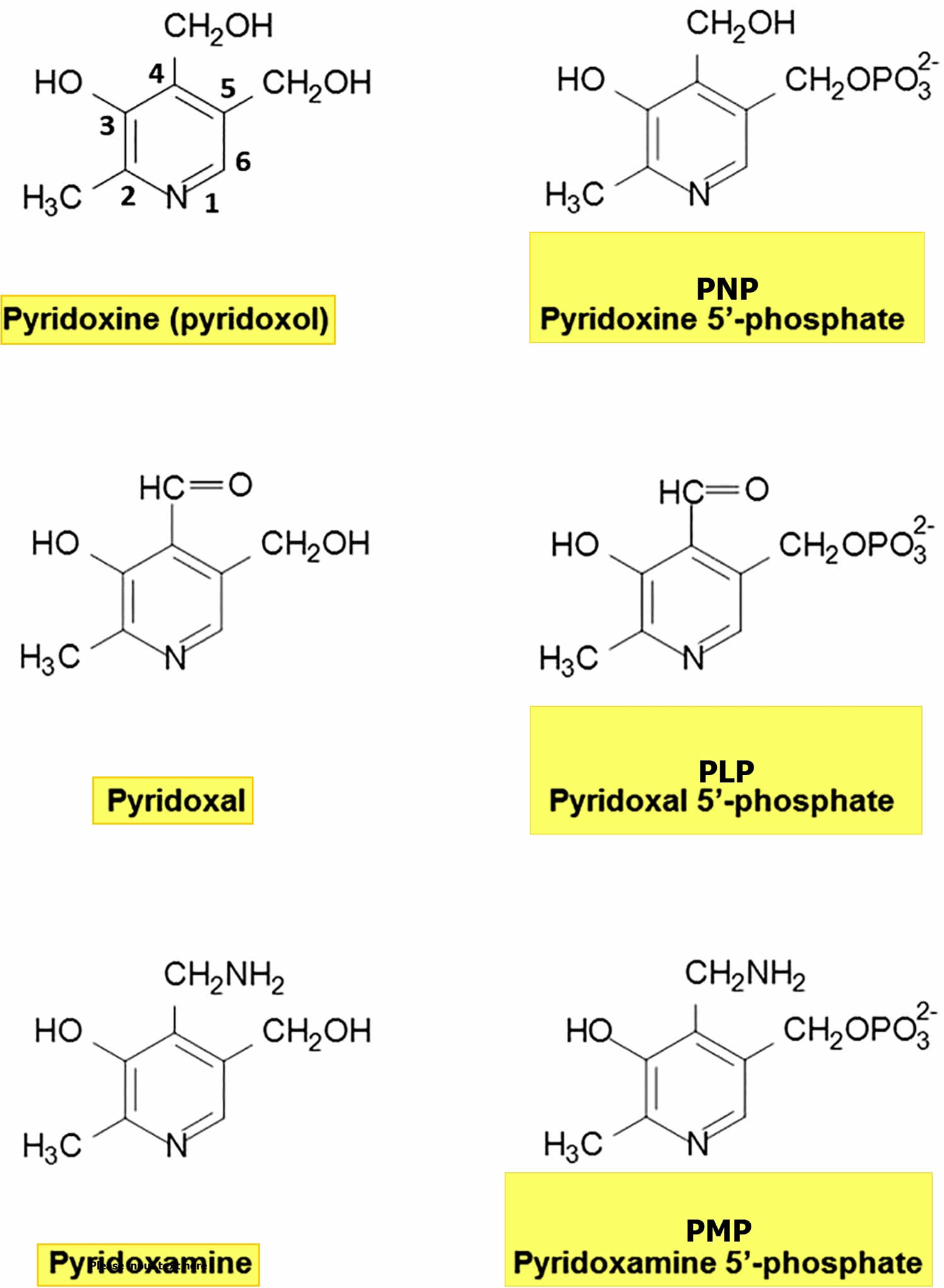
Vitamin B6 is a water-soluble vitamin that is naturally present in many foods, added to others, and available as a dietary supplement. Vitamin B6 is the generic name for six compounds (vitamers) with vitamin B6 activity (Figure 1) 5, 2, 25, 26, 27, 28:
- Pyridoxine (pyridoxol) an alcohol, commonly known as vitamin B6;
- Pyridoxal, an aldehyde;
- Pyridoxamine, which contains an amino group; and their respective 5’-phosphate esters.
- Pyridoxal 5’ phosphate (PLP) and pyridoxamine 5’ phosphate (PMP) are the active coenzyme forms of vitamin B6 involved in over 4% of all enzymatic reactions.
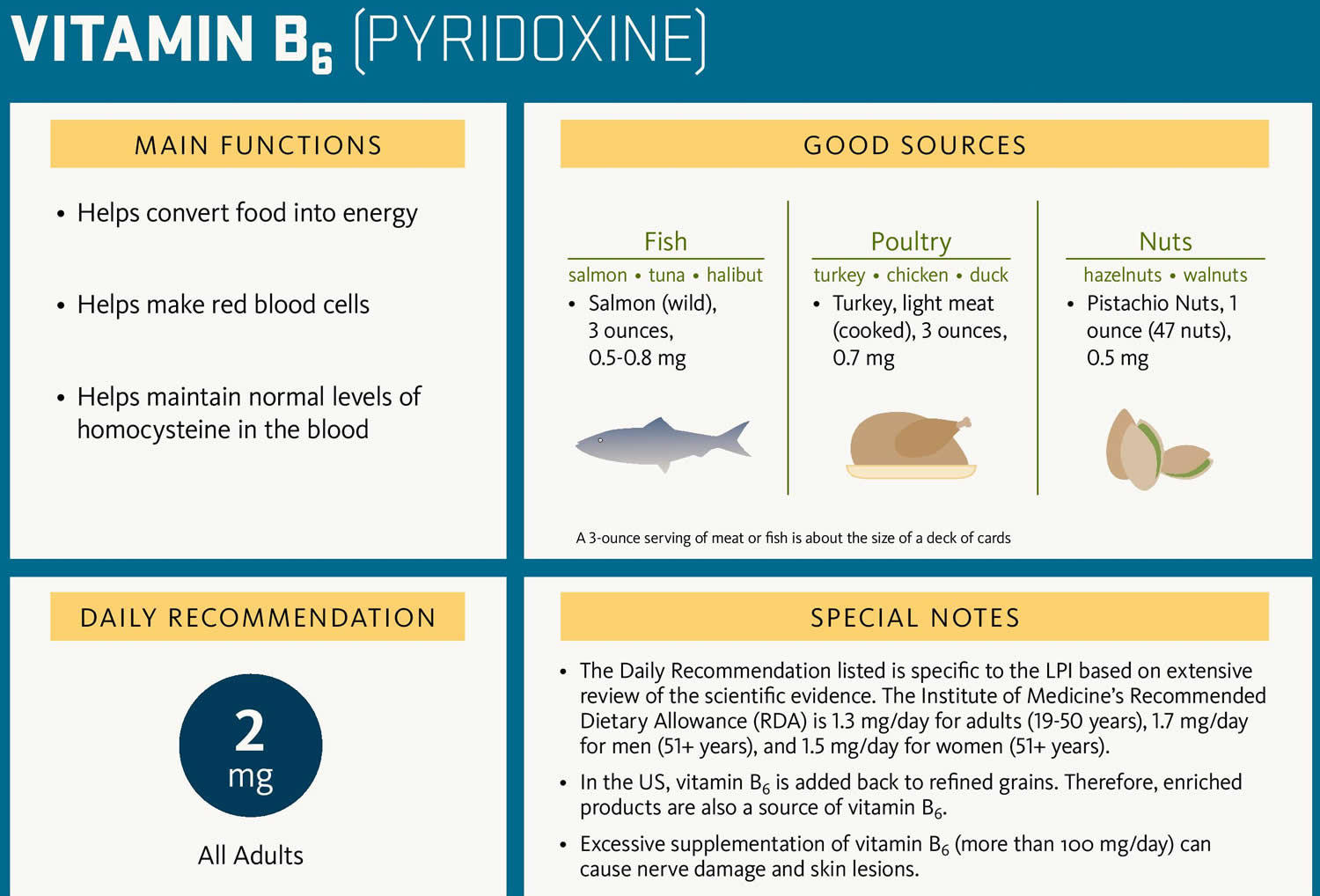
Vitamin B6 must be obtained from the diet because humans cannot synthesize it 29. Vitamin B6 is a vitamin that is naturally present in many foods. You can get recommended amounts of vitamin B6 by eating a variety of foods, including the following 18:
- Poultry, fish, and organ meats, all rich in vitamin B6.
- Potatoes and other starchy vegetables, which are some of the major sources of vitamin B6 for Americans.
- Fruit (other than citrus), which are also among the major sources of vitamin B6 for Americans.
Your body needs vitamin B6 for more than 100 enzyme reactions, mostly concerned with protein metabolism 22. Vitamin B6 is also involved in brain development during pregnancy and infancy as well as immune function 18. Both pyridoxal 5’ phosphate (PLP) and pyridoxamine 5’ phosphate (PMP) are involved in amino acid metabolism, and pyridoxal 5’ phosphate (PLP) is also involved in the metabolism of one-carbon units, carbohydrates, and lipids 21. Vitamin B6 also plays a role in cognitive development through the biosynthesis of neurotransmitters and in maintaining normal levels of homocysteine, an amino acid in the blood 21. Vitamin B6 is involved in gluconeogenesis (metabolic pathway that results in the generation of glucose or sugar from certain non-carbohydrate breakdown products of lipids (fats) or proteins) and glycogenolysis (metabolic pathway in which glycogen breaks down into glucose or sugar), immune function (for example, it promotes lymphocyte and interleukin-2 production), and hemoglobin formation 21.
Your body absorbs vitamin B6 in the jejunum, the second part of your small intestine. Phosphorylated forms of vitamin B6 are dephosphorylated, and the pool of free vitamin B6 is absorbed by passive diffusion 2. In fruit and vegetables, vitamin B6 is present principally as pyridoxine and its phosphate and glucoside 30. In meat and fish, vitamin B6 is mainly present as pyridoxal 5’ phosphate (PLP) and pyridoxamine 5’ phosphate (PMP) 30. Synthesis of vitamin B6 by the gut microbiota (microorganisms, including bacteria, archaea, fungi, and viruses, that live in the digestive tracts of humans) can make a significant contribution to your vitamin B6 intake and may explain why dietary vitamin B6 deficiency is rare 31. Vitamin B6 deficiency or pyridoxine deficiency can occur in the first year of life when the gut flora is not fully established 30; in the 1950s, infants fed a milk formula that had been overheated during production developed seizures due to vitamin B6 deficiency (pyridoxine deficiency) 32.
Figure 1. Vitamin B6 chemical structures
What does Vitamin B6 do?
Vitamin B6 includes a group of closely related compounds: pyridoxine, pyridoxal, and pyridoxamine and pyridoxamine 5’ phosphate (PMP) with pyridoxal 5’ phosphate (PLP) being the only active vitamin B6 vitamer that acts as a cofactor involved in over 100 enzymes that catalyze essential chemical reactions in the human body, a role that is enabled by its reactive aldehyde group 34. Your body needs vitamin B6 for more than 100 enzyme reactions, mostly concerned with protein metabolism 22. Vitamin B6 is also involved in brain development during pregnancy and infancy as well as immune function 18. Both pyridoxal 5’ phosphate (PLP) and pyridoxamine 5’ phosphate (PMP) are involved in amino acid metabolism, and pyridoxal 5’ phosphate (PLP) is also involved in the metabolism of one-carbon units, carbohydrates, and lipids 21. Vitamin B6 also plays a role in cognitive development through the biosynthesis of neurotransmitters and in maintaining normal levels of homocysteine, an amino acid in the blood 21. Vitamin B6 is involved in gluconeogenesis (metabolic pathway that results in the generation of glucose or sugar from certain non-carbohydrate breakdown products of lipids (fats) or proteins) and glycogenolysis (metabolic pathway in which glycogen breaks down into glucose or sugar), immune function (for example, it promotes lymphocyte and interleukin-2 production), and hemoglobin formation 21.
Pyridoxal 5’ phosphate (PLP) dependent enzymes have been classified into five structural classes known as Fold Type 1-5 35:
- Fold Type 1 – aspartate aminotransferase family
- Fold Type 2 – tryptophan synthase family
- Fold Type 3 – alanine racemase family
- Fold Type 4 – D-amino acid aminotransferase family
- Fold Type 5 – glycogen phosphorylase family
The many biochemical reactions catalyzed by PLP-dependent enzymes are involved in essential biological processes, such as hemoglobin and amino acid biosynthesis, as well as fatty acid metabolism. Of note, PLP also functions as a coenzyme for glycogen phosphorylase, an enzyme that catalyzes the release of glucose from stored glycogen 29. Much of the PLP in the human body is found in muscle bound to glycogen phosphorylase. PLP is also a coenzyme for reactions that generate glucose from amino acids, a process known as gluconeogenesis 36.
Nervous system function
In the brain, the pyridoxal 5’ phosphate (PLP)-dependent enzyme aromatic L-amino acid decarboxylase catalyzes the synthesis of two major neurotransmitters: serotonin from the amino acid tryptophan and dopamine from L-3,4-dihydroxyphenylalanine (L-Dopa) 29. Other neurotransmitters, including glycine, D-serine, glutamate, histamine, and γ-aminobutyric acid (GABA), are also synthesized in reactions catalyzed by pyridoxal 5’ phosphate (PLP)-dependent enzymes 37.
Hemoglobin synthesis and function
Pyridoxal 5’ phosphate (PLP) functions as a coenzyme of 5-aminolevulinic acid synthase, which is involved in the synthesis of heme, an iron-containing component of hemoglobin 29. Hemoglobin is found in red blood cells and is critical to their ability to transport oxygen throughout the body. Both pyridoxal and pyridoxal 5’ phosphate (PLP) are able to bind to the hemoglobin molecule and affect its ability to pick up and release oxygen. However, the impact of this on normal oxygen delivery to tissues is not known 36, 38. Vitamin B6 deficiency may impair hemoglobin synthesis and lead to microcytic anemia 26.
Tryptophan metabolism
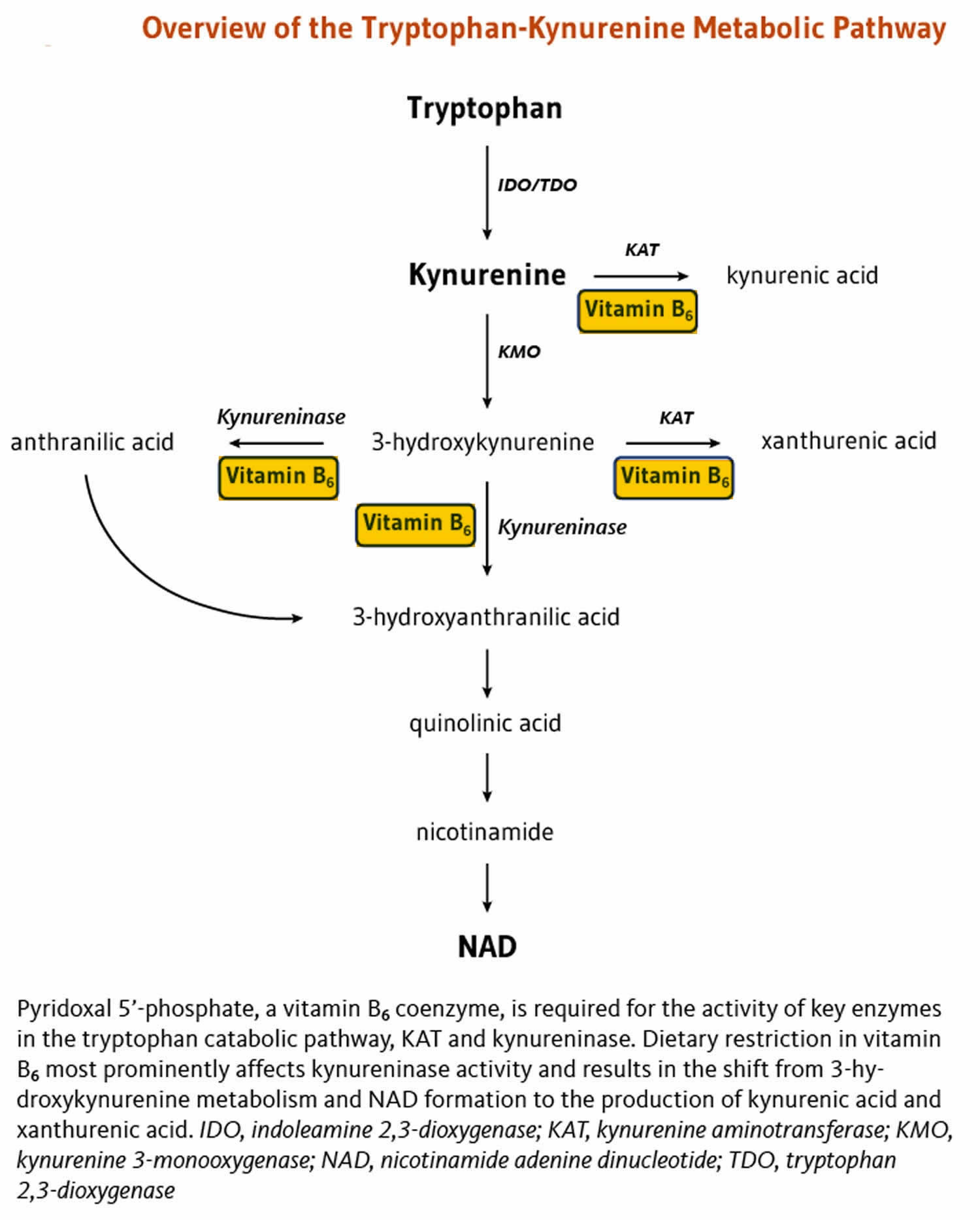
Deficiency in vitamin B3, Niacin, is easily prevented by adequate dietary intakes. The dietary requirement for niacin (vitamin B3) and the niacin coenzyme, nicotinamide adenine dinucleotide (NAD), can be also met, though to a fairly limited extent, by the catabolism of the essential amino acid tryptophan in the tryptophan-kynurenine pathway (Figure 2). Key reactions in the tryptophan-kynurenine metabolic pathway are pyridoxal 5’ phosphate (PLP)-dependent; in particular, pyridoxal 5’ phosphate (PLP) is the cofactor for the enzyme kynureninase, which catalyzes the conversion of 3-hydroxykynurenine to 3-hydroxyanthranilic acid 29. A reduction in PLP availability appears to primarily affect kynureninase activity, limiting NAD production and leading to higher concentrations of kynurenine, 3-hydroxykynurenine, and xanthurenic acid in blood and urine (Figure 2) 39. Thus, while dietary vitamin B6 restriction impairs nicotinamide adenine dinucleotide (NAD) synthesis from tryptophan, adequate PLP levels help maintain NAD formation from tryptophan 40. The effect of vitamin B6 inadequacy on immune activation and inflammation may be partly related to the role of PLP in the tryptophan-kynurenine metabolism 29.
Figure 2. Tryptophan-kynurenine pathway
Hormone function
Steroid hormones, such as estrogen and testosterone, exert their effects in the body by binding to steroid hormone receptors in the nucleus of target cells. The nuclear receptors themselves bind to specific regulatory sequences in DNA and alter the transcription of target genes. Experimental studies have uncovered a mechanism by which PLP may affect the activity of steroid receptors and decrease their effects on gene expression. It was found that PLP could interact with RIP140/NRIP1, a repressor of nuclear receptors known for its role in reproductive biology 41. Yet, additional research is needed to confirm that this interaction can enhance RIP140/NRIP1 repressive activity on steroid receptor-mediated gene expression. If the activity of steroid receptors for estrogen, progesterone, testosterone, or other steroid hormones can be inhibited by PLP, it is possible that vitamin B6 status may influence one’s risk of developing diseases driven by steroid hormones, such as breast and prostate cancers 36.
Nucleic acid synthesis
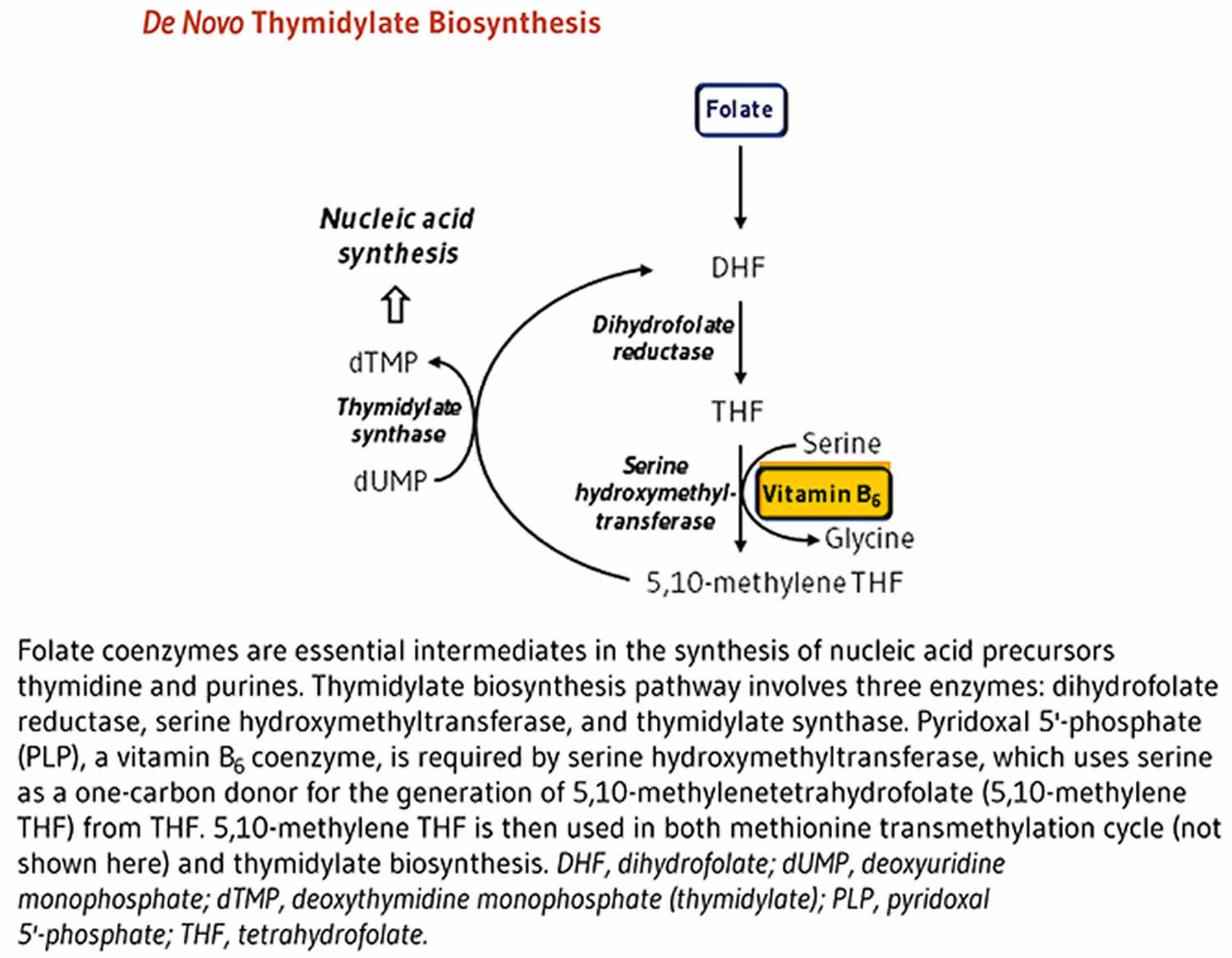
The synthesis of nucleic acids from precursors thymidine and purines is dependent on folate coenzymes. The de novo thymidylate (dTMP) biosynthesis pathway involves three enzymes: dihydrofolate reductase (DHFR), serine hydroxymethyltransferase (SHMT), and thymidylate synthase (TYMS) (Figure 3) 29. PLP serves as a coenzyme for serine hydroxymethyltransferase (SHMT), which catalyzes the simultaneous conversions of serine to glycine and tetrahydrofolate (THF) to 5,10-methylene THF 29. The latter molecule is the one-carbon donor for the generation of dTMP from deoxyuridine monophosphate (dUMP) by thymidylate synthase (TYMS) 29.
Figure 3. Vitamin B6 in nucleic acid synthesis
How much vitamin B6 do you need?
The amount of vitamin B6 you need depends on your age. Average daily recommended amounts are listed below in milligrams (mg). Intake recommendations for vitamin B6 and other nutrients are provided in the Dietary Reference Intakes (DRIs) developed by the Institute of Medicine 5. Dietary Reference Intake (DRI) is the general term for a set of reference values used for planning and assessing nutrient intakes of healthy people. These values, which vary by age and gender, include:
- Recommended Dietary Allowance (RDA): Average daily level of intake sufficient to meet the nutrient requirements of nearly all (97%–98%) healthy individuals; often used to plan nutritionally adequate diets for individuals.
- Adequate Intake (AI): Intake at this level is assumed to ensure nutritional adequacy; established when evidence is insufficient to develop an RDA.
- Estimated Average Requirement (EAR): Average daily level of intake estimated to meet the requirements of 50% of healthy individuals; usually used to assess the nutrient intakes of groups of people and to plan nutritionally adequate diets for them; can also be used to assess the nutrient intakes of individuals.
- Tolerable Upper Intake Level (UL): Maximum daily intake unlikely to cause adverse health effects.
Table 1 lists the current Recommended Dietary Allowances (RDAs) for vitamin B6 5. For infants from birth to 12 months, the Institute of Medicine Food and Nutritional Board established an Adequate Intake (AI) for vitamin B6 that is equivalent to the mean intake of vitamin B6 in healthy, breastfed infants.
The Food and Nutrition Board has established Tolerable Upper Intake Level (the maximum daily intake unlikely to cause adverse health effects) for vitamin B6 that apply to both food and supplement intakes (Table 2) 5. The Food and Nutrition Board noted that although several reports show sensory neuropathy occurring at doses lower than 500 mg/day, studies in patients treated with vitamin B6 (average dose of 200 mg/day) for up to 5 years found no evidence of this effect 5. Based on limitations in the data on potential harms from long-term use, the Food and Nutrition Board halved the dose used in these studies to establish a Tolerable Upper Intake Level (UL) of 100 mg/day for adults. The Tolerable Upper Intake Level (ULs) are lower for children and adolescents based on body size. The Tolerable Upper Intake Level (ULs) do not apply to individuals receiving vitamin B6 for medical treatment, but such individuals should be under the care of a physician.
Table 1. Recommended Dietary Allowances (RDAs) for Vitamin B6
| Life Stage | Recommended Amount |
|---|---|
| Birth to 6 months* | 0.1 mg |
| Infants 7–12 months* | 0.3 mg |
| Children 1–3 years | 0.5 mg |
| Children 4–8 years | 0.6 mg |
| Children 9–13 years | 1.0 mg |
| Teens 14–18 years (boys) | 1.3 mg |
| Teens 14–18 years (girls) | 1.2 mg |
| Adults 19–50 years | 1.3 mg |
| Adults 51+ years (men) | 1.7 mg |
| Adults 51+ years (women) | 1.5 mg |
| Pregnant teens and women | 1.9 mg |
| Breastfeeding teens and women | 2.0 mg |
Footnote: *Adequate Intake (AI) = Intake at this level is assumed to ensure nutritional adequacy; established when evidence is insufficient to develop an RDA.
[Source 23 ]Table 2. Tolerable Upper Intake Levels (ULs) for Vitamin B6
| Age | Male | Female | Pregnancy | Lactation |
|---|---|---|---|---|
| Birth to 6 months | Not possible to establish* | Not possible to establish* | ||
| 7–12 months | Not possible to establish* | Not possible to establish* | ||
| 1–3 years | 30 mg | 30 mg | ||
| 4–8 years | 40 mg | 40 mg | ||
| 9–13 years | 60 mg | 60 mg | ||
| 14–18 years | 80 mg | 80 mg | 80 mg | 80 mg |
| 19+ years | 100 mg | 100 mg | 100 mg | 100 mg |
Footnotes: *Breast milk, formula, and food should be the only sources of vitamin B6 for infants.
[Source 23 ]Vitamin B6 Supplements
Vitamin B6 is available in multivitamins, in supplements containing other B complex vitamins, and as a stand-alone supplement that contain only vitamin B6 42. The most common vitamin B6 vitamer in supplements is pyridoxine (in the form of pyridoxine hydrochloride [HCl]), although some supplements contain PLP 23.
Vitamin B6 supplements are available in oral capsules or tablets (including sublingual and chewable tablets) and liquids. Absorption of vitamin B6 from supplements is similar to that from food sources and does not differ substantially among the various forms of supplements 5. Although the body absorbs large pharmacological doses of vitamin B6 well, it quickly eliminates most of the vitamin in the urine 43.
About 28% to 36% of the general population uses supplements containing vitamin B6 20, 44. Adults aged 51 years or older and children younger than 9 are more likely than members of other age groups to take supplements containing vitamin B6 23.
Can vitamin B6 be harmful?
High intakes of vitamin B6 from food sources have not been reported to cause adverse effects 22. People almost never get too much vitamin B6 from food. But taking high levels of vitamin B6 from supplements for a year or longer can cause severe nerve damage, leading people to lose control of their bodily movements. The symptoms usually stop when they stop taking the supplements. Other symptoms of too much vitamin B6 include painful, unsightly skin patches, extreme sensitivity to sunlight, nausea, and heartburn.
The ingestion of megadoses (> 500 mg/day) of vitamin B6 or pyridoxine (eg, taken to treat carpal tunnel syndrome or premenstrual syndrome although efficacy is unproven) may cause painful neurological symptoms known as sensory neuropathy with deficits in a stocking-glove distribution, including progressive sensory ataxia and severe impairment of position and vibration senses 45. Symptoms include pain and numbness of the extremities and in severe cases, difficulty walking 29. Senses of touch, temperature, and pain are less affected. Motor and central nervous systems are usually intact.
Sensory neuropathy typically develops at doses of pyridoxine in excess of 1,000 mg per day. However, there have been a few case reports of individuals who developed sensory neuropathies at doses of less than 500 mg daily over a period of months 29. Yet, none of the studies in which an objective neurological examination was performed reported evidence of sensory nerve damage at intakes below 200 mg pyridoxine daily 46.
However, chronic administration of 1–6 g oral pyridoxine per day for 12–40 months can cause severe and progressive sensory neuropathy characterized by ataxia (loss of control of bodily movements) 47, 48, 49, 50, 46. Symptom severity appears to be dose dependent, and the symptoms usually stop if the patient discontinues the pyridoxine supplements as soon as the neurologic symptoms appear. Other effects of excessive vitamin B6 intakes include painful, disfiguring dermatological lesions; photosensitivity; and gastrointestinal symptoms, such as nausea and heartburn 5, 48, 49, 2.
The scientific literature includes isolated case reports of congenital defects in the infants of individuals who took pyridoxine supplements during the first half of pregnancy 23. However, a more recent observational study found no association between pyridoxine supplementation (mean dose 132.3 ± 74 mg/day) in pregnant people starting at 7 weeks gestation and continuing for 9 ± 4.2 weeks and teratogenic effects in their infants 51.
To prevent sensory neuropathy in virtually all individuals, the Food and Nutrition Board of the Institute of Medicine set the tolerable upper intake level (UL) for pyridoxine at 100 mg/day for adults (Table 2) 22. Because placebo-controlled studies have generally failed to show therapeutic benefits of high doses of pyridoxine, there is little reason to exceed the tolerable upper intake level (UL) of 100 mg/day. The Tolerable Upper Intake Level (ULs) do not apply to individuals receiving vitamin B6 for medical treatment, but such individuals should be under the care of a physician.
- Diagnosis of vitamin B6 toxicity is clinical.
- Treatment of vitamin B6 toxicity is to stop taking vitamin B6. Recovery is slow and, for some patients, incomplete.
What foods provide vitamin B6?
Vitamin B6 is found naturally in many foods and is added to other foods. You can get recommended amounts of vitamin B6 by eating a variety of foods, including the following 18:
- Poultry, fish, and organ meats, all rich in vitamin B6.
- Potatoes and other starchy vegetables, which are some of the major sources of vitamin B6 for Americans.
- Fruit (other than citrus), which are also among the major sources of vitamin B6 for Americans.
Vitamin B6 is found in a wide variety of foods 5, 21, 52 and is added to other foods. The richest sources of vitamin B6 include fish, beef liver and other organ meats, potatoes and other starchy vegetables, and fruit (other than citrus).
In the United States, adults obtain most of their dietary vitamin B6 from fortified cereals, beef, poultry, starchy vegetables, and some non-citrus fruits 5, 21, 53. About 75% of vitamin B6 from a mixed diet is bioavailable 5.
The U.S. Department of Agriculture’s (USDA’s) FoodData website (https://fdc.nal.usda.gov) lists the nutrient content of many foods and provides a comprehensive list of foods containing vitamin B6 arranged by nutrient content (https://ods.od.nih.gov/pubs/usdandb/VitaminB6-Content.pdf) and by food name (https://ods.od.nih.gov/pubs/usdandb/VitaminB6-Food.pdf).
Table 3. Food Sources of Vitamin B6
| Food | Milligrams (mg) per serving | Percent Daily Value (DV)* |
|---|---|---|
| Chickpeas, canned, 1 cup | 1.1 | 65 |
| Beef liver, pan fried, 3 ounces | 0.9 | 53 |
| Tuna, yellowfin, fresh, cooked, 3 ounces | 0.9 | 53 |
| Salmon, sockeye, cooked, 3 ounces | 0.6 | 35 |
| Chicken breast, roasted, 3 ounces | 0.5 | 29 |
| Breakfast cereals, fortified with 25% of the DV for vitamin B6 | 0.4 | 25 |
| Potatoes, boiled, 1 cup | 0.4 | 25 |
| Turkey, meat only, roasted, 3 ounces | 0.4 | 25 |
| Banana, 1 medium | 0.4 | 25 |
| Marinara (spaghetti) sauce, ready to serve, 1 cup | 0.4 | 25 |
| Ground beef, patty, 85% lean, broiled, 3 ounces | 0.3 | 18 |
| Waffles, plain, ready to heat, toasted, 1 waffle | 0.3 | 18 |
| Bulgur, cooked, 1 cup | 0.2 | 12 |
| Cottage cheese, 1% low-fat, 1 cup | 0.2 | 12 |
| Squash, winter, baked, ½ cup | 0.2 | 12 |
| Rice, white, long-grain, enriched, cooked, 1 cup | 0.1 | 6 |
| Nuts, mixed, dry-roasted, 1 ounce | 0.1 | 6 |
| Raisins, seedless, ½ cup | 0.1 | 6 |
| Onions, chopped, ½ cup | 0.1 | 6 |
| Spinach, frozen, chopped, boiled, ½ cup | 0.1 | 6 |
| Tofu, raw, firm, prepared with calcium sulfate, ½ cup | 0.1 | 6 |
| Watermelon, raw, 1 cup | 0.1 | 6 |
Footnote: *DV = Daily Value. The U.S. Food and Drug Administration (FDA) developed Daily Values (DVs) to help consumers compare the nutrient contents of foods and dietary supplements within the context of a total diet. The Daily Value (DV) for vitamin B6 is 1.7 mg for adults and children age 4 years and older 54. FDA does not require food labels to list vitamin B6 content unless vitamin B6 has been added to the food. Foods providing 20% or more of the DV are considered to be high sources of a nutrient, but foods providing lower percentages of the DV also contribute to a healthful diet.
[Source 23 ]Vitamin B6 deficiency causes
Dietary vitamin B6 deficiency, though rare, can develop because extensive processing can deplete foods of vitamin B6. In the United States and other western cultures, vitamin B6 deficiency is rare due to adequate diets, including vitamin B6 sources from fish, organ meats, poultry, potatoes, grains, legumes, and non-citrus fruits.
Isolated B6 deficiency is rare and is usually found in association with other B vitamin deficiencies such as folic acid and B12.
Secondary vitamin B6 deficiency or pyridoxine deficiency most often results from 55, 1:
- Vitamin B6 or Pyridoxine intake is reduced in cases of severe malnutrition.
- Protein-energy malnutrition
- Malabsorption states such as celiac disease, inflammatory bowel disease (Crohn’s disease, and ulcerative colitis), and post weight loss surgery
- Vitamin B6 or Pyridoxine absorption is reduced in elderly persons and in patients with intestinal disease or who have undergone surgery.
- Chronic alcohol dependence
- Autoimmune diseases, such as rheumatoid arthritis, have increased breakdown and metabolic requirements of vitamin B6, resulting in higher demand for dietary supplementation of vitamin B6.
- Pyridoxine clearance is enhanced by liver disorders, such as hepatitis, and by several medications.
- Pyridoxine breakdown is enhanced in conditions associated with increased alkaline phosphatase levels.
- Use of pyridoxine-inactivating drugs (eg, anticonvulsants, isoniazid, cycloserine, levodopa, hydralazine, corticosteroids, penicillamine) 56, 57, 58, 59
- Excessive loss during hemodialysis and the patient who have undergone kidney transplants are more at risk of vitamin B6 deficiency. Patients with chronic renal failure, especially those receiving hemodialysis or peritoneal dialysis, have low plasma levels of vitamin B6 and usually respond well to oral or parenteral vitamin B6 therapy 60, 61.
- Pregnancy – Pregnancy can cause a pyridoxine-deficient state; however, a change in the ratio of plasma PLP to pyridoxal does occur, thereby falsely suggesting a deficiency state if only serum PLP is measured.
Rarely, secondary deficiency results from increased metabolic demand (eg, in hyperthyroidism).
Rare inborn errors of metabolism can affect pyridoxine metabolism.
Risk factors for developing vitamin B6 deficiency
Several factors contribute to an increased risk for vitamin B6 deficiency or pyridoxine deficiency 62:
- Advanced age
- Medical conditions that may increase the risk for vitamin B6 deficiency or pyridoxine deficiency include the following:
- Severe malnutrition
- Sickle cell disease
- Inflammatory conditions 63, 64
- Rheumatoid arthritis 63
- Hospitalization
- Celiac disease
- Hepatitis and extrahepatic biliary obstruction
- Hepatocellular carcinoma
- Chronic renal failure
- Kidney transplant 65
- Hyperoxaluria types 1 and 2
- High serum alkaline phosphatase level, such as in cirrhosis and tissue injury
- Catabolic state
- Medical procedures that may increase the risk for vitamin B6 deficiency or pyridoxine deficiency include the following:
- Hemodialysis
- Peritoneal dialysis
- Phototherapy for hyperbilirubinemia
- Medications that may increase the risk for vitamin B6 deficiency or pyridoxine deficiency include the following:
- Cycloserine
- Hydralazine
- Isoniazid
- D-penicillamine
- Pyrazinamide
- Social-behavioral conditions that may increase the risk for vitamin B6 deficiency or pyridoxine deficiency include the following:
- Excessive alcohol ingestion (except for pyridoxine-supplemented beer)
- Tobacco smoking
- Severe malnutrition
- Other risk factors that may increase the risk for pyridoxine deficiency include the following:
Groups at Risk of Vitamin B6 deficiency
Frank vitamin B6 deficiencies are relatively rare in the United States but some individuals might have marginal vitamin B6 status 2. The following groups are among those most likely to have inadequate intakes of vitamin B6.
Individuals with impaired kidney function
People with poor kidney function, including those with end-stage renal disease (also called end-stage kidney disease or kidney failure) and chronic renal insufficiency, often have low vitamin B6 concentrations 21. Plasma pyridoxal 5’ phosphate (PLP) concentrations are also low in patients receiving maintenance kidney dialysis or intermittent peritoneal dialysis, as well as those who have undergone a kidney transplant, perhaps due to increased metabolic clearance of pyridoxal 5’ phosphate (PLP) 69. Patients with kidney disease often show clinical symptoms similar to those of people with vitamin B6 deficiency 69.
Individuals with Autoimmune Disorders
People with rheumatoid arthritis often have low vitamin B6 concentrations, and vitamin B6 concentrations tend to decrease with increased disease severity 21. These low vitamin B6 levels are due to the inflammation caused by the disease and, in turn, increase the inflammation associated with the disease. Although vitamin B6 supplements can normalize vitamin B6 concentrations in patients with rheumatoid arthritis, they do not suppress the production of inflammatory cytokines or decrease levels of inflammatory markers 21, 70.
Patients with celiac disease, Crohn’s disease, ulcerative colitis, inflammatory bowel disease, and other malabsorptive autoimmune disorders tend to have low plasma pyridoxal 5’ phosphate (PLP) concentrations 21. The mechanisms for this effect are not known. However, celiac disease is associated with lower pyridoxine absorption, and low PLP concentrations in inflammatory bowel disease could be due to the inflammatory response 21.
People with Alcohol Dependence
Plasma pyridoxal 5’ phosphate (PLP) concentrations tend to be very low in people with alcohol dependence 5. Alcohol produces acetaldehyde, which decreases net pyridoxal 5’ phosphate (PLP) formation by cells and competes with Pyridoxal 5’ phosphate in protein binding 5. As a result, the PLP in cells might be more susceptible to hydrolysis by membrane-bound phosphatase. People with alcohol dependence might benefit from pyridoxine supplementation 21.
Vitamin B6 deficiency prevention
The human body cannot store vitamin B6, and therefore a daily source is required. However, in the United States isolated vitamin B6 deficiency is rare, because most children, adolescents, and adults in the United States consume the recommended amounts of vitamin B6, according to an analysis of data from the 2003–2004 National Health and Nutrition Examination Survey 20. The average vitamin B6 intake is about 1.5 mg/day in women and 2 mg/day in men 5.
Vitamin B6 (Pyridoxine) supplementation is indicated in cases of vitamin B6 deficiency, which may be due to poor kidney function, autoimmune diseases, increased alcohol intake (chronic alcohol use), or in people who take these medications: isoniazid, cycloserine, valproic acid, phenytoin, carbamazepine, primidone, hydralazine, and theophylline 71, 72, 73, 74, 37, 75, 76.
Vitamin B6 deficiency is usually found in association with other B vitamin deficiencies such as folic acid and B12. So these B vitamin supplements are also needed.
There is evidence to suggest reduced bioavailability 77 as well as digestibility 78 of vitamin B6 from plant foods compared to animal foods. This may be important to those who favor a plant-based diet exclusively (i.e., vegans and vegetarians) 79. These individuals may need vitamin B6 supplementation. The major vitamin B6 supplement in multivitamins is pyridoxine hydrochloride.
Prophylactic administration of vitamin B6 (Pyridoxine) should be provided when a patient is using certain medications, such as isoniazid (30-450 mg/day, which may be based gram for gram) and penicillamine (100 mg/day) 80.
Estrogen-induced reduction in tryptophan metabolism may require vitamin B6 (Pyridoxine) supplementation of 20-25 mg/day 80.
Vitamin B6 deficiency symptoms
Signs and symptoms of vitamin B6 deficiency or pyridoxine deficiency include the following 81, 82, 83 :
- General symptoms – Weakness, dizziness
- Oral signs and symptoms – Glossitis (inflammation of the tongue), angular cheilitis (scaling on the lips and cracks at the corners of the mouth)
- Dermatologic signs and symptoms – Seborrheic dermatitis
- Neurologic symptoms in adults – Distal limb numbness and weakness, impaired vibration and proprioception, sensory ataxia, generalized seizures
- Neurologic symptoms in neonates and young infants – Hypotonia; irritability; restlessness; focal, bilateral motor, or myoclonic seizures; infantile spasms
Vitamin B6 deficiency in adults causes peripheral neuropathy and a pellagra-like syndrome, with seborrheic dermatitis, glossitis, and angular cheilitis. Additional clinical findings of vitamin B6 deficiency may include mental status changes, depression, confusion, EEG abnormalities, seizures and normocytic, microcytic, or sideroblastic anemia 45.
Rarely, vitamin B6 deficiency may present with seizures in infants 84, 85. Seizures, particularly in infants, may be refractory to treatment with anticonvulsants.
Current studies are evaluating the role of B6 deficiency in heart disease, cancer, attention deficit hyperactivity disorders (ADHD) and cognitive decline as medical conditions that may respond to supplementation 3, 29, 23. To date, there is no clear evidence to support vitamin B6 supplement use beyond the normal dietary intake. However, some studies indicate a reduction of symptoms in the premenstrual syndrome (PMS) with supplementation of vitamin B6, particularly a decrease in moodiness, irritability, and forgetfulness 29, 23. The American College of Obstetrics and Gynecology recommend vitamin B6 supplementation (1.9 mg per day) for hyperemesis gravidarum (severe nausea and vomiting during pregnancy) 86.
Figure 4. Glossitis

Figure 5. Angular cheilitis

Figure 6. Seborrheic dermatitis

Vitamin B6 deficiency diagnosis
Diagnosis of vitamin B6 deficiency is usually clinical. There is no single accepted laboratory test of vitamin B6 status; measurement of serum pyridoxal phosphate is most common. Plasma Pyridoxal 5’ phosphate (PLP) of less than 20 nmol/L is considered vitamin B6 deficiency 24.
Early or subclinical vitamin B6 deficiency may have vague or fleeting symptoms; however, new-onset sensory polyneuropathy, altered mental status, dermatitis in adults, or seizures in infancy should raise clinical suspicion of a clinically significant B6 deficiency 1.
Vitamin B6 deficiency should be considered in 1:
- Any infant who has seizures
- Any patient who has seizures refractory to treatment with anticonvulsants
- Any patient with deficiencies of other B vitamins, particularly in patients with alcoholism or protein-energy undernutrition
Testing for vitamin B6 can be difficult in real-time in many clinical scenarios. Direct biomarkers B6 vitamers in serum, plasma, red blood cell, and urine are used. Serum measurement of the active vitamin pyridoxal 5′-phosphate (PLP) form is available in some clinical settings. However, the assay is not widely available or timely 1. Serum or urinary 4-Pyridoxic acid (4PA) is the end product of vitamin B6 catabolism, is an indicator of recent vitamin B6 intake. A clinical alternative is an indirect measurement technique of vitamin B6, which includes measuring urinary excretion of xanthurenic acid (an amino acid catabolite of tryptophan) following a measured bolus of tryptophan 1. Increased levels of xanthurenic acid may indicate inadequate active B6 for the formation of the amino acid tryptophan 87. Urinary excretion of xanthurenic acid is usually less than 65 mmol/day following a 2 g tryptophan load. Excretion of xanthurenic acid above this threshold suggests abnormal tryptophan metabolism due to vitamin B6 insufficiency.
Red blood cell transaminase activity, with and without pyridoxal 5′-phosphate (PLP) added, has been used as a functional test of pyridoxine status and maybe a more accurate reflection of vitamin B6 status in critically ill patients 88. Urinary 4-pyridoxic acid excretion greater than 3.0 mmol/day can be used as an indicator of adequate short-term vitamin B6 status (this is often reported as “urinary pyridoxic acid”) 1.
Vitamin B6 deficiency treatment
In vitamin B6-deficient states and illnesses, treatment dosage is variable and depends on the severity of symptoms 1. Vitamin B6 (Pyridoxine) is available therapeutically in both oral and parenteral formulations. Neonates with vitamin B6 deficiency seizures may require 10 to 100 mg intravenous (IV) Pyridoxine for effective treatment of active seizures. Less serious or less acute presentations can be supplemented with Pyridoxine doses ranging from 25 mg to 600 mg per day orally depending on symptom complex.
Levels of pyridoxine hydrochloride supplementation in various medical conditions are as follows 89:
- Cirrhosis – 50 mg/d
- Hemodialysis – 5-50 mg/d
- Peritoneal dialysis – 2.5-5 mg/d
- Chronic renal failure – 2.5-5 mg/d
- Sideroblastic anemia – 50-600 mg/d
- Pyridoxine-dependent seizures – 100 mg/d
- Homocystinuria – 100-500 mg/d
- Homocystinemia – 100-500 mg/d
- Gyromitra poisoning – 25 mg/kg IV
At one time, pyridoxine supplementation was given to people with sickle cell anemia; however, no changes were noted in these patients’ hematologic indexes or disease activity.
Importantly, vitamin B6 or Pyridoxine therapy can be life-saving in refractory Isoniazid (a potent antibiotic used in the treatment of tuberculosis) overdose-induced seizures 1. The vitamin B6 (Pyridoxine) dose is equal to the known amount of Isoniazid (INH) ingested or a maximum of 5,000 mg and is dosed 1,000 to 4,000 mg IV as the first dose, then 1,000 mg IM or IV every 30 minutes 90. In ethylene glycol overdose, vitamin B6 is recommended at 50 to 100 mg IV every 6 hours to facilitate shunting the metabolism of ethylene glycol to nontoxic pathways leading to glycine (nontoxic) instead of toxic pathways leading to toxic metabolites such as formate.
Additional, less common uses are in hydralazine overdose, where the recommended dose of vitamin B6 is 25 mg/kg, the first third administered intramuscularly, and the remainder as a 3-hour IV infusion. Gyromitra (mushroom) toxicity treatment is at 25 mg/kg infused IV over 30 min 1.
Hyperemesis gravidarum (severe nausea and vomiting during pregnancy) may respond to vitamin B6 at a dosage of 25 mg orally every 8 hours.
Vitamin B6 deficiency prognosis
If diagnosed appropriately, vitamin B6 deficiency is effectively treated with adequate oral or parenteral vitamin B6 (pyridoxine) supplementation.
Care should be taken when supplementing pyridoxine, because high pyridoxine states can cause peripheral neuropathy characterized by ataxia and burning pain in the feet, beginning approximately 1 month to 3 years following supplementation 91. Although this usually occurs at very high supplementation doses, complications have been reported with doses as low as 50 mg/day 91.
Care should also be taken when prescribing pyridoxine supplementation to postpartum women who are breastfeeding, because high doses of pyridoxine can cause hypocalcaemia (low blood calcium) 91. A cohort study of postmenopausal women found that a high intake of pyridoxine, coupled with a high intake of vitamin B12, is linked to an increased risk of hip fracture. Compared with women who consumed less than 2 mg/d of total pyridoxine, those whose intake was 35 mg/d or higher had an elevated fracture risk 92.
Injecting pyridoxine into an infant or neonate can cause a precipitous decrease in blood pressure.
Pyridoxine has the highest adverse outcome per toxic exposure for any vitamin, although no deaths have been reported.
References- Brown MJ, Ameer MA, Beier K. Vitamin B6 Deficiency. [Updated 2022 Jul 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470579
- McCormick D. Vitamin B6. In: Bowman B, Russell R, eds. Present Knowledge in Nutrition. 9th ed. Washington, DC: International Life Sciences Institute; 2006.
- Altun H, Şahin N, Belge Kurutaş E, Güngör O. Homocysteine, Pyridoxine, Folate and Vitamin B12 Levels in Children with Attention Deficit Hyperactivity Disorder. Psychiatr Danub. 2018 Sep;30(3):310-316. doi: 10.24869/psyd.2018.310
- Bailey R.L., West K.P., Jr., Black R.E. The epidemiology of global micronutrient deficiencies. Ann. Nutr. Metab. 2015;66(Suppl. 2):22–33. doi: 10.1159/000371618
- Institute of Medicine. Food and Nutrition Board. Dietary Reference Intakes: Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline. Washington, DC: National Academy Press; 1998. https://www.nap.edu/catalog/6015/dietary-reference-intakes-for-thiamin-riboflavin-niacin-vitamin-b6-folate-vitamin-b12-pantothenic-acid-biotin-and-choline
- Sawhney A, Singhal S, Patel R. Isolated Pyridoxine Deficiency Presenting as Peripheral Neuropathy Post-chemotherapy. Cureus. 2022 Jul 10;14(7):e26725. doi: 10.7759/cureus.26725
- Wang HS, Kuo MF. Vitamin B6 related epilepsy during childhood. Chang Gung Med J. 2007 Sep-Oct;30(5):396-401. http://cgmj.cgu.edu.tw/3005/300502.pdf
- Mayengbam S, Chleilat F, Reimer RA. Dietary Vitamin B6 Deficiency Impairs Gut Microbiota and Host and Microbial Metabolites in Rats. Biomedicines. 2020 Nov 2;8(11):469. doi: 10.3390/biomedicines8110469
- Hellmann H., Mooney S. Vitamin B6: A molecule for human health? Molecules. 2010;15:442–459. doi: 10.3390/molecules15010442
- Matxain J.M., Padro D., Ristila M., Strid A., Eriksson L.A. Evidence of high *OH radical quenching efficiency by vitamin B6. J. Phys. chem. B. 2009;113:9629–9632. doi: 10.1021/jp903023c
- Bird RP. The Emerging Role of Vitamin B6 in Inflammation and Carcinogenesis. Adv Food Nutr Res. 2018;83:151-194. doi: 10.1016/bs.afnr.2017.11.004
- Jung HY, Kim W, Hahn KR, Kwon HJ, Nam SM, Chung JY, Yoon YS, Kim DW, Yoo DY, Hwang IK. Effects of Pyridoxine Deficiency on Hippocampal Function and Its Possible Association with V-Type Proton ATPase Subunit B2 and Heat Shock Cognate Protein 70. Cells. 2020 Apr 25;9(5):1067. doi: 10.3390/cells9051067
- Selhub J, Bagley LC, Miller J, Rosenberg IH. B vitamins, homocysteine, and neurocognitive function in the elderly. Am J Clin Nutr. 2000 Feb;71(2):614S-620S. doi: 10.1093/ajcn/71.2.614s
- Balk EM, Raman G, Tatsioni A, Chung M, Lau J, Rosenberg IH. Vitamin B6, B12, and folic acid supplementation and cognitive function: a systematic review of randomized trials. Arch Intern Med. 2007 Jan 8;167(1):21-30. doi: 10.1001/archinte.167.1.21
- Riggs KM, Spiro A 3rd, Tucker K, Rush D. Relations of vitamin B-12, vitamin B-6, folate, and homocysteine to cognitive performance in the Normative Aging Study. Am J Clin Nutr. 1996 Mar;63(3):306-14. doi: 10.1093/ajcn/63.3.306
- Walden M., Tian L., Ross R.L., Sykora U.M., Byrne D.P., Hesketh E.L., Masandi S.K., Cassel J., George R., Ault J.R., et al. Metabolic control of BRISC-SHMT2 assembly regulates immune signalling. Nature. 2019;570:194–199. doi: 10.1038/s41586-019-1232-1
- Qian B., Shen S., Zhang J., Jing P. Effects of vitamin B6 deficiency on the composition and functional potential of T cell populations. J. Immunol. Res. 2017;2017:2197975. doi: 10.1155/2017/2197975
- Vitamin B6. https://ods.od.nih.gov/factsheets/VitaminB6-Consumer
- Mackey AD, Davis SR, Gregory JF. , III. In: Modern Nutrition in Health and Disease. Shils ME, Shike M, Ross AC, Cabellero B, Cousins RJ, editor. Philadelphia: Lippencott; 2006. Vitamin B6; pp. 452–461.
- Morris MS, Picciano MF, Jacques PF, Selhub J. Plasma pyridoxal 5′-phosphate in the US population: the National Health and Nutrition Examination Survey, 2003-2004. Am J Clin Nutr. 2008 May;87(5):1446-54. doi: 10.1093/ajcn/87.5.1446
- Mackey A, Davis S, Gregory J. Vitamin B6. In: Shils M, Shike M, Ross A, Caballero B, Cousins R, eds. Modern Nutrition in Health and Disease. 10th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2005.
- Institute of Medicine. Food and Nutrition Board. Dietary Reference Intakes: Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline. Washington, DC: National Academy Press; 1998. https://nap.nationalacademies.org/read/6015/chapter/1
- Vitamin B6. https://ods.od.nih.gov/factsheets/VitaminB6-HealthProfessional
- Centers for Disease Control and Prevention . Second National Report on Biochemical Indicators of Diet and Nutrition in the U.S. Population. National Center for Environmental Health; Atlanta, GA, USA: Apr, 2012. https://www.cdc.gov/nutritionreport/pdf/Nutrition_Book_complete508_final.pdf
- Dakshinamurti S, Dakshinamurti K. Vitamin B6. In: Zempleni J, Rucker RB, McCormick DB, Suttie JW, eds. Handbook of Vitamins. 4th ed. New York: CRC Press (Taylor & Fracis Group); 2007:315-359.
- McCormick DB. Vitamin B6. In: Bowman BA, Russell RM, eds. Present Knowledge in Nutrition. Vol. I. Washington, D.C.: International Life Sciences Institute; 2006:269-277.
- Galluzzi L, Vacchelli E, Michels J, Garcia P, Kepp O, Senovilla L, Vitale I, Kroemer G. Effects of vitamin B6 metabolism on oncogenesis, tumor progression and therapeutic responses. Oncogene. 2013 Oct 17;32(42):4995-5004. doi: 10.1038/onc.2012.623
- di Salvo ML, Contestabile R, Safo MK. Vitamin B(6) salvage enzymes: mechanism, structure and regulation. Biochim Biophys Acta. 2011 Nov;1814(11):1597-608. doi: 10.1016/j.bbapap.2010.12.006
- Vitamin B6. https://lpi.oregonstate.edu/mic/vitamins/vitamin-B6
- Wilson, MP, Plecko, B, Mills, PB, Clayton, PT. Disorders affecting vitamin B6 metabolism. J Inherit Metab Dis. 2019; 42: 629– 646. https://doi.org/10.1002/jimd.12060
- Magnúsdóttir S, Ravcheev D, de Crécy-Lagard V, Thiele I. Systematic genome assessment of B-vitamin biosynthesis suggests co-operation among gut microbes. Front Genet. 2015 Apr 20;6:148. doi: 10.3389/fgene.2015.00148
- COURSIN DB. Convulsive seizures in infants with pyridoxine-deficient diet. J Am Med Assoc. 1954 Jan 30;154(5):406-8. doi: 10.1001/jama.1954.02940390030009
- Stach K, Stach W, Augoff K. Vitamin B6 in Health and Disease. Nutrients. 2021 Sep 17;13(9):3229. doi: 10.3390/nu13093229
- Da Silva VR, Russell KA, Gregory JF 3rd. Vitamin B6. In: Erdman JW Jr., Macdonald IA, Zeisel SH. Present Knowldege in Nutrition. 10th ed: Wiley-Blackwell; 2012:307-320.
- Eliot AC, Kirsch JF. Pyridoxal phosphate enzymes: mechanistic, structural, and evolutionary considerations. Annu Rev Biochem. 2004;73:383-415. doi: 10.1146/annurev.biochem.73.011303.074021
- Leklem JE. Vitamin B-6. In: Shils M, Olson JA, Shike M, Ross AC, eds. Modern Nutrition in Health and Disease. 9th ed. Baltimore: Williams & Wilkins; 1999:413-422.
- Clayton PT. B6-responsive disorders: a model of vitamin dependency. J Inherit Metab Dis. 2006 Apr-Jun;29(2-3):317-26. doi: 10.1007/s10545-005-0243-2
- Schnackerz KD, Benesch RE, Kwong S, Benesch R, Helmreich EJ. Specific receptor sites for pyridoxal 5′-phosphate and pyridoxal 5′-deoxymethylenephosphonate at the alpha and beta NH2-terminal regions of hemoglobin. J Biol Chem. 1983 Jan 25;258(2):872-5.
- Rios-Avila L, Nijhout HF, Reed MC, Sitren HS, Gregory JF 3rd. A mathematical model of tryptophan metabolism via the kynurenine pathway provides insights into the effects of vitamin B-6 deficiency, tryptophan loading, and induction of tryptophan 2,3-dioxygenase on tryptophan metabolites. J Nutr. 2013 Sep;143(9):1509-19. doi: 10.3945/jn.113.174599
- Oxenkrug G. Insulin resistance and dysregulation of tryptophan-kynurenine and kynurenine-nicotinamide adenine dinucleotide metabolic pathways. Mol Neurobiol. 2013 Oct;48(2):294-301. doi: 10.1007/s12035-013-8497-4
- Huq MD, Tsai NP, Lin YP, Higgins L, Wei LN. Vitamin B6 conjugation to nuclear corepressor RIP140 and its role in gene regulation. Nat Chem Biol. 2007 Mar;3(3):161-5. doi: 10.1038/nchembio861
- Natural Medicines Comprehensive Database. Vitamin B6. 2011. http://naturaldatabase.therapeuticresearch.com/home.aspx?cs=&s=ND
- Simpson JL, Bailey LB, Pietrzik K, Shane B, Holzgreve W. Micronutrients and women of reproductive potential: required dietary intake and consequences of dietary deficiency or excess. Part I–Folate, Vitamin B12, Vitamin B6. J Matern Fetal Neonatal Med. 2010 Dec;23(12):1323-43. doi: 10.3109/14767051003678234
- Bailey RL, Gahche JJ, Lentino CV, Dwyer JT, Engel JS, Thomas PR, Betz JM, Sempos CT, Picciano MF. Dietary supplement use in the United States, 2003-2006. J Nutr. 2011 Feb;141(2):261-6. doi: 10.3945/jn.110.133025
- Merck Sharp & Dohme Corp., Merck Manual. Vitamin B6. https://www.merckmanuals.com/professional/nutritional-disorders/vitamin-deficiency,-dependency,-and-toxicity/vitamin-b-6
- Bender DA. Non-nutritional uses of vitamin B6. Br J Nutr. 1999 Jan;81(1):7-20. https://core.ac.uk/reader/1804412
- Morris MS, Picciano MF, Jacques PF, Selhub J. Plasma pyridoxal 5′-phosphate in the US population: the National Health and Nutrition Examination Survey, 2003-2004. Am J Clin Nutr. 2008 May;87(5):1446-54. doi: 10.1093/ajcn/87.5.1446.
- Bendich A, Cohen M. Vitamin B6 safety issues. Ann N Y Acad Sci. 1990;585:321-30. doi: 10.1111/j.1749-6632.1990.tb28064.x
- Gdynia HJ, Müller T, Sperfeld AD, Kühnlein P, Otto M, Kassubek J, Ludolph AC. Severe sensorimotor neuropathy after intake of highest dosages of vitamin B6. Neuromuscul Disord. 2008 Feb;18(2):156-8. doi: 10.1016/j.nmd.2007.09.009
- Perry TA, Weerasuriya A, Mouton PR, Holloway HW, Greig NH. Pyridoxine-induced toxicity in rats: a stereological quantification of the sensory neuropathy. Exp Neurol. 2004 Nov;190(1):133-44. doi: 10.1016/j.expneurol.2004.07.013
- Shrim A, Boskovic R, Maltepe C, Navios Y, Garcia-Bournissen F, Koren G. Pregnancy outcome following use of large doses of vitamin B6 in the first trimester. J Obstet Gynaecol. 2006 Nov;26(8):749-51. doi: 10.1080/01443610600955826
- U.S. Department of Agriculture, Agricultural Research Service. 2011. USDA National Nutrient Database for Standard Reference, Release 24. Nutrient Data Laboratory Home Page. https://www.ars.usda.gov/northeast-area/beltsville-md/beltsville-human-nutrition-research-center/nutrient-data-laboratory/
- Subar AF, Krebs-Smith SM, Cook A, Kahle LL. Dietary sources of nutrients among US adults, 1989 to 1991. J Am Diet Assoc. 1998 May;98(5):537-47. doi: 10.1016/S0002-8223(98)00122-9
- Food Labeling: Revision of the Nutrition and Supplement Facts Labels. https://www.federalregister.gov/documents/2016/05/27/2016-11867/food-labeling-revision-of-the-nutrition-and-supplement-facts-labels
- Pyridoxine Deficiency. https://emedicine.medscape.com/article/124947-overview#a7
- Joyce T, Brown FC, Adalat S, Reid CJD, Sinha MD. Vitamin B6 blood concentrations in paediatric dialysis patients. Pediatr Nephrol. 2018 Nov;33(11):2161-2165. doi: 10.1007/s00467-018-4053-9
- Echaniz-Laguna A, Mourot-Cottet R, Noel E, Chanson JB. Regressive pyridoxine-induced sensory neuronopathy in a patient with homocystinuria. BMJ Case Rep. 2018 Jun 28;2018:bcr2018225059. doi: 10.1136/bcr-2018-225059
- Strobbe S, Van Der Straeten D. Toward Eradication of B-Vitamin Deficiencies: Considerations for Crop Biofortification. Front Plant Sci. 2018 Apr 6;9:443. doi: 10.3389/fpls.2018.00443
- Banihani SA. A Systematic Review Evaluating the Effect of Vitamin B6 on Semen Quality. Urol J. 2017 Dec 30;15(1):1-5. doi: 10.22037/uj.v0i0.3808
- Jankowska M, Marszałł M, Dębska-Ślizień A, Carrero JJ, Lindholm B, Czarnowski W, Rutkowski B, Trzonkowski P. Vitamin B6 and the immunity in kidney transplant recipients. J Ren Nutr. 2013 Jan;23(1):57-64. doi: 10.1053/j.jrn.2012.01.023
- Henning BF, Zidek W, Riezler R, Graefe U, Tepel M. Homocyst(e)ine metabolism in hemodialysis patients treated with vitamins B6, B12 and folate. Res Exp Med (Berl). 2001 Mar;200(3):155-68.
- Woolf K, Manore MM. Elevated plasma homocysteine and low vitamin B-6 status in nonsupplementing older women with rheumatoid arthritis. J Am Diet Assoc. 2008 Mar;108(3):443-53; discussion 454. doi: 10.1016/j.jada.2007.12.001
- Chiang EP, Smith DE, Selhub J, Dallal G, Wang YC, Roubenoff R. Inflammation causes tissue-specific depletion of vitamin B6. Arthritis Res Ther. 2005;7(6):R1254-62. doi: 10.1186/ar1821
- Kelly PJ, Kistler JP, Shih VE, Mandell R, Atassi N, Barron M, Lee H, Silveira S, Furie KL. Inflammation, homocysteine, and vitamin B6 status after ischemic stroke. Stroke. 2004 Jan;35(1):12-5. doi: 10.1161/01.STR.0000106481.59944.2F
- Balasa VV, Kalinyak KA, Bean JA, Stroop D, Gruppo RA. Hyperhomocysteinemia is associated with low plasma pyridoxine levels in children with sickle cell disease. J Pediatr Hematol Oncol. 2002 Jun-Jul;24(5):374-9. doi: 10.1097/00043426-200206000-00010
- Kaczorowska M, Kmiec T, Jakobs C, Kacinski M, Kroczka S, Salomons GS, Struys EA, Jozwiak S. Pyridoxine-dependent seizures caused by alpha amino adipic semialdehyde dehydrogenase deficiency: the first polish case with confirmed biochemical and molecular pathology. J Child Neurol. 2008 Dec;23(12):1455-9. doi: 10.1177/0883073808318543
- Striano P, Battaglia S, Giordano L, Capovilla G, Beccaria F, Struys EA, Salomons GS, Jakobs C. Two novel ALDH7A1 (antiquitin) splicing mutations associated with pyridoxine-dependent seizures. Epilepsia. 2009 Apr;50(4):933-6. doi: 10.1111/j.1528-1167.2008.01741.x
- Khayat M, Korman SH, Frankel P, Weintraub Z, Hershckowitz S, Sheffer VF, Elisha MB, Wevers RA, Falik-Zaccai TC. PNPO deficiency: an under diagnosed inborn error of pyridoxine metabolism. Mol Genet Metab. 2008 Aug;94(4):431-434. doi: 10.1016/j.ymgme.2008.04.008
- Merrill AH Jr, Henderson JM. Diseases associated with defects in vitamin B6 metabolism or utilization. Annu Rev Nutr. 1987;7:137-56. doi: 10.1146/annurev.nu.07.070187.001033
- Chiang EP, Selhub J, Bagley PJ, Dallal G, Roubenoff R. Pyridoxine supplementation corrects vitamin B6 deficiency but does not improve inflammation in patients with rheumatoid arthritis. Arthritis Res Ther. 2005;7(6):R1404-11. doi: 10.1186/ar1839
- Vech RL, Lumeng L, Li TK. Vitamin B6 metabolism in chronic alcohol abuse The effect of ethanol oxidation on hepatic pyridoxal 5′-phosphate metabolism. J Clin Invest. 1975 May;55(5):1026-32. doi: 10.1172/JCI108003
- Snider DE Jr. Pyridoxine supplementation during isoniazid therapy. Tubercle. 1980 Dec;61(4):191-6. doi: 10.1016/0041-3879(80)90038-0
- Raskin NH, Fishman RA. Pyridoxine-deficiency neuropathy due to hydralazine. N Engl J Med. 1965 Nov 25;273(22):1182-5. doi: 10.1056/NEJM196511252732203
- Nair S, Maguire W, Baron H, Imbruce R. The effect of cycloserine on pyridoxine-dependent metabolism in tuberculosis. J Clin Pharmacol. 1976 Aug-Sep;16(8-9):439-43. doi: 10.1002/j.1552-4604.1976.tb02419.x
- Apeland T, Frøyland ES, Kristensen O, Strandjord RE, Mansoor MA. Drug-induced pertubation of the aminothiol redox-status in patients with epilepsy: improvement by B-vitamins. Epilepsy Res. 2008 Nov;82(1):1-6. doi: 10.1016/j.eplepsyres.2008.06.003
- Lheureux P, Penaloza A, Gris M. Pyridoxine in clinical toxicology: a review. Eur J Emerg Med. 2005 Apr;12(2):78-85. doi: 10.1097/00063110-200504000-00007
- Reynolds R.D. Bioavailability of vitamin B-6 from plant foods. Am. J. Clin. Nutr. 1988;48:863–867. doi: 10.1093/ajcn/48.3.863
- Roth-Maier D.A., Kettler S.I., Kirchgessner M. Availability of vitamin B6 from different food sources. Int. J. Food Sci. Nutr. 2002;53:171–179. doi: 10.1080/09637480220132184
- Schorgg P., Bärnighausen T., Rohrmann S., Cassidy A., Karavasiloglou N., Kühn T. Vitamin B6 Status among Vegetarians: Findings from a Population-Based Survey. Nutrients. 2021;13:1627. doi: 10.3390/nu13051627
- Pyridoxine Deficiency Treatment & Management. https://emedicine.medscape.com/article/124947-treatment#d5
- Pyridoxine Deficiency. https://emedicine.medscape.com/article/124947-overview
- Jung H.Y., Kim W., Hahn K.R., Kwon H.J., Nam S.M., Chung J.Y., Yoon Y.S., Kim D.W., Yoo D.Y., Hwang I.K. Effects of pyridoxine deficiency on hippocampal function and its possible association with V-type proton ATPase subunit B2 and heat shock cognate protein 70. Cells. 2020;9:1067. doi: 10.3390/cells9051067
- Spinneker A, Sola R, Lemmen V, Castillo MJ, Pietrzik K, González-Gross M. Vitamin B6 status, deficiency and its consequences–an overview. Nutr Hosp. 2007 Jan-Feb;22(1):7-24.
- HUNT AD Jr, STOKES J Jr, McCRORY WW, STROUD HH. Pyridoxine dependency: report of a case of intractable convulsions in an infant controlled by pyridoxine. Pediatrics. 1954 Feb;13(2):140-5.
- Agadi S, Quach MM, Haneef Z. Vitamin-responsive epileptic encephalopathies in children. Epilepsy Res Treat. 2013;2013:510529. doi: 10.1155/2013/510529
- Rollón N, Fernández-Jiménez MC, Moreno-Carralero MI, Murga-Fernández MJ, Morán-Jiménez MJ. Microcytic anemia in a pregnant woman: beyond iron deficiency. Int J Hematol. 2015 May;101(5):514-9. doi: 10.1007/s12185-014-1723-7
- Mayengbam S, House JD, Aliani M. Investigation of vitamin B₆ inadequacy, induced by exposure to the anti-B₆ factor 1-amino D-proline, on plasma lipophilic metabolites of rats: a metabolomics approach. Eur J Nutr. 2016 Apr;55(3):1213-23. doi: 10.1007/s00394-015-0934-x
- Ubbink JB, Serfontein WJ, de Villiers LS. Stability of pyridoxal-5-phosphate semicarbazone: applications in plasma vitamin B6 analysis and population surveys of vitamin B6 nutritional status. J Chromatogr. 1985 Aug 9;342(2):277-84. doi: 10.1016/s0378-4347(00)84518-1
- Pyridoxine Deficiency Treatment & Management. https://emedicine.medscape.com/article/124947-treatment
- Badrinath M, John S. Isoniazid Toxicity. [Updated 2022 Jun 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK531488
- Pyridoxine Deficiency. https://emedicine.medscape.com/article/124947-overview#a2
- Meyer HE, Willett WC, Fung TT, Holvik K, Feskanich D. Association of High Intakes of Vitamins B6 and B12 From Food and Supplements With Risk of Hip Fracture Among Postmenopausal Women in the Nurses’ Health Study. JAMA Netw Open. 2019 May 3;2(5):e193591. doi: 10.1001/jamanetworkopen.2019.3591





{kind=link}