
What is HDL Cholesterol ?
Cholesterol is a waxy, fat-like substance that occurs naturally in all parts of the body. Your bodies need cholesterol to make cell membranes, key hormones like testosterone and estrogen, the bile acids needed to digest and absorb fats and vitamin D. Cholesterol is so important to the body that the liver and intestines make it from scratch. However, cholesterol also is found in some of the foods you eat.
Cholesterol is carried through your bloodstream by carriers made of fat (lipid) and proteins. These are called – lipoproteins.
Two types of lipoproteins carry cholesterol to and from cells. One is low-density lipoprotein or LDL. The other is high-density lipoprotein or HDL. The amount of each type of cholesterol in your blood can be measured by a blood test.
HDL cholesterol is “good” cholesterol because HDL cholesterol absorbs cholesterol and carries it back to the liver, which flushes it from the body. Think of it as the “healthy” cholesterol, so higher levels are better. Experts believe HDL acts as a scavenger, carrying LDL cholesterol away from the arteries and back to the liver. There it’s broken down and passed from the body.
When checking LDL and HDL, doctors often include another type of fat called triglycerides.
- Total cholesterol is a measure of the total amount of cholesterol in your blood and is based on the HDL, LDL, and triglycerides numbers.
- LDL cholesterol makes up the majority of the body’s cholesterol. LDL is known as “bad” cholesterol because having high levels can lead to plaque buildup in your arteries and result in heart disease and stroke.
- HDL cholesterol absorbs cholesterol and carries it back to the liver, which flushes it from the body. HDL is known as “good” cholesterol because having high levels can reduce the risk for heart disease and stroke.
- Triglycerides are a type of fat found in your blood that your body uses for energy. The combination of high levels of triglycerides with low HDL cholesterol or high LDL cholesterol can increase your risk for heart attack and stroke.
A low HDL cholesterol level is associated with a high incidence of cardiovascular disease in the context of a wide variety of concomitant conditions such as type 2 diabetes mellitus and obesity 1. HDL cholesterol can stimulate the removal of cholesterol from cells, including those involved in atherosclerosis, and can deliver the cholesterol to the liver where some of it may be secreted in bile and excreted, a process called reverse cholesterol transport 2. However, unlike LDL cholesterol, genetic variation that affects HDL cholesterol is not associated with expected differences in cardiovascular disease unless LDL cholesterol or triglyceride is also affected by the genetic variants 3 or reverse cholesterol transport is impaired 4. Still, these genetic studies, often called mendelian randomization, may not be capturing important loci for the protective effect of HDL that may be reflective in HDL cholesterol raising by dietary fats compared with carbohydrates. Although increases in HDL cholesterol by some pharmacological treatments have not decreased cardiovascular disease 5, 6, this does not directly pertain to the effects of dietary fat because the underlying mechanisms of effects of drugs such as a cholesterylester transfer protein inhibitor and nicotinic acid are probably not the same as those affected by dietary fats and carbohydrates. The HDL field is working toward a functional approach to cardiovascular disease risk prediction and treatment. For example, a small experimental study showed that consumption of saturated fat reduces the anti-inflammatory potential of HDL and impairs arterial endothelial function. In contrast, the anti-inflammatory activity of HDL improves after consumption of polyunsaturated fat 7. Replacing saturated fat with polyunsaturated or monounsaturated
fat (1% daily energy exchanged) lowers HDL cholesterol slightly by 0.2 and 0.1 mg/dL 8. Using carbohydrates as a replacement lowers HDL cholesterol more by 0.4 mg/dL. Carbohydrates also lower HDL cholesterol when replacing monounsaturated or polyunsaturated fats. Both low- and high-glycemic-index carbohydrates lower HDL cholesterol 9, 10.
Experts believe HDL cholesterol may act in a variety of helpful ways that tend to reduce the risk for heart disease 11:
- High HDL cholesterol 60 mg/dL or higher is Protective against heart disease.
- HDL cholesterol scavenges and removes LDL or “bad” cholesterol.
- HDL reduces, reuses, and recycles LDL cholesterol by transporting it to the liver where it can be reprocessed.
- HDL cholesterol acts as a maintenance crew for the inner walls (endothelium) of blood vessels. Damage to the inner walls is the first step in the process of atherosclerosis, which causes heart attacks and strokes. HDL scrubs the wall clean and keeps it healthy.
People with high blood triglycerides usually also have lower HDL cholesterol. Genetic factors, type 2 diabetes, smoking, being overweight and being sedentary can all lower HDL cholesterol. Women tend to have higher levels of HDL cholesterol than men do.
A healthy HDL cholesterol level may protect against heart attack and stroke. Studies show low levels of HDL cholesterol increase the risk of heart disease. HDL cholesterol does not completely eliminate LDL cholesterol. Only one-fourth to one-third of blood cholesterol is carried by HDL.
| Desirable Cholesterol Levels | |
|---|---|
| Total cholesterol | Less than 200 milligrams per deciliter of blood (mg/dL) or 5.18 mmol/L |
| LDL (“bad” cholesterol) | Less than 100 mg/dL (2.59 mmol/L) |
| HDL (“good” cholesterol) | 60 mg/dL (1.55 mmol/L) or higher |
| Triglycerides | Less than 150 mg/dL (1.70 mmol/L) |
Footnote:
Total blood (or serum) cholesterol is a composite of different measurements. Your total blood cholesterol is calculated by adding your HDL and LDL cholesterol levels, plus 20% of your triglyceride level.
Triglycerides are the most common type of fat in your blood. Triglycerides come from food, and your body also makes them. When you eat, your body converts calories it doesn’t need into triglycerides, which are stored in fat cells. High triglyceride levels are associated with several factors, including being overweight, eating too many sweets or drinking too much alcohol, smoking, being sedentary, or having diabetes with elevated blood sugar levels.
“Normal ranges” are less important than your overall cardiovascular risk. Like HDL and LDL cholesterol levels, your total blood cholesterol level should be considered in context with your other known risk factors.
Your doctor can recommend treatment approaches accordingly.
[Source 12 ]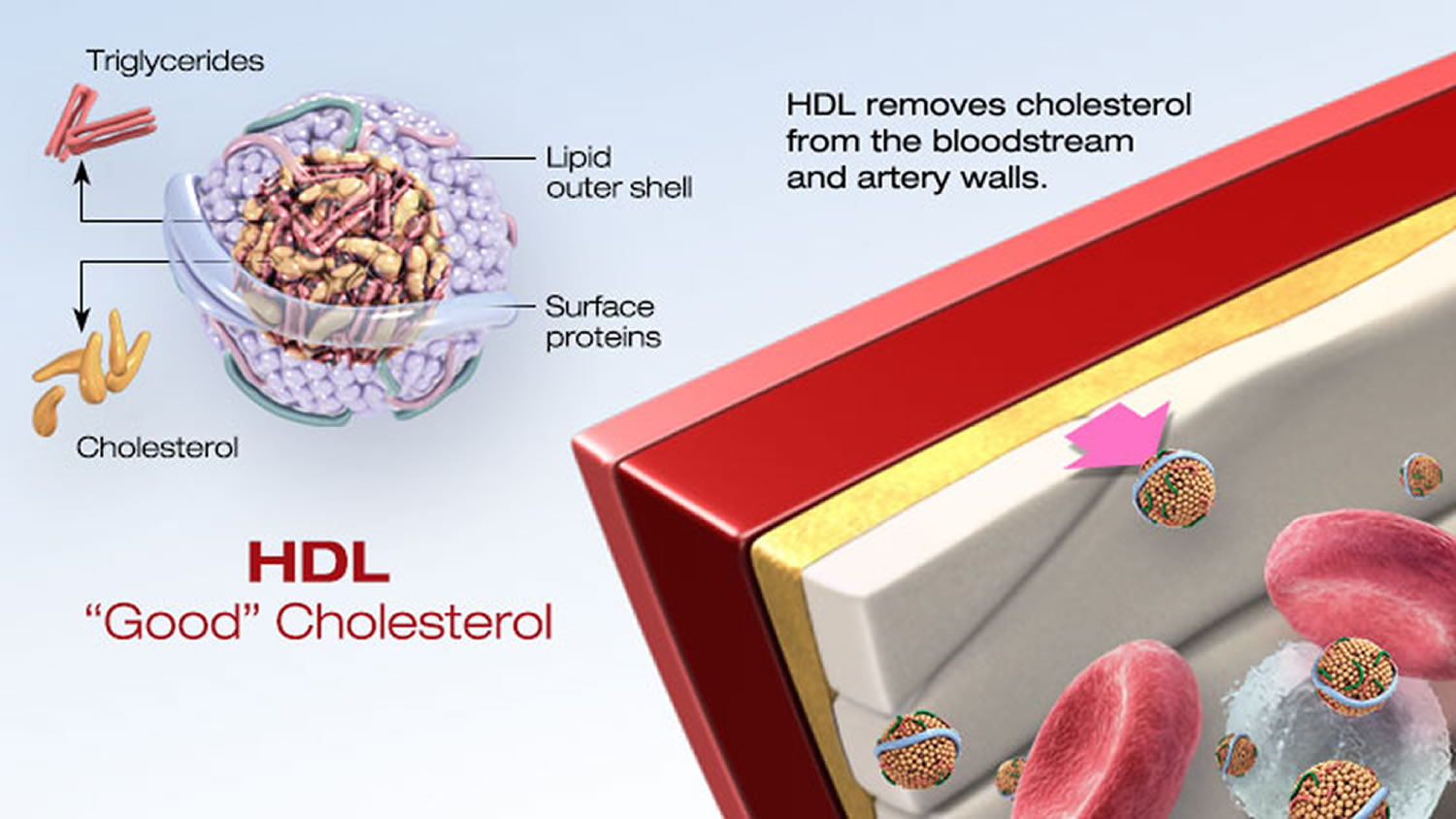
What can you do if your HDL Cholesterol Level is Low ?
If your HDL is low, you can take several steps to boost your HDL level and reduce your heart disease risk 13:
- Get physically active or exercise – Aerobic exercise for 30 to 60 minutes on most days of the week can help pump up your HDL levels. Some studies suggest that physical activity can raise HDL cholesterol. The American Heart Association recommends three to four 40-minute sessions of moderate- to vigorous-intensity aerobic activity per week for adults trying to lower their LDL cholesterol or blood pressure.
- Eat better fats. The monounsaturated and polyunsaturated fats described above can raise HDL cholesterol levels.
- Cut out trans fats. Not only do they increase LDL cholesterol, they decrease HDL cholesterol too.
- Quit smoking – Tobacco smoke lowers HDL, and quitting can increase HDL levels.
- Keep a healthy weight – Being overweight increases LDL cholesterol and reduces HDL cholesterol levels. Losing even a few pounds will increase your HDL-C and lower your LDL-C and blood pressure. Avoiding obesity besides improving HDL levels, reduces risk for heart disease and multiple other health conditions.
- Emerging Risk Factors Consortium. Major lipids, apolipoproteins and risk of vascular disease. JAMA. 2009;302:1993–2000
- Rosenson RS, Brewer HB Jr, Davidson WS, Fayad ZA, Fuster V, Goldstein J, Hellerstein M, Jiang XC, Phillips MC, Rader DJ, Remaley AT, Rothblat GH, Tall AR, Yvan-Charvet L. Cholesterol efflux and atheroprotection: advancing the concept of reverse cholesterol transport. Circulation. 2012;125:1905–1919. doi: 10.1161/ CIRCULATIONAHA.111.066589.
- Voight BF, Peloso GM, Orho-Melander M, Frikke-Schmidt R, Barbalic M, et. al. Plasma HDL cholesterol and risk of myocardial infarction: a mendelian randomisation study. Lancet. 2012;380:572–580. doi: 10.1016/S0140-6736(12)60312-2.
- Zanoni P, Khetarpal SA, Larach DB, Hancock-Cerutti WF, Millar JS, Cuchel M, DerOhannessian S, et. al. Global Lipids Genetics Consortium. Rare variant in scavenger receptor BI raises HDL cholesteroland increases risk of coronary heart disease. Science. 2016;351:1166–1171. doi: 10.1126/science.aad3517.
- AIM-HIGH Investigators. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy [published correction appears in N Engl J Med. 2012;367:189]. N Engl J Med. 2011;365:2255.
- Schwartz GG, Olsson AG, Abt M, Ballantyne CM, Barter PJ, Brumm J, Chaitman BR, Holme IM, Kallend D, Leiter LA, et. al; dal-OUTCOMES Investigators. Effects of dalcetrapib in atients with a recent acute coronary syndrome. N Engl J Med. 2012;367:2089–2099. doi: 10.1056/NEJMoa1206797.
- Nicholls SJ, Lundman P, Harmer JA, Cutri B, Griffiths KA, Rye KA, Barter PJ, Celermajer DS. Consumption of saturated fat impairs the anti-inflammatory properties of high-density lipoproteins and endothelial function. J Am Coll Cardiol. 2006;48:715–720. doi: 10.1016/j.jacc.2006.04.080.
- Mensink RP. Effects of Saturated Fatty Acids on Serum Lipids and Lipoproteins: A Systematic Review and Regression Analysis. Geneva, Switzerland: World Health Organization; 2016.
- Sacks FM, Carey VJ, Anderson CA, Miller ER 3rd, Copeland T, Charleston J, Harshfield BJ, Laranjo N, McCarron P, Swain J, White K, Yee K, Appel LJ. Effects of high vs low glycemic index of dietary carbohydrate on cardiovascular disease risk factors and insulin sensitivity: the OmniCarb randomized clinical trial. JAMA. 2014;312:2531–2541. doi: 10.1001/jama.2014.16658.
- TG and HDL Working Group of the Exome Sequencing Project, National Heart, Lung, and Blood Institute. Loss-of-function mutations in APOC3, triglycerides, and coronary disease. N Engl J Med. 2014;371:22–31.
- Centers for Heart Disease and Stroke Prevention. State Heart Disease and Stroke Prevention Programs Address High Blood Cholesterol. https://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_state_cholesterol.htm
- National Cholesterol Education Program. Third Report of the National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. https://www.nhlbi.nih.gov/files/docs/guidelines/atp3xsum.pdf
- American Heart Association. Why Cholesterol Matters. http://heartinsight.heart.org/Summer-2017/Why-Cholesterol-Matters/





{kind=link}