
How to whiten teeth naturally
Teeth whitening has become one of the most frequently requested dental procedures by the public due to influence by the portrayal of perfect white smiles in the media 1. In the late 1980’s several companies introduced both home-based products and professionally applied tooth whitening products into the U.S. marketplace. These have gained popularity with the public who has come to demand whiter, more perfect smiles 2. And now the public has come to demand whiter, more perfect smiles and in response many choices for teeth whitening that have been made available. These include home-based products such as toothpastes, gels, and films, as well as in-office based systems where products containing highly concentrated bleaching agents are applied under professional supervision. The profession and public have been aware of certain risks related to tooth whitening such as increased tooth sensitivity and gingival irritation 1. New research has shown that there are other risks such as tooth surface roughening and softening, increased potential for demineralization, degradation of dental restorations, and unacceptable color change of dental restorations. The new research is also focused on optimizing whitening procedures to reduce tooth sensitivity and to increase the persistence of the whitening.
Causes of teeth discoloration
There are several different methods for whitening teeth, each with their own mechanism of action. The effectiveness of these different methods is dependent upon the particular tooth discoloration that is being treated. Causes of tooth discoloration can be categorized into two main groups (see Figure. 1):
- Intrinsic staining.
- Extrinsic staining.
Intrinsic staining
Intrinsic staining, sometimes called internal staining, can be attributed to factors such as genetics, age (from enamel wear over time exposing yellower dentin), antibiotics, high levels of fluoride, and developmental disorders and can start before the tooth has erupted. After eruption of the tooth some dental restorations can cause tooth staining.
Extrinsic staining
Extrinsic staining, sometimes called external staining, is largely due to environmental factors including smoking, pigments in beverages and foods, antibiotics, and metals such as iron or copper. Colored compounds from these sources are adsorbed into acquired dental pellicle or directly onto the surface of the tooth causing a stain to appear. See Figure. 1 for examples of the staining from these sources.
Figure 1. Examples of teeth staining

Note: Extrinsic staining examples: A. Smoking; B. Wine stain; and C. Food stain. Intrinsic staining examples: D. Age yellowing; E. Decay; F. Orthodontic white spot lesion; G. Mild fluorosis; H. Amalgam restoration; I. Tetracycline stain; J. Genetic (amelogenesis imperfecta); K. and Non-vital coloring.
How does teeth whitening generally work ?
Hydrogen peroxide (H2O2) is a powerful oxidising agent 1. It gives rise to agents known to be effective bleaching agents. The mechanisms of bleaching involve the degradation of the extracellular matrix and oxidation of chromophores located within enamel and dentin. However, hydrogen peroxide produces also local undesirable effects on tooth structures and oral mucosa. In clinical conditions, the daily low-level doses used to produce tooth whitening never generate general acute and sub-acute toxic effects. Genotoxicity and carcinogenicity only occur at concentrations that are never reached during dental treatments. Some transient adverse effects have been reported on the oral mucosa and the digestive tract if the product is swallowed. Local effects may occur on the oral mucosa and dental tissues during whitening, namely, pulp sensitivity, cervical resorption, release of selected components of dental restorative materials, and alteration of the enamel surface. Most of the local effects are dependent of the technique and concentration of the product so far used, but as the results of bleaching obtained are not stable, repeated treatments add to the adverse effects. The informed decision to administer or not and the control of bleaching effects should stand in the hand of dental surgeons and certainly not as it appears at present, as cosmetics sold without any restriction despite the potential health hazards of peroxides.
Teeth whitening is any process that lightens the color of a tooth 1. Whitening may be accomplished by physical removal of the stain or a chemical reaction to lighten the tooth color 1. Bleaching is defined here as the chemical degradation of the chromogens. The active ingredient in most whitening products is hydrogen peroxide (H2O2) which is delivered as hydrogen peroxide or carbamide peroxide 1. Carbamide peroxide is a stable complex that breaks down in contact with water to release hydrogen peroxide. Because carbamide peroxide releases hydrogen peroxide the chemistry of most tooth whitening is that of hydrogen peroxide 1.
Teeth stains consist of compounds that have color or darker shades called chromogens that are accumulated in the tooth (intrinsic) or on the tooth (extrinsic). Chromogens fall into two categories: large organic compounds that have conjugated double bonds in their chemical structure as shown in Figure 2A; and metal containing compounds. Bleaching of the organic compounds by hydrogen peroxide involves reacting with the double bonds to oxidize the double bond as shown in Figure 2B. This causes the chromogen to become a lighter colored compound. Bleaching of the metallic compounds is much more difficult; better esthetic options may be veneers, bonding, or crowns. There are some professional products that contain sodium hypochlorite (NaOCl) which reacts with the double bonds of the chromogen in much the same way as peroxide as shown in Figure 2C 1.
New studies have shown that aggressive tooth bleaching can cause increased tooth sensitivity, changes in tooth microstructure, and restoration changes. Aggressive bleaching can chemically react with composite restorations, glass ionomer cements, sealants, and ceramic crowns, thus reducing their stability 1.
- In one in test tube study 3, seven tooth colored restoration substrates including a nanohybrid composite, a microhybrid composite, a flowable composite, and a packable composite resin, along with a compomer, a glass ionomer cement and a sintered ceramic used for CAD/CAM restorations were exposed to 40 % hydrogen peroxide gel following manufacturer’s instructions at either 25 °C or 37 ° C and placed in artificial saliva between treatments. All of the materials were found to have surface softening with greater softening observed at 37 °C except for the sintered ceramic. No substance loss was observed for any material. However, the conditions of the experiments did not include subsequent abrasion (toothbrushing with dentifrice) as would occur in vivo and thus loss of restorative material from the softened surfaces is possible 3.
- Another in laboratory study looked at the effect of home bleaching on color change and translucency of resin composites. Five commercially available composites were treated for 14 days with either 10 % carbamide gel or 10 % hydrogen peroxide gel following manufacturer’s instructions. There was significant (and unacceptable) color change in all of the composites with either of the home-based treatments. They found no significant difference between the carbamide peroxide and hydrogen peroxide treatments in the color changes. Interestingly, there was no change in the resin composite translucency indicating that the color change was restricted to the surface of the resin composites 4.
- A randomized clinical trial showed that in-office bleaching of restored teeth using a 35 % hydrogen peroxide product caused tooth sensitivity in all cases. There was significantly greater intensity of tooth sensitivity pain for teeth that had restorations than for sound teeth. It was concluded that in-office bleaching with 35 % hydrogen peroxide was effective for patients with restored teeth, however that a higher degree of pain was found for these patients, especially associated with the upper lateral incisors 5.
Figure 2. How Teeth Whitening Generally Work
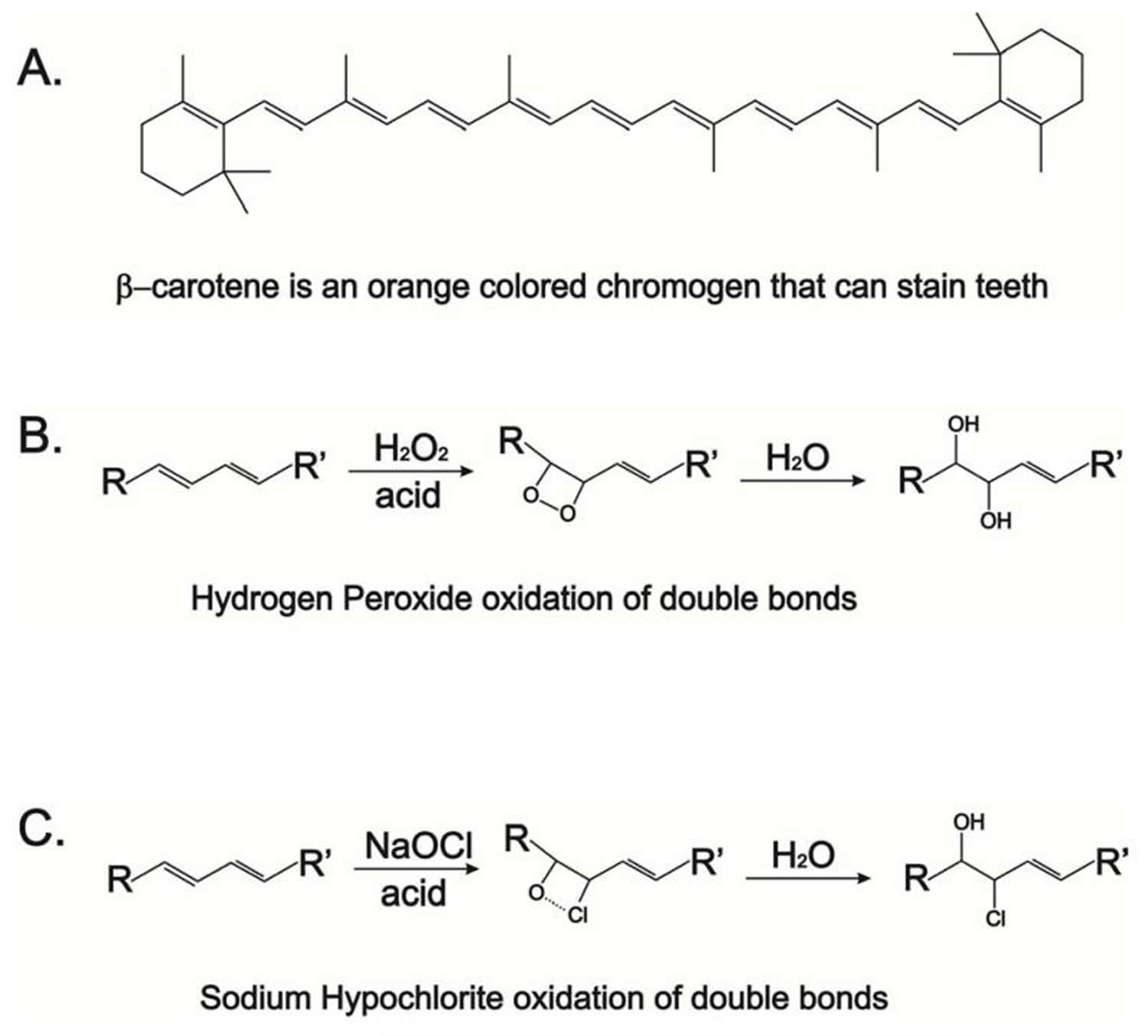
Note: Chemistry of chromogen bleaching. A. β-carotene is an example of an organic chromogen with many conjugated double bonds; B. Chemical reaction of hydrogen peroxide with a chromogen double bond; and C. Chemical reaction of sodium hypochlorite with a chromogen double bond.
How to whiten teeth naturally overnight
Different product types are marketed to address the particular stain to be removed. The broad categories include: cleansers such as smokers’ toothpastes which contain larger amounts of detergents and abrasives to aid in the removal of chromogens from the tooth surfaces; bleaches to react with the chromogens to lighten color; and products that have both increased cleansing and bleaching. More severe or complex stains are best lightened professionally, while over-the-counter products can be used for milder cases 1. The treatment time required for reaching the tooth whitening end point is dependent on the time of exposure and the concentration of bleaching compound. This end point is dependent on the type of whitening employed, usually 1 to 2 shades for cleansers and over-the-counter (OTC) gels, and more for professionally applied products.
There are many teeth whitening systems out there. The following approach is in accordance with the American Academy of Cosmetic Dentistry 6.
Teeth whitening methods can be generally categorized into the following:
Tray-Based Tooth Whiteners
Tray-based tooth whitening systems are available both professionally and over-the-counter (OTC) 1. This method involves use of a fitted tray containing carbamide peroxide-bleaching gel worn for 2 to 4 hours a day or overnight 1. Usually by following the manufacturer instructions tooth whitening is noticeable in a few days, lightening the teeth by 1 or 2 shades.
The tray-based tooth whiteners can be done at-home under a dentist supervision. The most popular bleaching method is use of dentist-prescribed carbamide peroxide or hydrogen peroxide in trays used outside the dental office 7. Usually a dentist will give advice and provide supervision to patients and thus prevent most potential side effects or adverse events encountered in the bleaching procedure, including excessive bleaching to unnatural colors or whitening teeth so much that surrounding teeth restorations appear to be darker. Two significant challenges still remain with at-home bleaching. Many people find that carbamide peroxide or hydrogen peroxide is available in their local grocery store or chemist with non-custom trays. They then continue bleaching by using these relatively inexpensive gels and solutions in the well-fitted trays made by their dental care providers. Additionally, the many available over-the-counter bleaching products like gel, strips, paint-on-solutions, gum and other products – have allowed people the opportunity to bleach too much 7. The result of this “user-initiated” and “user-bleaching” method is that the teeth become too white and the surrounding teeth restorations like resin-based composite or tooth colored crowns appear to be too dark. Subsequently at-home users usually complain about their mismatching teeth restorations and often the otherwise acceptable restorations must be replaced with materials that matched the bleached teeth 7.
The results of this study 8 concur with those of previously reported studies that nightguard vital bleaching using a 10% carbamide peroxide whitening solution according to the manufacturer’s instructions is efficacious and safe, with minimal side effects. In addition, long-term shade retention was reported by 82% of the participants at the end of the study, with no adverse side effects 8. The whitening effect lasted up to 47 months in 82% of the patients, with no adverse side effects reported at the end of the study.
In-Office Whitening
Quicker tooth lightening can be achieved through in-office whitening because the products deliver higher concentrations of peroxide than over-the-counter (OTC) products. Consequently, gingival tissues are usually protected before the agent is applied, but post procedure tooth sensitivity is common and color returns to the teeth relatively soon 7. Some products claim to increase the oxidation of chromogens by exposure to heat or an intense blue light with a wave length between 480 nm and 520 nm to activate the product while on the tooth, causing the chemical reactions to proceed faster. Some professionals use laser systems to increase the rate of the chemical reactions. This use of lasers is considered to be an ‘off-label’ use of laser systems in dentistry by the US Food and Drug Administration 1. In a systematic review by Buchalla and Attin 9 found no added benefit from light-activated systems and thus the American Dental Association does not endorse such whitening systems 1. Moreover, existing literature reveals that activation of bleaching agents by heat, light or laser may have an adverse effect on teeth pulpal tissue due to an increase of intra-pulpal temperature exceeding the critical value of 5.5 degrees Celsius 9. Tooth lightening results are seen after one 30- to 60-minute treatment. More dramatic results can be obtained with several applications.
This randomized clinical study 10 assessed efficacy in terms of color change and production of sensitivity of at-home whitening alone with home whitening supplemented with in-office bleaching. Thirty-six subjects (aged 19 to 58 years) were randomly assigned to one of three different treatment groups: (A) home whitening for two weeks, with 16% carbamide peroxide in custom-made trays; (B) home whitening for two weeks, with 16% carbamide peroxide in custom-made trays supplemented with in-office bleaching with 9% hydrogen peroxide (in the same trays); or (C) home whitening for two weeks, with 16% carbamide peroxide in custom-made trays supplemented with in-office bleaching with 27% hydrogen peroxide (in the same trays). The efficacy of teeth whitening was assessed by determining the color change associated with the six upper anterior (front) teeth using a value-ordered shade guide. Sensitivity was self-assessed with the use of a visual analog scale. Teeth shade and sensitivity were assessed at the following points: pretreatment; immediately after the home whitening phase; immediately after the in-office phase (groups B and C); and one week post active treatment. At the one week follow-up visit, subjects in group A had a mean color change of 5.9 (teeth were lighter) immediately after cessation of treatment. Subjects in groups B and C experienced a greater change in mean shade immediately following their respective in-office treatments of 5.1 and 5.4. However, within one week, the shade of these teeth regressed to a similar degree to that achieved by subjects treated in group A. Overall, no significant difference in shade change or sensitivity was produced between the three groups 10. Investigators concluded that the in-office element of combined whitening produced no significant difference in tooth color or sensitivity when compared with home whitening alone 10.
A systematic review and meta-analysis of the literature to evaluate the influence of light on bleaching efficacy and tooth sensitivity during in-office bleaching found that light increases the risk of tooth sensitivity during in-office bleaching 11. This review also found that light did not improve the bleaching effect when high concentrations of hydrogen peroxide (25–35%) were employed 11. The authors conclude that “dentists should use the light-activated system with great caution or avoid its use.” One disturbing aspect of this systematic review is that after nearly 30 years of tooth whitening there were only 11 randomized clinical trials of sufficient quality to be included in the meta-analysis out of the 301 studies regarding light-activated bleaching. Clearly there is a need for high quality clinical trials to help the profession understand the effects and risks associated with tooth whitening products and procedures 1.
Whitening Toothpastes
Whitening toothpastes typically contain higher amounts of abrasives and detergents than standard toothpastes, to remove tougher stains. Whitening toothpastes do not contain bleach (sodium hypochlorite), but some contain low concentrations of carbamide peroxide or hydrogen peroxide that help lighten tooth color 1. Whitening toothpastes typically can lighten tooth color by about one or two shades 1.
Whitening Strips and Gels
Whitening strips were introduced into the market in the late 1980’s. They deliver a thin layer of peroxide gel on plastic strips shaped to fit onto the buccal surfaces of the teeth 1. There are a variety of white strip products on the market with varying instructions. A typical set of instructions are to apply the strips twice daily for 30 minutes for 14 days 1. Tooth lightening can be seen in several days and this method can lighten the teeth by 1 or 2 shades 1. There are some newer whitening strip products that require only one 30-minute application per day that have the same whitening end point as the two-a-day products 1.
Whitening gels are peroxide-based gels applied with a small brush directly to the surface of the teeth 1. Manufacturer’s instructions are usually twice a day applications for 14 days 1. Like the whitening strips, the teeth can usually be lightened by 1 or 2 shades.
In a systematic review comparing the effectiveness and safety of over-the-counter whitening strips compared to home-whitening with the American Dental Association (ADA)-recommended home-whitening using the 10 % carbamide peroxide gel 12. Eight studies were included in the systematic review. The systematic review revealed no significant difference between the intervention groups for tooth-whitening efficacy measured and gingival sensitivity were similar, regardless of the whitening method used 12. The observed gingival irritation was higher when the 10 % carbamide peroxide gel was applied on tray. The conclusion from this review was that, there is no sound evidence in dental literature to suggest that the American Dental Association (ADA)-recommended whitening technique based on 10 % carbamide peroxide gel could be substituted by the whitening strips. The existing studies, with their limitations, revealed similar tooth whitening and tooth and gingival sensitivity for both whitening techniques 12.
Whitening Rinses
Whitening rinses contain oxygen sources such as hydrogen peroxide to react with the chromogens 1. Manufacturer’s instructions are for twice a day rinsing for 60 seconds each. It takes up to 3 months to see a 1 or 2 shade improvement in tooth color 1.
How long will the treated, whitened teeth last ?
It is difficult to predict the persistence of bleaching regimens because some people may routinely expose their teeth to food or beverages which are known to stain teeth and would experience re-staining within a month. However, if the teeth are not exposed to chromogens such as coffee, red wine, cigarette smoke, then it would be reasonable to assume that whitened teeth could persist or up to a year 1. There are several in vitro and clinical studies on this topic.
- In a recent clinical trial it was found that by following a regimen consisting of in-office bleaching for two sessions with a 1-week interval, followed by home bleaching once a month for 3 months gave more persistence in color change over a 6-month period than in-office bleaching alone 13. This later study shows that this regimen for whitening maintenance can extend the effectiveness of the whitening treatment.
- An in vitro study that looked at the color change of enamel, dentine, and combined enamel and dentin of bleached tooth samples found that the color was not stable over time with regard to lightness. However, yellowness did not return to baseline within 1 year 14.
- Another in vitro study designed to evaluate the color stability of bleaching after light activation with either a halogen unit, laser, LED unit; or bleaching without light activation found that all the tested methods achieved good aesthetic results even 3 months after the end of the bleaching. Additionally, the authors found that light activation of the bleaching agent was not beneficial compared to bleaching alone and light activation made no difference in the color stability up to 3 months after bleaching 15.
- In a randomized clinical trial involving 90 patients using a split mouth design, found that the degree of bleaching obtained with a home-bleaching technique using 10 % carbamide peroxide gel applied via a tray was similar to that obtained with the in-office technique that applied 35 % hydrogen peroxide, regardless of light irradiation or the combination of home/in-office techniques 16. The use of a light source for in-office bleaching did not influence the rate of bleaching, or the intensity of tooth sensitivity, or the durability of the bleaching effect; therefore, light irradiation is not recommended. The combination of in-office and home-bleaching techniques increased the rate of bleaching only in the first week. However, the same combination did not influence the results after the first week. Increase in the tooth sensitivity was observed with the in-office technique immediately after treatment, regardless of light irradiation 16. In view of these results – especially the higher degree of tooth sensitivity with the in-office techniques, the authors conclude that “Dentists must inform their patients about the expected outcomes of each procedure and provide an evidence-based choice.”
Teeth whitening risks and side effects
When manufacturer’s instructions are followed, hydrogen peroxide and carbamide peroxide based tooth whitening is safe and effective. However there are certain risks associated with teeth whitening such as increased teeth sensitivity, teeth surface roughening and softening, increased potential for teeth demineralization, degradation of dental restorations, unacceptable color change of dental restorations and gingival irritation.
Risks commonly reported with tooth whitening include increased tooth sensitivity and mild gingival irritation. The degree of these side effects is directly related to the concentration of the peroxide bleach component, duration of the treatment, and the non-bleach composition of the product used 1. Tooth sensitivity usually occurs at the time of treatment and can last several days; gingival irritation begins within a day of the treatment and can also last several days. There are additional risks that have been reported from in laboratory studies which include tooth erosion, tooth mineral degradation, increased susceptibility to demineralization, and pulpal damage 17. The ultimate endpoint for tooth whitening is dependent upon the tooth itself, with common wisdom telling us that all treatment regimens will eventually arrive at the same whitening endpoint. This is not exactly true as some very aggressive regimens can damage the tooth through dehydration and demineralization such that the tooth temporarily appears whiter 1.
The risk of tooth structure damage has received attention by researchers who have evaluated the effects of aggressive tooth bleaching treatments on tooth structure and susceptibility to demineralization. Some of these studies have found that aggressive whitening treatments can change the surface integrity, microstructure of enamel crystals, and susceptibility to demineralization.
- In an in vitro study performed in a lab, researchers tested five different bleaching products for erosion of human enamel. The five products included strips at 6.5 % hydrogen peroxide, and gels at 10 % and 22 % carbamide peroxide, 35 % hydrogen peroxide, and a sodium hypochlorite containing gel system. The researchers followed the manufacturer’s instructions and measured the loss of enamel surface by polarized light microscopy. They found that although some surfaces were softened, no enamel erosion was found 18).
- A new in vitro study conducted in Japan evaluated the susceptibility of a tooth to subsequent demineralization after a home based 10 % carbamide peroxide bleaching regimen compared to a more aggressive office-based 35 % hydrogen peroxide photoactivated regimen. Extracted teeth of color Vita shade A3 were bleached following manufacturer’s instructions until the shade was lightened to Vita shade A2 for all teeth. The teeth were then demineralized for two weeks and evaluated for mineral density loss. This study found that the surface integrity of the home-based treated teeth was altered such that significantly greater demineralization occurred in the home-based treated teeth than in the office-based treated teeth. The authors postulate that the peroxide in the office based gel penetrates deeper into the enamel before it was activated by photoirradiation 19.
- The effect of cold-light activated bleaching treatment on enamel surfaces in vitro was studied because there is concern that either heat (infrared) or ultraviolet light exposure of teeth and gingiva during office bleaching could cause pulp and/or gingival tissue damage 20. In this study the crystal and surface microstructure of dental enamel was evaluated after 35 % hydrogen peroxide bleaching with cold-light irradiation (group LP); 35 % hydrogen peroxide bleaching without cold-light irradiation (group P); a control group treated with what is identified as a silica dioxide catalyzing agent as a peroxide-free bleaching agent (control group NP); and a control group treated with the cold-light irradiation alone (control group L). The authors report that no color change or enamel crystal size change was observed in the two control groups, indicating that the cold-light treatment alone or the silica dioxide agent had no effect on the tooth structure. However, the groups that had 35 % hydrogen peroxide (with or without cold-light) did result in significant color change as well as significant decrease in crystal size and crystallinity. There was no significant difference in the degree of color change between the cold-light activated hydrogen peroxide and the hydrogen peroxide only groups. Additionally, surface roughness was observed to increase in all groups except the cold-light only control group. The authors conclude that the 35% hydrogen peroxide solution had a major demineralization effect on enamel surface and the cold-light had no significant increased or decreased effect on the demineralization or color change 20. The mechanism suggested for the surface demineralization is that during the bleaching procedure the pH of the whitening agent becomes more acidic and the hydrogen ions attack the enamel crystals, freeing calcium and phosphate ions from the enamel surface. Several important deductions can be made from this study: 1. Aggressive bleaching can lead to surface demineralization and reduction of enamel crystallinity; 2. Cold-light activation seems to have little effect on color change or tooth structure; and 3. Hydrogen peroxide reduces the pH on the tooth surface during treatment, leading to surface demineralization 1.
Summary
When manufacturer’s instructions are followed, hydrogen peroxide and carbamide peroxide based tooth whitening is safe and effective.
Home-based bleaching (following manufacturer’s instructions) results in less tooth sensitivity than in-office bleaching. Whereas in-office bleaching of restored teeth using a 35 % hydrogen peroxide product caused tooth sensitivity in all cases.
The studies reviewed above on the persistence of whitening treatments found that light activation had no effect on the bleaching when high concentrations of hydrogen peroxide (25–35%) were employed. The efficacy of light activation is controversial with numerous studies finding both improvement in short term and long term whitening as well as studies that find no effect on whitening at all.
The degree of bleaching obtained with a home-bleaching technique using 10 % carbamide peroxide gel applied via a tray was similar to that obtained with the in-office technique that applied 35 % hydrogen peroxide, regardless of light irradiation or the combination of home/in-office techniques 16.
Aggressive bleaching with high concentrations of hydrogen peroxide office-based products causes enamel softening, surface roughness, and an increase in the susceptibility of the tooth to demineralization, based upon laboratory test findings.
Following a regimen consisting of in-office bleaching for two sessions with a 1-week interval, followed by home bleaching once a month for 3 months gave more persistence in color change over a 6-month period than in-office bleaching alone 13. This later study shows that this regimen for whitening maintenance can extend the effectiveness of the whitening treatment. Therefore the optimal regimen to obtain persistence of tooth whitening is to follow an in-office treatment with monthly home-based touch-up treatments using over-the-counter products. Dental restorations are susceptible to unacceptable color change even when using the home-based over-the-counter systems. Teeth with restorations have a significantly greater chance of becoming sensitive and result in a greater degree of pain when exposed to whitening regimens.
Lastly, there are certain risks associated with teeth whitening such as increased teeth sensitivity, teeth surface roughening and softening, increased potential for teeth demineralization, degradation of dental restorations, unacceptable color change of dental restorations and gingival irritation. You should be aware of the risks associated with teeth whitening and learn to identify adverse occurrences so that you may seek professional help when required.
Supervision of the tooth whitening strategy by an oral healthcare professional will reduce the potential risks and optimize benefits of tooth bleaching 21.
References- Carey CM. Tooth Whitening: What We Now Know. The journal of evidence-based dental practice. 2014;14 Suppl:70-76. doi:10.1016/j.jebdp.2014.02.006. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4058574/
- Are snow-white teeth really so desirable? Christensen GJ J Am Dent Assoc. 2005 Jul; 136(7):933-5. https://www.ncbi.nlm.nih.gov/pubmed/16060475/
- Yu H, Li Q, Wang Y, Cheng H. Effects of temperature and in-office bleaching agents on surface and subsurface properties of aesthetic restorative materials. J Dent. 2013;41:1290–1296. https://www.ncbi.nlm.nih.gov/pubmed/23927898
- Kurtulmus-Yilmaz S, Cengiz E, Ulusoy N, Ozak ST, Yuksel E. The effect of home-bleaching application on the color and translucency of five resin composites. J Dent. 2013;41S:e70–e75. https://www.ncbi.nlm.nih.gov/pubmed/23313829
- Bonafe E, Bacovis CL, Iensen S, Loguercia AD, Reis A, Kossatz S. Tooth sensitivity and efficacy of in-office bleaching in restored teeth. J Dent. 2013;41:363–369. https://www.ncbi.nlm.nih.gov/pubmed/23357647
- American Academy of Cosmetic Dentistry; Teeth Whitening. http://www.aacd.com/index.php
- Journal of the American Dental Association July 2005; Volume 136, Issue 7, Pages 933–935. http://jada.ada.org/article/S0002-8177(14)63062-2/fulltext
- Leonard RH Jr, Bentley C, Eagle JC, Garland GE, Knight MC, Phillips C. J Esthet Restor Dent. 2001;13(6):357-69. Nightguard vital bleaching: a long-term study on efficacy, shade retention. side effects, and patients’ perceptions. https://www.ncbi.nlm.nih.gov/pubmed/11778855
- External bleaching therapy with activation by heat, light or laser–a systematic review. Buchalla W, Attin T. Dent Mater. 2007 May; 23(5):586-96. https://www.ncbi.nlm.nih.gov/pubmed/16820199/
- Oper Dent. 2011 Sep-Oct;36(5):460-6. doi: 10.2341/10-159-C. Epub 2011 Aug 22. A clinical study comparing the efficacy and sensitivity of home vs combined whitening. http://www.jopdentonline.org/doi/10.2341/10-159-C?url_ver=Z39.88-2003
- He LB, Shao MY, Tan K, Xu X, Li JY. The effects of light on bleaching and tooth sensitivity during in-office vital bleaching: a systematic review and meta-analysis. J Dent. 2012;40:644–653. https://www.ncbi.nlm.nih.gov/pubmed/22525016
- Clin Oral Investig. 2016 Jan;20(1):1-14. doi: 10.1007/s00784-015-1547-8. Epub 2015 Aug 7. Efficacy and safety of over-the-counter whitening strips as compared to home-whitening with 10 % carbamide peroxide gel–systematic review of RCTs and metanalysis. https://link.springer.com/article/10.1007%2Fs00784-015-1547-8
- Al Quran FAM, Mansour Y, Al-Hyarl S, Al Wahadnl A, Mair L. Efficacy and persistence of tooth bleaching using a diode laser with three different treatment regimens. Eur J Esthet Dent. 2011;6:436–445. https://www.ncbi.nlm.nih.gov/pubmed/22238726
- Wiegand A, Drebenstedt S, Roos M, Magalhaes AC, Attin T. 12-Month color stability of enamel, dentine, and enamel-dentine samples after bleaching. Clin Oral Invest. 2008;12:303–310. https://www.ncbi.nlm.nih.gov/pubmed/18369668
- Hahn P, Schondelmaier N, Wolkewitz M, Altenburger MJ, Polydorou O. Efficacy of tooth bleaching with and without light activation and its effect on the pulp temperature: an in vitro study. Odontol. 2013;101:67–74. https://www.ncbi.nlm.nih.gov/pubmed/22395767
- Bernardon JK, Sartori N, Ballarin A, Perdigao J, Lopes G, Baratieri LN. Clinical performance of vital bleaching techniques. Oper Dent. 2010;35:3–10. https://www.ncbi.nlm.nih.gov/pubmed/20166405
- Undesirable and adverse effects of tooth-whitening products: a review. Goldberg M, Grootveld M, Lynch E. Clin Oral Investig. 2010 Feb; 14(1):1-10. https://www.ncbi.nlm.nih.gov/pubmed/19543926/
- Tompkins AM, Coleman SS, Carey CM. Erosive Capacity of Five Commercial Bleaching Products on Human Enamel. J Dent Res. 2014;93(Spec Iss A
- Ogura K, Tanaka R, Shibata Y, Miyazaki T, Hisamitsu H. In vitro demineralization of tooth enamel subjected to two whitening regimens. J Am Dent Assoc. 2013;144:799–807. https://www.ncbi.nlm.nih.gov/pubmed/23813261
- Shi X-C, Ma H, Zhou J-L, Li W. The effect of cold-light-activated bleaching treatment on enamel surfaces in vitro. Internat J Oral Sci. 2012;4:208–213. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3633061/
- Safety issues of tooth whitening using peroxide-based materials ((Li Y, Greenwall L. Safety issues of tooth whitening using peroxide-based materials. Brit Dent J. 2013;215:29–4. https://www.ncbi.nlm.nih.gov/pubmed/23846062/





{kind=link}