
What is an abdominal migraine
Abdominal migraine is a common cause of chronic and recurrent abdominal pain in children 1. Abdominal migraine is characterized by episodic attacks of moderate to severe abdominal pain lasting ≥1 hour that is midline, periumbilical, or diffuse in location and accompanied by other symptoms including headache, anorexia, nausea, vomiting, photophobia or pallor 1. Abdominal migraine episodes are separated by weeks to months and there is a stereotypical pattern and symptoms in each patient 1. The pain is severe enough to interfere with normal daily activities. After appropriate medical evaluation, symptoms cannot be attributed to any other medical condition. Most often, there is a family history of migraine and it has a strong propensity to evolve into migraine headaches in adulthood 1.
Abdominal migraine is a poorly understood disorder largely due to a limited recognition of this condition by the medical community 2. The pathophysiology of abdominal migraine remains unclear and as a result treatment for this condition is suboptimal with avoidance of triggers and prophylactic treatment currently recommended when an episode begins.
Chronic abdominal pain in occurs in 11%–15% of children and adolescents 3 and accounts for 2%–4% of office visits to primary care clinicians and 50% of referrals to pediatric gastroenterologists 4. The overall prevalence of abdominal migraine is ~1%–9% 5. Abdominal migraine is most commonly seen in children aged 4–15 years. The average age of diagnosis is 3–10 years with peak incidence at 7 years 6. Most of the studies have shown a higher prevalence in girls compared to boys, similar to other functional gastrointestinal disorders and cephalic migraine 7. A few studies have shown equal prevalence in girls and boys 8.
Chronic and recurrent abdominal pain is a very distressing symptom that causes significant morbidity in affected children impairing their school performance and overall quality of life 9. Abdominal migraine is one of the most common causes of functional (unknown cause) abdominal pain in children, affecting up to 4% of the pediatric population 2 and is included under the Rome IV classification of functional gastrointestinal disorders 9. Abdominal migraine is also currently well recognized as a type of pediatric migraine variant and has specific diagnostic criteria under the International Classification of Headache Disorders III 2. Despite the presence of well-defined diagnostic criteria, abdominal migraine is still a lesser known entity and is underdiagnosed by both general pediatricians and pediatric gastroenterologists 10. Whilst abdominal migraine is not believed to continue into adulthood for the majority of children, it has the propensity to develop into probable migraine and recurrent abdominal pain in adulthood 2.
In 2006, Carson et al 10 conducted a retrospective chart review on children aged 1–21 years who were referred to an academic pediatric gastroenterology center with chief complaint of recurrent abdominal pain. International Classification of Headache Disorders II criteria were used to identify patients with abdominal migraine who met the diagnostic criteria. Of the 548 patients who met the inclusion criteria, 4.4% (20) met the International Classification of Headache Disorders II criteria for abdominal migraine. Another 50 (11%) had documentation lasting at least one criterion, but were otherwise consistent with abdominal migraine (probable abdominal migraine). Thus, abdominal migraine represented 4%–15% of children with chronic, idiopathic, recurrent abdominal pain. They also pointed out the “transAtlantic dissociation” of abdominal migraine. During the assessment period from January 2006 to December 2007, none of the children in the Pediatric Gastroenterology Clinic received a diagnosis of abdominal migraine. Most of the literature pertaining to abdominal migraine comes from Europe and UK and there are very little data from the USA 1. They hypothesized that there is inadequate awareness about abdominal migraine among clinicians in USA leading to underdiagnosis of the condition.
A 2008 study compared the prevalence of various functional gastrointestinal disorders in children with chronic, idiopathic abdominal pain using Rome II and Rome III criteria 11. The frequency of diagnosis of abdominal migraine in patients with chronic abdominal pain increased from 5% to 23% when using Rome III criteria. This proves that Rome III criteria had a more positive predictive value (100%) and a low negative predictive value (7.7%). This might have led to incorrect diagnosis of other functional abdominal pain disorders as abdominal migraine.
There have been no new studies reported so far that looked at the prevalence and other epidemiological characteristics of abdominal migraine based on Rome IV criteria released in 2016 1.
Abdominal migraine triggers
- Bright or flickering light
- Poor sleep
- Travel
- Prolonged fasting
- School or family stressors
- Dietary triggers (citrus food, caffeine, cheese, chocolate, carbonated drinks, colorings and flavorings)
Abdominal migraine prognosis
Abdominal migraine is considered as a precursor to cephalic migraine although abdominal pain is proven to resolve completely in most of the patients. Dignan et al 12 studied 54 patients with diagnosis of abdominal migraine and followed them up for 10 years. Abdominal pain symptoms had resolved completely in 61% cases. In all, 70% developed migraine with or without aura compared with 20% of the matched control group. abdominal migraine can also rarely persist in adulthood 13. Longitudinal studies are needed to study long-term prognosis and the course of childhood abdominal migraine into adulthood.
Abdominal migraine symptoms
Episodic bouts of intense periumbilical, midline, or diffuse abdominal pain lasting ≥1 hour. The symptoms cannot be fully explained by another medical condition. The abdominal pain may be associated with at least two of the following features: anorexia, nausea, vomiting, headache, photophobia, or pallor. Stereotypical pattern and symptoms are seen in the individual patient. At least two episodes in a 6-month period are needed to confirm the diagnosis.
Association with migraine
Abdominal migraine shares many clinical, epidemiologic, and pathophysiologic similarities with cephalic migraine 14. The International Headache Society included abdominal migraine in the International Classification of Headache Disorders classification in 2002. A history of migraine headache in a first-degree relative is described in 34%–90% of patients. A personal history of migraine headaches is seen in 24%–47% of patients. abdominal migraine and cephalic migraine also share common triggers and also similar relieving factors. abdominal migraine has been clearly shown to be a precursor to the development of migraine with and without aura. Also, many of the treatment strategies for migraine have been found to be effective in patients with abdominal migraine.
A 1995 study by Abu-Arafeh and Russell 15 reviewed the prevalence and clinical features of children with migraine and abdominal migraine. One hundred and fifty nine children with migraine and 58 children with abdominal migraine were included in the study. They concluded that patients with migraine and abdominal migraine shared many similarities to suggest a common pathogenesis. The prevalence of migraine in children with abdominal migraine was 24%, which was twice the prevalence of migraine in the general population (10%). Conversely, among children with migraine the prevalence of abdominal migraine was 9%, which was again twice the prevalence of abdominal migraine in the general population (4.1%). Also, a family history of migraine in a first-degree relative was twice as common in patients with abdominal migraine when compared to controls (34% vs 17%). Also, patients in the two groups had similar relieving and triggering factors and similar recurrent-associated symptoms.
A study by Good 16 showed that cyclic vomiting syndrome, abdominal migraine, and migraine with and without aura share many neurophysiologic similarities including abnormal vision-evoked electroencephalography (EEG)-beta activity, high-frequency photics following responses, and visual event-related potentials. This further supports the classification of abdominal migraine as a true migraine equivalent.
Of note, migraine is associated with other GI disorders that can be misdiagnosed as abdominal migraine. Prevalence of migraine is significantly high in patients with celiac disease 17. Children with migraine can present with abdominal pain and irritable bowel syndrome (IBS)-like symptoms 17.
Association with other pediatric migraine equivalents
Pediatric migraine variants are a group of paroxysmal, periodic syndromes occurring in patients who have migraine with or without aura, or have an increased propensity to develop migraine. It was previously called childhood periodic syndromes, recurrent pain syndromes, migraine equivalents, or migraine precursors 18.
Abdominal migraine, cyclic vomiting syndrome, benign paroxysmal vertigo, and benign paroxysmal torticollis are episodic syndromes that are associated with migraine headaches 18. Abdominal migraine and cyclic vomiting syndrome were initially thought to be a single disorder and the names were used interchangeably 19. It was later recognized that they are two separate entities 20. As mentioned earlier, abdominal migraine and cyclic vomiting syndrome have common electrophysiological characteristics 16.
Although no association has been shown between abdominal migraine and benign paroxysmal vertigo (BPPV), some link has been noted between motion sickness and abdominal migraine. Farqahar et al 21 reviewed the characteristics of a set of children with symptoms suggestive of abdominal migraine. He observed that motion sickness was a common complaint in these patients and their families although it was not formally analyzed. A link with motion sickness was further noted in epidemiologic studies conducted in 1983 and 1993 22. Of note, these studies were done when there were no clear guidelines to diagnose abdominal migraine. Also, there was no specific demarcation between cyclic vomiting syndrome and abdominal migraine at that time. Hence, the validity of these observations needs to be further elucidated.
Association with other functional abdominal pain disorders
Abdominal migraine belongs to the class of functional abdominal pain disorders under Rome IV classification of functional gastrointestinal disorders. The other disorders included are functional dyspepsia, IBS, cyclic vomiting syndrome, and functional abdominal pain – not otherwise specified. Many of the mechanisms postulated under pathogenesis of abdominal migraine, especially the visceral hyperalgesia theory, have been studied mostly in patients with functional gastrointestinal disorders (IBS and functional dyspepsia, in particular) 23. Helgeland et al noted that symptoms of IBS and abdominal migraine overlapped in 33% patients as per the Rome III criteria 24. Clinical association between abdominal migraine and other functional gastrointestinal disorders needs to be evaluated further in research studies as it may open new avenues in the treatment of abdominal migraine.
Association with atopy and food sensitivity
Studies have shown a correlation between abdominal migraine and atopy. Patients with cephalic migraine have a higher incidence of atopy and other allergic disorders 25. In addition, dietary modification is central in the management of abdominal migraine in a similar way as in cephalic migraine 26.
Bentley et al 8 in 1995 studied the response of 12 patients with symptoms suggestive of abdominal migraine to a modified dietary regimen avoiding potential allergens. Ten out of the 12 patients (83%) became symptom free or had diminished symptoms with dietary changes. Five out of 12 patients (41%) had a history of eczema, hay fever, or other forms of atopy.
Abdominal migraine clinical features and diagnostic criteria
Abdominal migraine is a well-recognized entity with specific diagnostic criteria under International Classification of Headache Disorders III (beta version) released in 2013 and Rome IV diagnostic criteria published in 2016 27. Abdominal migraine is included under “episodic syndromes that may be associated with migraine” under the International Classification of Headache Disorders classification 28. The International Classification of Headache Disorders defines abdominal migraine as an idiopathic cause of moderate to severe chronic, recurrent abdominal pain that is midline, periumbilical, or poorly localized, dull or just sore in quality. Attacks usually last 2–72 hours when not treated successfully or without treatment. Patient is completely free of symptoms between attacks. Patient has at least two associated symptoms among anorexia, nausea, vomiting, and pallor during the attack. At least five “pain episodes” are needed to fulfill the diagnosis.
Abdominal migraine is also included under the Rome classification of functional gastrointestinal disorder and Rome IV criteria recently published in May 2016 24. As per Rome IV, abdominal migraine is characterized by paroxysmal episodes of intense periumbilical, midline, or diffuse abdominal pain lasting ≥1 hour. Abdominal pain is the most severe and distressing symptom and is incapacitating and interferes with normal activities. After appropriate evaluation, symptoms cannot be fully explained by another medical condition. The abdominal pain may be associated with at least two of the following features: anorexia, nausea, vomiting, headache, photophobia, or pallor. Stereotypical pattern and symptoms are seen in the individual patient. At least two episodes in a 6-month period are needed to confirm the diagnosis.
The two criteria differ in several aspects including the number of episodes required to make the diagnosis and also the duration of each painful episode. As per International Classification of Headache Disorders III criteria, the patient has to be completely symptom free between the episodes. Rome IV uses the phrase “episodes are separated by weeks to months” to account for baseline gastrointestinal symptoms and avoid confusion in parents (this replaces the phrase “return to baseline health” in Rome III criteria). Rome IV criteria also remove the dictum that functional gastrointestinal disorder can only be diagnosed after organic diseases are excluded. The usage of “no evidence of organic disease” in Rome III has been replaced with “after appropriate evaluation, symptoms cannot be fully explained by another medical condition.” This change allows the clinician to make the diagnosis of abdominal migraine with selective or no testing. Having a diagnosis of abdominal migraine does not exclude the presence of other functional abdominal pain disorders for symptoms outside of the episodes.
The average duration of episodes is 1–17 hours and the average number of episodes per month varies from 2 to 20 29. Some patients may have more than one episode per day. Headache is the most common associated symptom.
Abdominal migraine causes
There are several hypotheses that have been postulated to explain the pathophysiology of abdominal migraine but none of them have been definitively confirmed.
Visceral hyperalgesia hypothesis
Visceral hypersensitivity is the most definitive and unifying theory explaining the pathophysiology of all functional gastrointestinal disorders 30. This theory is based on the strong association between the enteric nervous system and central nervous system (CNS) and their common embryonic origin. Patients with functional gastrointestinal disorders have a low threshold for nociceptive stimuli. A variety of ill-defined factors including genetic, environmental, psychosocial (early stressors in life) etc predispose an individual to visceral hyperalgesia. Postulated mechanisms for visceral hyperalgesia include sensitization of primary sensory neurons and central spinal neurons, altered descending inhibitory control, and impaired stress response. This in turn causes alteration of bowel–gut axis and causes abnormal secretion of excitatory neurotransmitters such as serotonin. Serotonin plays a key role in the regulation of gastrointestinal (GI) motility, secretion, and sensation. The bidirectional communication between the brain–gut neurons through various neural and hormonal circuits may lead to changes in the central nervous system (CNS) and cause other associated symptoms such as headache. Stimulation of the autonomic nervous system and sympathetic hyperactivity may account for symptoms such as pallor. Novel imaging techniques such as functional magnetic resonance imaging have shown defective visceral pain processing pathways in patients with functional gastrointestinal disorder.
Although, the theory of visceral hyperalgesia has not been specifically proven in patients with abdominal migraine, it is the most evidence-based explanation for all functional gastrointestinal disorders.
Altered gut motility hypothesis
Patients with abdominal migraine may have abnormal gut motility. It is postulated that functional abdominal pain results from distension of the gastrointestinal tract and abnormal contractions which cause hyperalgesia.
A study conducted in a tertiary referral center in Sri Lanka from 2007 to 2012 looked at gastric motility parameters in 17 children aged 4–12 years with abdominal migraine compared to healthy controls 29. They found that gastric emptying rate and antral motility parameters were significantly lower in children with abdominal migraine. Gastric emptying rate had a significant negative correlation with the average duration of pain episodes. The amplitude of antral contractions negatively correlated with scores obtained for severity of symptoms. These findings suggest a possible role of abnormal gastric motility in the pathogenesis of abdominal migraine.
Altered gut permeability hypothesis
Gut permeability may be altered in patients with abdominal migraine. Mucosal permeability is an indirect function of gut health. A study conducted by Bentley et al 8 in 1995 compared the gut mucosal permeability between 11 children with diagnosis of abdominal migraine and healthy controls. They found that gut mucosal permeability was significantly increased in patients with abdominal migraine when compared to healthy controls. Three patients were followed longitudinally over 3 years with follow-up tests three times a year. They noticed that the gut mucosal permeability decreased with symptomatic improvement and vice versa. This might explain why nonsteroidal anti-inflammatory drugs (NSAIDs) are not beneficial in patients with abdominal migraine; as these drugs increase mucosal permeability. However, no further research has been conducted to test this hypothesis and its implications in the management of children with abdominal migraine. Of note, this study was done before specific guidelines were published for the diagnosis of abdominal migraine.
Diet-induced allergy and altered mucosal immunity hypothesis
Dietary factors may also contribute to the symptoms of abdominal migraine 8. The role of diet in patients with cephalic migraine has been extensively studied 31. The incidence of cephalic migraine is significantly higher in patients with atopy and other allergic disorders. Certain dietary allergens might trigger mucosal immune responses and manifest the symptoms of abdominal migraine in susceptible individuals. This hypothesis is further supported by the response of some patients with abdominal migraine to an oligoantigenic diet with elimination of potential allergens 32.
In 1995, Bentley et al compared IgE levels and positive radioallergosorbent (RAST) tests in 14 patients with abdominal migraine and healthy controls 8. No significant decrease in IgE levels and positive radioallergosorbent (RAST) test rate was noted in patients with abdominal migraine when compared to the control group. Also, no dietary allergens could be identified via a skin prick test in these patients. This could be because abdominal migraine causes selective activation of gut mucosal immune response rather than systemic immunity.
In vitro studies have shown that enterocytes can express MHC class II antigen and secrete specific chemokines to stimulate epithelial lymphocytes and activate an immune response under the influence of dietary antigens; more recently, there has been evidence showing that the mucosal immune system is the master regulator of the gut–brain axis 33. The adaptive immune system (T-cells in particular) and the innate immune system (mucosal lymphoid cells, mast cells, and mononuclear phagocytic cells) play a key role in maintaining gut–brain homeostasis and are disrupted in patients with functional gastrointestinal disorders. A disrupted immune system is involved in the pathogenesis of cephalic migraine as well 34.
Further research specifically focused on altered immune responses in patients with abdominal migraine would help in identifying new treatment strategies.
Abnormal neuroregulation hypothesis
Abnormalities in the metabolism of neurotramitters causing an imbalance between excitatory amino acids and inhibitory amino acids have been well studied in cephalic migraine 35. A similar mechanism might be involved in the pathogenesis of abdominal migraine 16. In the CNS, glutamic acid and aspartic acid are the main excitatory neurotransmitters, whereas gamma aminobutyric acid (GABA) is the inhibitory neurotransmitter. The balance between these two systems regulates the function of other circuits of the brain involving dopamine, serotonin, and norepinephrine. CNS hyperexcitability plays a central role in the pathogenesis of cephalic migraine. Several factors (genetic, environmental, dietary, psychosocial stressors) activate the trigeminovascular system and cause the release of inflammatory neuropeptides and neurotrasmitters including catecholamine gene-related peptide, substance-P, serotonin, adenosine diphosphate, platelet activating factor, nitric oxide resulting in migraine headache. A similar mechanism involving increased activity of excitatory amino acids might play a role in the pathogenesis of abdominal migraine. This can explain the possible efficacy of certain medications that increase GABA (valproate) in patients with abdominal migraine 36.
Phenol sulfotransferase enzymes (S and P) are key enzymes involved in the metabolism of catecholamines and other amine neurotransmitters. Activity of the enzyme is significantly decreased in patients with diet-induced migraine 37. This results in an accumulation of inflammatory neuropeptides and neurotransmitters that activate the migraine cascade. The enzyme is also inhibited by several dietary constituents including cheese, red wine etc which can all precipitate migraine headache. In 1995, Bentley et al reviewed the platelet expression of these two isoenzymes (phenol sulfotransferase S and P) in 21 patients with abdominal migraine when compared to normal subjects 8. No significant change in enzyme activity was noted in the two groups. The level of enzyme activity in platelets might not be a true reflection of levels in the enteric nervous system. However, more studies are needed to confirm this hypothesis.
Genetic mutations and polymorphisms of genes, which are still not well defined, regulate ion channels, neurotransmitter metabolism, and mitochondrial metabolism in the CNS and contribute to the pathophysiology of migraine headaches 38. There is a strong genetic predisposition to the development of functional abdominal pain as well 4. A 2017 study found evidence suggesting Y2 receptor antagonism and YY gene deletion may be related to visceral hyperalgesia 39. The contribution of genetic factors to abdominal migraine is further supported by the presence of family history of migraine or chronic abdominal pain in most of the patients 15. However, more research is needed to identify these factors.
Menstrual cycle, pregnancy, lifestyle, diet, anxiety, chronic stress etc are the major psychosocial factors contributing to cephalic migraine 40. Stress and anxiety also play a role in the pathogenesis of functional gastrointestinal disorders 4. The role of these factors in abdominal migraine needs to be reviewed in further studies.
Other postulated theories
Autonomic instability, disturbances in the hypothalamus– pituitary axis, altered intestinal microbiome, small intestinal bacterial overgrowth, acute infectious diseases with chronic changes, lactose intolerance, and abnormal mitochondrial function are the other theories that have been proposed in the pathogenesis of functional gastrointestinal disorders and cephalic migraine 41. More research focused on pathophysiology of abdominal migraine needs to be performed to validate the role played by these different factors.
Abdominal migraine diagnosis
Abdominal migraine is a subjective diagnosis based on specific symptom-based guidelines as outlined by International Classification of Headache Disorders III and Rome IV. There are no proven objective markers to correctly make the diagnosis 42. Abnormal EEG changes with visual stimulation have been noted in patients with abdominal migraine 16. However, these changes are nonspecific and need further validation. A complete history and physical examination are of utmost importance. A thorough dietary and social history check should be obtained and the growth charts should also be evaluated. Patients should be carefully evaluated for the presence of any potential alarming symptoms or signs (Table 1). Further testing and imaging studies (as outlined in Table 2) should be reserved specifically for patients in whom there are alarm symptoms or if there is a high suspicion of an organic disease. It is a common misconception that further testing reduces anxiety. On the other hand, negative test results reinforce the fear of an unknown organic disease and worsen anxiety in both the patient and family.
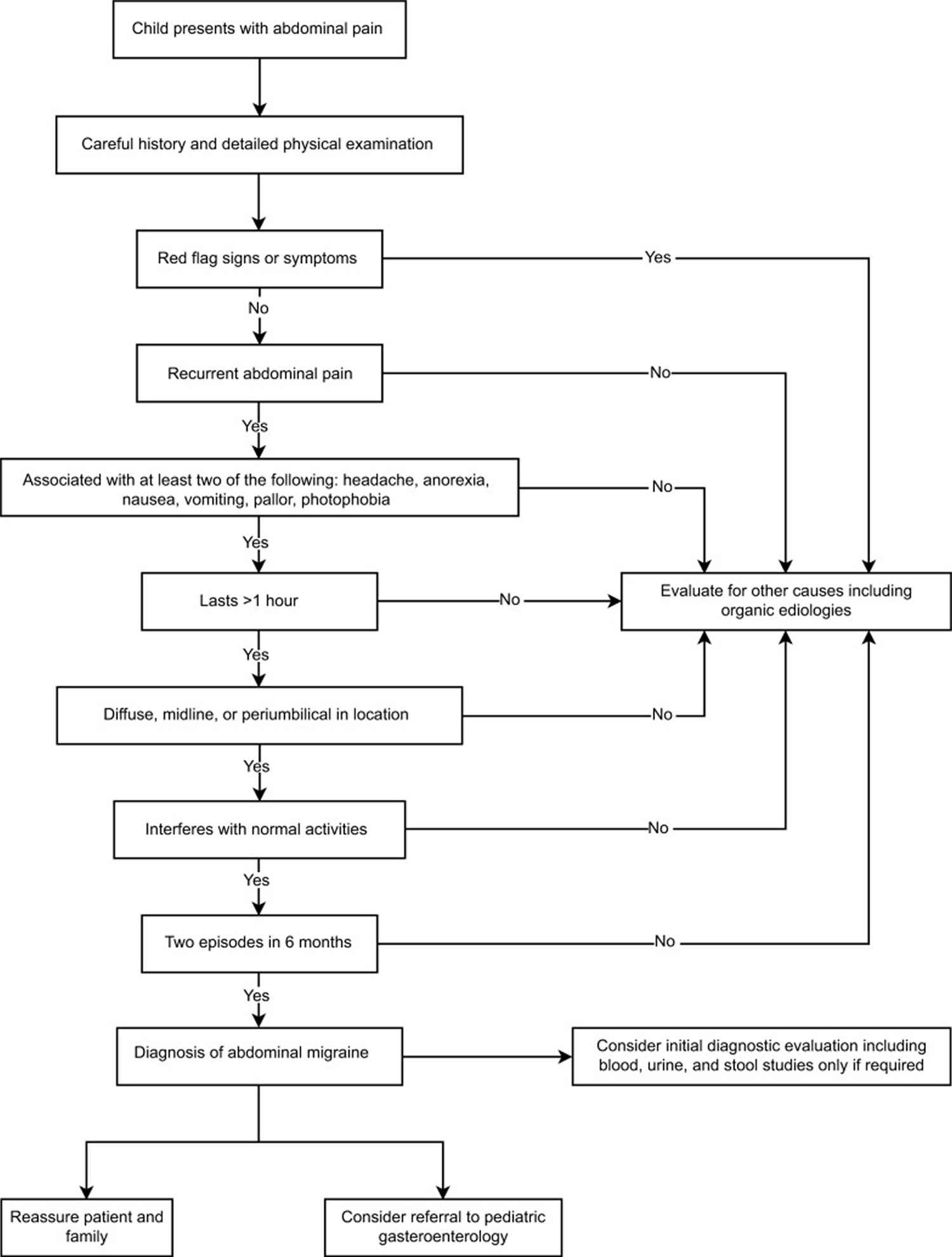
Scicchitano et al 43 proposed an algorithm in 2014 to achieve a timely diagnosis of abdominal migraine which was modified based on the updated Rome IV guidelines (Figure 1). If the diagnosis is still unclear or if there is any suspicion of an organic pathology, the patient should be referred to a pediatric gastroenterologist. To summarize, a comprehensive history and physical examination with judicious use of diagnostic tools would be optimal in making a diagnosis of abdominal migraine.
Table 1. Alarm symptoms and signs in children with abdominal migraine
| Alarm symptoms |
| Persistent right upper or right lower quadrant pain |
| Pain radiating to back |
| Persistent or bilious vomiting |
| Gastrointestinal blood loss |
| Hematuria |
| Chronic and unexplained diarrhea |
| Involuntary weight loss |
| Recurrent or unexplained fever |
| Dysphagia |
| Hematochezia, melena |
| Occult gastrointestinal blood loss |
| Nocturnal symptoms |
| Unexplained fever |
| Family history of inflammatory bowel disease, celiac disease, or familial |
| Mediterranean fever |
| Dysuria |
| Delayed puberty |
| Joint pain or joint swelling |
| Alarm signs |
| Deceleration of linear growth |
| Signs of peritonitis (rebound, guarding) |
| Leucocytosis |
| Hypoalbuminemia |
| Localized abdominal tenderness, away from umbilicus |
| Elevated inflammatory markers |
| Uveitis |
| Oral lesions |
| Icterus |
| Pallor |
| Rash with no identifiable cause |
| Organomegaly including hepatomegaly or splenomegaly |
| Arthritis |
| Costovertebral angle tenderness |
| Tenderness over the spine |
| Perianal abnormalities – anal skin tags, fissures |
Table 2. Diagnostic studies that should be considered in children presenting with chronic and recurrent abdominal pain
| Blood studies |
| Full blood count |
| Erythrocyte sedimentation rate |
| C-reactive protein |
| Electrolytes |
| Urea and creatinine |
| Glucose |
| Liver function tests |
| Amylase and lipase |
| Celiac antibodies |
| Pregnancy test |
| Urine and stool studies |
| Urinalysis with microscopy, culture, and sensitivity |
| Stool occult blood and microscopy |
| Stool test for Helicobacter pylori antigen |
| Fecal calprotectin |
| Radiological studies |
| Abdominal X-ray |
| Ultrasound of the abdomen and pelvis |
| Contrast study of upper gastrointestinal tract and small bowel |
| Magnetic resonance imaging of brain |
| Endoscopic procedures |
| Esophagogastroduodenoscopy |
| Colonoscopy |
Figure 1. Abdominal migraine diagnostic algorithm
Abdominal migraine treatment
There are no definitive guidelines for the management of abdominal migraine due to extreme paucity of studies in the literature 44. Most of the treatment options are based on few studies in relatively small numbers of children, anecdotal evidence, and close association of abdominal migraine with migraine headaches and functional gastrointestinal disorders 44. The present treatment options are summarized in Table 3. Nonpharmacotherapeutic interventions including explanation and reassurance, avoidance of triggers, and dietary modifications should be the initial step in management. Drug therapy should be considered only when these primary interventions fail 43.
Table 3. Treatment of abdominal migraine
| Nonpharmacologic therapy |
| Explanation and reassurance |
| Avoidance of triggers |
| Modified diet |
| Psychotherapy |
| Pharmacotherapy |
| Abortive therapy |
| Intranasal sumatriptan |
| IV valproate |
| Prophylactic therapies |
| Beta blocker: propranolol |
| 5-HT antagonists: cyproheptadine |
| Calcium channel blockers: flunarizine |
| 5-HT agonist with antihistamine properties: pizotifen |
Abbreviations: IV = intravenous; HT = hydroxytryptamine (serotonin).
Non pharmacotherapy
Explanation and reassurance
Explanation and reassurance in a biopsychosocial model of care should be the initial step once a clinical diagnosis of abdominal migraine is made 43. The parent/child dyad should be educated about the episodic nature of the illness, presence of possible triggers and relieving factors, association with migraine and other functional gastrointestinal disorders, and prognosis of the disease based on available data. The absence of any organic abdominal pathology should be reiterated. In addition, a positive outlook that abdominal migraine is eventually expected to improve on its own in most children will help cope with symptoms.
Avoidance of triggers
abdominal migraine and migraine share many common triggers as shown in previous studies 15. Many patients report improvement by avoiding triggers such as stress, travel, exercise, flickering lights, prolonged fasting, and alteration of sleep pattern. Russell et al observed that abdominal migraine that starts early in the morning can be prevented by taking a breakfast cereal before going to bed 45. This “breakfast at bedtime” should consist of a high-fiber cereal to prolong its glycemic effect. Further studies are needed to confirm its efficacy.
Dietary management
Dietary modifications recommended in migraine may also be effective in patients with abdominal migraine. Avoidance of dietary triggers may be helpful in some patients. A diet low in amines may also aid in reducing the frequency and severity of attacks. An oligoantigenic diet or few foods diet may be helpful in patients having frequent bouts of abdominal pain 46 This is implemented by restricting the diet initially and gradually reintroducing foods in an attempt to identify specific foods that may be affecting the individual patient. Russell et al 45 reported a favorable outcome in 17 out of 22 patients (77%) treated with an oligoantigenic diet.
A high-fiber diet may also be effective in some patients with recurrent abdominal pain.63 Probiotics have been found to be effective in patients with functional abdominal pain disorders, especially IBS and functional dyspepsia.63 Lactose intolerance has been noted in some patients with chronic abdominal pain and a lactose-free diet is effective in this subgroup 4. However, further research needs to be carried out to study the efficacy of these treatment options in children with abdominal migraine.
Behavior therapy
Psychotherapy, specifically cognitive behavior therapy, may be effective in patients with abdominal migraine. The biopsychosocial model of origin of functional abdominal pain suggests that psychological interventions may be helpful in these patients. Hypnotherapy, family therapy, and yoga have been found to be beneficial in children with functional abdominal pain, IBS in particular 47. More studies focused specifically on abdominal migraine need to be carried out to prove the efficacy of these treatment options.
Abdominal migraine medications
Medications is reserved for patients with frequent, severe symptoms or for those patients who do not respond well to nonpharmacological interventions 48. As there is no objective measurement of disease severity, the decision to start drug therapy is based on the clinician’s judgment and receptiveness of the family to various treatment options. Studies related to the use of these drugs in abdominal migraine are summarized in Table 4.
Abortive therapy
Triptans (5-hydroxytryptophan 1 A/D agonists) have been found to be effective for abortive therapy. Intranasal sumatriptan therapy has been studied in patients with abdominal migraine 49. Almotriptan has been found to be effective in patients with pediatric migraine 50. However, no studies have been conducted on patients with abdominal migraine. The efficacy of NSAIDs and acetaminophen needs to be studied with well-designed randomized control trials.
Preventive drug therapy
Beta blockers (propranolol), calcium channel blockers (flunarizine), serotonin antagonists (cyproheptadine, pizotifen), and GABA agonists (valproate) are the most common drugs that have used in patients with abdominal migraine 51 These drugs have been found to be effective in patients with cephalic migraine and hence were tried in patients with abdominal migraine due to similarities in their pathogenesis.
Scicchitano et al 43 recommend propranolol as the first-line choice of drug therapy when non-pharmaceutical interventions fail. Cyproheptadine is recommended as the second-line agent when propranolol is ineffective or contraindicated.
Table 4. Abortive and prophylactic therapy in abdominal migraine
| Study | Mechanism of action | Type of study | Participants | Interventions | Results |
|---|---|---|---|---|---|
| Abortive therapy with sumatriptan (Kakisaka et al)49 | Serotonin/5-hydroxytryptophan agonist (5-HT ID) | Case report (2010) | 1 child with abdominal migraine | Intranasal sumatriptan for acute attack of abdominal pain | Complete resolution of pain |
| Abortive therapy with IV valproate (Tan et al)52 | GABA agonist | Case report (2006) | 2 children with abdominal migraine | IV valproate | Symptomatic relief |
| Prophylactic therapy with cyproheptadine (Madani et al)51 | First-generation antihistamine with anti-serotoninergic and calcium channel blocking properties | Retrospective study (2016) | 18 children with abdominal migraine | 0.13–0.2 mg/kg/day | 72% of patients with improvement in symptoms |
| Prophylactic therapy with flunarizine (Kothare)53 | Calcium channel blocker | Clinical trial (2005) | 8 children with abdominal migraine | 7.5 mg daily PO | 61% reduction in frequency and 51% reduction in duration |
| Prophylactic therapy with propranolol vs cyproheptadine (Worawattanakul et al)44 | Propranolol – beta blocker Cyproheptadine – first-generation antihistamine with anti-serotoninergic and calcium channel blocking properties | Retrospective study (1999) | 36 children with abdominal migraine (12 treated with cyproheptadine; 24 treated with propranolol) | Cyproheptadine 0.25–0.5 mg/kg/day of propranolol 10–20 mg BID–TID | 33% complete resolution, 50% fair response, 17% no response 75% excellent response, 8% fair response, 17% no response |
| Prophylactic therapy with pizotifen syrup (Symon and Russell)54 | Serotonin antagonist (5-HT 2A and 2D) | Double-blind placebo controlled trial (1995) | 14 children with abdominal migraine | 5 mL BID to TID (0.25 mg/5 mL) | Effective in 70% of patients |
Abbreviations: HT = hydroxytryptamine (serotonin); BID =twice a day; TID = thrice a day; PO = orally; GABA = gamma aminobutyric acid; IV = intravenous.
[Source 1] References- Mani J, Madani S. Pediatric abdominal migraine: current perspectives on a lesser known entity. Pediatric Health, Medicine and Therapeutics. 2018;9:47-58. doi:10.2147/PHMT.S127210. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5923275/
- Napthali K, Koloski N, Talley NJ. Abdominal migraine. Cephalalgia. 2016;36(10):980–986. https://www.ncbi.nlm.nih.gov/pubmed/26582952
- Chronic Abdominal Pain In Children: a Technical Report of the American Academy of Pediatrics and the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. Di Lorenzo C, Colletti RB, Lehmann HP, Boyle JT, Gerson WT, Hyams JS, Squires RH Jr, Walker LS, Kanda PT, AAP Subcommittee., NASPGHAN Committee on Chronic Abdominal Pain. J Pediatr Gastroenterol Nutr. 2005 Mar; 40(3):249-61.
- McFerron BA, Waseem S. Chronic recurrent abdominal pain. Pediatr Rev. 2012;33(11):509–517.
- Lewis ML, Palsson OS, Whitehead WE, Van Tilburg MA. Prevalence of functional gastrointestinal disorders in children and adolescents. J Pediatr. 2016;177:39–43.
- Mani J, Madani S. Pediatric abdominal migraine: current perspectives on a lesser known entity. Pediatric Health, Medicine and Therapeutics. 2018;9:47-58. doi:10.2147/PHMT.S127210 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5923275/
- Chitkara DK, Rawat DJ, Talley NJ. The epidemiology of childhood recurrent abdominal pain in Western countries: a systematic review. Am J Gastroenterol. 2005;100(8):1868–1875.
- Bentley D, Kehely A, Al-Bayaty M, Michie CA. Abdominal migraine as a cause of vomiting in children. J Pediatr Gastroenterol Nutr. 1995;21:S49–S51
- Drossman DA, Hasler WL. Rome IV – functional GI disorders: disorders of gut-brain interaction. Gastroenterology. 2016;150(6):1257–1261.
- Carson L, Lewis D, Tsou M, et al. Abdominal migraine: an underdiagnosed cause of recurrent abdominal pain in children. Headache. 2011;51(5):707–712.
- Baber KF, Anderson J, Puzanovova M, Walker LS. Rome II versus Rome III classification of functional gastrointestinal disorders in pediatric chronic abdominal pain. J Pediatr Gastroenterol Nutr. 2008;47(3):299.
- Dignan F, Abu-Arafeh I, Russell G. The prognosis of childhood abdominal migraine. Arch Dis Child. 2001;84(5):415–418.
- Kunishi Y, Iwata Y, Ota M, Kurakami Y, Matsubayashi M, Kanno M. Abdominal migraine in a middle-aged woman. Intern Med. 2016;55(19):2793.
- Mortimer MJ, Kay J, Jaron A. Clinical epidemiology of childhood abdominal migraine in an urban general practice. Dev Med Child Neurol. 1993;35(3):243–248
- Abu-Arafeh I, Russell G. Prevalence and clinical features of abdominal migraine compared with those of migraine headache. Arch Dis Child. 1995;72(5):413–417
- Good PA. Neurologic investigations of childhood abdominal migraine: a combined electrophysiologic approach to diagnosis. J Pediatr Gastroenterol Nutr. 1995;21(Suppl 1):S44–S48.
- Dimitrova AK, Ungaro RC, Lebwohl B, et al. Prevalence of migraine in patients with celiac disease and inflammatory bowel disease. Headache. 2013;53(2):344–355
- Lagman-Bartolome AM, Lay C. Pediatric migraine variants: a review of epidemiology, diagnosis, treatment, and outcome. Curr Neurol Neurosci Rep. 2015;15(6):1–4.
- Symon DN. Is cyclical vomiting an abdominal form of migraine in children? Dig Dis Sci. 1999;44(8 Suppl):23S–25S
- Catto-Smith AG, Ranuh R. Abdominal migraine and cyclical vomiting. Semin Pediatr Surg. 2003;12:254–258
- Farquhar HG. Abdominal migraine in children. Br Med J. 1956;1(4975):1082–1085.
- Lanzi G, Balottin U, Ottolini A, Burgio FR, Fazzi E, Arisi D. Cyclic vomiting and recurrent abdominal pains as migraine or epileptic equivalents. Cephalalgia. 1983;2:115–118
- Bremner AR, Sandhu BK. Recurrent abdominal pain in childhood: the functional element. Indian Pediatr. 2009;46(5):375–379
- Helgeland H, Flagstad G, Grøtta J, Vandvik PO, Kristensen H, Markestad T. Diagnosing pediatric functional abdominal pain in children (4–15 years old) according to the Rome III Criteria: results from a Norwegian prospective study. J Pediatr Gastroenterol Nutr. 2009;49(3):309–315.
- Özge A, Öksüz N, Ayta S, et al. Atopic disorders are more common in childhood migraine and correlated headache phenotype. Pediatr Int. 2014;56(6):868–872
- Egger J, Wilson J, Carter CM, Turner MW, Soothill JF. Is migraine food allergy? A double-blind controlled trial of oligoantigenic diet treatment. Lancet. 1983;322(8355):865–869.
- Drossman DA, Hasler WL. Rome IV – functional GI disorders: disorders of gut-brain interaction. Gastroenterology. 2016;150(6):1257–1261
- Napthali K, Koloski N, Talley NJ. Abdominal migraine. Cephalalgia. 2016;36(10):980–986.
- Devanarayana NM, Rajindrajith S, Benninga MA. Abdominal migraine in children: association between gastric motility parameters and clinical characteristics. BMC Gastroenterol. 2016;16(1):26.
- Korterink J, Devanarayana NM, Rajindrajith S, Vlieger A, Benninga MA. Childhood functional abdominal pain: mechanisms and management. Nat Rev Gastroenterol Hepatol. 2015;12(3):159–171.
- Mehle ME. Migraine and allergy: a review and clinical update. Curr Allergy Asthma Rep. 2012;12(3):240–245.
- Dignan F, Abu-Arafeh I, Russell G. The prognosis of childhood abdominal migraine. Arch Dis Child. 2001;84(5):415–418
- Powell N, Walker MM, Talley NJ. The mucosal immune system: master regulator of bidirectional gut-brain communications. Nat Rev Gastroenterol Hepatol. 2017;14(3):143–159.
- Loewendorf AI, Matynia A, Saribekyan H, Gross N, Csete M, Harrington M. Roads less traveled: sexual dimorphism and mast cell contributions to migraine pathology. Front Immunol. 2016;7:140.
- D’Andrea G. Pathogenesis of chronic migraine: the role of neuromodulators. J Headache Pain. 2015;16(S1):A38.
- Tan V, Sahami AR, Peebles R, Shaw RJ. Abdominal migraine and treatment with intravenous valproic acid. Psychosomatics. 2006;47(4):353–355
- Jones AL, Rubin GL, Coughtrie MW, Roberts RC, Colvin W. Reduced platelet phenolsulphotransferase activity towards dopamine and 5-hydroxytryptamine in migraine. Eur J Clin Pharmacol. 1995;49(1):109–114
- Kusumi M, Ishizaki K, Kowa H, et al. Glutathione S-transferase polymorphisms: susceptibility to migraine without aura. Eur Neurol. 2003;49(4):218–222.
- Hassan AM, Jain P, Mayerhofer R, et al. Visceral hyperalgesia caused by peptide YY deletion and Y2 receptor antagonism. Sci Rep. 2017;7:40968
- D’Andrea G. Pathogenesis of chronic migraine: the role of neuromodulators. J Headache Pain. 2015;16(S1):A38
- Napthali K, Koloski N, Talley NJ. Abdominal migraine. Cephalalgia. 2016;36(10):980–986
- Popovich DM, Schentrup DM, McAlhany AL. Recognizing and diagnosing abdominal migraines. J Pediatr Health Care. 2010;24(6):372–377
- Scicchitano B, Humphreys G, Mitton SG, Jaiganesh T. Abdominal migraine in childhood: a review. Pediatr Health Med Ther. 2014;5:73–81.
- Worawattanakul M, Rhoads JM, Lichtman SN, Ulshen MH. Abdominal migraine: prophylactic treatment and follow-up. J Pediatr Gastroenterol Nutr. 1999;28(1):37–40
- Russell G, Abu-Arafeh I, Symon DN. Abdominal migraine: evidence for existence and treatment options. Paediatr Drugs. 2002;4(1):1–8
- Egger J, Wilson J, Carter CM, Turner MW, Soothill JF. Is migraine food allergy? A double-blind controlled trial of oligoantigenic diet treatment. Lancet. 1983;322(8355):865–869
- Gulewitsch MD, Weimer K, Enck P, Schwille-Kiuntke J, Hautzinger M, Schlarb AA. Stress reactivity in childhood functional abdominal pain or irritable bowel syndrome. Eur J Pain. 2017;21(1):166–177.
- Russell G, Abu-Arafeh I, Symon DN. Abdominal migraine: evidence for existence and treatment options. Paediatr Drugs. 2002;4(1):1–8.
- Kakisaka Y, Wakusawa K, Haginoya K, et al. Efficacy of sumatriptan in two pediatric cases with abdominal pain-related functional gastrointestinal disorders: does the mechanism overlap that of migraine? J Child Neurol. 2010;25(2):234–237
- Kacperski J, Hershey AD. Newly approved agents for the treatment and prevention of pediatric migraine. CNS Drugs. 2016;30(9):837–844
- Madani S, Cortes O, Thomas R. Cyproheptadine use in children with functional gastrointestinal disorders. J Pediatr Gastroenterol Nutr. 2016;62(3):409–413
- Tan V, Sahami AR, Peebles R, Shaw RJ. Abdominal migraine and treatment with intravenous valproic acid. Psychosomatics. 2006;47(4):353–355.
- Kothare SV. Efficacy of flunarizine in the prophylaxis of cyclical vomiting syndrome and abdominal migraine. Eur J Paediatr Neurol. 2005;9(1):23–26
- Symon DN, Russell G. Double blind placebo controlled trial of pizotifen syrup in the treatment of abdominal migraine. Arch Dis Child. 1995;72(1):48–50





{kind=link}