
What are absence seizures
An absence seizure or absence epilepsy is used to be known as Petit mal seizure, is the term for a type of seizure involving staring spells. An absence seizure is a generalized onset seizure, which means it begins in both sides of the brain at the same time 1. Absence seizures involve a brief (usually less than 15 seconds) disturbance of brain function due to abnormal electrical activity in the brain resulting in sudden lapses in awareness. Someone having an absence seizure may look like he or she is staring blankly into space for a few seconds (staring episodes). Then, there is a quick return to a normal level of alertness. This type of seizure usually doesn’t lead to physical injury. Recovery is immediate and the young person continues what they were doing so the seizure may go unnoticed. The young person may also not be aware that they have had a seizure. Although brief, these seizures can cause the young person to miss out on parts of their learning, but they will not know what they have missed. Their failure to respond when they are spoken to often results in the young person being told off in school for not paying attention or for daydreaming.
The easiest way to spot an absence seizure is to look for a blank stare that lasts for a few seconds. People in the midst of having an absence seizure don’t speak, listen, or appear to understand. An absence seizure doesn’t typically cause you to fall down. You could be in the middle of making dinner, walking across the room, or typing an e-mail when you have the seizure. Then suddenly you snap out of it and continue as you were before the seizure. However, if you experience jerking motions, it may be a sign of another type of seizure taking place along with the absence seizure. Some children who have absence seizures also develop other seizures. Absence seizures may occur with other types of seizures, such as generalized tonic-clonic seizures (grand mal seizures), twitches or jerks (myoclonus), or sudden loss of muscle strength (atonic seizures).
Signs and symptoms of absence seizures usually include:
- Sudden stop in motion without falling
- Stopping activity (suddenly not talking or moving)
- Being very still
- Lip smacking
- Fluttering the eyelids
- Chewing motions with the mouth
- Finger rubbing
- Small movements of both hands
- Suddenly returning to activity when the seizure ends
Afterward, there’s no memory of the incident. Some people have many episodes daily, which interfere with school or daily activities. Unexplained difficulties in school and learning difficulties may be the first sign of absence seizures.
Absence seizures are more common in children than in adults. Absence seizures occur most often in people under age 20, usually in children ages 4 to 12. Many children outgrow absence seizures in their teens and do not usually continue into adulthood.
Absence seizures result from overactivity in the brain. In some cases, absence seizures are triggered by flashing lights or when the person breathes faster and more deeply than usual (hyperventilates).
You may have absence seizures repeatedly for years before heading to the doctor for a diagnosis. You may have “staring spells” without thinking of them as a medical problem or a seizure.
What causes this delay?
- It’s very common for people to mistake absence seizures for daydreaming or not paying attention.
- Absence seizures are most likely to affect children, and paying attention is a common problem for children. Since daydreaming can happen often in school for many different reasons, it may be hard to know if the staring is a seizure or not.
- Often the first clue that a child may be having absence seizures is when he or she starts having trouble in school.
An electroencephalography (EEG) is a test most often used to diagnose absence seizures. The EEG records the brain’s electrical activity and spots any abnormalities that could indicate an absence seizure. During the EEG, you may be asked to breath fast or close your eyes while lights are flashed fast. These things may make it easier to see absence seizure patterns on an EEG.
Absence seizures is classified as typical or atypical absence seizure depending on seizure characteristics and EEG (electroencephalogram) pattern. Atypical absence seizures do not start or finish as abruptly as typical absence seizures. Atypical absence seizures usually last longer and may have additional features such as changes in muscle tone. These changes may result in small movements, such as a slight nodding of the head or a chewing action and the young person may continue to respond to their surroundings. These atypical absence seizures are often associated with other seizure types or learning disabilities.
About 10% of seizures in children with epilepsy are typical absence seizures. Annual incidence has been estimated at 0.7 to 4.6/100,000 people in the general population, and 6 to 8/100,000 in children aged 0 to 15 years 2. Prevalence is 5 to 50/100,000 people in the general population. Similar figures were found in the USA (Connecticut) and in Europe-based (Scandinavia, France) population studies. Age of onset ranges from 3 to 13 years, with a peak at 6 to 7 years 2.
- Absence seizures have a typical spike and wave pattern on the EEG – showing regular symmetrical generalized spike and wave complexes with a frequency of 3 Hz, and usually occur in children with normal development and intelligence. Atypical absence seizures have different EEG changes and clinical manifestations, and have a different natural history and response to treatment.
- Absence seizures can be differentiated from complex partial seizures by their abrupt ending and lack of a postictal phase.
- About 10% of seizures in children with epilepsy are typical absence seizures, with genetic factors considered to be the main cause. Where they are the only manifestation of epilepsy, they generally resolve spontaneously by the age of 12 years.
Generalized absence seizures usually start in childhood, but can occur in adults. Absence seizures are brief and characterized by staring, loss of expression, unresponsiveness and stopping activity. Sometimes eye blinking or upward eye movements are seen. The person usually recovers immediately and resumes their previous activity, with no memory of the event.
An indication of simple absence seizure is a vacant stare, which may be mistaken for a lapse in attention that lasts about 10 seconds, though it may last as long as 20 seconds, without any confusion, headache or drowsiness afterward.
Absence seizures usually can be controlled with anti-seizure medications, changes in lifestyle for adults and children, such as activity and diet, and sometimes surgery. Your doctor can tell you more about these options.
Absence seizures key points:
- Absence seizures are seizures that generally last just a few seconds, and are characterized by a blank or “absent” stare.
- Absence seizures usually occur in children between ages 4 to 14, but it’s possible to have an absence seizure at any age.
- Absence seizures are easy to miss, but tests and an evaluation of symptoms can diagnose them.
- Your doctor can usually help find the right mix of medications and lifestyle changes to manage absence seizures.
- Without treatment, school performance, work, and relationships can suffer.
See your doctor:
- The first time you notice a seizure
- If this is a new type of seizure
- If the seizures continue to occur despite taking anti-seizure medication
If you think your child may be having absence seizures, talk to your child’s doctor about your concerns right away. Absence seizures may be confused with other types of seizures. That’s another reason why it’s so important that your child see a doctor for a correct diagnosis. If the diagnosis is not clear or your child continues to have problems, see an epilepsy specialist called an epileptologist.
Kids who have absence seizures aren’t usually in danger during a seizure. However, absence seizures may cause your child to:
- Have trouble learning at school
- Have social problems
- Misbehave more often
Contact your local emergency services number in your area:
- If you observe prolonged automatic behaviors lasting minutes to hours — activities such as eating or moving without awareness — or prolonged confusion, possible symptoms of a condition called absence status epilepticus
- After any seizure lasting more than five minutes
What do absence seizures look like?
There are two types of absence seizures that may look a bit different. Both types of seizures are short, and people often don’t notice them at first. They may come and go so quickly that no one notices anything wrong. Or observers may mistake the symptoms for simple daydreaming or not paying attention.
Typical absence seizures
- Typical absence seizures are the most common.
- The person suddenly stops all activity. It may look like he or she is staring off into space or just has a blank look.
- The eyes may turn upwards and eyelids flutter.
- The seizures usually last less than 10 seconds.
Atypical absence seizures
- These absence seizures are called atypical because they may be longer, have a slower onset and offset, and involve different symptoms.
- The seizure still starts with staring into space, usually with a blank look.
- There is usually a change in muscle tone and movement. You may see
- Blinking over and over that may look like fluttering of the eyelids
- Smacking the lips or chewing movements
- Rubbing fingers together or making other hand motions
- An atypical absence seizure lasts longer, up to 20 seconds or more.
How can I tell the difference between absence seizures and daydreaming?
If you’re wondering whether your child is daydreaming or having absence seizures, here are a few key differences to look for.
Daydreaming
- Daydreaming is more likely to happen when your child is bored (for example, during a long class at school)
- Usually comes on slowly
- Can be interrupted
- Tends to continue until something stops it (for example, the teacher, a friend, or parent getting the child’s attention)
Absence seizures
- Absence seizures can happen anytime, including during physical activity
- Usually come on very suddenly, without warning
- Cannot be interrupted
- End on their own, typically within 10-20 seconds
How can I tell the difference between absence seizures and focal impaired awareness seizures?
Seizures that involve staring and a change in awareness are sometimes mislabeled as absence seizures. People often confuse absence seizures with focal impaired awareness seizures.
There are some key signs that happen before and after a seizure that help us to decide which type of seizure a person is having. The length of a seizure and the frequency of seizures are also helpful observations to keep track of. All of this information, along with the results of EEG testing, can help to accurately diagnose which type of seizure a person is having.
The following features are more suggestive of focal impaired awareness seizures:
- Warning (aura) prior to the seizure
- Confusion and sleepiness after the seizure (postictal state)
- Duration longer than 30-45 seconds
- Frequency is less often than daily
How common are absence seizures?
The incidence of absence seizures is between 0.7 and 4.6 per 100,000 in the general population and around 6 to 8 per 100,000 in the pediatric population younger than 15 years 3.
Childhood absence epilepsy is a common pediatric epilepsy syndrome. Among all cases of epilepsy in school-aged children, 10% to 17% are due to childhood absence epilepsy 4. The age of onset for childhood absence epilepsy is typically between 4 and 10 years, with a peak between ages 5 and 7. Girls have childhood absence epilepsy more frequently than boys 5.
What’s it like to have an absence seizure?
- When people have absence seizures, they are not aware of what is happening around them. For example, they will not notice if someone tries to speak to them during a seizure.
- If a person is speaking when their seizure begins, they will stop talking, often in the middle of a sentence. It may seem like a pause to an observer.
- Often a child may have many absence seizures in a row.
- An observer may not see the beginning or end of a seizure. The person may just look confused and not know what has happened.
What happens after an absence seizure?
When an absence seizure ends, the person usually continues doing whatever they were doing before the seizure. They are almost always wide awake and able to think clearly. Generally, no first aid is needed for this type of seizure.
When absence seizures happen close together or a person has many in a day, the person may look or act confused and lose track of what has been going on. For children in school, they may not be aware of what has happened in the classroom, miss instructions from the teacher, or have incomplete work.
If someone has absence seizures, how often will they happen?
- The number of absence seizures a person may have varies a lot.
- Seizure medicines can control absence seizures in many children so they have rare seizures or none at all.
- Other people may have hundreds of brief absence seizures a day.
What types of epilepsy occur in children?
The most common epilepsy types in children include 6:
- Absence epilepsy or absence seizures: Brief spells during which the child loses awareness for a few seconds. They become pale, stare into space and don’t respond if you talk to them. Their eyelids may also twitch, and their eyes or head may roll back. These brief absences can occur up to one hundred times a day.
- Rolandic epilepsy: One side of the face twitches, and sometimes one arm or one leg twitches too. The child may also experience tingling, numbness, problems with speech and swallowing, and start salivating more (“drooling”). They are usually aware of this happening. This kind of seizure typically happens while falling asleep or waking up.
- Juvenile myoclonic epilepsy: This type of epilepsy first arises in puberty. The seizures involve muscle twitching and jerking movements of the arms and shoulders. They usually happen in the morning after waking up. The knees sometimes give way too.
- Infantile spasms (West syndrome): This severe type of epilepsy nearly always starts in babies. During seizures, the child’s whole body bends and stretches, and the muscles in their neck and torso convulse (jerk and twitch). The seizures usually occur shortly after waking up or while falling asleep. They often only last a few seconds, but can occur up to a hundred times in a row with short breaks between them.
How does epilepsy affect children?
About 70% of all children with epilepsy have a normal mental development and are just as intelligent as children who don’t have epilepsy. The epilepsy doesn’t affect their daily life much. The medication often works well, and sometimes isn’t needed at all.
Frequent seizures, on the other hand, can have physical and emotional effects. These include the following 6:
- Poor concentration: The children are tired or very restless. This might reduce their performance.
- Low self-esteem: Many children are ashamed of having seizures. Knowing that you might have an epileptic seizure can be unsettling because it’s beyond your control.
- Fear of having another seizure: Many children and parents live with this fear. As a result, they might start avoiding activities with other people and doing less sports – even though there’s no need to do so in many cases.
There’s also a risk of injury, for instance due to a seizure-related fall 7. But with enough treatment and support, it’s often possible to live a good life despite having epilepsy.
Developmental disorders, brain damage and mental disability are more common in people who have epilepsy. These may be either the result or the cause of the seizures.
Absence seizure symptoms
An indication of simple absence seizure is a vacant stare, which may be mistaken for a lapse in attention that lasts about 10 seconds, though it may last as long as 20 seconds, without any confusion, headache or drowsiness afterward.
The staring episodes may:
- Occur many times a day
- Occur for weeks to months before being noticed
- Interfere with school and learning
- Be mistaken for lack of attention, daydreaming or other misbehavior
During the seizure, the person may:
- Stop walking and start again a few seconds later
- Stop talking in mid-sentence and start again a few seconds later
The person usually does not fall during the seizure.
Right after the seizure, the person is usually:
- Wide awake
- Thinking clearly
- Unaware of the seizure
Specific symptoms of typical absence seizures may include:
- Changes in muscle activity, such as no movement, hand fumbling, fluttering eyelids, lip smacking, chewing
- Changes in alertness (consciousness), such as staring episodes, lack of awareness of surroundings, sudden halt in movement, talking, and other awake activities
Some absence seizures begin slower and last longer. These are called atypical absence seizures. Symptoms are similar to regular absence seizures, but muscle activity changes may be more noticeable.
Afterward, there’s no memory of the incident. Some people have many episodes daily, which interfere with school or daily activities.
A child may have absence seizures for some time before an adult notices the seizures, because they’re so brief. A decline in a child’s learning ability may be the first sign of this disorder. Teachers may comment about a child’s inability to pay attention or that a child is often daydreaming.
Unexplained difficulties in school and learning difficulties may be the first sign of absence seizures.
Absence seizures complications
While most children outgrow absence seizures, some:
- Must take anti-seizure medications throughout life to prevent seizures
- Eventually have full convulsions, such as generalized tonic-clonic seizures
Other complications can include:
- Learning difficulties
- Behavior problems
- Social isolation
Absence seizures causes
Like other kinds of seizures, absence seizures are caused by abnormal electrical impulses from nerve cells (neurons) in the brain 8. The brain’s nerve cells normally send electrical and chemical signals across the synapses that connect them. In people who have seizures, the brain’s usual electrical activity is altered. During an absence seizure, these electrical signals repeat themselves over and over in a three-second pattern. Doctors often don’t know why this happens. Most absence seizures are less than 15 seconds long. It’s rare for an absence seizure to last longer than 15 seconds. They can happen suddenly without any warning signs.
People who have seizures may also have altered levels of the chemical messengers that help the nerve cells communicate with one another (neurotransmitters).
In addition, many children appear to have a genetic predisposition to absence seizures. Absence seizures occur in multiple genetic generalized epilepsies including childhood absence epilepsy, juvenile absence epilepsy and juvenile myoclonic epilepsy 9. Atypical absence seizures have been reported in up to 60% of patients with Lennox-Gastaut syndrome 4. In 1951, Lennox reported that 66% of monozygotic twins showed concordance for the EEG pattern of 3-Hertz spike-and-wave. Doose at al., described 252 patients with absence epilepsy with a 3-Hertz spike-and-wave pattern. He proposed that there was multifactorial inheritance. The voltage-gated T-type calcium channel gene, the GABA-A receptor subunits GABRG2 and GABRG3, and the CACNA1A gene are thought to be involved in the etiology of this epilepsy syndrome 5, 3. However, the mode of inheritance and the majority of genes implicated in childhood absence epilepsy are still unknown 5.
Risk factors for developing absence seizures
Certain factors are common to children who have absence seizures, including:
- Age. Absence seizures are more common in children between the ages of 4 and 14.
- Sex. Absence seizures are more common in girls.
- Family members who have seizures. Nearly half of children with absence seizures have a close relative who has seizures.
Absence seizures pathophysiology
Although some of the pathways involved in the development of absence seizures have been described, their pathophysiological mechanisms are yet to be fully understood 8. The cortico-thalamic-cortical circuit is considered to play a major role in the pathophysiology of absence seizures 10.
Some of the neurons involved in the cortico-thalamic-cortical system include 11:
- Cortical glutamatergic neurons are originating on cortical layer VI and projecting to the nucleus reticularis of the thalamus.
- Thalamic relay neurons that have excitatory projections to cortical pyramidal neurons.
- Neurons from the thalamic nucleus reticularis containing inhibitory GABA-ergic projections that connect with other neurons from the same nucleus, and with thalamic relay neurons. These neurons do not connect directly with the cortex 5.
Neurons from the thalamic nucleus reticularis can fire in an oscillatory pattern (for example, rhythmic bursts involved in the generation of sleep spindles) or continuously in single spikes (tonic firing during wakefulness) 11. Shifts between these two firing patterns in the thalamic nucleus reticularis are modulated by spikes present in thalamocortical networks and neurons from the thalamic nucleus reticularis. These are mediated through low-threshold transient calcium channels known as T-type channels. After depolarization, T-type channels briefly allow calcium inflow before becoming inactivated. Reactivation requires a relatively long hyperpolarization facilitated by GABA-B receptors. Therefore, abnormal oscillatory rhythms can originate from T-type channel abnormalities, or from the increased GABA-B activity 5.
As explained by the genetics of absence epilepsy, genes coding for T-type calcium channels and for GABA receptors have been associated with the etiopathogenesis of this type of epilepsy. Medications that suppress T-type calcium channels, such as ethosuximide and valproate, are effective anti-absence drugs. Conversely, medications that increase GABA-B activity (e.g., vigabatrin) exacerbate the frequency of absence seizures. In contrast, GABA-A agonists (e.g., benzodiazepines), that preferentially enhance GABA-ergic activity in neurons from the thalamic nucleus reticularis, can suppress absence seizures 5.
Absence seizures prevention
Taking your medicines exactly as your doctor prescribed is one of the best ways to manage absence seizures. But you can also make some changes in your life to help prevent absence seizures from happening. These include:
- Get plenty of sleep each night.
- Find ways to manage your stress.
- Eat a healthy diet.
- Exercise regularly.
It is important to note that some sodium channel blockers like phenytoin, carbamazepine, gabapentin, pregabalin, and vigabatrin can worsen absence seizures 5.
Absence seizures diagnosis
A general pediatric neurologist or a pediatric epileptologist should be consulted when a patient has staring spells that are suspected to be seizures. Your doctor will ask for a detailed description of the seizures and conduct a physical exam. This will include a detailed look at the brain and nervous system.
- An EEG (electroencephalogram) will be done to check the electrical activity in the brain. Electroencephalography (EEG) is painless procedure that measures waves of electrical activity in the brain. Brain waves are transmitted to the EEG machine via small electrodes attached to the scalp with paste or an elastic cap. People with seizures often have abnormal electrical activity seen on this test. Absence seizure has a classic EEG finding of 3 Hz spike and wave discharges 11. In some cases, the test shows the area in the brain where the seizures start. The brain may appear normal after a seizure or between seizures. Rapid breathing (hyperventilation) during an EEG study can trigger an absence seizure.
- Blood tests may also be ordered to check for other health problems that may be causing the seizures.
- Head CT or MRI scans may be done to find the cause and location of the problem in the brain. In absence seizures, brain-imaging studies, such as magnetic resonance imaging (MRI), will be normal. But tests such as MRI can produce detailed images of the brain, which can help rule out other problems, such as a stroke or a brain tumor. Because your child will need to hold still for long periods, talk with your doctor about the possible use of sedation.
- Spinal tap to test the cerebrospinal fluid.
Figure 1. Absence seizure EEG
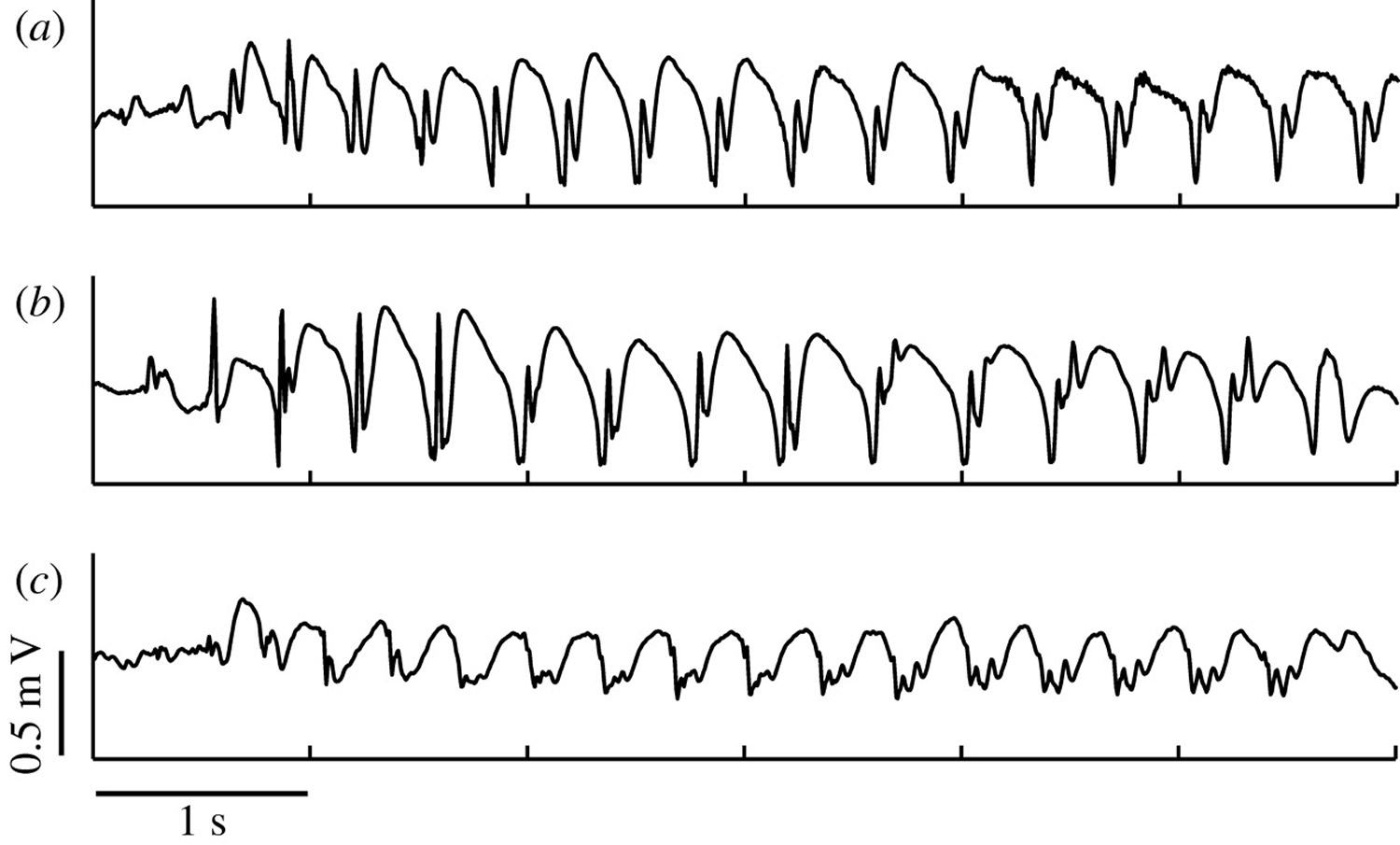
Note: The EEG recordings of three different patients with childhood absence epilepsy. (a) A typical spike–wave oscillation. (b) During a seizure, the EEG profile can show additional spikes. (c) A similar EEG recording as in (b). Again observe a polyspike–wave pattern; however, it is difficult to discern whether the spikes are leading the wave or vice versa.
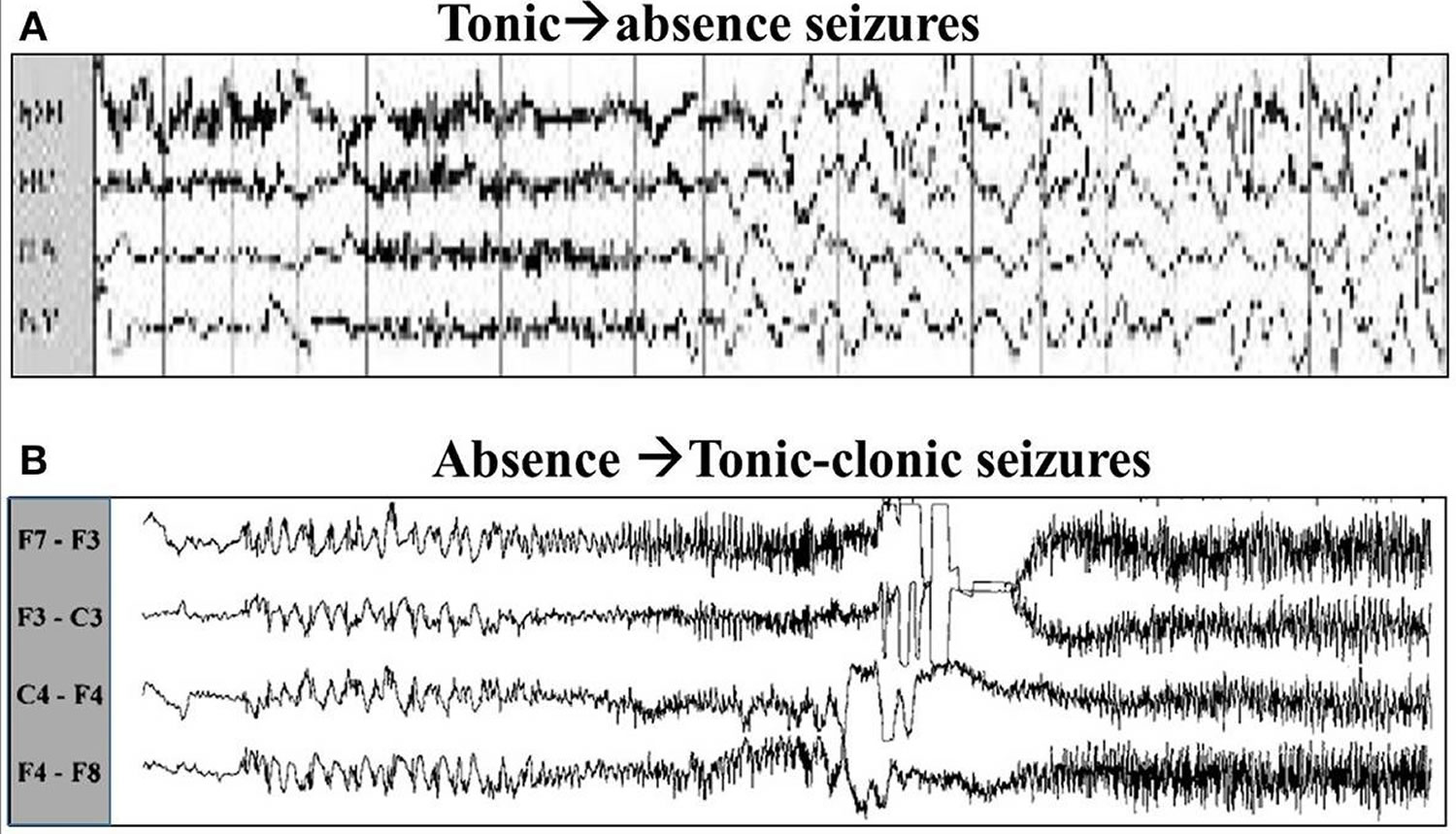
[Source 12]Figure 2. Absence seizures EEG
Absence seizures treatment
Absence seizures can affect your ability to perform at work or school, so it’s a good idea to see your healthcare provider about treatment.
Absence seizures can be treated with a number of different antiseizure medicines. The type of medicine that your healthcare provider recommends you take will also depend on what other seizure disorder you may have. If you have more than one type of seizure disorder, you may need to take multiple medicines.
Absence seizure medication
- Ethosuximide (Zarontin). This is the drug most doctors start with for absence seizures. In most cases, seizures respond well to this drug. Possible side effects include nausea, vomiting, sleepiness, trouble sleeping, hyperactivity. For this reason, ethosuximide should be taken with meals. Ethosuximide has been associated with aplastic anemia, skin reactions, and renal and hepatic impairment.
- Valproic acid (Depakene). Girls who continue to need medication into adulthood should discuss potential risks of valproic acid with their doctors. Valproic acid has been associated with higher risk of birth defects in babies, and doctors advise women against using it during pregnancy or while trying to conceive. Doctors may recommend the use of valproic acid in children who have both absence and grand mal (tonic-clonic) seizures. Valproate has been associated with behavioral and cognitive abnormalities, liver necrosis, and pancreatitis.
- Lamotrigine (Lamictal). Some studies show this drug to be less effective than ethosuximide or valproic acid, but it has fewer side effects. Side effects may include skin rash and nausea.
Lifestyle and home remedies
Dietary therapy
Following a diet that’s high in fat and low in carbohydrates, known as a ketogenic diet or “keto diet” for short, can improve seizure control. This is used only if traditional medications fail to control the seizures. Ketogenic diet involves eating mainly fats and hardly any carbohydrates. This diet causes your metabolism to change: Your body breaks down fats instead of sugars to get energy. There are more fatty acids (building blocks of fats) in the blood as a result. Fatty acids are thought to affect the way signals are passed between nerve cells in the brain, and it is believed that this reduces the number of epileptic seizures. But it’s not exactly clear how the keto diet works.
The possible side effects of a ketogenic diet include nausea, constipation, diarrhea and weight loss. Another problem is that many children find it difficult to stick to this diet over the long term.
There’s a lack of research on the long-term effects of the keto diet. Doctors recommend coming off “keto diet” after about two years. If seizures then start occurring more often, the ketogenic diet can be started again.
Ketogenic diet isn’t easy to maintain, but is successful at reducing seizures for some people. Variations on a high-fat, low-carbohydrate diet, such as the glycemic index and modified Atkins diets, though less effective, aren’t as restrictive as the ketogenic diet and may also provide benefit.
Additional options
Here are other steps you might take to help with seizure control:
- Take medication correctly. Don’t adjust the dosage before talking to your doctor. If you feel your medication should be changed, discuss it with your doctor.
- Get enough sleep. Lack of sleep can trigger seizures. Be sure to get adequate rest every night.
- Wear a medical alert bracelet. This will help emergency personnel know how to treat you correctly if you have another seizure.
- Ask your doctor about driving or recreation restrictions. Someone with a seizure disorder will have to be seizure-free for reasonable lengths of time (intervals vary from state to state) before being able to drive. Don’t bathe or swim unless someone else is nearby to help if needed.
Coping and support
If you’re living with a seizure disorder, you may feel anxious or stressed about what your future holds. Stress can affect your mental health, so it’s important to talk with your doctor about your feelings and seek resources for help.
At home
Your family members can provide much-needed support. Tell them what you know about the seizure disorder. Let them know they can ask you questions, and be open to conversations about their worries. Help them understand the condition by sharing any educational materials or other resources that your doctor has given you.
At school
Talk with your child’s teachers and coaches about your child’s seizure disorder and how it affects your child at school. Discuss what your child might need from them if a seizure happens at school.
You’re not alone
Remember, you don’t have to go it alone. Reach out to family and friends. Ask your doctor about local support groups or join an online support community. Don’t be afraid to ask for help. Having a strong support system is important to living with any medical condition.
Living with absence seizures
Most people with epilepsy live full and active lives with medicine and other lifestyle changes. But it can be challenging at times to manage large and small life events when you have epilepsy. Depending on your age and the severity and type of epilepsy, you may need support with the following:
- Behavioral and emotional issues. It is important to get enough sleep and manage stress when you have epilepsy. Stress and lack of sleep can trigger seizures. If you have trouble sleeping, talk with your healthcare provider about how to make sure you get enough sleep. Learn coping techniques that will help you manage stress and anxiety.
- Employment. With proper treatment, people with epilepsy can do just about any job safely and effectively. But, certain jobs in which there is a high risk to public safety may not be an option. Epilepsy is covered under the Americans with Disabilities Act. This law prohibits discrimination against people with epilepsy and other disabilities.
- Coping with discrimination and stigma. Children and adults with epilepsy may face discrimination and struggle to overcome the stigma associated with this neurological condition. Help educate family, friends, co-workers, and classmates on your condition. Let them know what to expect and how to help during a seizure.
- Education. Children with epilepsy may be entitled to special services under the Individuals with Disabilities Education Act (IDEA). Working closely with the child’s teacher and school nurse will help improve management of epilepsy at school. It’s important for parents of children with epilepsy to balance safety and fun. Allow your child to have some age-appropriate independence and participate in sports and other activities at school, when possible.
- Driving. Each state has different driving laws for people with epilepsy. Licensing may depend on how severe seizures are and how well they are controlled. Consider public transportation where it is available. If you continue to have absence seizures, it may not be safe for you to drive.
- Support and online resources. You may feel alone in dealing with day-to-day life with epilepsy, but be assured that many people have epilepsy. You can find local support groups through your healthcare provider or local hospital. Many online resources give tools and tips for managing this condition. Online social media support groups bring together people from all over the world who are managing their epilepsy. These groups provide support and encouragement.
If you have trouble managing your absence seizures, you may want to work more closely with your healthcare provider to find a better way to treat them.
Absence seizures prognosis
In childhood absence epilepsy, in which typical absence seizures are the only type of seizures suffered by the child, seizures generally cease spontaneously by 12 years of age or sooner. Children who start having absence seizures before age 9 are much more likely to outgrow them than children whose absence seizures start after age 10. In about 7 out of 10 children with absence seizures, the seizures may go away by age 18. If this happens, medicines may not be needed as an adult. For other children, seizure medication may be needed long-term. A neurologist can help you learn about the risks, treatments, and outlook for the future.
Less than 10% of children develop infrequent generalized tonic clonic seizures and it is rare for them to continue having absence seizures. In other epileptic syndromes (in which absence seizures may coexist with other types of seizure) prognosis is varied, depending on the syndrome. Absence seizures have a significant impact on quality of life. The episode of unconsciousness may occur at any time and usually without warning. Affected children need to take precautions to prevent injury during absences and should refrain from activities that would put them at risk if seizures occurred (e.g., climbing heights, swimming unsupervised, or cycling on busy roads) 7. Often, school staff members are the first to notice the recurrent episodes of absence seizures, and treatment is generally initiated because of the adverse impact on learning. Difficulty with language and reading is also commonly reported. Depression, anxiety and ADHD (attention deficit hyperactivity disorder) have also been reported more frequently in patients with childhood absence epilepsy 4.
References- Absence Seizures. https://www.epilepsy.com/learn/types-seizures/absence-seizures
- Posner E. Absence seizures in children. BMJ Clinical Evidence. 2008;2008:0317. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2907950
- Guilhoto LM. Absence epilepsy: Continuum of clinical presentation and epigenetics? Seizure. 2017 Jan;44:53-57. doi: 10.1016/j.seizure.2016.11.031
- Matricardi S, Verrotti A, Chiarelli F, Cerminara C, Curatolo P. Current advances in childhood absence epilepsy. Pediatr Neurol. 2014 Mar;50(3):205-12. doi: 10.1016/j.pediatrneurol.2013.10.009
- Pearl PL. Epilepsy Syndromes in Childhood. Continuum (Minneap Minn). 2018 Feb;24(1, Child Neurology):186-209. doi: 10.1212/CON.0000000000000568
- InformedHealth.org [Internet]. Cologne, Germany: Institute for Quality and Efficiency in Health Care (IQWiG); 2006-. Epilepsy in children: Types and treatment options. 2020 Aug 27. Available from: https://www.ncbi.nlm.nih.gov/books/NBK561513
- Carmant L, Kramer U, Holmes GL, Mikati MA, Riviello JJ, Helmers SL. Differential diagnosis of staring spells in children: a video-EEG study. Pediatr Neurol. 1996 Apr;14(3):199-202. doi: 10.1016/0887-8994(96)00080-x
- Vincenzo Crunelli, Magor L Lőrincz, Cian McCafferty, Régis C Lambert, Nathalie Leresche, Giuseppe Di Giovanni, François David, Clinical and experimental insight into pathophysiology, comorbidity and therapy of absence seizures, Brain, Volume 143, Issue 8, August 2020, Pages 2341–2368, https://doi.org/10.1093/brain/awaa072
- Unterberger I, Trinka E, Kaplan PW, Walser G, Luef G, Bauer G. Generalized nonmotor (absence) seizures-What do absence, generalized, and nonmotor mean? Epilepsia. 2018 Mar;59(3):523-529. doi: 10.1111/epi.13996
- Onat FY, van Luijtelaar G, Nehlig A, Snead OC 3rd. The involvement of limbic structures in typical and atypical absence epilepsy. Epilepsy Res. 2013 Feb;103(2-3):111-23. doi: 10.1016/j.eplepsyres.2012.08.008
- Albuja AC, Khan GQ. Absence Seizure. [Updated 2021 Aug 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499867
- Marten F., Rodrigues S., Benjamin O., Richardson M. P., Terry J. R. (2009). Onset of polyspike complexes in a mean-field model of human electroencephalography and its application to absence epilepsy. Philos. Trans. Roy. Soc. Lond. A Math. Phys. Eng. Sci. 367, 1145–1161. 10.1098/rsta.2008.0255 http://rsta.royalsocietypublishing.org/content/367/1891/1145.long
- Absence seizures with evolution into generalized tonic-clonic activity: clinical and EEG features. Mayville C, Fakhoury T, Abou-Khalil B. Epilepsia. 2000 Apr; 41(4):391-4. https://www.ncbi.nlm.nih.gov/pubmed/10756402
- Shih T. T., Hirsch L. J. (2003). Tonic-absence seizures: an underrecognized seizuretype. Epilepsia 44, 461–465. 10.1046/j.1528-1157.2003.39602.x https://www.ncbi.nlm.nih.gov/pubmed/12614405





{kind=link}