
What is agoraphobia
Agoraphobia is an anxiety disorder that involves intense fear and anxiety of any place or situation where escape might be difficult or that help wouldn’t be available if things go wrong 1. Many people assume agoraphobia is simply a an obsessive, persistent, intense fear of open places, but it’s actually a more complex condition. Agoraphobia usually involves fear of being in a crowded area, bridges, or of being alone outside of the home; traveling in a car, bus, or airplane; or being in a crowded area. With agoraphobia, you avoid places or situations because you do not feel safe in public places. The fear is worse when the place is crowded. Most people who have agoraphobia develop it after having one or more panic attacks, causing them to worry about having another attack and avoid the places where it may happen again. People with agoraphobia often have a hard time feeling safe in any public place, especially where crowds gather. You may feel that you need a companion, such as a relative or friend, to go with you to public places. The fear can be so overwhelming that you may feel unable to leave your home.
Agoraphobia often begins with a stressful event, such as loss of a job or relationship. The stressful event might lead a person to avoid the outside world. Over time, this avoidance grows to include more and more places. The stressful event might also trigger a panic attack. Panic attacks are very distressing, so the person may begin to avoid any situation that could trigger another attack.
You are more likely to experience agoraphobia if you have a family history of agoraphobia or anxiety, if you have anxiety, or if you have experienced a panic attack in the past 2.
Someone with agoraphobia may be scared of:
- spending time alone
- traveling on public transport, such as a bus, plane or train
- visiting a shopping center
- enclosed spaces, such as movie theaters, elevators or small stores
- open spaces, such as parking lots, bridges or malls
- leaving home alone
- crowds or waiting in line
- places where escape might be hard
- losing control in a public place
Symptoms of agoraphobia include:
- depending on others
- feeling detached or separated from others
- feeling helpless
- feeling that the body is not real
- feeling that the environment is not real
- having an unusual temper or agitation
- staying in the house for long periods
These situations cause anxiety because you fear you won’t be able to escape or find help if you start to feel panicked or have other disabling or embarrassing symptoms.
In addition:
- Fear or anxiety almost always results from exposure to the situation
- Your fear or anxiety is out of proportion to the actual danger of the situation
- You avoid the situation, you need a companion to go with you, or you endure the situation but are extremely distressed
- You experience significant distress or problems with social situations, work or other areas in your life because of the fear, anxiety or avoidance
- Your phobia and avoidance usually lasts six months or longer
If someone with agoraphobia finds themselves in a stressful situation, they’ll usually experience the symptoms of a panic attack, such as:
- rapid heartbeat
- rapid breathing (hyperventilating)
- feeling hot and sweaty
- feeling sick
- chest pain or discomfort
- choking
- dizziness or fainting
- nausea or other stomach distress
- racing heart
- short of breath
- sweating
- trembling
They’ll avoid situations that cause anxiety and may only leave the house with a friend or partner. They’ll order groceries online rather than going to the supermarket. This change in behavior is known as avoidance.
Agoraphobia usually develops as a complication of panic disorder, an anxiety disorder involving panic attacks and moments of intense fear. Agoraphobia can arise by associating panic attacks with the places or situations where they occurred and then avoiding them.
A minority of people with agoraphobia have no history of panic attacks. In these cases, their fear may be related to issues like a fear of crime, terrorism, illness, or being in an accident. Traumatic events, such as bereavement, may contribute towards agoraphobia, as well as certain genes inherited from your parents.
A diagnosis of agoraphobia can usually be made if:
- you’re anxious about being in a place or situation where escape or help may be difficult if you feel panicky or have a panic attack, such as in a crowd or on a bus
- you avoid situations described above, or endure them with extreme anxiety or the help of a companion
- there’s no other underlying condition that may explain your symptoms
The relationship between agoraphobia and panic disorder remains not been clearly established 3. Regarding this issue, 2 hypotheses have been proposed. It has been suggested that agoraphobia is a subtype of panic disorder. Grant et al 4 reported that panic disorder accompanied by agoraphobia could be a severe complication of panic disorder and agoraphobia was considered to result from recurrent panic attacks. On the other hand, agoraphobia could be a distinct disease independent of panic disorder 5, 6, 7. Recently, in the Diagnostic and Statistical Manual of Mental Disorders 5th edition (DSM-5), published by the American Psychiatric Association, agoraphobia has been separated from panic disorder as an independent condition, based on the following findings. Agoraphobia could occur without panic symptoms 8, is not always secondary to panic symptoms 4 and there are differences in prevalence, sex specific incidence rate, and treatment outcome between agoraphobia and panic disorder 8.
The current definition of agoraphobia in the Diagnostic and Statistical Manual of Mental Disorders 5th edition (DSM-5), published by the American Psychiatric Association, assigns a prominent role in the diagnosis to marked fear or anxiety about actual or anticipated exposure to public places or situations such as “using public transportation; being in open spaces; being in enclosed places; standing in line or being in a crowd; or being outside of the home alone in other situations” 9. Fear or anxiety must recur most of the time in at least two or more of the listed common situations. For the diagnosis, the individual must show both fears of exposure to public places and active avoidance of such situations. The fear or anxiety must not be related to a realistic threat or be explained by sociocultural context, and it should be not a consequence of substance use or withdrawal from it. Six months or more of persistent or recurrent symptomatology must be proved to make the diagnosis 9.
There is some disparity in estimates for the prevalence of agoraphobia as it has only recently received its own diagnostic criteria rather than as a qualifier for panic disorder 3. The National Institute of Mental Health estimates that the lifetime prevalence of agoraphobia is 1.3%, with an annual incidence rate of 0.9%. An estimated 1.3% of U.S. adults experience agoraphobia at some time in their lives 10. The prevalence of agoraphobia among adults was similar for females (0.9%) and males (0.8%). Of adults with agoraphobia in the past year, an estimated 40.6% had serious impairment, 30.7% had moderate impairment, and 28.7% had mild impairment. There is an increase in the risk of developing agoraphobia in late adolescence and early adulthood, with the overall average age at onset being 17 years. Based on diagnostic interview data from National Comorbidity Survey Adolescent Supplement, an estimated 2.4% of adolescents had agoraphobia at some time during their life, and all had severe impairment. The prevalence of agoraphobia among adolescents was higher for females (3.4%) than for males (1.4%).
In two-thirds of all cases of agoraphobia, initial onset is before age 35 years. There is a substantial incidence risk in late adolescence and early adulthood, with indications for a second high incidence risk phase after age 40 years. First onset in childhood is rare. The overall mean age at onset for agoraphobia is 17 years, although the age at onset without preceding panic attacks or panic disorder is 25-29 years.
The clinical features of agoraphobia are relatively consistent across the lifespan, although the type of agoraphobic situations triggering fear, anxiety, or avoidance, as well as the type of cognitions, may vary. For example, in children, being outside of the home alone is the most frequent situation feared, whereas in older adults, being in shops, standing in line, and being in open spaces are most often feared. Also, cognitions often pertain to becoming lost (in children), to experiencing panic-like symptoms (in adults), to falling (in older adults).
The percentage of individuals with agoraphobia reporting panic attacks or panic disorder preceding the onset of agoraphobia ranges from 30% in community samples to more than 50% in clinic samples. The majority of individuals with panic disorder show signs of anxiety and agoraphobia before the onset of panic disorder.
Agoraphobia treatment can be challenging because it usually means confronting your fears. But with psychotherapy and medications, you can escape the trap of agoraphobia and live a more enjoyable life.
With psychological treatment (talking therapies), most people with agoraphobia will make significant improvements, particularly if the three steps described below are followed.
A stepwise approach is usually recommended for treating agoraphobia and any underlying panic disorder:
- Educate yourself about your condition, possible lifestyle changes you can make, and self-help techniques to help relieve symptoms.
- Enrol yourself on a guided self-help programme.
- More intensive treatments, such as cognitive behavioral therapy (CBT) or medication.
Lifestyle changes may include taking regular exercise, eating more healthily, and avoiding alcohol, drugs and drinks that contain caffeine, such as tea, coffee and cola.
Self-help techniques that can help during a panic attack include staying where you are, focusing on something that’s non-threatening and visible, and slow, deep breathing.
If your agoraphobia fails to respond to these treatment methods, your doctor may suggest trying a guided self-help programme. This involves working through self-help manuals that cover the types of issues you might be facing, along with practical advice about how to deal with them.
Medication may be recommended if self-help techniques and lifestyle changes aren’t effective in controlling your symptoms. You’ll usually be prescribed a course of selective serotonin reuptake inhibitors (SSRIs), which are also used to treat anxiety and depression.
In severe cases of agoraphobia, medication can be used in combination with other types of treatment, such as cognitive behavioral therapy (CBT) and relaxation therapy.
Speak to your doctor if you think you have the symptoms of agoraphobia.
You should also seek medical advice if you have any of the following:
- chest pain
- shortness of breath
- headaches
- dizziness
- fainting episodes
- unexplained weakness
- the sensation your heart is beating irregularly (palpitations)
- depression
- thoughts of suicide or self-harm
While self-help coping strategies can be very effective, if your worries, fears, or anxiety attacks have become so great that they’re causing extreme distress or disrupting your daily routine, it’s important to seek professional help.
If you’re experiencing a lot of physical symptoms, you should start by getting a medical checkup. Your doctor can check to make sure that your anxiety isn’t caused by a medical condition, such as a thyroid problem, hypoglycemia, or asthma. Since certain drugs and supplements can cause anxiety, your doctor will also want to know about any prescriptions, over-the-counter medications, herbal remedies, and recreational drugs you’re taking.
If your physician rules out a medical cause, the next step is to consult with a therapist who has experience treating anxiety disorders. The therapist will work with you to determine the cause and type of your disorder and devise a course of treatment.
How can I overcome my panic and agoraphobia?
Fortunately, there are a number of strategies that you can use to overcome your panic and agoraphobia. These include:
- Understanding more about anxiety and panic.
- Learning breathing strategies that help to keep panic at bay.
- Learning how to challenge your unhelpful thoughts and see things in a more realistic light.
- Removing the use of avoidance and safety behaviors and gradually confronting your fears.
It can sometimes be more helpful to try out the ideas above one at a time, rather and trying to learn them all at once. However simply take things at your own pace.
Panic is simply a more extreme form of anxiety. You also know that due to the unpleasant and severe nature of panic, people often become frightened about the physical symptoms they experience. For example, they worry that their symptoms are early signs of a heart attack, chocking, fainting or going mad. As soon as people think in these catastrophic terms, they make themselves even more anxious and their physical symptoms get stronger. Of course, as their physical symptoms grow stronger, so does their belief that they are going to have a heart attack or choke etc. Soon a vicious cycle develops that often leads to a full blown panic attack.
From this information, it is clear to see that not fully recognizing and understanding the physical symptoms of anxiety and panic is a major part of the problem. Therefore an important goal is to become more knowledgeable about anxiety and panic. By learning more about how anxiety and panic affects us, and why you experience it in the first place, you can begin to see that it is not harmful. This can help us to be less fearful of the uncomfortable symptoms you experience, meaning you won’t misinterpret them as catastrophic. This prevents the vicious cycle of panic occurring and keeps our symptoms at a more manageable level.
When considering this, it is therefore important to remember that anxiety is a natural feeling that everyone experiences. Of course, some people experience anxiety more often than others. It is also true that the intensity of anxiety people experience varies at times (i.e. it can range from mild anxiety to a full blown panic attack). However, anxiety is not harmful; in-fact it is quite the opposite. As you will see next, you actually experience anxiety because of the benefits it has brought over the years.
If after reading this section you are still concerned that some your symptoms are not caused by anxiety, you should contact your doctor to have this clarified before continuing with this guide.
Why am I experiencing anxiety?
The symptoms you experience when anxious are often referred to as the ‘fight or flight’ response. This comes from the idea that people primarily experience anxiety to help them either fight or run away from danger. For example, if someone was attacking you, two options open to you would be to either – fight them off (fight) or try to run away (flight). Your fight or flight response would kick in to help you at this point. For example:
- Your hearts would begin beating more quickly (supplying blood to our muscles).
- You would sweat (to cool us down).
- Your muscles would become tense (ready for action).
- You would take deeper breaths (to supply oxygen to our muscles).
In essence, all of these responses would aid your escape or improve your ability to stay and fight the attacker. When considered in this way, you can see how the symptoms of anxiety are helpful to you. Indeed, all of the physical symptoms you experience when anxious play a helpful role in protecting you in such circumstances.
The fight or flight response was likely even more vital to human survival back in the days of early man, when people had to hunt for their food and were under a greater threat from predators. Nowadays you do not face the same threats, but unfortunately, your body and mind have not caught up with these changes. As a result, you now experience anxiety in situations where it is not necessarily as helpful because you cannot fight or run away from them (e.g. financial problems, stress at work, busy places, open spaces, etc). However, the one thing that has stayed true is the fact that these symptoms are not dangerous; they are in many ways the right response but at the wrong time.
When thinking about anxiety in this way, you can begin to see that you should not fear it; instead you should see it as your body’s healthy protection system. Remembering this can help you to be less fearful of the symptoms of anxiety. Instead of seeing the symptoms as dangerous (e.g. the early symptoms of a heart attack) you should think of them as a safe and natural response. By understanding this, you can stop the catastrophic misinterpretations that lead to panic attacks.
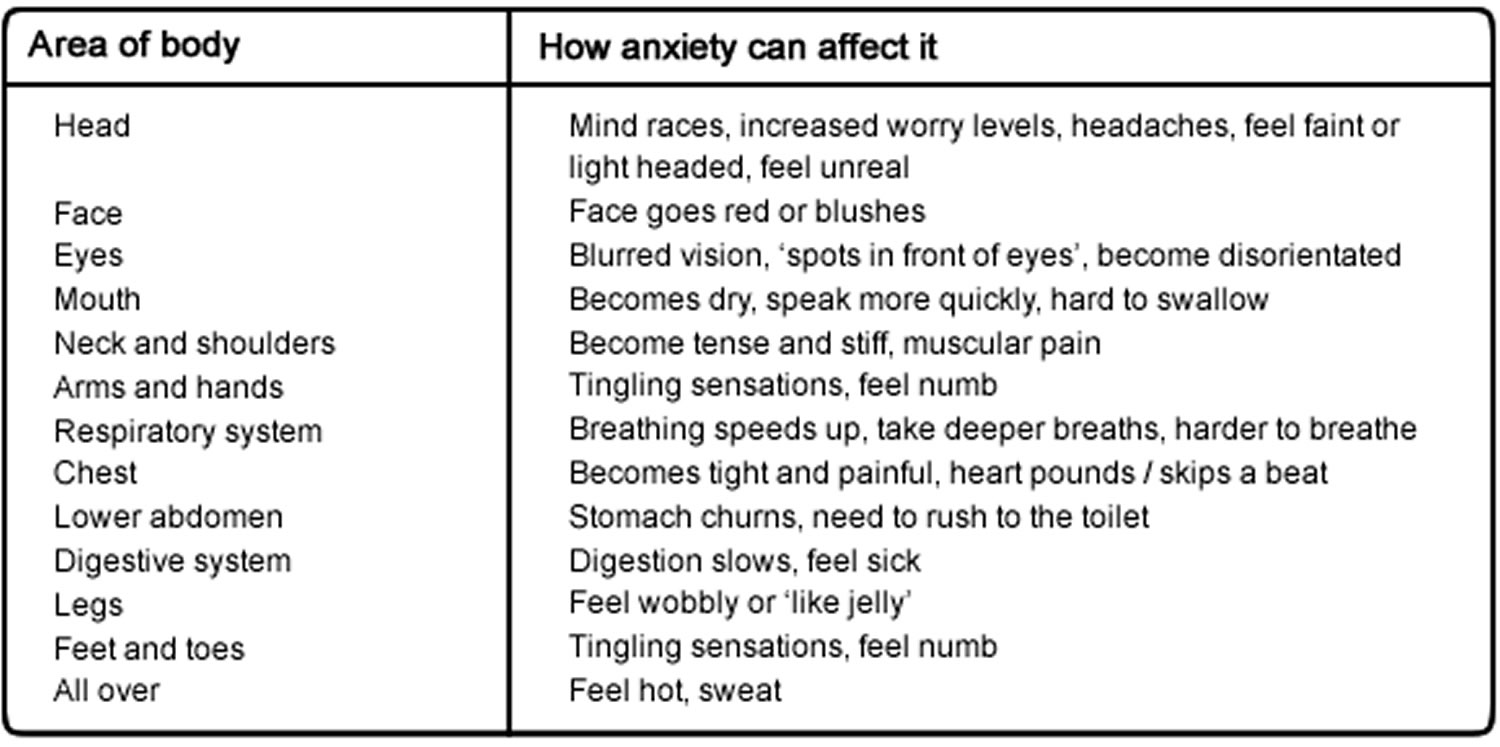
How does anxiety affect your body?
Anxiety can be particularly difficult to recognize because it affects our body in so many different ways. Over and above this, anxiety can affect everyone slightly differently. For example, some people regularly get headaches when anxious, whilst others may be more prone to becoming breathless or light headed. Below is a list of some of the different ways anxiety can affect us. Being more aware of these can help us to recognize that many of the physical changes we notice in our bodies are in fact anxiety symptoms. This can help stop us from misinterpreting bodily changes as something more serious.
Coping statements
When you are anxious or panicky, it is easy to forget what you have just learned (e.g. that it is not dangerous and cannot harm us). It can therefore be helpful to have ‘coping statements’ that you can refer to. These are basically statements that you can use to remind yourself about the facts of anxiety and panic, whenever you begin experiencing them. Reminding yourself about these facts can help to prevent cycles of panic occurring. These coping statements may particularly helpful when it comes to ‘Removing the use of avoidance and safety behaviors’.
Coping statements
- Anxiety is normal
- Panic is simply high levels of anxiety
- Everyone experiences anxiety and panic at times
- Anxiety and panic are not dangerous
- Anxiety is designed to protect us and is not harmful
- By remembering these symptoms are nothing more than anxiety, I can prevent a cycle of panic occurring
- I can tolerate the symptoms of anxiety and panic without them getting out of control
- Slowing my breathing down can help me to control my anxiety and panic
- My anxiety and panic will pass naturally given time, it doesn’t last forever
- I can continue without using escape, avoidance or safety behaviours
- I don’t always have to feel in complete control
- I’ve never fainted, choked, gone mad, or had a heart attack before
- People can’t tell how anxious I feel
Feel free to add in any other statements that may help you cope.
Learning how to control your breathing
People who experience panic attacks often have a tendency to ‘over breath’ when they are anxious. This basically means that they take deeper breaths than normal (which they are sometimes unaware of). This usually has the affect of making them feel short of breath and as though they are going to choke. As a result of these sensations, they take deeper breaths to try and correct this which actually just makes the sensations worse (this pattern is often referred to as hyperventilation). Before long a cycle of panic can develop.
Taking deeper breaths than usual also results in people ending up with the wrong amount of carbon dioxide in their bodies. This normally results in them feeling dizzy and disorientated. It can also cause chest pains to emerge. These sensations typically leave people feeling as though they are about to faint or have a heart attack which can also cause a cycle of panic to begin.
By learning ‘controlled breathing’ exercises, you can learn how to slow your breathing down to a better rate. This helps to fend off the uncomfortable physical feelings such as dizziness, light-headedness, chest pains, and shortness of breath. By doing so you can stop the cycle of panic and the feelings soon pass.
The following steps will take you through a ‘controlled breathing’ exercise. You can use this strategy whenever you feel anxious or panicky. In particular, you should use this strategy if you ever feel faint, light-headed or short of breath, as it should help these sensations to pass.
Step 1
Try to get into a slower and stable breathing rhythm. A good rhythm is to breathe in for three seconds, hold this breathe for two seconds, and then breathe out for three seconds. Make sure you don’t take too big ‘gulps’ of air whilst doing so.
Step 2
It can be helpful to count to yourself as you do this (e.g. in one, two, three hold for two; out one, two, three hold for two).
Step 3
As you breathe, try to make sure that your stomach expands as you take each breathe. This helps you to stop breathing from the chest which tends to result in short and shallow breaths that can add to the problem.
Step 4
Repeat this action for a few minutes. You should soon begin to feel the uncomfortable sensations pass.
‘Controlled breathing’ exercises can also be used as a more general relaxation strategy anytime you like. Many people find slowing their breathing down in this way to be very relaxing.
To master this technique, it would actually be helpful to practice it at times when you are not in an anxious or panicky state. This will help you master the technique for times when your symptoms are more troublesome.
Challenging unhelpful thoughts
The way that you think about things has an impact on our panic and agoraphobia. Many of these thoughts occur outside of our control, and can be negative or unhelpful. It is therefore important to remember that they are just thoughts, without any real basis, and are not necessarily facts. Even though you may believe a lot of our unhelpful thoughts when you are anxious or panicky, it is good to remember that they should be questioned as they are often based on wrong assumptions.
The following section will help you begin to recognize if you are thinking about things in an unhelpful or unrealistic way, and discuss how you can start to make changes to this. By doing so, you can learn to see things in a more realistic light which can help to reduce your panic and agoraphobia. You might have unhelpful thoughts about all kinds of things. Here are some examples:
Interpreting physical changes in the body as dangerous:
- These feelings are dangerous
- This will lead to a heart attack
- I’m going to faint / choke
- I’m going crazy
Underestimating your ability to cope in certain situations:
- It’ll be too busy
- I won’t be able to escape
- I’ll have a panic attack
- I’ll embarrass myself
Believing you must always be in complete control:
- I should never be anxious
- Feeling anxious means I’m weak
- I should always feel 100% in control
You might find it difficult to identify an unhelpful thought. Try thinking about a time when you felt panicky. Consider what was running through your mind at that time.
Patterns of unhelpful thinking
First you need to be able to recognize an unhelpful thought. Then you can challenge it. Being aware of the common patterns that unhelpful thoughts follow can help you to recognize when you have them. Here are some of the common patterns that our unhelpful thoughts follow:
Predicting the Future:
When we feel panicky it is common for us to spend a lot of time thinking about the future and predicting what could go wrong, rather than just letting things be. In the end most of our predictions don’t happen and we have wasted time and energy being worried and upset about them. For example:
- Worrying that the supermarket will be very busy.
- Worrying you will choke and suffocate if you go into a lift.
Catastrophizing:
People commonly ‘catastrophize’ when they feel panicky, which basically means that they often blow things out of proportion. For example:
- I’ll get anxious, completely lose it and totally embarrass myself – when in all likelihood you have experienced anxiety in the past and coped well.
- The bus will get so busy that my exit will be blocked and I won’t be able to get off.
Should Statements:
People often imagine how they would like things to be or how they ‘should be’ rather than accepting how things really are. For example:
- I should always be 100% comfortable in crowds.
- I should be able to travel on trains.
This critical style of thinking simply creates extra pressure and stress.
Over Generalizing:
Based on one isolated incident you assume that all others will follow a similar pattern in the future. Basically, you find it hard to see a negative event as a one off which can leave you feeling hopeless. For example:
- Because you had a panic attack one time whilst shopping, you believe that you will panic in every shop you go into in the future.
What If Statements:
Have you ever wondered “what if” something bad happens? For example:
- What if I have a panic attack at the party?
- What if I faint on the train?
These thoughts result in you restricting your activities.
Black and White Thinking:
Often when feeling panicky, people see things as either black or white, there is no in between. For example:
- They believe any sign of anxiety is weak.
- They believe they never cope well when they go out.
This sets up expectations that can hold you back.
Ignoring the Positives:
Often people can ignore the positive aspects of life or situations, and instead focus on the negative elements. For example:
They remember feeling panicky in the supermarket, but forget that they always cope well in the busy town center.
These thoughts keep our confidence levels low and we attempt to do less.
Labeling:
Do you find that you attach negative ‘labels’ to yourself? For example:
- I’m weak.
- I’m always panicking.
- I’m incapable.
Labels like these tend to follow you around and hold you back.
Challenges to an unhelpful thought
Now you can challenge your unhelpful thoughts by asking these questions.
Is there any evidence that contradicts this thought?
- I was in a coffee shop a few weeks back and I didn’t have a panic attack.
- I’ve been in this restaurant in the past and coped fine.
Can you identify any of the patterns of unhelpful thinking described earlier?
- I’m predicting the future, as I can’t say for sure what will happen.
- I’m discounting positives as I’ve coped in similar situations in the past.
What would you say to a friend who had this thought in a similar situation?
- I’d say you’ve coped before so there is no reason you can’t cope again.
What are the costs and benefits of thinking in this way?
Costs:
- Its making me anxious before I even go in.
- Its making me want to avoid it and let down my friend.
- It makes it hard to focus on anything other than how I am feeling.
Benefits: I can’t think of any.
Is there a proactive solution to this unhelpful thought?
- I could read my coping statements before I go in.
- I could use breathing exercises to help me calm down.
Once you have asked yourself these questions, you should read through your answers. Try to come up with a more balanced or rational view. For example:
- Although I may get anxious, it doesn’t mean I’ll have a panic attack. I’ve been in similar situations before and I’ve coped OK.
Try to apply these questions to the unhelpful thoughts that you notice. It can help to reduce your panic and agoraphobia. You can use this technique to test your thoughts are realistic and balanced.
Removing the use of avoidance and safety behaviors
One of the main reasons that people find it difficult to overcome their panic and agoraphobia is because they avoid situations that they worry about panicking in. Furthermore, whenever they do confront these situations, they tend to use safety behaviors. Safety behaviors are any actions that people use to try and minimize the anxiety they experience in such situations (e.g. only traveling on buses that are very quiet; going shopping late at night when it is quiet; sitting down if they feel light-headed; only going to public places if they have a friend with them).
Although it is easy to see why people use avoidance and safety behaviors to cope with their panic and agoraphobia, in the longer term these strategies only make things worse. This is because, the longer you avoid a situation you fear, the more frightening it becomes. Perhaps even more importantly, avoidance and ‘safety behaviors’ prevent us from having the opportunity to prove that you can cope in these situations and that they are not as frightening as previously thought. Because of this, one of the best ways to overcome panic and agoraphobia is to gradually confront these situations without using safety behaviors.
Of course confronting these situations can be daunting, especially given that your anxiety levels rise when you do so. You may also have experienced a panic attack in similar situations in the past. However, your new knowledge of anxiety and panic should help you to keep your anxiety at a manageable level. Remember, if you don’t misinterpret these symptoms as catastrophic (e.g. the early signs of a heart attack, losing control etc) you can fend off panic attacks.
If you can do this, research shows that when you are anxious (e.g. on a bus; in a supermarket etc), our anxiety eventually peaks and drops if you remain in that situation for long enough. It is almost as though our bodies and minds become ‘used to’ the situation and our anxiety begins to fall. This may take around 30 minutes, but often happens more quickly. More importantly, if you subsequently confront the same situation again, the amount of anxiety you experience will be less and less on each occasion. Not only this, but it will pass more quickly each time too, until the point that the situation causes us little or no anxiety.
For instance, do you remember ever being nervous before starting a new job or college course? In these situations, it is normal to feel very anxious before you arrive. However once you arrive, often you gradually begin to feel more comfortable and relaxed as the day progresses. Not only this, as each day passes in your new surroundings, you usually begin to feel less and less nervous.
The same is true when you confront a situation that makes you anxious. Although your anxiety may be high beforehand and initially rise when you confront it, this will soon begin to drop if you remain in the situation for long enough. Following this, each time you confront the same situation, the levels of anxiety you experience will get less and less, just as it would as each day passed in a new job. Soon you should be able to confront such situations and feel minimal (if any) fear at all.
Remember your new knowledge about anxiety and panic should help you to stay in the situations you fear for long enough to allow this to happen. This is because it can help you to prevent cycles of panic occurring like they did in the past.
Agoraphobia symptoms
The severity of agoraphobia can vary significantly between individuals. For example, someone with severe agoraphobia may be unable to leave the house, whereas someone who has mild agoraphobia may be able to travel short distances without problems. Individuals with agoraphobia are fearful and anxious about two or more of the following situations: using public transportation; being in open spaces; being in enclosed places; standing in line or being in a crowd; or being outside of the home alone in other situations. The individual fears these situations because of thoughts that escape might be difficult or help might not be available in the event of developing panic-like symptoms or other incapacitating or embarrassing symptoms. These situations almost always induce fear or anxiety and are often avoided and require the presence of a companion.
Symptoms of agoraphobia include:
- Being afraid of spending time alone
- Being afraid of places where escape might be hard
- Being afraid of losing control in a public place
- Depending on others
- Feeling detached or separated from others
- Feeling helpless
- Feeling that the body is not real
- Feeling that the environment is not real
- Having an unusual temper or agitation
- Staying in the house for long periods
The symptoms of agoraphobia can be broadly classified into three types:
- Physical
- Cognitive
- Behavioral
These are explained in more detail below.
Physical symptoms
The physical symptoms of agoraphobia usually only occur when you find yourself in a situation or environment that causes anxiety. However, many people with agoraphobia rarely experience physical symptoms because they deliberately avoid situations that make them anxious.
The physical symptoms of agoraphobia can be similar to those of a panic attack and may include:
- rapid heartbeat
- rapid breathing (hyperventilating)
- shortness of breath
- feeling hot and sweaty
- feeling sick
- chest pain or discomfort
- difficulty swallowing (dysphagia)
- choking
- nausea or other stomach distress
- diarrhea
- trembling
- dizziness
- ringing in the ears (tinnitus)
- feeling faint or fainting
- trembling
Cognitive symptoms
The cognitive symptoms of agoraphobia are feelings or thoughts that can be, but aren’t always, related to the physical symptoms.
Cognitive symptoms may include fear that:
- a panic attack will make you look stupid or feel embarrassed in front of other people
- a panic attack will be life threatening – for example, you may be worried your heart will stop or you’ll be unable to breathe
- you would be unable to escape from a place or situation if you were to have a panic attack
- you’re losing your sanity
- you may lose control in public
- you may tremble and blush in front of people
- people may stare at you
There are also psychological symptoms that aren’t related to panic attacks, such as:
- feeling you would be unable to function or survive without the help of others
- a fear of being left alone in your house (monophobia)
- a general feeling of anxiety or dread
Behavioral symptoms
Symptoms of agoraphobia relating to behavior include:
- avoiding situations that could lead to panic attacks, such as crowded places, public transport and queues
- being housebound – not being able to leave the house for long periods of time
- needing to be with someone you trust when going anywhere
- avoiding being far away from home
Some people are able to force themselves to confront uncomfortable situations, but they feel considerable fear and anxiety while doing so.
Panic disorder and agoraphobia
Some people have a panic disorder in addition to agoraphobia. Panic disorder is a type of anxiety disorder in which you experience sudden attacks of extreme fear that reach a peak within a few minutes and trigger intense physical symptoms (panic attacks). You might think that you’re totally losing control, having a heart attack or even dying.
Fear of another panic attack can lead to avoiding similar circumstances or the place where it occurred in an attempt to prevent future panic attacks.
Signs and symptoms of a panic attack can include:
- Rapid heart rate
- Trouble breathing or a feeling of choking
- Chest pain or pressure
- Lightheadedness or dizziness
- Feeling shaky, numb or tingling
- Excessive sweating
- Sudden flushing or chills
- Upset stomach or diarrhea
- Feeling a loss of control
- Fear of dying
Agoraphobia complications
Agoraphobia is associated with significant distress and can greatly limit your life’s activities. If your agoraphobia is severe, you may not even be able to leave your home and dependent on others for anything that requires leaving your home. Without treatment, some people become housebound for years. You may not be able to visit with family and friends, go to school or work, run errands, or take part in other normal daily activities. You may become dependent on others for help. This can lead to self-medication with non-prescription medications or other substances. Agoraphobia is also associated with an increased risk of developing comorbid major depressive disorder, persistent depressive disorder (dysthymia), and substance use disorders.
Agoraphobia can also lead to or be associated with:
- Depression
- Alcohol or drug abuse while trying to self-medicate
- Other mental health disorders, including other anxiety disorders or personality disorders
- Be unable to function at work or in social situations
- Feel isolated, lonely, depressed, or suicidal.
Agoraphobia causes
The exact cause of agoraphobia is unknown. Most cases of agoraphobia develop as a complication of panic disorder and begins to fear situations or environments that might lead to another panic attack. Panic disorder is an anxiety disorder where you regularly have sudden attacks of panic and moments of intense fear. Everyone experiences feelings of anxiety and panic at certain times. It’s a natural response to stressful or dangerous situations. But for someone with panic disorder, feelings of anxiety, stress and panic occur regularly and at any time, often for no apparent reason. As with many mental health conditions, the exact cause of panic disorder isn’t fully understood. However, most experts think a combination of biological and psychological factors may be involved.
Recently, in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), published by the American Psychiatric Association, agoraphobia has been separated from panic disorder as an independent condition, based on the following findings. Agoraphobia could occur without panic symptoms 8, is not always secondary to panic symptoms 4 and there are differences in prevalence, sex specific incidence rate, and treatment outcome between agoraphobia and panic disorder 11. The DSM-5 further stratifies risk factors into three categories: temperamental (neuroticism, sensitivity to anxiety, and anxiety disorders), environmental (negative or traumatic events in childhood, and reduced warmth or overprotectiveness in childhood), and genetic and physiological predisposition.
Agoraphobia is usually first identified in young adults, with the mean age of diagnosis beginning in the mid to late twenties. There is no consensus on the childhood experiences, personality characteristics, or psychosocial risk factors that lead to a diagnosis of agoraphobia 1. However, factors such as parental overprotectiveness, the presence of childhood fears or night terrors, experience of grief or bereavement early in life, unhappy or traumatic childhoods, or genetic predisposition may contribute to the development of agoraphobia. Comorbid personality types include dependent, obsessive-compulsive, or otherwise “highly-neurotic” may also contribute to the development of agoraphobia 12.
Agoraphobia can sometimes develop if a person has a panic attack in places or specific situations where they occurred and then avoiding them.
They begin to worry so much about having another panic attack that they feel the symptoms of a panic attack returning when they’re in a similar situation or environment.
A minority of people with agoraphobia have no history of panic attacks. In these cases, their fear may be related to issues like a fear of crime, terrorism, illness, or being in an accident.
Traumatic events, such as bereavement, may contribute towards agoraphobia, as well as certain genes inherited from your parents.
Panic disorder
As with many mental health conditions, the exact cause of panic disorder isn’t fully understood. However, most experts think a combination of biological and psychological factors may be involved.
Biological factors
There are a number of theories about the type of biological factors that may be involved with panic disorders. These are outlined below.
‘Fight or flight’ reflex
One theory is panic disorder is closely associated with your body’s natural “fight or flight” reflex – its way of protecting you from stressful and dangerous situations.
Anxiety and fear cause your body to release hormones, such as adrenaline, and your breathing and heart rate are increased. This is your body’s natural way of preparing itself for a dangerous or stressful situation.
In people with panic disorder, it’s thought the fight or flight reflex may be triggered wrongly, resulting in a panic attack.
Neurotransmitters
Another theory is an imbalance in levels of neurotransmitters in the brain can affect mood and behavior. This can lead to a heightened stress response in certain situations, triggering the feelings of panic.
The fear network
The “fear network” theory suggests the brains of people with panic disorders may be wired differently from most people.
There may be a malfunction in parts of the brain known to generate both the emotion of fear and the corresponding physical effect fear can bring. They may be generating strong emotions of fear that trigger a panic attack.
Spatial awareness
Links have been found between panic disorders and spatial awareness. Spatial awareness is the ability to judge where you are in relation to other objects and people.
Some people with panic disorder have a weakened balance system and awareness of space. This can cause them to feel overwhelmed and disorientated in crowded places, triggering a panic attack.
Psychological factors
Psychological factors that increase your risk of developing agoraphobia include:
- a traumatic childhood experience, such as the death of a parent or being sexually abused
- experiencing a stressful event, such as bereavement, divorce, or losing your job
- a previous history of mental illnesses, such as depression, anorexia nervosa, or bulimia
- alcohol misuse or drug misuse
- being in an unhappy relationship, or in a relationship where your partner is very controlling
What keeps your panic and agoraphobia going?
Unhelpful thoughts
People with unhelpful thoughts make it more difficult for them to overcome their panic and agoraphobia. For example, because people interpret symptoms of anxiety as dangerous (e.g. a sign of a heart attack or going crazy), they actually make themselves even more anxious. To illustrate, someone may notice a change in their breathing and think this is a sign that they are about to choke and die, as opposed to a normal physical symptom of anxiety. Another example could be believing that their increased heart rate is a sign they are about to have a heart attack. As soon as people think in these catastrophic terms, they make themselves even more anxious and their physical symptoms get stronger. Of course, as their physical symptoms grow stronger, so does their belief that they are going to choke or have a heart attack. This creates a vicious cycle that often leads to a full blown panic attack.
The unhelpful thoughts people have about being unable to cope in certain situations also keeps their panic and agoraphobia going. For instance, they may believe that because they had a panic attack whilst shopping once, they will have another one every time they shop in the future. This of course stops them from ever trying and they don’t have the chance to prove otherwise.
Avoidance
As you have learned, people tend to avoid or escape situations that they believe will trigger a panic attack (e.g. buses, restaurants, the countryside, the cinema etc). Although this is a very understandable way of coping, it is actually one of the main reasons that people find it hard to overcome their difficulties. This is because by avoiding these situations, people prevent themselves from having the opportunity to prove that they can cope in them better than they think. Furthermore, the longer someone has been afraid of a situation and avoided it, the more daunting it becomes and it is increasingly difficult to face. Not only this, but when people avoid one situation, they begin to doubt they will cope in similar situations and start avoiding more and more. Soon their fear generalizes to the point that their lifestyle is extremely restricted.
Using Safety Behaviors
Often, the only time that someone with symptoms of panic and agoraphobia feels capable of facing their feared situations, is when they use what is known as a ‘safety behavior.’ An example of a safety behavior would be: only going into town if you are with someone you trust (to come to your rescue if you panic), gripping tightly onto a shopping trolley (to reduce the chances of fainting), or lying or sitting down when you feel anxious (to avoid fainting). Basically, a safety behavior is anything people do to try and make it easier for them to cope with their fears.
Although such safety behaviors help people cope with symptoms of panic and agoraphobia in the short term, they are actually unhelpful in the longer term. This is because, like avoidance, safety behaviors stop people from having the opportunity to prove to themselves that they can cope with their fears, without putting such precautions into place. Instead they may put their successes down to other factors (e.g. “I only coped because I had my friend with me” or “I would’ve fainted if it wasn’t for my trolley”) and their fears remain in place. Before long people become reliant on their safety behaviors and avoid going places when they are unable to use them.
Increased Self Focus
Another factor that helps keep people’s panic and agoraphobia going is their tendency to be hypervigilant. This means that they study their body for any sign of physical changes that may suggest a panic attack is on its way. Although they do this, hoping to be reassured that everything feels normal, this strategy actually makes things worse. This is because they tend to notice small physical changes that would have otherwise gone unnoticed (e.g. feeling hot). Once a small change has been noticed, people naturally ‘keep their eye’ on it. However, the more they focus on a change, the more anxious they become and a vicious cycle begins that can lead to a panic attack. Alternatively, if people notice a change due to hypervigilance, they tend to escape the situation that has triggered it. However, as we know, this strategy is unhelpful too.
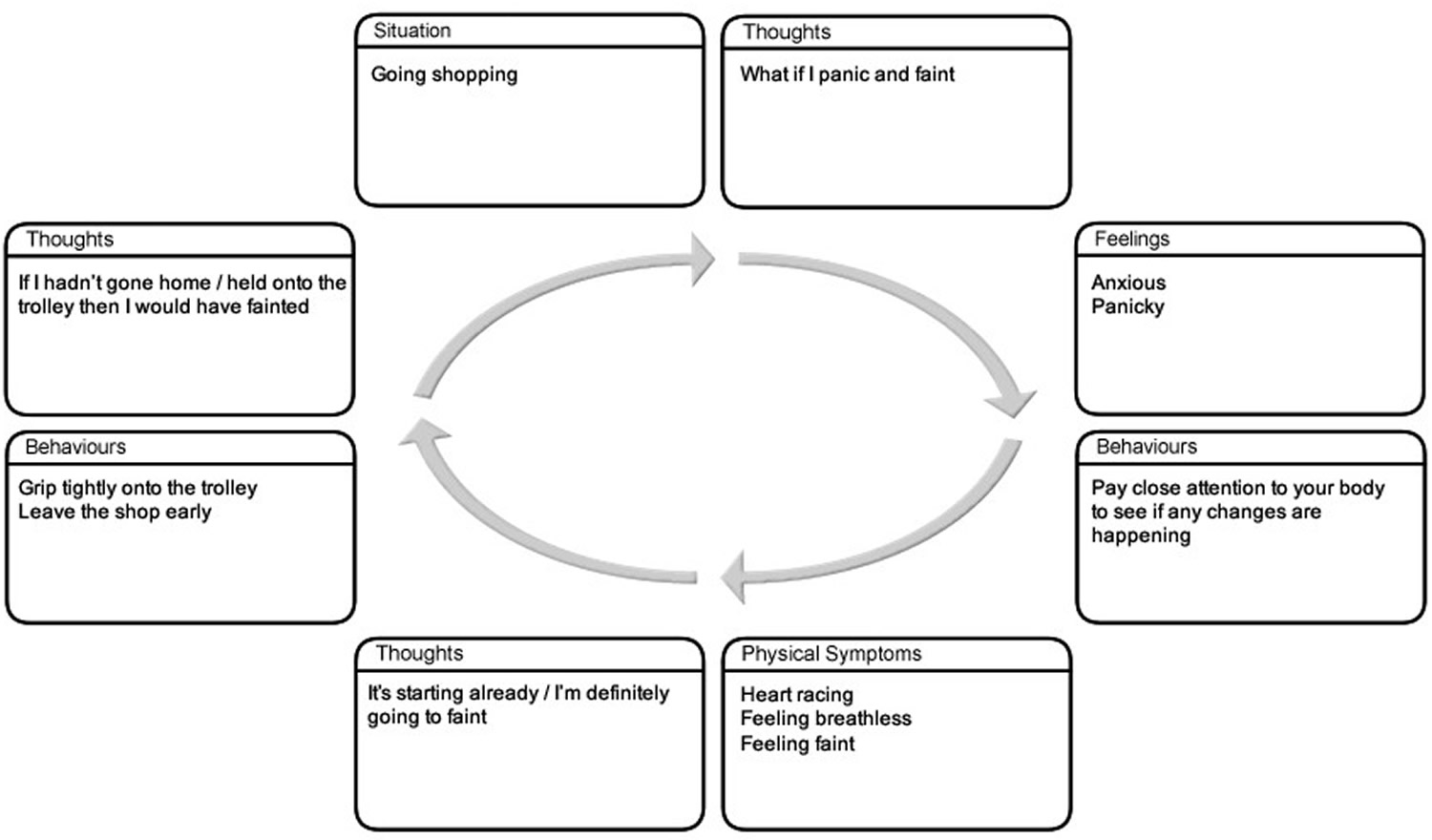
It is likely that a combination of all these factors play a role in keeping your panic and agoraphobia going. See figure 1 for an illustration of how these factors can interact and make it difficult for us to overcome our panic and agoraphobia.
Figure 1. What keeps your panic and agoraphobia going
Agoraphobia without panic disorder
Occasionally, a person can develop symptoms of agoraphobia even though they don’t have a history of panic disorder or panic attacks.
This type of agoraphobia can be triggered by a number of different irrational fears (phobias), such as the fear of:
- being a victim of violent crime or a terrorist attack if you leave your house
- becoming infected by a serious illness if you visit crowded places
- doing something by accident that will result in you embarrassing or humiliating yourself in front of others
Risk factors for developing agoraphobia
Agoraphobia can begin in childhood, but usually starts in the late teen or early adult years — usually before age 35 — but older adults can also develop it. Women are diagnosed with agoraphobia more often than men are.
Risk factors for agoraphobia include:
- Having panic disorder or other phobias
- Responding to panic attacks with excessive fear and avoidance
- Experiencing stressful life events, such as abuse, the death of a parent or being attacked
- Having an anxious or nervous temperament
- Having a blood relative with agoraphobia
Agoraphobia prevention
There’s no sure way to prevent agoraphobia. However, anxiety tends to increase the more you avoid situations that you fear. If you start to have mild fears about going places that are safe, try to practice going to those places over and over again before your fear becomes overwhelming. If this is too hard to do on your own, ask a family member or friend to go with you, or seek professional help.
If you experience anxiety going places or have panic attacks, get treatment as soon as possible. Get help early to keep symptoms from getting worse. Anxiety, like many other mental health conditions, can be harder to treat if you wait.
Agoraphobia diagnosis
Speak to your doctor if you think you may be affected by agoraphobia. If you’re unable to visit your doctor in person or you don’t feel ready to visit your doctor in person, it should be possible to arrange a telephone consultation.
Your doctor will ask you to describe your symptoms, how often they occur, and in what situations. It’s very important to tell your doctor about how you’ve been feeling and how your symptoms are affecting you.
Your doctor also want to know how your symptoms are affecting your daily behavior. Your doctor may ask you the following questions:
- Do you find leaving your house stressful?
- Are there certain places or situations you have to avoid?
- Do you have any avoidance strategies to help you cope with your symptoms, such as relying on others to shop for you?
It can sometimes be difficult to talk to someone else about your feelings, emotions, and personal life, but try not to feel anxious or embarrassed. Your doctor needs to know as much as possible about your symptoms to make the correct diagnosis and recommend the most appropriate treatment.
Agoraphobia is diagnosed based on:
- Signs and symptoms
- In-depth interview with your doctor or a mental health professional
- Physical exam to rule out other conditions that could be causing your symptoms
- Criteria for agoraphobia listed in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), published by the American Psychiatric Association
Physical examination
Your doctor may want to do a physical examination, and in some cases they may decide to carry out blood tests to look for signs of any physical conditions that could be causing your symptoms.
For example, an overactive thyroid gland (hyperthyroidism) can sometimes cause symptoms that are similar to the symptoms of a panic attack.
By ruling out any underlying medical conditions, your doctor will be able to make the correct diagnosis.
Confirming the diagnosis
To definitively diagnose a patient with agoraphobia, you must have intense fear in response to or when anticipating entering into at least two of the five following situations:
- using public transportation (automobiles, buses, trains),
- being in open spaces (marketplaces, parking lots),
- being in enclosed spaces like theaters or malls,
- standing in lines or crowds, or
- being outside of the home alone.
This fear, which is out of proportion to the actual stimulus, must be accompanied by behavioral or cognitive modifications to avoid placing oneself in situations where the exposure may occur. These symptoms must be present for at least six months and must cause significant distress to the patient and impairment in their lives. The symptoms also should not be better explained by another psychiatric diagnosis, be directly caused by a medical diagnosis, or occur in the context of substance use or withdrawal.
If there’s any doubt about the diagnosis, you may be referred to a psychiatrist for a more detailed assessment.
Agoraphobia DSM 5 Diagnostic Criteria
The DSM-5 outlines the criteria by which a diagnosis of agoraphobia is possible 13:
- Criterion A. Marked fear or anxiety about two (or more) of the following five situations:
- Using public transportation (e.g., automobiles, buses, trains, ships, planes).
- Being in open spaces (e.g., parking lots, marketplaces, bridges).
- Being in enclosed places (e.g., shops, theaters, cinemas).
- Standing in line or being in a crowd.
- Being outside of the home alone.
- Criterion B. The individual fears or avoids these situations because of thoughts that escape might be difficult or help might not be available in the event of developing panic-like symptoms or other incapacitating or embarrassing symptoms (e.g., fear of falling in the elderly; fear of incontinence).
- Criterion C. The agoraphobic situations almost always provoke fear or anxiety.
- Criterion D. The agoraphobic situations are actively avoided, require the presence of a companion, or are endured with intense fear or anxiety.
- Criterion E. The fear or anxiety is out of proportion to the actual danger posed by the agoraphobic situations and to the sociocultural context.
- Criterion F. The fear, anxiety, or avoidance is persistent, typically lasting for 6 months or more.
- Criterion G. The fear, anxiety, or avoidance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
- Criterion H. If another medical condition (e.g., inflammatory bowel disease, Parkinson’s disease) is present, the fear, anxiety, or avoidance is clearly excessive.
- Criterion I. The fear, anxiety, or avoidance is not better explained by the symptoms of another mental disorder—for example, the symptoms are not confined to specific phobia, situational type; do not involve only social situations (as in social anxiety disorder): and are not related exclusively to obsessions (as in obsessive-compulsive disorder), perceived defects or flaws in physical appearance (as in body dysmoφhic disorder), reminders of traumatic events (as in posttraumatic stress disorder), or fear of separation (as in separation anxiety disorder).
Note: Agoraphobia is diagnosed irrespective of the presence of panic disorder. If an individual’s presentation meets criteria for panic disorder and agoraphobia, both diagnoses should be assigned.
The essential feature of agoraphobia is marked, or intense, fear or anxiety triggered by the real or anticipated exposure to a wide range of situations (Criterion A). The diagnosis requires endorsement of symptoms occurring in at least two of the following five situations:
- using public transportation, such as automobiles, buses, trains, ships, or planes;
- being in open spaces, such as parking lots, marketplaces, or bridges;
- being in enclosed spaces, such as shops, theaters, or cinemas;
- standing in line or being in a crowd; or
- being outside of the home alone.
The examples for each situation are not exhaustive; other situations may be feared. When experiencing fear and anxiety cued by such situations, individuals typically experience thoughts that something terrible might happen (Criterion B). Individuals frequently believe that escape from such situations might be difficult (e.g., “can’t get out of here”) or that help might be unavailable (e.g., “there is nobody to help me”) when panic-like symptoms or other incapacitating or embarrassing symptoms occur. “Panic-like symptoms” refer to any of the 13 symptoms included in the criteria for panic attack, such as dizziness, faintness, and fear of dying. “Other incapacitating or embarrassing symptoms” include symptoms such as vomiting and inflammatory bowel symptoms, as well as, in older adults, a fear of falling or, in children, a sense of disorientation and getting lost.
The amount of fear experienced may vary with proximity to the feared situation and may occur in anticipation of or in the actual presence of the agoraphobic situation. Also, the fear or anxiety may take the form of a full- or limited-symptom panic attack (i.e., an expected panic attack). Fear or anxiety is evoked nearly every time the individual comes into contact with the feared situation (Criterion C). Thus, an individual who becomes anxious only occasionally in an agoraphobic situation (e.g., becomes anxious when standing in line on only one out of every five occasions) would not be diagnosed with agoraphobia. The individual actively avoids the situation or, if he or she either is unable or decides not to avoid it, the situation evokes intense fear or anxiety (Criterion D). Active avoidance means the individual is currently behaving in ways that are intentionally designed to prevent or minimize contact with agoraphobic situations. Avoidance can be behavioral (e.g., changing daily routines, choosing a job nearby to avoid using public transportation, arranging for food delivery to avoid entering shops and supermarkets) as well as cognitive (e.g., using distraction to get through agoraphobic situations) in nature. The avoidance can become so severe that the person is completely homebound. Often, an individual is better able to confront a feared situation when accompanied by a companion, such as a partner, friend, or health professional.
The fear, anxiety, or avoidance must be out of proportion to the actual danger posed by the agoraphobic situations and to the sociocultural context (Criterion E). Differentiating clinically significant agoraphobic fears from reasonable fears (e.g., leaving the house during a bad storm) or from situations that are deemed dangerous (e.g., walking in a parking lot or using public transportation in a high-crime area) is important for a number of reasons. First, what constitutes avoidance may be difficult to judge across cultures and sociocultural contexts (e.g., it is socioculturally appropriate for orthodox Muslim women in certain parts of the world to avoid leaving the house alone, and thus such avoidance would not be considered indicative of agoraphobia). Second, older adults are likely to overattribute their fears to age-related constraints and are less likely to judge their fears as being out of proportion to the actual risk. Third, individuals with agoraphobia are likely to overestimate danger in relation to panic-like or other bodily symptoms. Agoraphobia should be diagnosed only if the fear, anxiety, or avoidance persists (Criterion F) and if it causes clinically significant distress or impairment in social, occupational, or other important areas of functioning (Criterion G). The duration of “typically lasting for 6 months or more” is meant to exclude individuals with short-lived, transient problems. However, the duration criterion should be used as a general guide, with allowance for some degree of flexibility.
Associated features supporting the diagnosis
In its most severe forms, agoraphobia can cause individuals to become completely homebound, unable to leave their home and dependent on others for services or assistance to provide even for basic needs. Demoralization and depressive symptoms, as well as abuse of alcohol and sedative medication as inappropriate self-medication strategies, are common.
Agoraphobia treatment
The goal of agoraphobia treatment is to help you feel and function better. The success of treatment usually depends in part on how severe the agoraphobia is. Agoraphobia treatment usually includes both psychotherapy and medication. Psychotherapy involves working with a therapist to set goals and learn practical skills to reduce your anxiety symptoms. Cognitive behavioral therapy (CBT) is one of the most effective forms of psychotherapy for anxiety disorders, including agoraphobia. It may take some time, but treatment can help you get better.
A stepwise approach is usually recommended for treating agoraphobia and any underlying panic disorder.
The steps are as follows:
- Find out more about your condition, the lifestyle changes you can make, and self-help techniques to help relieve symptoms.
- Enrol yourself on a guided self-help programme.
- Undertake more intensive treatments, such as cognitive behavioral therapy (CBT), or see if your symptoms can be controlled using medication.
Studies have generally concluded that cognitive-behavioral therapy (CBT) effectively addresses and alleviates target symptoms, lessens other anxiety symptoms, and improves the patient’s quality of life 14. For patients with more severe forms of agoraphobia or for those who prefer medication over psychotherapy, there are several effective options for medication management. Selective serotonin receptor inhibitors (SSRIs) are generally considered first-line therapy, with therapeutic doses being the same as in depression 15. Serotonin-norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), and benzodiazepines have also been effective alternatives SSRIs in the treatment of panic disorder and agoraphobia 16. SSRIs are generally preferable to these other medications because of the side effect profile, affordability, availability, decreased potential for abuse, and better tolerability 17. There is also data suggesting that the combination of CBT with medication may be most effective in the symptomatic management of agoraphobia and panic disorder 18.
The various treatments for agoraphobia are outlined below.
Lifestyle changes and self-help techniques
Learning more about agoraphobia and its association with panic disorder and panic attacks may help you control your symptoms better. For example, there are techniques you can use during a panic attack to bring your emotions under control.
Having more confidence in controlling your emotions may make you more confident coping with previously uncomfortable situations and environments.
These self-help techniques are described below:
- Stay where you are – try to resist the urge to run to a place of safety during a panic attack; if you’re driving, pull over and park where it’s safe to do so.
- Focus – it’s important for you to focus on something non-threatening and visible, such as the time passing on your watch, or items in a supermarket; remind yourself the frightening thoughts and sensations are a sign of panic and will eventually pass.
- Breathe slowly and deeply – feelings of panic and anxiety can get worse if you breathe too quickly; try to focus on slow, deep breathing while counting slowly to three on each breath in and out.
- Challenge your fear – try to work out what it is you fear and challenge it; you can achieve this by constantly reminding yourself that what you fear isn’t real and will pass.
- Creative visualization – during a panic attack, try to resist the urge to think negative thoughts, such as “disaster”; instead, think of a place or situation that makes you feel peaceful, relaxed or at ease: once you have this image in your mind, try to focus your attention on it.
- Don’t fight an attack – trying to fight the symptoms of a panic attack can often make things worse; instead, reassure yourself by accepting that although it may seem embarrassing and your symptoms may be difficult to deal with, the attack isn’t life threatening.
Making some lifestyle changes can also help. For example, ensure you:
- take regular exercise – exercise can help relieve stress and tension and improve your mood
- have a healthy diet – a poor diet can make the symptoms of panic and anxiety worse
- avoid using drugs and alcohol – they may provide short-term relief, but in the long term they can make symptoms worse
- avoid drinks containing caffeine, such as tea, coffee or cola – caffeine has a stimulant effect and can make your symptoms worse
Guided self-help
If your symptoms don’t respond to these self-help techniques and lifestyle changes, your doctor may recommend enrolling on a guided self-help programme. This involves working through self-help manuals that cover the types of issues you might be facing, along with practical advice about how to deal with them.
Guided self-help for agoraphobia is based on cognitive behavioral therapy (CBT), which aims to change unhelpful and unrealistic patterns of thinking to bring about positive changes in behavior.
In turn, cognitive behavioral therapy (CBT) uses a type of therapy called exposure therapy, which involves being gradually exposed to the object or situation you fear and using relaxation techniques and breathing exercises to help reduce your anxiety.
As part of the programme, you may have brief sessions with a cognitive behavioral therapy (CBT) therapist – around 20 to 30 minutes long – over the telephone or face to face. You may also be invited to take part in group work with other people with a history of agoraphobia and panic disorders.
Most self-help programmes consist of a series of goals to work towards over the course of five to six weeks.
More intensive therapies
If the self-help programme hasn’t worked, you may be referred for more intensive therapies. There are three main options:
- CBT with a therapist
- applied relaxation
- medication
Cognitive behavioral therapy (CBT)
Cognitive behavioral therapy (CBT) is based on the idea that unhelpful and unrealistic thinking leads to negative behavior. CBT aims to break this cycle and find new ways of thinking that can help you behave more positively. Cognitive behavioral therapy focuses on teaching you specific skills to better tolerate anxiety, directly challenge your worries and gradually return to the activities you’ve avoided because of anxiety. Through this process, your symptoms improve as you build on your initial success. For example, many people with agoraphobia have the unrealistic thought that if they have a panic attack it will kill them.
The CBT therapist will try to encourage a more positive way of thinking – for example, although having a panic attack may be unpleasant, it isn’t fatal and will pass. This shift in thinking can lead to more positive behavior in terms of a person being more willing to confront situations that previously scared them.
Generally with cognitive behavioral therapy (CBT) you can learn:
- What factors may trigger a panic attack or panic-like symptoms and what makes them worse
- How to cope with and tolerate symptoms of anxiety
- Ways to directly challenge your worries, such as the likelihood of bad things happening in social situations
- That your anxiety gradually decreases if you remain in situations and that you can manage these symptoms until they do
- How to change unwanted or unhealthy behaviors through desensitization, also called exposure therapy, to safely face the places and situations that cause fear and anxiety
If you have trouble leaving your home, you may wonder how you could possibly go to a therapist’s office. Therapists who treat agoraphobia are well aware of this problem.
If you feel homebound due to agoraphobia, look for a therapist who can help you find alternatives to office appointments, at least in the early part of treatment. He or she may offer to see you first in your home or meet you in what you consider a safe place (safe zone). Some therapists may also offer some sessions over the phone, through email, or using computer programs or other media.
If the agoraphobia is so severe that you cannot access care, you might benefit from a more intensive hospital program that specializes in the treatment of anxiety.
You may want to take a trusted relative or friend to your appointment who can offer comfort, help and coaching, if needed.
CBT is usually combined with exposure therapy. Your therapist will set relatively modest goals at the start of treatment, such as going to your local corner shop. As you become more confident, more challenging goals can be set, such as going to a large supermarket or having a meal in a busy restaurant.
A course of CBT usually consists of 12 to 15 weekly sessions, with each session lasting about an hour.
Applied relaxation
Applied relaxation is based on the premise that people with agoraphobia and related panic disorder have lost their ability to relax. The aim of applied relaxation is therefore to teach you how to relax.
This is achieved using a series of exercises designed to teach you how to:
- spot the signs and feelings of tension
- relax your muscles to relieve tension
- use these techniques in stressful or everyday situations to prevent you feeling tense and panicky
As with CBT, a course of applied relaxation therapy consists of 12 to 15 weekly sessions, with each one lasting about an hour.
Agoraphobia medication
In some cases, medication can be used as a sole treatment for agoraphobia. Antidepressants are more effective than anti-anxiety medications in the treatment of agoraphobia. In more severe cases, it can also be used in combination with CBT or applied relaxation therapy.
- Antidepressants. Certain antidepressants called selective serotonin reuptake inhibitors (SSRIs), such as fluoxetine (Prozac) and sertraline (Zoloft), are used for the treatment of panic disorder with agoraphobia. Other types of antidepressants may also effectively treat agoraphobia.
- Anti-anxiety medication. Anti-anxiety drugs called benzodiazepines are sedatives that, in limited circumstances, your doctor may prescribe to temporarily relieve anxiety symptoms. Benzodiazepines are generally used only for relieving acute anxiety on a short-term basis. Because they can be habit-forming, these drugs aren’t a good choice if you’ve had long-term problems with anxiety or problems with alcohol or drug abuse.
It may take weeks for medication to relieve symptoms. And you may have to try several different medications before you find one that works best for you.
Both starting and ending a course of antidepressants can cause side effects that create uncomfortable physical sensations or even panic attack symptoms. For this reason, your doctor likely will gradually increase your dose during treatment, and slowly decrease your dose when he or she feels you’re ready to stop taking medication.
Selective serotonin reuptake inhibitors (SSRIs)
If medication is recommended for you, you’ll usually be prescribed a course of selective serotonin reuptake inhibitors (SSRIs).
Selective serotonin reuptake inhibitors (SSRIs) were originally developed to treat depression, but they’ve subsequently proved effective for helping treat other mood disorders, such as anxiety, feelings of panic, and obsessional thoughts.
An SSRI called sertraline is usually recommended for people with agoraphobia. Side effects associated with sertraline include:
- feeling sick
- loss of sex drive (libido)
- blurred vision
- diarrhea or constipation
- feeling agitated or shaky
- excessive sweating
These side effects should improve over time, although some can occasionally persist.
If sertraline fails to improve your symptoms, you may be prescribed an alternative selective serotonin reuptake inhibitor (SSRI) or a similar type of medication known as serotonin-norepinephrine reuptake inhibitors (SNRIs).
The length of time you’ll have to take an selective serotonin reuptake inhibitor (SSRI) or serotonin-norepinephrine reuptake inhibitor (SNRI) for will vary depending on your response to treatment. Some people may have to take SSRIs for 6 to 12 months or more.
When you and your doctor decide it’s appropriate for you to stop taking SSRIs, you’ll be weaned off them by slowly reducing your dosage. You should never stop taking your medication unless your doctor specifically advises you to.
Pregabalin
If you’re unable to take selective serotonin reuptake inhibitors (SSRIs) or serotonin-norepinephrine reuptake inhibitors (SNRIs) for medical reasons or you experience troublesome side effects, another medication called pregabalin may be recommended. Dizziness and drowsiness are common side effects of pregabalin.
Benzodiazepines
If you experience a particularly severe flare-up of panic-related symptoms, you may be prescribed a short course of benzodiazepines. These are tranquilizers designed to reduce anxiety and promote calmness and relaxation.
Taking benzodiazepines for longer than two weeks in a row isn’t usually recommended as they can become addictive.
Alternative medicine
Certain dietary and herbal supplements claim to have calming and anti-anxiety benefits. Before you take any of these for agoraphobia, talk with your doctor. Although these supplements are available without a prescription, they still pose possible health risks.
For example, the herbal supplement kava, also called kava kava, appeared to be a promising treatment for anxiety, but there have been reports of serious liver damage, even with short-term use. The Food and Drug Administration has issued warnings but not banned sales in the United States. Avoid using any product that contains kava until more-rigorous safety studies are done, especially if you have liver problems or take medications that affect your liver.
Coping and support
Living with agoraphobia can make life difficult. Professional treatment can help you overcome this disorder or manage it effectively so that you don’t become a prisoner to your fears.
You can also take these steps to cope and care for yourself when you have agoraphobia:
- Stick to your treatment plan. Take medications as directed. Keep therapy appointments. Communicate regularly with your therapist. Consistency can make a big difference, especially when it comes to practicing skills and taking your medication.
- Try not to avoid feared situations. It’s hard to go to places or be in situations that make you uncomfortable or that bring on symptoms of anxiety. But practicing going to more and more places can make them less frightening and anxiety provoking. Family, friends and your therapist can help you work on this.
- Learn calming skills. Working with your therapist, you can learn how to calm and soothe yourself. Meditation, yoga, massage and visualization are simple relaxation techniques that also may help. Practice these techniques when you aren’t anxious or worried, and then put them into action during stressful situations.
- Avoid alcohol and recreational drugs. Also limit or avoid caffeine. These substances can worsen your panic or anxiety symptoms.
- Take care of yourself. Get enough sleep, be physically active every day, and eat a healthy diet, including lots of vegetables and fruits.
- Join a support group. Support groups for people with anxiety disorders can help you connect to others facing similar challenges and share experiences.
- Anxiety and Depression Association of America (https://adaa.org/supportgroups)
- Anxiety Care UK (https://anxietycare.org.uk/)
- Mind in England & Wales (https://www.mind.org.uk/)
- Beyond Blue Australia (https://www.beyondblue.org.au/)
Agoraphobia prognosis
The DSM-5 describes the course of agoraphobia as “persistent and chronic,” with complete remission being relatively rare (10%) except with treatment or intervention 13. Most people can get better with medicines and cognitive behavioral therapy (CBT). Around a third of people with agoraphobia eventually achieve a complete cure and remain free from symptoms. Around half experience an improvement in symptoms, but they may have periods when their symptoms become more troublesome – for example, if they feel stressed. Despite treatment, about one in five people with agoraphobia continue to experience troublesome symptoms.
Without early and effective help, agoraphobia may become harder to treat. Rates of remission are reduced when the severity of agoraphobia is higher. A range of other disorders, in particular other anxiety disorders, depressive disorders, substance use disorders, and personality disorders, may complicate the course of agoraphobia. The chance of a favorable prognosis is also reduced by the presence of comorbid anxiety disorders, depression, personality disorders, or substance use disorders 19. The DSM-5 states that remission rates without treatment are quite low, with averages estimated at about 10% 19.
References- Balaram K, Marwaha R. Agoraphobia. [Updated 2022 Jun 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554387
- Noyes R Jr, Crowe RR, Harris EL, Hamra BJ, McChesney CM, Chaudhry DR. Relationship between panic disorder and agoraphobia. A family study. Arch Gen Psychiatry. 1986 Mar;43(3):227-32. doi: 10.1001/archpsyc.1986.01800030037004
- Shin J, Park DH, Ryu SH, Ha JH, Kim SM, Jeon HJ. Clinical implications of agoraphobia in patients with panic disorder. Medicine (Baltimore). 2020 Jul 24;99(30):e21414. doi: 10.1097/MD.0000000000021414
- Grant BF, Hasin DS, Stinson FS, Dawson DA, Goldstein RB, Smith S, Huang B, Saha TD. The epidemiology of DSM-IV panic disorder and agoraphobia in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions. J Clin Psychiatry. 2006 Mar;67(3):363-74. doi: 10.4088/jcp.v67n0305
- Roest AM, de Vries YA, Lim CCW, Wittchen HU, Stein DJ, Adamowski T, Al-Hamzawi A, Bromet EJ, Viana MC, de Girolamo G, Demyttenaere K, Florescu S, Gureje O, Haro JM, Hu C, Karam EG, Caldas-de-Almeida JM, Kawakami N, Lépine JP, Levinson D, Medina-Mora ME, Navarro-Mateu F, O’Neill S, Piazza M, Posada-Villa JA, Slade T, Torres Y, Kessler RC, Scott KM, de Jonge P; WHO World Mental Health Survey Collaborators. A comparison of DSM-5 and DSM-IV agoraphobia in the World Mental Health Surveys. Depress Anxiety. 2019 Jun;36(6):499-510. doi: 10.1002/da.22885
- Kim JBJC. A comparison study between panic disorder with agoraphobia and panic disorder without agoraphobia. J Korean Soc Biol Ther Psychiatry 1998;4:196–203.
- Maier W, Roth M, Buller R, et al. Agoraphobia in panic disorder: an indicator of the severity of panic disorder or a distinct diagnostic entity? Psychiatr Ann 1991;21:374–81.
- Asmundson GJ, Taylor S, Smits JA. Panic disorder and agoraphobia: an overview and commentary on DSM-5 changes. Depress Anxiety. 2014 Jun;31(6):480-6. doi: 10.1002/da.22277
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Press; 2013.
- Harvard Medical School, 2007. National Comorbidity Survey (NCS). https://www.hcp.med.harvard.edu/ncs/index.php
- Kessler RC, Chiu WT, Jin R, Ruscio AM, Shear K, Walters EE. The epidemiology of panic attacks, panic disorder, and agoraphobia in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2006 Apr;63(4):415-24. doi: 10.1001/archpsyc.63.4.415
- Tearnan BH, Telch MJ, Keefe P. Etiology and onset of agoraphobia: a critical review. Compr Psychiatry. 1984 Jan-Feb;25(1):51-62. doi: 10.1016/0010-440x(84)90022-1
- American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders (Fifth ed.). Arlington, VA: American Psychiatric Publishing. ISBN 978-0-89042-555-8.
- Carpenter, J. K., Andrews, L. A., Witcraft, S. M., Powers, M. B., Smits, J., & Hofmann, S. G. (2018). Cognitive behavioral therapy for anxiety and related disorders: A meta-analysis of randomized placebo-controlled trials. Depression and anxiety, 35(6), 502–514. https://doi.org/10.1002/da.22728
- Otto MW, Tuby KS, Gould RA, McLean RY, Pollack MH. An effect-size analysis of the relative efficacy and tolerability of serotonin selective reuptake inhibitors for panic disorder. Am J Psychiatry. 2001 Dec;158(12):1989-92. doi: 10.1176/appi.ajp.158.12.1989
- Plag J, Petzold MB, Gechter J, Liebscher C, Ströhle A. Patients’ characteristics and their influence on course of fear during agoraphobic symptom provocation: may SS(N)RI treatment compensate unfavorable individual preconditions? Nord J Psychiatry. 2018 Jul;72(5):325-335. doi: 10.1080/08039488.2018.1457178
- Pollack MH, Lepola U, Koponen H, Simon NM, Worthington JJ, Emilien G, Tzanis E, Salinas E, Whitaker T, Gao B. A double-blind study of the efficacy of venlafaxine extended-release, paroxetine, and placebo in the treatment of panic disorder. Depress Anxiety. 2007;24(1):1-14. doi: 10.1002/da.20218
- Furukawa, T. A., Watanabe, N., & Churchill, R. (2007). Combined psychotherapy plus antidepressants for panic disorder with or without agoraphobia. The Cochrane database of systematic reviews, 2007(1), CD004364. https://doi.org/10.1002/14651858.CD004364.pub2
- Balaram K, Marwaha R. Agoraphobia. [Updated 2021 Mar 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554387





{kind=link}