What is the amniotic sac
The amniotic sac is the bag of membranes containing the growing fetus and the amniotic fluid inside the uterus. The amniotic sac is filled with amniotic fluid. The amniotic sac forms about 12 days after getting pregnant and is completely formed within the first 3 weeks of pregnancy. Amniotic sac filled with fluid acts as a cushion to protect the developing fetus. The outer membrane of the amniotic sac is called the amnion, and an outer layer known as the chorion. The internal amniotic sac cavity is filled with amniotic fluid. This fluid buffers the developing embryo and fetus from physical shock until the time of birth. Normal amounts of amniotic fluid may vary, but, generally, women carry about 500 to 1000 ml of amniotic fluid. Amniotic fluid helps protect and cushion the fetus and plays an important role in the development of many of the fetal organs including the lungs, kidneys, and gastrointestinal tract. Amniotic fluid is produced by the fetal lungs and kidneys. It is taken up with fetal swallowing and sent across the placenta to the mother’s circulation. Too much or too little amniotic fluid is associated with abnormalities in development and pregnancy complications. Differences in the amount of fluid may be the cause or the result of the problem.
With further development of the fetus, specifically the fetal urinary system, the fluid in this potential space increases as the developing fetus excretes urine. Fetal urine comprises most of the amniotic fluid. Typically, the amniotic sac remains intact throughout the duration of gestation, and the amniotic membranes will spontaneously rupture, releasing the amniotic fluid either immediately preceding spontaneous labor or sometimes after the onset of spontaneous labor 1. You may have heard the expression, “The mother’s water broke just before she gave birth.” This refers to the rupture of the amniotic sac and release of its amniotic fluid near the start of labor, the process that expels the mature fetus from the uterus.
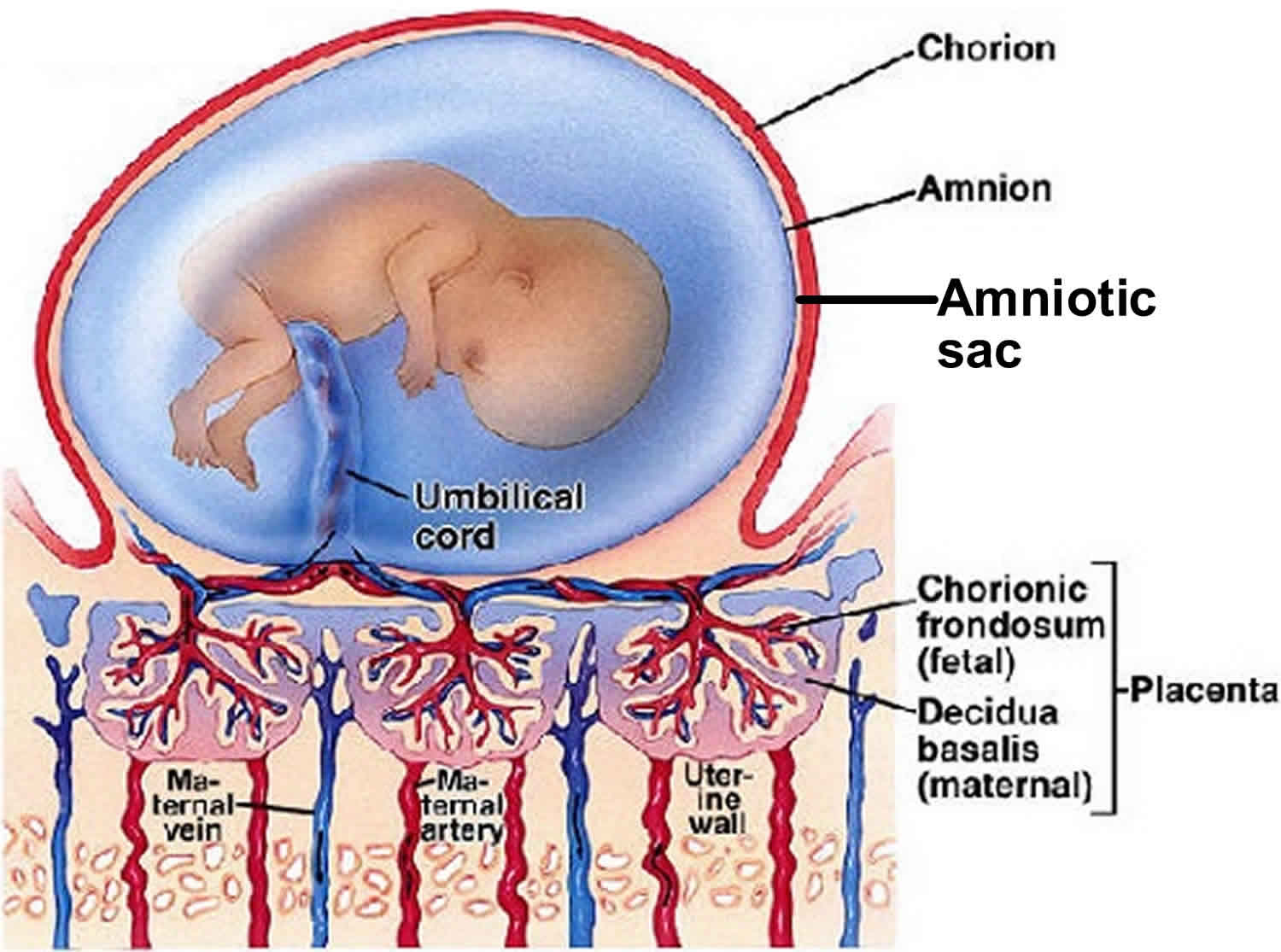
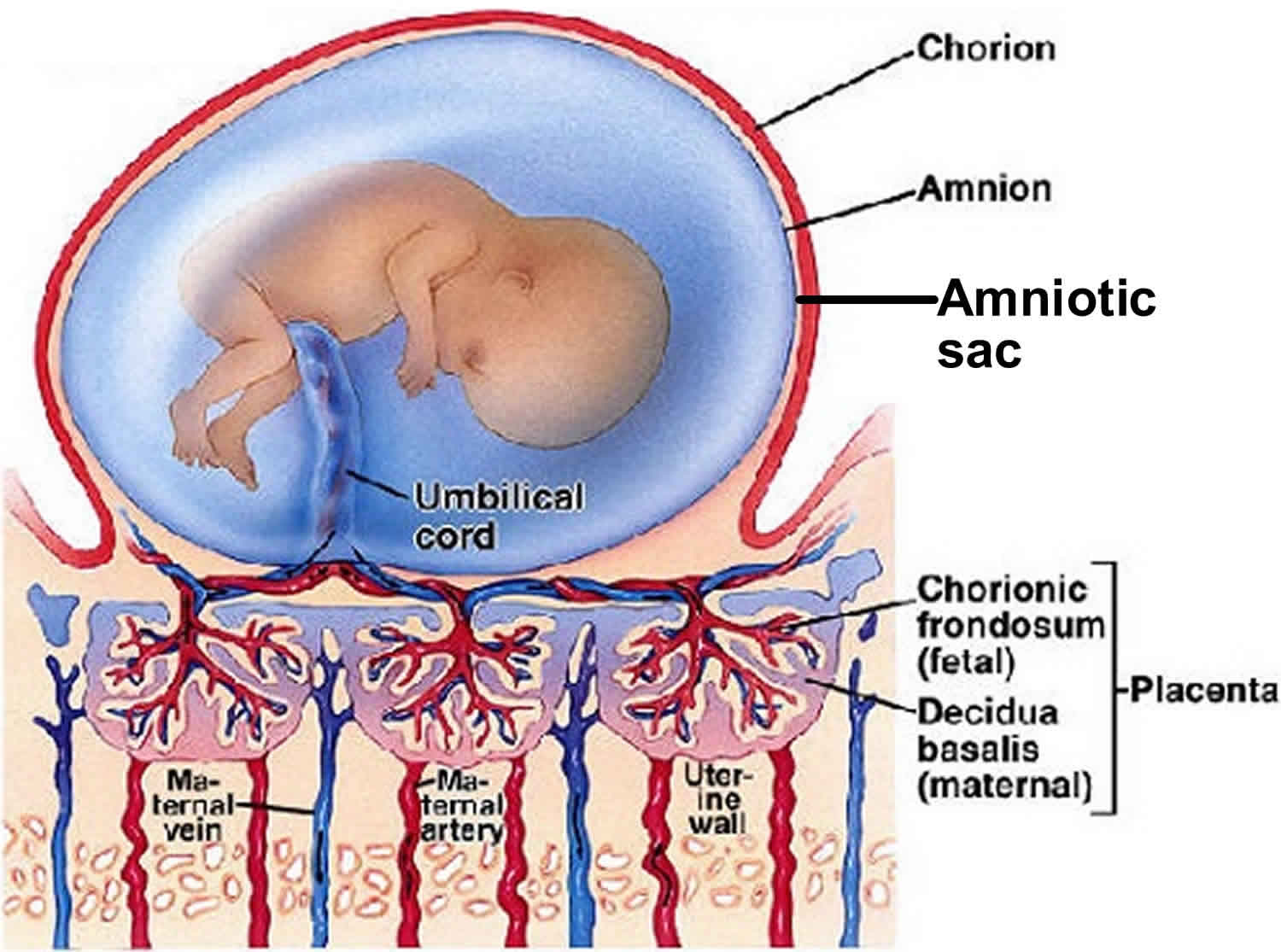
Figure 1. Amniotic sac
Amniotic sac function
The amniotic sac is the bag of membranes containing the fetus and the amniotic fluid. Amniotic sac filled with fluid acts as a cushion to protect the developing fetus.
Here’s what the amniotic sac and amniotic fluid does:
- Cushions and protects your baby
- Keeps a steady temperature around your baby
- Helps your baby’s lungs grow and develop because your baby breathes in the fluid
- Helps your baby’s digestive system develop because your baby swallows the fluid
- Helps your baby’s muscles and bones develop because your baby can move around in the fluid
- Keeps the umbilical cord (the cord that carries food and oxygen from the placenta to your baby) from being squeezed
In the early weeks of pregnancy, the amniotic fluid is mostly water that comes from your body. After about 20 weeks of pregnancy, your baby’s urine makes up most of the fluid. Amniotic fluid also contains nutrients, hormones (chemicals made by the body) and antibodies (cells in the body that fight off infection).
The amount of amniotic fluid increases until about 36 weeks of pregnancy. At that time, it makes up about 1 quart. After that, the amount of amniotic fluid usually begins to decrease.
Sometimes you can have too little or too much amniotic fluid. Too little fluid is called oligohydramnios. Too much fluid is called polyhydramnios. Either one can cause problems for a pregnant woman and her baby. Even with these conditions, though, most babies are born healthy.
Amniotic sac vs Placenta
The placenta is a circular vascular structure that attaches to the uterine wall and allows metabolic exchange between the fetus and the mother. All nutrients flows from the mother to the embryo. The developing fetus relies on the placenta for nutrition and many developmentally essential functions. The placenta has both embryonic and maternal components. The embryonic portion comes from the outermost embryonic membrane. The maternal portion develops from the decidua basalis of the uterus. The placental membrane separates the embryonic blood from maternal blood but is thin enough to allow diffusion and transport of nutrients and waste. A normal placenta is round or oval shaped and about 22 cm in diameter. It is 2 cm to 2.5 cm thick and weighs about a pound.
Amniotic sac rupture
Premature rupture of membranes is a rupture (breaking open) of the amniotic sac before labor begins. If premature rupture of membranes occurs before 37 weeks of pregnancy, it is called preterm premature rupture of membranes (PPROM).
Premature rupture of membranes occurs in about 8 to 10 percent of all pregnancies. Preterm premature rupture of membranes (PPROM) (before 37 weeks) accounts for one fourth to one third of all preterm births.
What causes premature rupture of amniotic sac?
Rupture of the amniotic sac near the end of pregnancy (term) may be caused by a natural weakening of the membranes or from the force of contractions. Before term, preterm premature rupture of membranes (PPROM) is often due to an infection in the uterus. Other factors that may be linked to premature rupture of the amniotic sac include the following:
- Low socioeconomic conditions (as women in lower socioeconomic conditions are less likely to receive proper prenatal care)
- Sexually transmitted infections (STIs), such as chlamydia and gonorrhea
- Previous preterm birth
- Vaginal bleeding
- Cigarette smoking during pregnancy
- Unknown causes
Prevention of premature rupture of the amniotic sac
Unfortunately, there is no way to actively prevent premature rupture of the amniotic sac. However, this condition does have a strong link with cigarette smoking and mothers should stop smoking as soon as possible.
Why is premature rupture of the amniotic sac a concern?
Premature rupture of the amniotic sac is a complicating factor in as many as one third of premature births. A significant risk of preterm premature rupture of membranes (PPROM) (before 37 weeks) is that the baby is very likely to be born within a few days of the membrane rupture. Another major risk of premature rupture of the amniotic sac is development of a serious infection of the placental tissues called chorioamnionitis, which can be very dangerous for mother and baby. Other complications that may occur with premature rupture of the amniotic sac include placental abruption (early detachment of the placenta from the uterus), compression of the umbilical cord, cesarean birth, and postpartum (after delivery) infection.
What are the symptoms of premature rupture of the amniotic sac?
The following are the most common symptoms of premature rupture of the amniotic sac. However, each woman may experience symptoms differently. Symptoms may include:
- Leaking or a gush of watery fluid from the vagina
- Constant wetness in underwear
If you notice any symptoms of premature rupture of the amniotic sac, be sure to call your doctor as soon as possible. The symptoms of premature rupture of the amniotic sac may resemble other medical conditions. Consult your doctor for a diagnosis.
How is premature rupture of the amniotic sac diagnosed?
In addition to a complete medical history and physical examination, Premature rupture of the amniotic sac may be diagnosed in several ways, including the following:
- An examination of the cervix (may show fluid leaking from the cervical opening)
- Testing of the pH (acid or alkaline) of the fluid
- Looking at the dried fluid under a microscope (may show a characteristic fern-like pattern)
- Ultrasound. A diagnostic imaging technique that uses high-frequency sound waves and a computer to create images of blood vessels, tissues, and organs. Ultrasounds are used to view internal organs as they function, and to assess how much fluid is around the baby.
Treatment for premature rupture of the amniotic sac
Specific treatment for premature rupture of the amniotic sac will be determined by your doctor based on:
- Your pregnancy, overall health, and medical history
- Extent of the condition
- Your tolerance for specific medications, procedures, or therapies
- Expectations for the course of the condition
- Your opinion or preference
Treatment for premature rupture of the amniotic sac may include:
- Hospitalization
- Expectant management (in very few cases of preterm premature rupture of membranes (PPROM), the membranes may seal over and the fluid may stop leaking without treatment, although this is uncommon unless premature rupture of the amniotic sac was from a procedure, such as amniocentesis, early in gestation)
- Monitoring for signs of infection, such as fever, pain, increased fetal heart rate, and/or laboratory tests.
- Giving the mother medications called corticosteroids that may help mature the lungs of the fetus (lung immaturity is a major problem of premature babies). However, corticosteroids may mask an infection in the uterus.
- Antibiotics (to prevent or treat infections)
- Tocolytics. Medications used to stop preterm labor.
- Women with preterm premature rupture of membranes (PPROM) usually deliver at 34 weeks if stable. If there are signs of abruption, chorioamnionitis, or fetal compromise, then early delivery would be necessary.





{kind=link}