What is androgen
Androgens also known as male sex hormones are an important class of C19 steroid hormones that control normal male development and reproductive function. This includes the embryological development of the primary male sex organs, and the development of male secondary sex characteristics at puberty and fertility. Androgens are synthesized in the testes, the ovaries, and the adrenal glands. The main circulating androgen is testosterone, which is produced by special endocrine tissue (the Leydig cells) in the male testicles and can also act as a pro-hormone after being metabolized to dihydrotestosterone (DHT) or estradiol (E2) 1. Although testosterone is considered to be a “male” sex hormone, testosterone is present in the blood of both men and women. Testosterone is also produced by the adrenal glands in both males and females and, in small amounts, by the ovaries in females. Both men and women also produce weak acting androgens in the zona reticularis of the adrenal glands. These weak-acting androgens are known as dehydroepiandrosterone (DHEA) and androstenedione. They bind to testosterone receptors with weaker affinity but can also be converted to testosterone in the peripheral tissues if produced at high amounts 2.
In males, testosterone stimulates development of secondary sex characteristics, including enlargement of the penis, growth of body hair, muscle development, and a deepening voice. It is present in large amounts in males during puberty and in adult males to regulate the sex drive and maintain muscle mass. In women, testosterone is converted to estradiol (estrogen), the main sex hormone in females.
Testosterone production is stimulated and controlled by luteinizing hormone (LH), which is manufactured by the pituitary gland. Testosterone works within a negative feedback mechanism: as the testosterone level increases, luteinizing hormone (LH) production decreases, which slows testosterone production; decreased testosterone causes increased production of LH, which in turn stimulates testosterone production.
Testosterone levels are diurnal, peaking in the early morning hours (about 4:00 to 8:00 am), with the lowest levels in the evening (about 4:00 to 8:00 pm). Levels also increase after exercise and also decrease with age.
About two-thirds of testosterone circulates in the blood bound to sex-hormone binding globulin (SHBG) and slightly less than one-third bound to albumin. A small percent (less than 4%) circulates as free testosterone. The free plus the albumin-bound testosterone is the bioavailable fraction, which can act on target tissues.
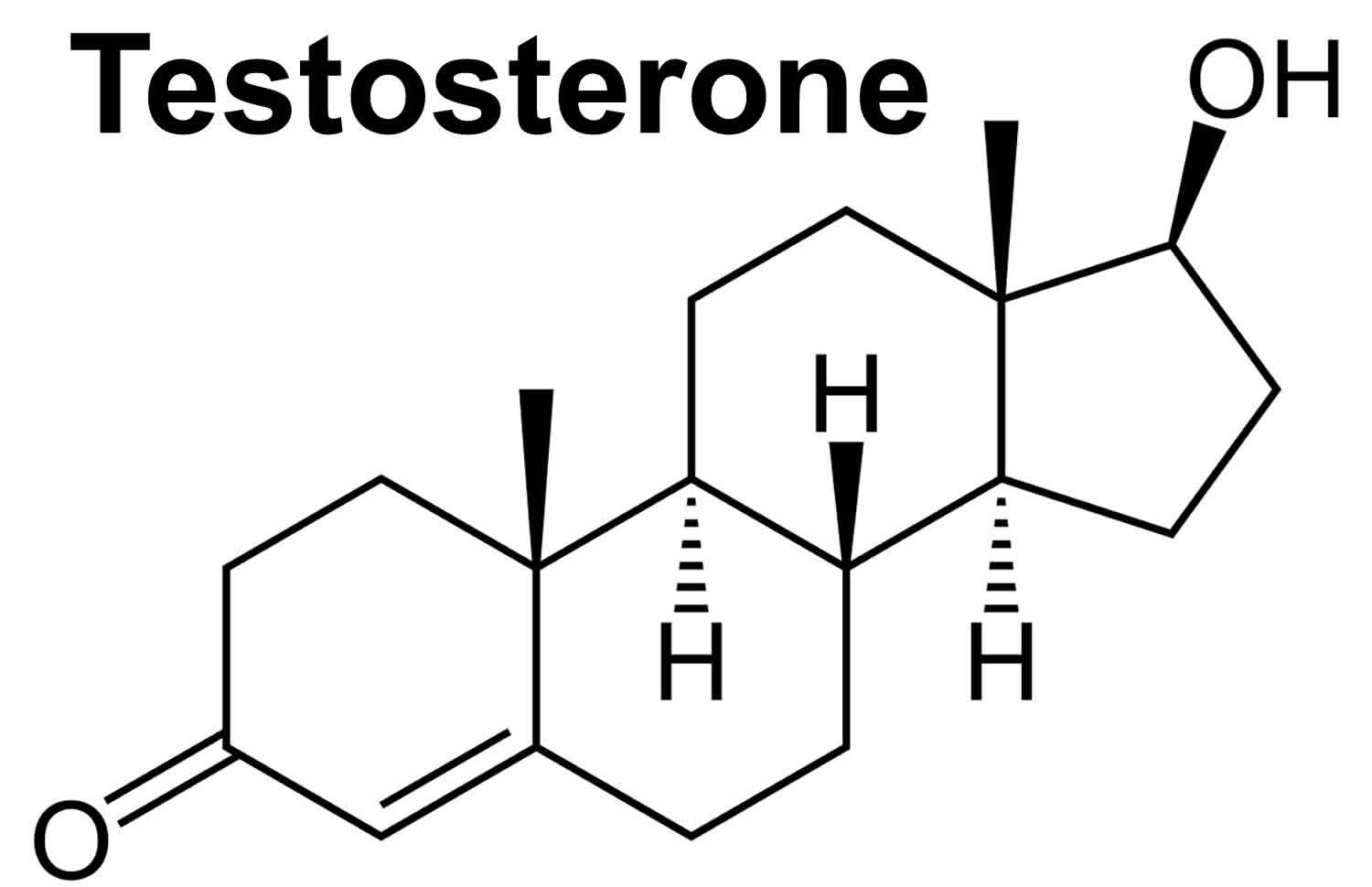
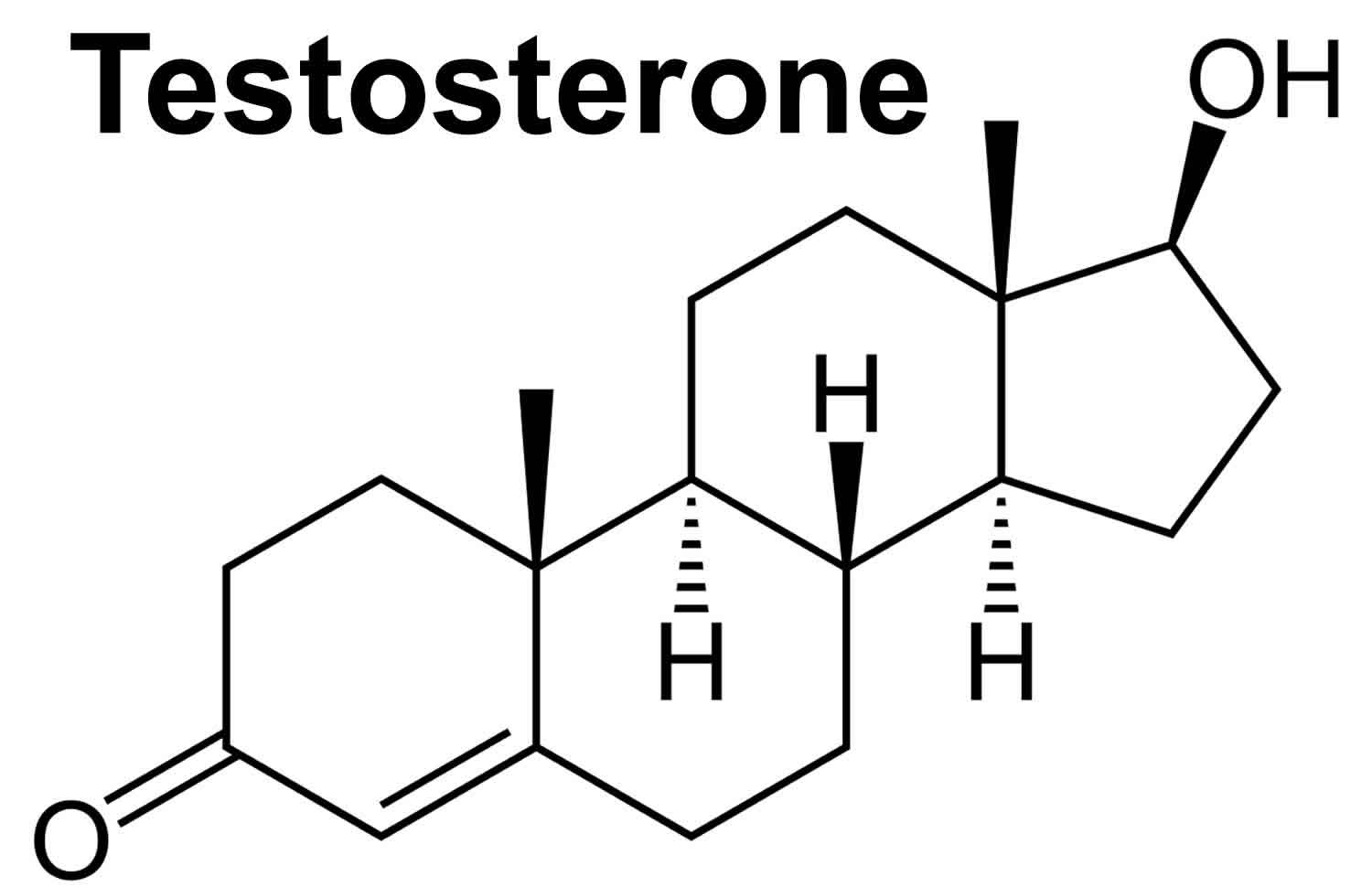
Testosterone together with its potent metabolite, dihydrotestosterone (DHT), are the principal androgens in the circulation of mature male mammals 3. Testosterone has a characteristic four ring C18 steroid structure and is synthesized mainly by Leydig cells, located in the interstitium of the testis between the seminiferous tubules. Leydig cell secretion creates a very high local concentration of testosterone in the testis as well as a steep downhill concentration gradient into the bloodstream maintaining circulating testosterone levels which exert characteristic androgenic effects on distant androgen sensitive target tissues. The biological actions of testosterone and dihydrotestosterone (DHT) are mediated by the androgen receptor, a member of the nuclear receptor superfamily encoded by a single gene located on the X chromosome, which then leads to a characteristic patterns of gene expression by regulating the transcription of an array of androgen responsive target genes. This physiological definition of an androgen in the whole animal is now complemented by a biochemical and pharmacological definition of an androgen as a chemical that effectively competes with testosterone binding to the androgen receptor 4 to stimulate post-receptor functions in isolated cells or cell-free systems. In addition, non-genomic mechanisms of androgen action involving rapid, membrane-mediated nontranscriptional processes in the cytoplasm have been described but not yet fully characterized 5.
Testosterone makes a man look and feel like a man. In a man, testosterone helps:
- Keep bones and muscles strong
- Determine hair growth and where fat is on the body
- Make sperm
- Maintain sex drive and erections
- Make red blood cells
- Boost energy and mood
Testosterone can be used to treat and manage various medical conditions. Medical conditions in which testosterone can be used include metastatic breast cancer, delayed puberty, hypogonadotropic hypogonadism (congenital or acquired), and primary hypogonadism. Toxic effects of testosterone and synthetic androgens include over-masculinization, hirsutism, decreased menses, acne, and clitoral enlargement. Rarely, synthetic androgens can cause hepatic adenoma, cholestatic jaundice, and prostatic hypertrophy. Synthetic androgens and testosterone are contraindicated in pregnancy.
Androgen antagonists come in different types. Gonadotropin-releasing hormone (GnRH) analogs, if given continuously, can act as medical castration drugs and are used in treating prostate cancer. Androgen receptor inhibitors, like flutamide and spironolactone, can be used for patients with hirsutism. Steroid synthesis inhibitors, like ketoconazole, can be used in Cushing disease. 5-alpha reductase inhibitors, like finasteride, can be used to treat benign prostatic hyperplasia 6.
Figure 1. Testosterone
Androgen deficiency
Decreased production of testosterone can occur with aging, certain medications, chemotherapy, hypothalamus-pituitary axis disorders, primary hypogonadism, cryptorchidism and orchitis, and with genetic disorders such as Klinefelter and Kallmann syndrome. Klinefelter syndrome is the most common congenital abnormality that results in primary hypogonadism. In Klinefelter, there is dysgenesis of seminiferous tubules and loss of Sertoli cells which leads to a decrease in inhibin levels and a resultant increase in follicle stimulating hormone (FSH). FSH upregulates aromatase leading to increased conversion of androgens to estrogens. In Klinefelter, there is also Leydig cell dysfunction which leads to decreased testosterone levels and an increase in luteinizing hormone (LH) due to loss of negative feedback. In Kallmann syndrome, failed migration of gonadotropin-releasing hormone (GnRH)-producing neurons leads to lack of gonadotropin-releasing hormone (GnRH). No gonadotropin-releasing hormone (GnRH) results in a decrease in follicle stimulating hormone (FSH), luteinizing hormone (LH), testosterone, and sperm count. Specific to Kallmann syndrome, in comparison to other causes of hypogonadotropic hypogonadism, is defects in the sensation of smell (hyposmia or anosmia) 7.
5-alpha reductase is an enzyme that converts testosterone to dihydrotestosterone (DHT). Male patients with 5-alpha reductase deficiency present with normal female or male genitalia or ambiguous genitalia at birth due to lack of dihydrotestosterone (DHT) 8. These patients have a male internal urogenital tract (anti-Mullerian hormone is still present). At puberty, adolescents with this enzyme deficiency, who may have been raised as girls due to lack of secondary male characteristics, begin to develop male secondary sex characteristics and have primary amenorrhea. These patients will have normal testosterone and LH, low dihydrotestosterone (DHT), and an increased testosterone-to-DHT ratio. In contrast to 5-alpha reductase deficiency, androgen insensitivity syndrome (discussed in detail below) is a condition in which patients lack functional androgen receptors (AR gene defect) resulting in under-virilization. These patients, like those with 5-alpha reductase deficiency, have a 46 XY karyotype. In contrast, however, these patients have normal female external genitalia and usually undescended testes. In adolescence, they experience primary amenorrhea and breast development but have no pubic or axillary hair and lack the deepening voice changes that occur with puberty. They will have a blind vaginal pouch and abnormal internal reproductive organs (fallopian tubes, uterus, and the upper portion of the vagina) due to the production of the Mullerian inhibiting factor. These patients will have high levels of testosterone and LH 9.
Androgen function
Testosterone
Testosterone is the main androgen in men. Testosterone is responsible for regulating sex differentiation, producing male sex characteristics, spermatogenesis and fertility. Testosterone’s effects are first seen in the fetus. During the first 6 weeks of development, the reproductive tissues of males and females are identical. At around week 7 in utero, the SRY (sex-related gene on the Y chromosome) initiates the development of the testicles 10. Sertoli cells from the testis cords (fetal testicles) eventually develop into seminiferous tubules. Sertoli cells produce a Mullerian-inhibiting substance, which leads to the regression of the fallopian tubes, uterus, and upper segment of the vagina (Mullerian structures normally present in females). Fetal Leydig cells and endothelial cells migrate into the gonad and produce testosterone, which supports the differentiation of the Wolffian duct (paramesonephric duct) structures that go on to become the male urogenital tract. Testosterone also gets converted to dihydrotestosterone (DHT) in the periphery (discussed below) and induces the formation of the prostate and male external genitalia. Testosterone is also responsible for testicular descent through the inguinal canal, which occurs in the last 2 months of fetal development. When an embryo lacks a Y chromosome and thus the SRY gene, ovaries develop. Fetal ovaries do not produce adequate amounts of testosterone, thus the Wolffian ducts do not develop. There is also an absence of Mullerian-inhibiting substance in these individuals, leading to the development of the Mullerian ducts and female reproductive structures 11.
Testosterone is responsible for the development of primary sexual development, which includes testicular descent, spermatogenesis, enlargement of the penis and testes, and increasing libido. The testes usually begin the descent into the scrotum around 7 months of gestation, when the testes begin secreting reasonable quantities of testosterone. If a male child is born with undescended but normal testes that do not descend by 4 to 6 months of age, administration of testosterone can help the testes descend through the inguinal canals 12.
Testosterone is also involved in regulating secondary male characteristics, which are those responsible for masculinity. These secondary sex characteristics include male hair patterns, vocal changes, and voice deepening, anabolic effects which include growth spurts in puberty (testosterone increases tissue growth at the epiphyseal plate early on and eventual closure of plate later in puberty) and skeletal muscle growth (testosterone stimulates protein synthesis). Testosterone also stimulates erythropoiesis, which results in a higher hematocrit in males versus females. Testosterone levels tend to drop with increasing age; because of this, men tend to experience a decrease in testicular size, a drop in libido, lower bone density, muscle mass decline, increased fat production, and decreased erythropoiesis which leads to possible anemia.
In women, androgens have potential roles in relaxation of the myometrium via non-genomic, androgen receptor-independent pathways, preventing premature uterine contractions in pregnancy 13.
Dehydroepiandrosterone (DHEA)
- Plays a role in developing male secondary sexual characteristics at puberty
- Can be converted by the body into more potent androgens, such as testosterone and androstenedione
- Can be converted into the female hormone estrogen
Dehydroepiandrosterone (DHEA) is a relatively weak androgen produced by the adrenals and ovaries/testes. Dehydroepiandrosterone (DHEA) serves as a precursor for other hormones including testosterone and estrogen. The sulfated form of DHEA, dehydroepiandrosterone sulfate (DHEAS), is specific for the adrenal glands. Dehydroepiandrosterone sulfate (DHEAS) is produced almost exclusively by the adrenal glands, with smaller amounts being produced by a woman’s ovaries and a man’s testicles. Dehydroepiandrosterone sulfate (DHEAS) is useful as a marker for adrenal gland function. Adrenal tumors (cancerous and non-cancerous) and adrenal hyperplasia can lead to the overproduction of dehydroepiandrosterone sulfate (DHEAS). Rarely, an ovarian tumor may produce dehydroepiandrosterone sulfate (DHEAS).
In polycystic ovary syndrome (PCOS), abnormal gonadotropin-releasing hormone (GnRH) secretion leads to an increase in LH secretion. LH stimulates androgen production by ovarian theca cells which leads to hirsutism, male escutcheon, acne and androgenic alopecia in women affected with PCOS 14. In adrenal and ovarian tumors, there is usually rapidly progressing androgenic symptoms (hirsutism, virilization). If testosterone is elevated and dehydroepiandrosterone sulfate (DHEAS) is normal, this is most likely from an ovarian tumor. If dehydroepiandrosterone sulfate (DHEAS) is elevated and testosterone is relatively normal, this is most likely an adrenal tumor.
Excess dehydroepiandrosterone sulfate (DHEAS):
- May not be noticed in adult men
- Can cause early (precocious) puberty in young boys
- Can lead to absence of menstrual periods (amenorrhea) and the development of masculine physical characteristics (virilization) in girls and women, such as excess body and facial hair (hirsutism)
- Can cause a female baby to be born with genitals that are not distinctly male or female in appearance (ambiguous external genitalia)
The test for dehydroepiandrosterone sulfate (DHEAS) is ordered along with tests for testosterone and several other male hormones (androgens) to:
- Evaluate adrenal gland function
- Distinguish DHEAS-secreting conditions that are caused by the adrenal glands from those that originate in the testicles or rarely in the ovaries (ovarian tumors)
- Help diagnose tumors in the outer layer (cortex) of the adrenal gland (adrenocortical tumors) and adrenal cancers
- Help diagnose congenital adrenal hyperplasia and adult-onset adrenal hyperplasia
In women, concentrations of DHEAS are often measured, along with other hormones such as follicle stimulating hormone (FSH), luteinizing hormone (LH), prolactin, estrogen, and testosterone, to help diagnose polycystic ovary syndrome (PCOS) and to help rule out other causes of infertility, lack of menstrual period (amenorrhea), and presence of excess facial and body hair (hirsutism).
DHEAS levels may be ordered with other hormones to investigate and diagnose the cause of the development of masculine physical characteristics (virilization) in young girls and early (precocious) puberty in young boys.
Dehydroepiandrosterone sulfate (DHEAS) may be measured when a woman presents with signs and symptoms such as amenorrhea, infertility, and/or those related to virilization. These changes vary in severity and may include:
- A deeper voice
- Excess facial or body hair (hirsutism)
- Male pattern baldness
- Muscularity
- Acne
- Enlargement of the Adam’s apple
- Decreased breast size
Dehydroepiandrosterone sulfate (DHEAS) test may also be ordered when a young girl shows signs of virilization or when a female infant has external genitalia that are not distinctly male or female in appearance (ambiguous genitalia).
DHEAS may also be measured when young boys show signs of precocious puberty, the development of a deeper voice, pubic hair, muscularity, and an enlarged penis well before the age of normal puberty.
Androstenedione
Androstenedione is an androgen, one of several “male” sex hormones that are responsible for the onset of sexual differentiation in males and females and the development of secondary male physical characteristics such as a deep voice and facial hair. Though it is considered to be a “male” sex hormone, it is present in the blood of both men and women and is a precursor that can be converted by the body into more potent androgens, such as testosterone, or converted into the female hormone estrogen. This test measures the amount of androstenedione in the blood.
Androstenedione is produced by the ovaries in women, the testicles in men, and by the adrenal glands in both:
- The pituitary hormone luteinizing hormone (LH) stimulates the release of androstenedione by the ovaries and testicles.
- The pituitary hormone adrenocorticotropic hormone (ACTH) stimulates the release of androstenedione by the adrenal glands.
The level of androstenedione in the blood will vary during the day in a “diurnal pattern,” and it will vary during a woman’s menstrual cycle. Because of its origins, androstenedione can be useful as a marker of adrenal gland function, of androgen production, and of the function of the ovaries or testicles. An androstenedione test is often performed after results of other tests, such as testosterone or 17-hydroxyprogesterone, are found to be abnormal.
An excess level of androstenedione and other androgens can cause children to have sex organs that are not clearly male or female (ambiguous external genitalia), excess body hair (hirsutism), and abnormal menstrual periods in girls and precocious (early) puberty in girls and boys.
Adrenal tumors, ACTH-producing tumors, and adrenal hyperplasia can lead to the overproduction of androstenedione. Women with polycystic ovary syndrome (PCOS) may have higher levels of androstenedione as well. While elevated levels may not be noticed in adult men, they can lead to noticeable male physical characteristics (virilization) and a lack of monthly menstrual periods (amenorrhea) in females.
Androstenedione testing is used to evaluate the function of the adrenal gland and the ovaries or the testicles as well as the production of hormones related to the development of male sex organs and physical characteristics (androgens). It is most commonly used to determine the cause of symptoms of excess androgens in a woman who has an elevated testosterone level, along with a few other laboratory tests for this purpose.
An androstenedione level may be used to:
- Evaluate adrenal gland function and to distinguish between androgen-secreting conditions that are caused by the adrenal glands from those that originate in the ovaries or testicles, if results of DHEAS and testosterone testing are abnormal
- Help diagnose tumors in the outer layer (cortex) of the adrenal gland or tumors outside of the adrenal gland that secrete ACTH (ectopic) and separate these conditions from ovarian or testicular tumors and cancers
- Diagnose congenital adrenal hyperplasia (CAH) and monitor CAH treatment, in addition to tests for testosterone and 17-hydroxyprogesterone
- Help diagnose polycystic ovarian syndrome (PCOS) and help rule out other causes of infertility, no monthly menstrual periods (amenorrhea), and excess body and facial hair (hirsutism) in women who have abnormal results on tests for DHEAS, testosterone, and other hormones such as follicle stimulating hormone (FSH), luteinizing hormone (LH), prolactin, and estrogen
- Investigate and diagnose the cause of male physical characteristics (virilization) in young girls and early (precocious) puberty in young boys
- Help determine the cause of delayed puberty and investigate suspected ovarian or testicular failure
Figure 2. The pituitary gland location

Figure 3. The hypothalamus and pituitary gland (anterior and posterior) endocrine pathways and target organs

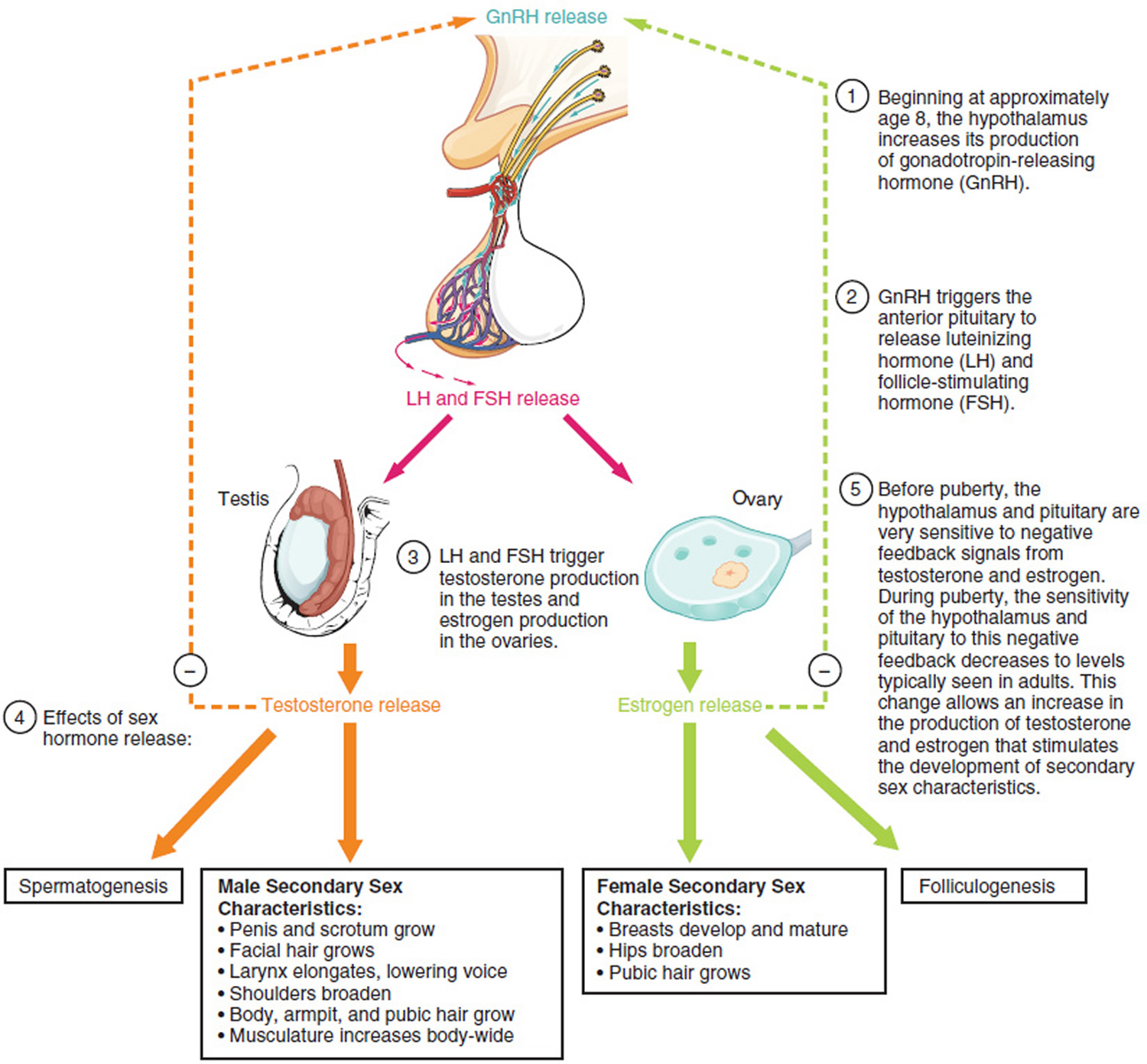
Figure 4. Hypothalamus and anterior pituitary stimulating sperm production
Testosterone physiology
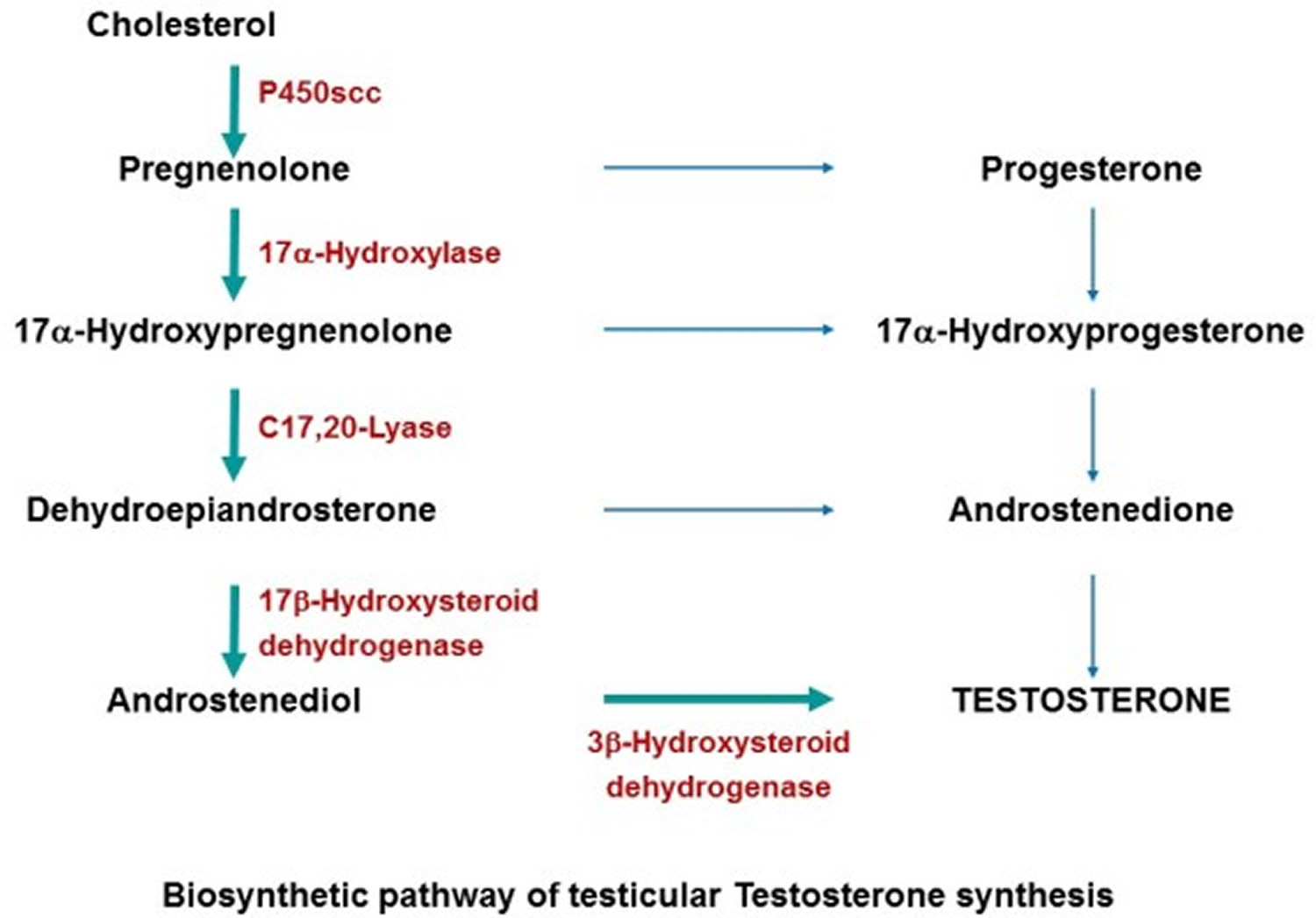
Testosterone is synthesized by an enzymatic sequence of steps from cholesterol 15 within the 500 million Leydig cells located in the interstitial compartment of the testis between the seminiferous tubules, which constitutes approximately 5% of mature testis volume.
In puberty, the hypothalamic-pituitary-gonadal axis takes a major role in regulating testosterone levels and gonadal function (see Figures 3 and 4). The hypothalamus secretes gonadotropin-releasing hormone (GnRH), which travels down the hypothalamo-hypophyseal portal system to the anterior pituitary, which secretes luteinizing hormone (LH) and follicle stimulating hormone (FSH) (see Figure 3). LH (luteinizing hormone) and FSH (follicle stimulating hormone) are two gonadotropic hormones which travel through the blood and act on receptors in the gonads. LH (luteinizing hormone) in particular acts on the Leydig cells to increase testosterone production. Testosterone limits its own secretion via negative feedback. High levels of testosterone in the blood feedback to the hypothalamus to suppress the secretion of gonadotropin-releasing hormone (GnRH) and also feedback to the anterior pituitary, making it less responsive to GnRH stimuli 16.
Throughout the reproductive life of males, the hypothalamus releases GnRH in pulses every 1 to 3 hours. Despite this pulsatile release, however, average plasma levels of FSH and LH remain fairly constant from the start of puberty, where levels spike, to the third decade of life, where levels peak and slowly begin to decline. Prior to puberty, testosterone levels are low, reflecting the low secretion of GnRH and gonadotropins (LH & FSH). Changes in neuronal input to the hypothalamus and brain activity during puberty, cause a dramatic rise in GnRH secretion.
Leydig cells in the testes function to turn cholesterol into testosterone. Luteinizing hormone (LH) regulates the initial step in this process. Two important intermediates in this process are dehydroepiandrosterone (DHEA) and androstenedione. Androstenedione is converted to testosterone by the enzyme 17-beta-hydroxysteroid dehydrogenase. The majority of testosterone is bound to plasma proteins such as sex-hormone-binding-globulin (SHBG) and albumin. This majority supply of protein-bound testosterone acts as a surplus of testosterone hormone for the body. The small amounts of free testosterone in the blood act at the level of the tissues, primarily the seminal vesicles, bone, muscle, and prostate gland. At the cellular level, testosterone gets converted to dihydrotestosterone (DHT) by the enzyme 5-alpha-reductase. Testosterone and dihydrotestosterone (DHT) can bind to cell receptors and regulate protein expression.
In many cases, measurement of total testosterone provides a healthcare practitioner with adequate information. However, in certain cases, for example when the level of sex-hormone-binding-globulin (SHBG) is abnormal, a test for free or bioavailable testosterone may be performed as it may more accurately reflect the presence of a medical condition.
What are free testosterone and bioavailable testosterone?
Testosterone is present in the blood as “free” testosterone (less than 4%) or bound testosterone (~98%). The latter may be loosely bound to albumin (about one-third), the main protein in the fluid portion of the blood, or bound to a specific binding protein called sex hormone binding globulin or SHBG (about two-thirds). The percentages in the three fractions varies greatly. The binding between testosterone and albumin is not very strong and is easily reversed, so the term bioavailable testosterone refers to the sum of free testosterone plus albumin-bound testosterone.
It is suggested that bioavailable testosterone represents the fraction of circulating testosterone that readily enters cells and better reflects the bioactivity of testosterone than does the simple measurement of serum total testosterone. Also, varying levels of SHBG can result in inaccurate measurements of bioavailable testosterone. Decreased SHBG levels can be seen in obesity, hypothyroidism, androgen use, and nephritic syndrome (a form of kidney disease). Increased levels are seen in cirrhosis, hyperthyroidism, and estrogen use. In these situations, measurement of free testosterone may be more useful.
Androgen excess
Over-production of androgens can occur in the following conditions: polycystic ovarian syndrome (PCOS), adrenal virilization/adrenal tumors, ovarian or testicular tumors, Cushing syndrome, and as a result of exogenous steroid use.
Impaired testosterone metabolism can occur in certain cases of congenital adrenal hyperplasia (CAH). In classic congenital adrenal hyperplasia (CAH) (95% of cases), due to 21 hydroxylase deficiency, newborns usually present with ambiguous genitalia and later develop salt wasting, vomiting, hypotension, and acidosis. A marked increase in 17-hydroxyprogesterone is diverted towards adrenal androgen synthesis and leads to hyperandrogenism. Hyperandrogenism impairs hypothalamic sensitivity to progesterone leading to a rapid rise in gonadotropin-releasing hormone (GnRH) synthesis and thus increased LH and FSH. Elevations in LH and FSH lead to increased gonadal steroid production (17-hydroxyprogesterone, dehydroepiandrosterone [DHEA], testosterone, LH, and FSH). Diagnosis is with adrenocorticotropic hormone stimulation test showing exaggerated 17 hydroxyprogesterone response 17.
Anti-androgens
Antiandrogens are drugs that compete with androgens for binding to the androgen receptor. By competing for binding to the androgen receptor, antiandrogens reduce the ability of androgens to promote prostate cancer cell growth. Because antiandrogens do not block androgen production, they are rarely used on their own to treat prostate cancer. Instead, they are used in combination with orchiectomy or an luteinizing hormone-releasing hormone (LHRH) agonist. Use of an antiandrogen drug in combination with orchiectomy or an luteinizing hormone-releasing hormone (LHRH) agonist is called combined androgen blockade, complete androgen blockade, or total androgen blockade. Antiandrogens that are approved in the United States to treat prostate cancer include flutamide, enzalutamide, bicalutamide, and nilutamide. Antiandrogens are given as pills to be swallowed.
Hirsutism is a condition where women have excess hair on their face or body. The main symptom of hirsutism is unwanted hair growth on a woman’s face, chest, and back. This thick, dark hair is different from the normal, fine “baby” hair on other parts of the body. Doctor may prescribe anti-androgens to treat most cases of hirsutism, common anti-androgens are spironolactone and finasteride. These block your body from producing male hormones. They also can decrease the amount of new hair growth. However, they cannot get rid of the hair you already have. Anti-androgens take at least 3 to 6 months to work. They can cause birth defects. Do not take them if you are pregnant or trying to get pregnant.
Testosterone test
Testosterone testing is used to diagnose several conditions in men, women, girls, and boys.
The testosterone test may be used to help evaluate conditions such as:
- Delayed or precocious (early) puberty in boys
- Decreased sex drive in men and women
- Erectile dysfunction in men
- Infertility in men and women
- Testicular tumors in men
- Hypothalamus or pituitary disorders
- Hirsutism and virilization in girls and women
Typically, a test for total testosterone is used for diagnosis. The total testosterone test measures testosterone that is bound to proteins in the blood (e.g., albumin and sex-hormone binding globulin [SHBG]) as well as testosterone that is not bound (free testosterone).
About two-thirds of testosterone circulates in the blood bound to SHBG and slightly less than one-third bound to albumin. A small percent (less than 4%) circulates as free testosterone. Free testosterone plus the testosterone bound to albumin is the bioavailable testosterone, which can act on target tissues.
In many cases, the total testosterone test provides adequate information. However, in certain cases, for example when the level of sex-hormone binding globulin [SHBG] is abnormal, a test for free or bioavailable testosterone may be performed as it may more accurately reflect the presence of a medical condition.
Depending on the reason for testing, other tests and hormone levels may be done in conjunction with testosterone testing. Some examples include:
- Sex-hormone binding globulin (SHBG)
- Luteinizing hormone (LH) and follicle stimulating hormone (FSH)
- Estrogens
- DHEAS
- Prolactin
- 17-Hydroxyprogesterone
- Androstenedione
When is testosterone test ordered?
In men, the test may be ordered when infertility is suspected or when a man has a decreased sex drive or erectile dysfunction. Some other symptoms include lack of beard and body hair, decreased muscle mass, and development of breast tissue (gynecomastia). Low levels of total and bioavailable testosterone have also been associated with, or caused by, a greater presence of visceral fat (midriff or organ fat), insulin resistance, and increased risk of coronary artery disease.
In boys with delayed or slowly progressing puberty, the test is often ordered with the luteinizing hormone (LH) and follicle stimulating hormone (FSH) tests. Although there are differences from individual to individual as to when puberty begins, it is generally by the age of 10 years. Some symptoms of delayed puberty may include:
- Delayed development of muscle mass
- Lack of deepening of the voice or growth of body hair
- Slow or delayed growth of testicles and penis
The test also can be ordered when a young boy seems to be undergoing a very early (precocious) puberty with obvious secondary sex characteristics. Causes of precocious puberty in boys, due to increased testosterone, include various tumors and congenital adrenal hyperplasia.
In females, testosterone testing may be done when a woman has irregular or no menstrual periods (amenorrhea), is having difficulty getting pregnant, or appears to have masculine features, such as excessive facial and body hair, male pattern baldness, and/or a low voice. Testosterone levels can rise because of tumors that develop in either the ovary or adrenal gland or because of other conditions, such as polycystic ovarian syndrome (PCOS).
What does abnormal testosterone test result mean?
Alcoholism and liver disease in males can decrease testosterone levels. Drugs, including androgens other than testosterone and steroids, can also decrease testosterone levels.
Prostate cancer responds to androgens, so many men with advanced prostate cancer receive drugs that lower testosterone levels.
Drugs such as anticonvulsants, barbiturates, and clomiphene can cause testosterone levels to rise. Women taking estrogen therapy may have increased total testosterone levels.
Males
The normal range for testosterone levels in men is broad and varies by stage of maturity and age. It is normal for testosterone levels to slowly decline, usually after age 30. Testosterone may decrease more in men who are obese or chronically ill and with the use of certain medications.
A low testosterone level (hypogonadism) may be due to:
- Hypothalamic or pituitary disease
- Genetic diseases that can cause decreased testosterone production in young men (Klinefelter, Kallman, and Prader-Willi syndromes) or testicular failure and infertility (as in myotonic dystrophy, a form of muscular dystrophy)
- Impaired testosterone production because of acquired damage to the testes, such as from alcoholism, physical injury, or viral diseases like mumps
- Chronic disease, such as diabetes
Men who are diagnosed with consistently low testosterone levels and have related signs and symptoms may be prescribed testosterone replacement therapy by their healthcare providers. However, testosterone supplements are not approved by the Food and Drug Administration to boost strength, athletic performance, or prevent problems from aging. Use for these purposes may be harmful.
Increased testosterone levels in males can indicate:
- Testicular tumors
- Adrenal tumors that are producing testosterone
- Use of androgens (also called anabolic steroids)
- Early puberty of unknown cause in boys
- Congenital adrenal hyperplasia in babies and children
Females
In women, testosterone levels are normally low. Increased testosterone levels can indicate:
- PCOS
- Ovarian or adrenal gland tumor
- Congenital adrenal hyperplasia
Androgen deficiency in adult men
Low testosterone also called hypogonadism, generally refers to a condition in which a man does not produce enough testosterone.
Testosterone is the most important sex hormone that men have. It is responsible for the typical male characteristics, such as facial, pubic, and body hair as well as muscle. This hormone also helps maintain sex drive, sperm production, and bone health.
The brain and pituitary gland (a small gland at the base of the brain) control testosterone production by the testicles. Low testosterone can originate from testicular disease or failure (primary hypogonadism) or from disease or failure of the pituitary gland or hypothalamus (secondary hypogonadism).
In the short term, low testosterone can cause:
- A drop in sex drive
- Poor erections
- Low sperm count
- Enlarged breasts
Over time, low testosterone may cause a man to lose body hair, muscle bulk, and strength and to gain body fat. Chronic (long-term) low testosterone may also cause weak bones (osteoporosis), mood changes, less energy, and smaller testes. Signs and symptoms (what you see and feel) vary from person to person.
Low testosterone is common in older men. An accurate blood test needs to be done in the morning between 7am-10am.
Causes of low testosterone
Beginning around age 30 to 40, testosterone levels may start to slowly decrease. This occurs naturally. This is a normal part of aging and often doesn’t cause problems. Low testosterone by itself is not a disease. Nor is a low testosterone level by itself an indication to take testosterone by injection or by a patch. Laboratory testing and a clinical evaluation of signs and symptoms are both important components of diagnosing testosterone deficiency in adult men.
Besides aging, there are a wide variety of factors that can contribute to low testosterone. Some causes are related to conditions that arise later in life, like obesity. Others are related to conditions that people are born with, like Klinefelter syndrome, though these are much rarer.
Some other causes of low testosterone include:
- Chronic disease such as type 2 diabetes, HIV/AIDS, liver disease, kidney disease or autoimmune diseases
- Injury or trauma to the testicles
- Removal of testicles to treat cancer
- Anabolic steroid use in the past
- Chemotherapy or radiation
- Use of medications such as antidepressants or narcotic pain medications
- Problems with glands in the brain (hypothalamus and pituitary) that control hormone production
- Low thyroid function
- Too much body fat (obesity)
- Other disorders, chronic diseases, medical treatments, or infection
Treatment with testosterone replacement therapy can help relieve signs and symptoms of low testosterone. However, there are risks associated with treatment, and it may not be appropriate for every man with low testosterone.
Healthy lifestyle choices, including exercise, good nutrition, maintaining a healthy weight and avoiding excessive use of illicit drugs and/or alcohol, can help keep testosterone levels within a normal range. There are no known ways to prevent low testosterone linked to genetic conditions, testicular damage, or pituitary disorders.
Low testosterone signs and symptoms
Some men with low testosterone do not have any symptoms. Low testosterone can produce a wide range of signs and symptoms that vary from man to man. Some symptoms are specifically linked to testosterone levels, such as:
- Reduced body and facial hair
- Very small testicles
- Incomplete/delayed sexual development
Examples of symptoms that are suggestive of testosterone deficiency include:
- Low sex drive
- Problems having an erection or erectile dysfunction
- Decreased spontaneous erections
- Enlarged breasts
- Infertility
- Low sperm count
Other symptoms are non-specific and a variety of other conditions could cause them. Examples include:
- Decrease in muscle size and strength
- Bone loss
- Symptoms of depression or changes in mood
- Ongoing weakness or fatigue
- Increased body fat, obesity
- Irritability
- Sleep problems such as insomnia
- Decreased brain function, such as poor memory or trouble concentrating
Some symptoms may be a normal part of aging. For example, it is normal to feel less interested in sex as you get older. But, it is not usually normal to have no interest in sex.
Symptoms may also be caused by other conditions, such as high blood pressure. If any of these symptoms are bothering you, talk with your health care provider.
Low testosterone diagnosis
Diagnosing low testosterone begins with a history of an individual’s signs and symptoms, along with a physical exam, followed by laboratory tests to look at testosterone levels. The Endocrine Society and the American Urological Association recommend relying on both clinical examination and laboratory testing to diagnose low testosterone.
It is important to note that screening for low testosterone in men without signs and symptoms is not recommended.
Additional laboratory tests are used to determine the underlying cause of low testosterone and monitor individuals receiving testosterone replacement therapy.
Laboratory Tests
- Testosterone level—this is the most important blood test for detecting low testosterone. Blood samples should be taken in the morning, after fasting, to help control for the daily variation in testosterone levels. The normal range is generally 300 to 1,000 ng/dL, but this depends on the lab that conducts the test. To get a diagnosis of low testosterone, you may need more than one early morning (7–10 AM) blood test and, sometimes, tests of pituitary gland hormones. Testosterone levels are typically sampled on at least two different days to confirm results. About 30% of men with an initial low testosterone result have normal levels after a repeated measurement. Testosterone is also measured to monitor treatment. About two-thirds of testosterone circulates in the blood bound to sex hormone binding globulin (SHBG) and slightly less than one-third bound to albumin. A small percent (less than 4%) circulates as free testosterone. The free plus the albumin-bound testosterone is the bioavailable fraction, which can act on target tissues. In many cases, measurement of total testosterone provides adequate information. However, in certain cases, for example when the level of SHBG is abnormal, a test for free or bioavailable testosterone may be performed as it may more accurately reflect the presence of a medical condition. Reference ranges for testosterone levels in adult men vary by age. (Levels naturally decrease as men age.) While accuracy of laboratory testing has significantly evolved over the past few decades, lab-to-lab variability can occur due to differences in testing equipment, chemical reagents, and techniques. This is why the reference range for testosterone is not provided here. It is important to use the range supplied by the laboratory that performed the test to evaluate whether results are “within normal limits.” It is also worthwhile recognizing that even in younger men, because the reference range is usually the central 95% of the results within a population, by definition, 2.5% of men will have a testosterone level below the lower limit of the reference interval. Another issue to consider is whether older men should have their own reference range for testosterone or should the reference range for men only be based on testosterone levels of men in 20’s or 30’s. In summary, men must consult their healthcare practitioner about the meaning of their testosterone test results.
- Luteinizing hormone (LH) and follicle-stimulating hormone (FSH)—LH is a hormone that stimulates testosterone production and FSH is associated with sperm production. These tests are used together to help distinguish between low testosterone caused by a testicular problem from low testosterone caused by a problem originating in the pituitary gland or hypothalamus. When LH and FSH levels are high and testosterone is low, it indicates that the cause of low testosterone originates in the testicles. When LH and FSH is normal or low, it indicates that a pituitary problem underlies low testosterone. Normal LH and FSH are typically seen with age-related low testosterone.
- Prolactin—prolactin is a pituitary hormone. It is tested if the pituitary gland is the suspected cause of low testosterone. High prolactin levels may indicate pituitary problems such as a tumor. High prolactin of any cause could interfere with normal testicular function.
Some tests may be done for men undergoing testosterone replacement therapy to monitor for side effects. Some examples include:
- Hemoglobin—hemoglobin may be monitored for an increase in red blood cells (polycythemia). Polycythemia can be a side effect of testosterone replacement therapy and can lead to vascular problems like blood clots.
- Lipid panel—to check for unhealthy lipid levels
- PSA—to screen for prostate cancer
Non-Laboratory Tests
- Magnetic resonance imaging (MRI) of the brain is sometimes used to check the pituitary gland and hypothalamus.
- A bone mineral density Dexa-Scan (dual-energy X-ray absorptiometry or DXA) may be used to look for changes in bone density due to low testosterone.
Low testosterone treatment
Men diagnosed with low testosterone due to late-onset hypogonadism may be treated with testosterone replacement therapy to improve signs and symptoms.
The American Urological Association recommends prescribing treatment only to men who meet the clinical and laboratory definitions of low testosterone. And testosterone replacement therapy may not be appropriate for everyone with a diagnosis of low testosterone. For example, the Endocrine Society recommends against routine replacement therapy for men over 65 and suggests making individualized treatment decisions for aging men. Treatment may also be inappropriate for individuals with certain health problems, such as prostate cancer or sleep apnea.
Some of the benefits and risks of hormone replacement therapy remain unclear and are the subjects of active research. It is important for individuals diagnosed with low testosterone to talk to their healthcare practitioner about expectations for treatment and the potential side effects.
If you have low testosterone, hormone therapy may help. The medicine used is man-made testosterone. This treatment is called testosterone replacement therapy. Testosterone replacement therapy can be given as a gel, patch, injection, or implant.
There are several ways to replace testosterone:
- Gel or patches that you put on your skin
- Injections (shots)
- Tablets that stick to the gums
- Pellets inserted under the skin or pills (in some countries outside the United States)
Testosterone replacement therapy may relieve or improve symptoms in some men. Testosterone replacement therapy may help keep bones and muscles strong. Testosterone replacement therapy seems to be more effective in young men with very low testosterone levels. But it is unclear whether testosterone replacement therapy is helpful for older men.
Testosterone replacement therapy has risks. These may include:
- Infertility
- Enlarged prostate leading to difficulty urinating
- Blood clots
- Worsening heart failure
Other possible risks of testosterone treatment include:
- A high red blood cell count
- Acne
- Breast enlargement
- An increase in prostate size
- Sleep apnea—the occasional stopping of breathing during sleep (rarely)
- Fluid buildup (edema) in ankles, feet and legs (rarely)
At this time, it is unclear whether testosterone replacement therapy increases the risk of heart attack, stroke, or prostate cancer.
Talk with your doctor about whether testosterone replacement therapy is right for you.
If you decide to start testosterone replacement therapy, be sure to see your doctor for regular checkups.
If I have a low testosterone level, will taking supplemental testosterone help?
Maybe. Testosterone supplements, either with gels, patches or injections, can raise testosterone levels. They may help to relieve some symptoms and/or prevent muscle and bone loss that occurs with aging in men; however, this has not been definitively proven. There is concern that testosterone replacement therapy may exacerbate preexisting prostate cancer, but no evidence of causing cancer. There are label warnings that testosterone administration may result in possible increased risk of heart attack and stroke. Although men with erectile dysfunction may have low testosterone, in many cases testosterone administration does not improve the symptoms because there are other underlying conditions. Therefore, consult a healthcare practitioner for a medical evaluation and consultation to determine if this is the right therapy for you.
Is the amount of hair directly proportional to the amount of testosterone in my body?
The amount, color, and texture of hair is largely determined by genetics. Studies have shown a proportional relationship of testosterone levels to the amount of body hair. The hair growth response to testosterone differs in different parts of the body. Hence, in some men, for example, testosterone promotes hair growth in the abdomen and back while hair growth is suppressed in the scalp, leading to male pattern baldness. Genetics plays a major role in the expression of the enzyme 5-alpha reductase, which converts testosterone to the hair-altering compound dihydrotestosterone, leading to a family tendency towards balding. The drug finasteride (Propecia®) inhibits the action of 5-alpha reductase and can reverse male pattern baldness in some men.
Androgen insensitivity syndrome
Androgen insensitivity syndrome is a rare condition that affects sexual development before birth and during puberty. A child born with androgen insensitivity syndrome is genetically male, but the external appearance of their genitals may be female or somewhere between male and female. People with androgen insensitivity syndrome are genetically male, with one X chromosome and one Y chromosome in each cell. Because their bodies are unable to respond to certain male sex hormones (called androgens), they may have mostly female external sex characteristics or signs of both male and female sexual development 18.
Androgen insensitivity syndrome is caused by a genetic fault that’s usually passed on to a child by their mother. This genetic fault means that, despite being genetically male, the body doesn’t respond to testosterone (the male sex hormone) properly and male sexual development doesn’t happen as normal.
This means the penis doesn’t form or is underdeveloped. The child’s genitals may appear female, or between male and female, but they don’t have a womb or ovaries and have fully or partially undescended testicles.
Women who carry the genetic fault won’t have androgen insensitivity syndrome themselves, but there’s a one in four chance each child they have will be born with the condition.
Someone with androgen insensitivity syndrome may benefit from psychological support, and in some cases may have treatment to alter the appearance of their genitals.
Most people born with the condition are unable to have children, but they’ll otherwise be perfectly healthy and able to lead a normal life.
Androgen insensitivity syndrome types
There are two main types of androgen insensitivity syndrome, which are determined by how much the body is able to use testosterone. These are:
Complete androgen insensitivity syndrome
Complete androgen insensitivity syndrome (Candrogen insensitivity syndrome) – where testosterone has no effect on sexual development, so the genitals are entirely female – including a vagina and labia (flaps of skin either side of the vaginal opening) – and affected babies are raised as girls. Complete androgen insensitivity syndrome (Candrogen insensitivity syndrome) isn’t usually obvious from birth, as affected babies have female genitals, as the genitals usually look normal for a girl. It’s often not diagnosed until puberty, when periods don’t start and pubic and underarm hair doesn’t develop.
Complete androgen insensitivity syndrome affects 2 to 5 per 100,000 people who are genetically male.
Complete androgen insensitivity syndrome occurs when the body cannot use androgens at all. People with this form of the condition have the external sex characteristics of females, but do not have a uterus and therefore do not menstruate and are unable to conceive a child (infertile). They are typically raised as females and have a female gender identity. Affected individuals have male internal sex organs (testes) that are undescended, which means they are abnormally located in the pelvis or abdomen, but this won’t be obvious unless they cause a hernia (where they push through a weakness in the surrounding tissue) or swelling in the labia. Undescended testes have a small chance of becoming cancerous later in life if they are not surgically removed. People with complete androgen insensitivity syndrome also have sparse or absent hair in the pubic area and under the arms.
The first obvious symptoms often don’t appear until puberty, which starts at around the age of 11.
When a girl with complete androgen insensitivity syndrome reaches puberty, she will:
- not start having periods
- develop little or no pubic and underarm hair
- develop breasts and have growth spurts as normal, although she may end up slightly taller than usual for a girl
Girls with complete androgen insensitivity syndrome don’t have a womb or ovaries, so are unable to get pregnant. Their vagina will also be shorter than normal, which may make having sex difficult.
Partial androgen insensitivity syndrome
Partial androgen insensitivity syndrome (Pandrogen insensitivity syndrome) – where testosterone still has some effect on sexual development, so the genitals are often between male and female. Partial androgen insensitivity syndrome (Pandrogen insensitivity syndrome) is usually noticed at birth because the genitals appear different.
Partial androgen insensitivity is thought to be at least as common as complete androgen insensitivity. Mild androgen insensitivity is much less common.
The partial and mild forms of androgen insensitivity syndrome result when the body’s tissues are partially sensitive to the effects of androgens. People with partial androgen insensitivity (also called Reifenstein syndrome) can have genitalia that look typically female, genitalia that have both male and female characteristics, or genitalia that look typically male. They may be raised as males or as females and may have a male or a female gender identity. People with mild androgen insensitivity are born with male sex characteristics, but they are often infertile and tend to experience breast enlargement at puberty.
The development of children with partial androgen insensitivity syndrome can vary.
In many cases, the genitalia are between male and female from birth. For example, affected babies may have:
- a very small penis or an enlarged clitoris (the sexual organ that helps women reach sexual climax)
- partially undescended testicles
- hypospadias – where the hole that carries urine out of the body is on the underside of the penis, rather than at the end
Children with partial androgen insensitivity syndrome are usually raised as boys, although they may experience poor penis development during puberty and develop small breasts. Most children with partial androgen insensitivity syndrome raised as boys will be infertile.
Some children with partial androgen insensitivity syndrome are raised as girls. Like those with complete androgen insensitivity syndrome, girls with partial androgen insensitivity syndrome will not have a womb or ovaries and will be unable to get pregnant.
Androgen insensitivity syndrome symptoms
Babies with androgen insensitivity syndrome will be genetically male, but will either have female genitals or an appearance between male and female genitalia.
There are two main types of androgen insensitivity syndrome, which affect people in different ways:
- complete androgen insensitivity
- partial androgen insensitivity
The main features of these two types are outlined above.
Androgen insensitivity syndrome causes
Mutations in the androgen receptor (AR) gene cause androgen insensitivity syndrome. The AR (androgen receptor) gene provides instructions for making a protein called an androgen receptor. Androgen receptors allow cells to respond to androgens, which are hormones (such as testosterone) that direct male sexual development. Androgens and androgen receptors also have other important functions in both males and females, such as regulating hair growth and sex drive. Mutations in the AR gene prevent androgen receptors from working properly, which makes cells less responsive to androgens or prevents cells from using these hormones at all. Depending on the level of androgen insensitivity, an affected person’s sex characteristics can vary from mostly female to mostly male.
Androgen receptors are present in many of the body’s tissues, where they attach (bind) to androgens. The resulting androgen-receptor complex then binds to DNA and regulates the activity of androgen-responsive genes. By turning the genes on or off as necessary, the androgen receptor helps direct the development of male sexual characteristics. Androgens and androgen receptors also have other important functions in both males and females, such as regulating hair growth and sex drive.
In one region of the AR gene, a DNA segment known as CAG is repeated multiple times. This CAG segment is called a triplet or trinucleotide repeat. In most people, the number of CAG repeats in the AR gene ranges from fewer than 10 to about 36.
Androgen insensitivity syndrome inheritance pattern
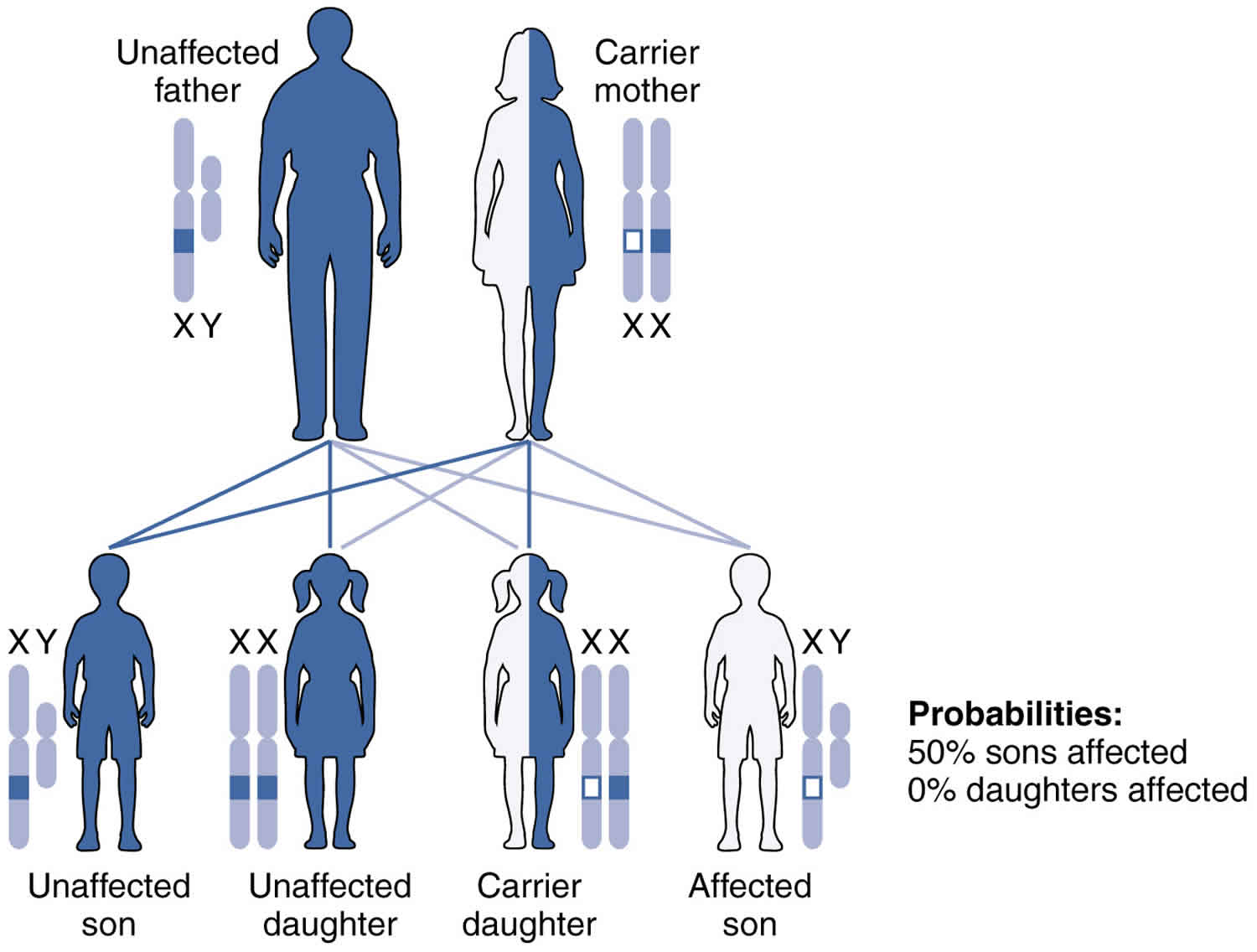
In most cases, the genetic fault is passed on to a child by their mother. The faulty gene is found on the mother’s X chromosome. Androgen insensitivity syndrome is inherited in an X-linked recessive pattern. A condition is considered X-linked if the mutated gene that causes the disorder is located on the X chromosome, one of the two sex chromosomes in each cell. In genetic males (who have only one X chromosome), one altered copy of the gene in each cell is sufficient to cause the condition. In genetic females (who have two X chromosomes), a mutation must be present in both copies of the gene to cause the disorder. Males are affected by X-linked recessive disorders much more frequently than females.
As the mother has two X chromosomes, the normal chromosome is able to make up for the faulty one, so she is a carrier of the faulty gene, but doesn’t have androgen insensitivity syndrome and is able to have children.
Any genetically female (XX) children the mother has will also inherit two X chromosomes and will be unaffected, although they too may be carriers and be able to pass the genetic fault on to any children they have.
If the mother has a genetically male (XY) child, there’s a chance they could pass on the faulty X chromosome, in addition to the Y chromosome the child gets from their father.
If this happens, the Y chromosome won’t be able to make up for the faulty X chromosome and the baby will develop androgen insensitivity syndrome.
This means women who carry the faulty X chromosome have a:
- one in four chance of giving birth to a girl who is unaffected, but can pass on the altered gene to her children
- one in four chance of having a boy who is unaffected
- one in four chance of having a girl who is unaffected and doesn’t carry the altered gene
- one in four chance of having a child with androgen insensitivity syndrome
About two-thirds of all cases of androgen insensitivity syndrome are inherited from mothers who carry an altered copy of the AR gene on one of their two X chromosomes. The remaining cases result from a new mutation that can occur in the mother’s egg cell before the child is conceived or during early fetal development.
Figure 5. Androgen insensitivity syndrome X-linked recessive inheritance pattern
Androgen insensitivity syndrome diagnosis
Androgen insensitivity syndrome is sometimes diagnosed soon after a baby is born, although often it’s not noticed until a child reaches puberty.
Doctors may suspect androgen insensitivity syndrome based on a child’s appearance and sexual development, but some tests will be needed to confirm the diagnosis.
Appearance and sexual development
Partial androgen insensitivity syndrome (Pandrogen insensitivity syndrome) is usually spotted soon after birth because the genitals have an unusual appearance.
Complete androgen insensitivity syndrome (Candrogen insensitivity syndrome) isn’t usually diagnosed at birth because the genitals look normal for a girl, although the condition may be picked up if the child develops a hernia.
Hernias are where an internal part of the body pushes through a weakness in the surrounding tissue. They can occur in babies with complete androgen insensitivity syndrome as a result of the testicles failing to move from the tummy into the scrotum.
When the baby has an operation to repair the hernia, the surgeon may find the testicles inside the hernia or in the tummy, and tests may be arranged to check for complete androgen insensitivity syndrome.
If a baby with complete androgen insensitivity syndrome doesn’t develop a hernia, the condition may go undiagnosed until puberty, when she doesn’t start having periods and doesn’t develop pubic and underarm hair.
Tests and scans
If androgen insensitivity syndrome is suspected, blood tests can be used to:
- check the sex chromosomes – sex chromosomes are bundles of genetic material that determine a person’s genetic sex; if their genetic sex is different from their physical appearance, they may have androgen insensitivity syndrome
- check for a genetic fault – androgen insensitivity syndrome is caused by a problem on the X chromosome, the sex chromosome a child with androgen insensitivity syndrome receives from their mother
- measure sex hormone levels – children with androgen insensitivity syndrome tend to have high levels of testosterone (the male sex hormone) in their blood
An ultrasound scan can also be carried out to confirm the absence of the womb and ovaries. Children with androgen insensitivity syndrome often have female genitals, but no female internal reproductive organs.
If a surgeon thinks they’ve found testicles in a baby’s tummy during a hernia repair operation, a small tissue sample (biopsy) may be taken and analysed to confirm they are testicles and not ovaries.
Testing family members and unborn babies
If someone in your family has androgen insensitivity syndrome and the specific genetic fault causing it has been identified, it may be possible to have a blood test to check if you carry the same fault and are at risk of passing it on to any children you have.
Testing can also be carried out in unborn babies when there’s a known family history of androgen insensitivity syndrome.
There are two main tests that can be carried out during pregnancy to determine whether a baby has the condition:
- chorionic villus sampling (CVS) – a sample of cells are removed from the afterbirth (placenta) for testing, usually with a needle; this is usually carried out between the 11th and 14th weeks of pregnancy
- amniocentesis – a needle is used to extract a sample of the fluid surrounding the baby, called amniotic fluid, for testing; this is usually carried out between the 15th and 20th weeks of pregnancy
It can be difficult to decide whether or not to have these tests, so it’s a good idea to speak to a genetic counselor first. It’s also important to be aware CVS and amniocentesis are estimated to carry around a 1 in 100 chance of causing a miscarriage.
Androgen insensitivity syndrome treatment
Surgery
Children with complete androgen insensitivity syndrome and partial androgen insensitivity syndrome will sometimes need surgery to help change their body and genitals to be more consistent with the gender they’re raised as.
Some procedures may be best carried out while your child is still young, but others can be delayed until they’re older.
Hernia repair
Children with androgen insensitivity syndrome sometimes develop a hernia (where an internal part of the body pushes through a weakness in the surrounding tissue) soon after birth. This is a result of their testicles failing to move from the tummy to the scrotum.
This can be repaired by closing and strengthening the gap created in the surrounding tissues. The testicles may also be removed during another operation.
Removing the testicles
Girls with complete androgen insensitivity syndrome will usually have their internal testicles removed, as there’s a very small risk they could become cancerous if left in place.
This procedure is often delayed until after puberty because the testicles produce hormones that help girls with complete androgen insensitivity syndrome develop a normal female body shape without hormone treatment, and the risk of the testicles becoming cancerous before adulthood is extremely low.
If you decide you’d prefer for your child’s testicles to be removed before puberty, hormone treatment will be needed to help them develop a more female body shape.
Moving the testicles and reconstructing the penis
Boys with partial androgen insensitivity syndrome may be born with fully or partially undescended testicles. If this happens, an operation can be carried out to move the testicles into the scrotum.
Surgery can also be carried out to straighten the penis and correct hypospadias, where the hole that carries urine out of the body is on the underside of the penis, rather than at the end.
Vaginal surgery
Girls with androgen insensitivity syndrome often have a shorter vagina than normal, which can make having sex difficult. Treatment for this is usually delayed until after puberty, so she can decide if she wants treatment for it and choose what treatment she prefers.
In many cases, surgery isn’t necessary because the vagina can be lengthened using a method called dilation. This involves inserting small plastic rods that gradually widen and deepen the vagina.
Alternatively, a procedure to remove skin and tissue from the genital area and use it to reconstruct the vagina can be carried out.
Women with partial androgen insensitivity syndrome can also have surgery to reduce the size of their clitoris. This may make it less sensitive, but achieving an orgasm should still be possible.
Male breast reduction
Boys with partial androgen insensitivity syndrome will sometimes experience some breast development around puberty. If this occurs, an operation can be carried out to remove the breast tissue.
Hormone therapy
If the testicles are removed when a girl with complete androgen insensitivity syndrome is a child, treatment with the hormone estrogen (the female sex hormone) is usually started at the age of 10 or 11, so female development begins at an age consistent with puberty.
This won’t cause periods to start, as people with complete androgen insensitivity syndrome don’t have a womb, but it will help them develop a more female body shape. It will also be continued after puberty to stop them developing menopausal symptoms and weak bones (osteoporosis).
Women with complete androgen insensitivity syndrome who had their testicles removed after puberty will also need to take estrogen to prevent the menopause and osteoporosis.
Children with partial androgen insensitivity syndrome may also need to take hormone supplements. Girls with partial androgen insensitivity syndrome who have their testicles removed may need estrogen to encourage puberty.
Boys with partial androgen insensitivity syndrome may need androgens (male sex hormones) to encourage certain male characteristics, such as the growth of facial hair, penis growth, or deepening of the voice.
Living with androgen insensitivity syndrome
Children with androgen insensitivity syndrome and their parents will be supported by a team of specialists, who will offer ongoing care and support. They will help you decide whether to raise your child as a girl or a boy while they’re still very young.
Most children with complete androgen insensitivity syndrome are raised as girls, while those with partial androgen insensitivity syndrome can be brought up either as girls or boys. It’s up to you as a parent, with help from specialists, to decide what you think is in the best interests of your child.
Once you’ve decided, you can learn about the treatments available that can help make your child’s body look more consistent with the chosen gender and help them develop more naturally.
This may involve surgery to alter the appearance or function of their genitals, and hormone treatment to encourage female or male development during puberty.
However, psychological support and advice to help you deal with any issues that arise as a result of your child’s condition is probably the most important aspect of care.
With appropriate care and support, most people with androgen insensitivity syndrome are able to come to terms with their condition and lead normal lives.
Choosing your child’s gender
As a parent of a child with androgen insensitivity syndrome, one of the biggest decisions you’ll have to make will be to choose which gender to raise your child as. You’ll be given lots of information to help you make this decision.
Most parents of children with complete androgen insensitivity syndrome (Candrogen insensitivity syndrome) choose to raise their child as a girl, as they have female genitals and often ultimately end up identifying with being female.
The decision is more difficult if your child has partial androgen insensitivity syndrome (Pandrogen insensitivity syndrome), as their genitals may have both male and female aspects. You’re entitled to specialist advice about your child’s future development and any gender identity issues that could arise later on.
Most children with partial androgen insensitivity syndrome stay with the gender they’ve been raised as. However, some people feel this doesn’t represent who they are and decide to switch gender in later life.
Talking to your child about androgen insensitivity syndrome
Parents often wonder when and what they should say to their child about their condition.
Many people feel it’s best to explain the basic facts about androgen insensitivity syndrome to the child as soon as possible. They can then be given more detailed information as they get older, as their ability to understand increases.
It’s usually recommended that a child fully understands their condition before they reach puberty. This can be a stressful time anyway, but it could be very traumatic if your child starts puberty without knowing about the possible changes they may experience, or the differences between them and their friends.
The situation can be more difficult if a girl with complete androgen insensitivity syndrome isn’t diagnosed until she has started puberty. The health professionals looking after your child can advise you on how to talk to your child and support you through this process.
Support for parents
If your child is diagnosed with androgen insensitivity syndrome, you should be offered counseling to help you come to terms with your emotions.
A diagnosis of androgen insensitivity syndrome can come as a shock to parents, and feelings of shame, guilt, anger and anxiety are common.
Talking to other parents who have a child with androgen insensitivity syndrome may also help. There are organizations that can put you in touch with other families affected by the condition.
- The Androgen Insensitivity Syndrome Support Group (http://www.aissg.org/)
- Accord Alliance promotes comprehensive and integrated approaches to care that enhance the health and well-being of people and families affected by differences of sex development (http://www.accordalliance.org/)
- AIS-DSD Support Group (http://aisdsd.org/)
Support for children
Some young children with androgen insensitivity syndrome don’t need psychological support because their condition is completely natural to them.
However, as a child gets older, they may need support from a therapist with experience in androgen insensitivity syndrome to help them understand and cope with their condition.
A long-term relationship between the child and therapist is ideal so any new issues can be discussed as the child matures.
Gender identity and gender dysphoria
Most children with androgen insensitivity syndrome grow up to feel they are the gender their parents chose to raise them as. This feeling is known as their gender identity.
In a few cases, older children and adults with androgen insensitivity syndrome feel their gender identity doesn’t match the gender they’ve been raised as. This is known as gender dysphoria.
People with gender dysphoria often have a desire to live as a member of the opposite sex, and may want treatment to make their physical appearance more consistent with their gender identity.
If your child is diagnosed with androgen insensitivity syndrome, you should be told about the issues of gender identity that could arise as your child gets older.
References- McEwan IJ, Brinkmann AO. Androgen Physiology: Receptor and Metabolic Disorders. [Updated 2016 Jun 12]. In: De Groot LJ, Chrousos G, Dungan K, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279028
- Hauser LJ, Jensen EL, Mirsky DM, Chan KH. Pediatric anosmia: A case series. Int. J. Pediatr. Otorhinolaryngol. 2018 Jul;110:135-139
- BS DJHMB. Androgen Physiology, Pharmacology and Abuse. [Updated 2016 Dec 12]. In: De Groot LJ, Chrousos G, Dungan K, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279000
- Quigley CA, DeBellis A, Marschke KB, El-Awady MK, Wilson EM, French FF (1995) Androgen receptor defects: historical, clinical and molecular perspectives. Endocrine Reviews. 16: 271-321
- Gonzalez-Montelongo MC, Marin R, Gomez T, Diaz M (2010) Androgens are powerful non-genomic inducers of calcium sensitization in visceral smooth muscle. Steroids. 75(8-9): 533-8
- Burdea L, Mendez MD. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Mar 20, 2018. 21 Hydroxylase Deficiency.
- Clark BJ, Prough RA, Klinge CM. Mechanisms of Action of Dehydroepiandrosterone. Vitam. Horm. 2018;108:29-73.
- Nassar GN, Leslie SW. Physiology, Testosterone. [Updated 2018 Oct 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526128/
- Kalfa N, Gaspari L, Ollivier M, Philibert P, Bergougnoux A, Paris F, Sultan C. MOLECULAR GENETICS OF HYPOSPADIAS AND CRYPTORCHIDISM RECENT DEVELOPMENTS. Clin. Genet. 2018 Aug 07
- Nassar GN, Leslie SW. Physiology, Testosterone. [Updated 2018 Oct 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526128
- Walters KA, Bertoldo MJ, Handelsman DJ. Evidence from animal models on the pathogenesis of PCOS. Best Pract. Res. Clin. Endocrinol. Metab. 2018 Jun;32(3):271-281.
- Spaziani M, Mileno B, Rossi F, Granato S, Tahani N, Anzuini A, Lenzi A, Radicioni AF. Endocrine and metabolic evaluation of classic Klinefelter syndrome and high-grade aneuploidies of sexual chromosomes with male phenotype: are they different clinical conditions? Eur. J. Endocrinol. 2018 Apr;178(4):343-352.
- Makieva S, Saunders PT, Norman JE. Androgens in pregnancy: roles in parturition. Hum Reprod Update. 2014;20(4):542-59. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4063701/
- Zhang JR, Zhang PY, Sun LG. [Mild androgen insensitivity syndrome: a case report]. Zhonghua Nei Ke Za Zhi. 2018 Aug 01;57(8):600-602
- Miller WL, Auchus RJ (2011) The molecular biology, biochemistry, and physiology of human steroidogenesis and its disorders. Endocrine Reviews. 32(1): 81-151
- Bozzola M, Bozzola E, Montalbano C, Stamati FA, Ferrara P, Villani A. Delayed puberty versus hypogonadism: a challenge for the pediatrician. Ann Pediatr Endocrinol Metab. 2018 Jun;23(2):57-61
- Baillargeon J, Kuo YF, Westra JR, Urban RJ, Goodwin JS. Testosterone Prescribing in the United States, 2002-2016. JAMA. 2018 Jul 10;320(2):200-202.
- Androgen insensitivity syndrome. https://ghr.nlm.nih.gov/condition/androgen-insensitivity-syndrome





{kind=link}