
Autonomic nervous system disorders
Your autonomic nervous system is the part of your nervous system that controls involuntary actions, such as the beating of your heart and the widening or narrowing of your blood vessels. When something goes wrong in this system, it can cause serious problems, including:
- Blood pressure problems
- Heart problems
- Trouble with breathing and swallowing
- Erectile dysfunction in men
Autonomic nervous system disorders can occur alone or as the result of another disease, such as Parkinson’s disease, alcoholism and diabetes. Problems can affect either part of the autonomic nervous system, as in complex regional pain syndromes, or all of the autonomic nervous system. Some types are temporary, but many worsen over time. When they affect your breathing or heart function, these disorders can be life-threatening.
Some autonomic nervous system disorders get better when an underlying disease is treated. Often, however, there is no cure. In that case, the goal of treatment is to improve symptoms.
Autonomic nervous system
The autonomic nervous system is the part of the nervous system that regulates cardiac muscle, smooth muscle, and glands. These tissues are often referred to as visceral effectors because they are usually associated with the viscera (internal organs) of the body. The term autonomic is derived from the Latin words auto- = self and -nomic = law because the autonomic nervous system was once thought to be self-governing.
The autonomic nervous system consists of autonomic motor neurons that regulate visceral activities by either increasing (exciting) or decreasing (inhibiting) ongoing activities in their eff ector tissues (cardiac muscle, smooth muscle, and glands). Changes in the diameter of the pupils, dilation and constriction of blood vessels, and adjustment of the rate and force of the heartbeat are examples of autonomic motor responses. Unlike skeletal muscle, tissues innervated by the autonomic nervous system oft en function to some extent even if their nerve supply is damaged. The heart continues to beat when it is removed for transplantation into another person, smooth muscle in the lining of the gastrointestinal tract contracts rhythmically on its own, and glands produce some secretions in the absence of autonomic nervous system control.
The autonomic nervous system consists of two main division (branches):
- the sympathetic nervous system and
- the parasympathetic nervous system.
Most organs receive nerves from both of these divisions, an arrangement known as dual innervation. In general, one division stimulates the organ to increase its activity (excitation), and the other division decreases the organ’s activity (inhibition). For example, neurons of the sympathetic nervous system increase heart rate, and neurons of the parasympathetic nervous system slow it down. The sympathetic nervous system promotes the fight-or-flight response, which prepares the body for emergency situations. By contrast, the parasympathetic nervous system enhances rest-and-digest activities, which conserve and restore body energy during times of rest or digesting a meal. Although both the sympathetic and parasympathetic divisions are concerned with maintaining health, they do so in dramatically different ways.
The autonomic nervous system is also comprised of a third division known as the enteric nervous system. The enteric nervous system consists of millions of neurons in plexuses that extend most of the length of the gastrointestinal tract. Its operation is involuntary. Although the neurons of the enteric nervous system can function autonomously, they can also be regulated by the other divisions of the autonomic nervous system. The enteric nervous system contains sensory neurons, interneurons, and motor neurons. Enteric sensory neurons monitor chemical changes within the gastrointestinal tract as well as the stretching of its walls. Enteric interneurons integrate information from the sensory neurons and provide input to motor neurons. Enteric motor neurons govern contraction of gastrointestinal tract smooth muscle and secretion of gastrointestinal tract glands.
Most autonomic motor pathways consist of two motor neurons in series; that is, one following the other. The first neuron (preganglionic neuron) has its cell body in the central nervous system; its myelinated axon extends from the central nervous system to an autonomic ganglion. The cell body of the second neuron (postganglionic neuron) is also in that same autonomic ganglion; its unmyelinated axon extends directly from the ganglion to the eff ector (smooth muscle, cardiac muscle, or a gland). Alternatively, in some autonomic pathways, the first motor neuron extends to specialized cells called chromaffin cells in the adrenal medullae (inner portion of the adrenal glands) rather than an autonomic ganglion. Chromaffin cells secrete the neurotransmitters epinephrine and norepinephrine (NE). Autonomic motor neurons release either Acetylcholine (ACh) or norepinephrine (NE).
Figure 1. Autonomic nervous system
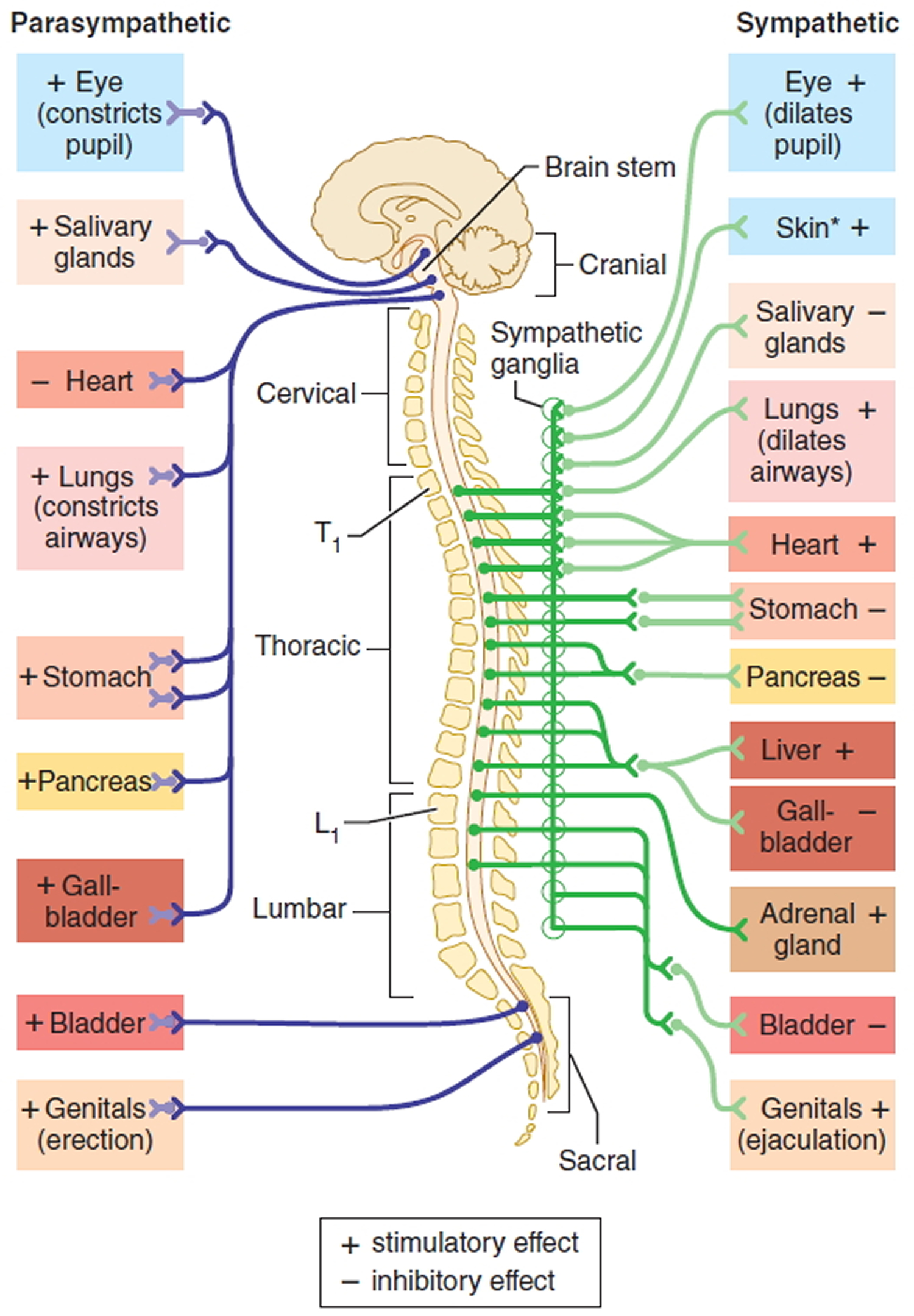
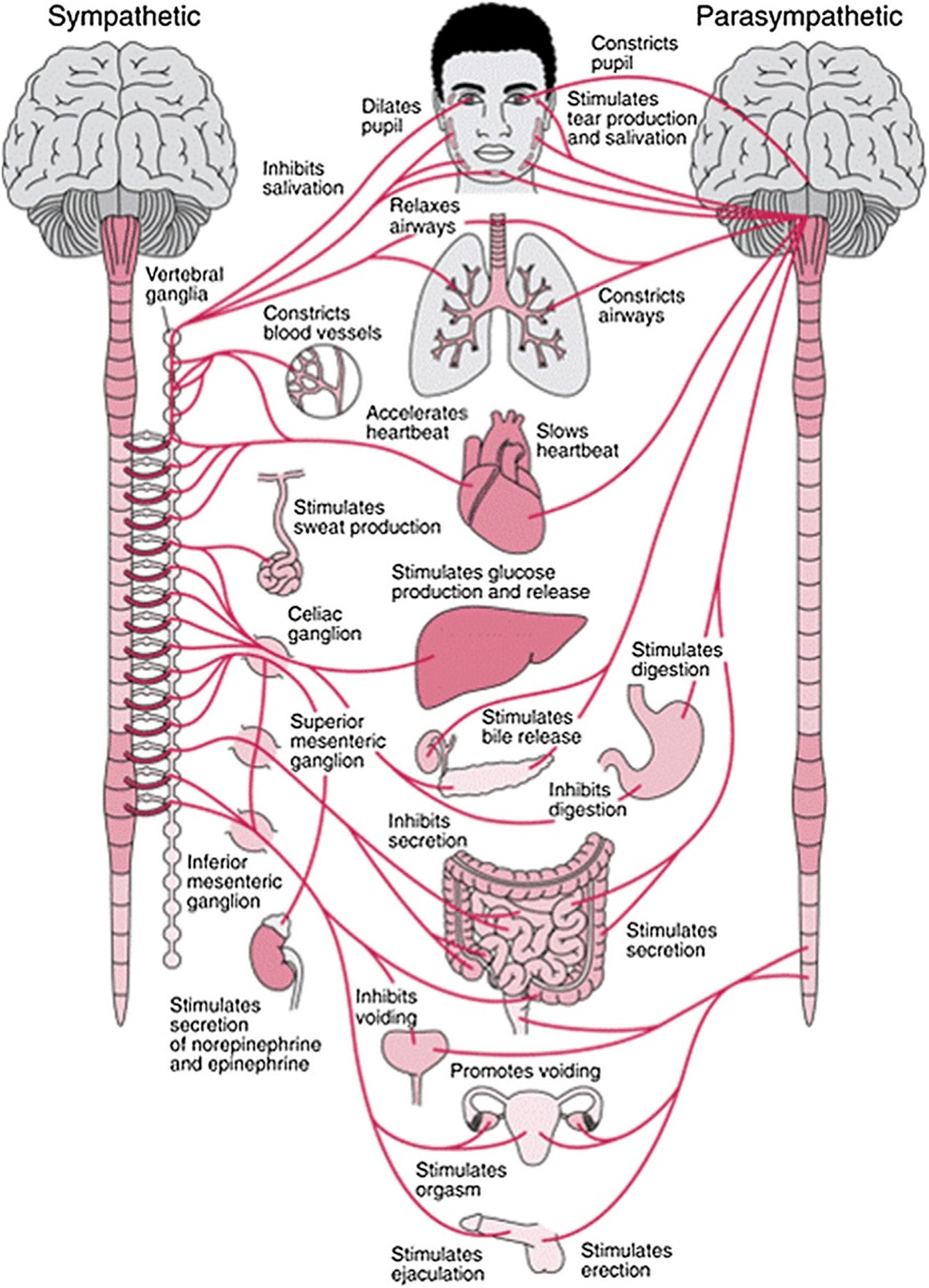
Figure 2. Autonomic nervous system
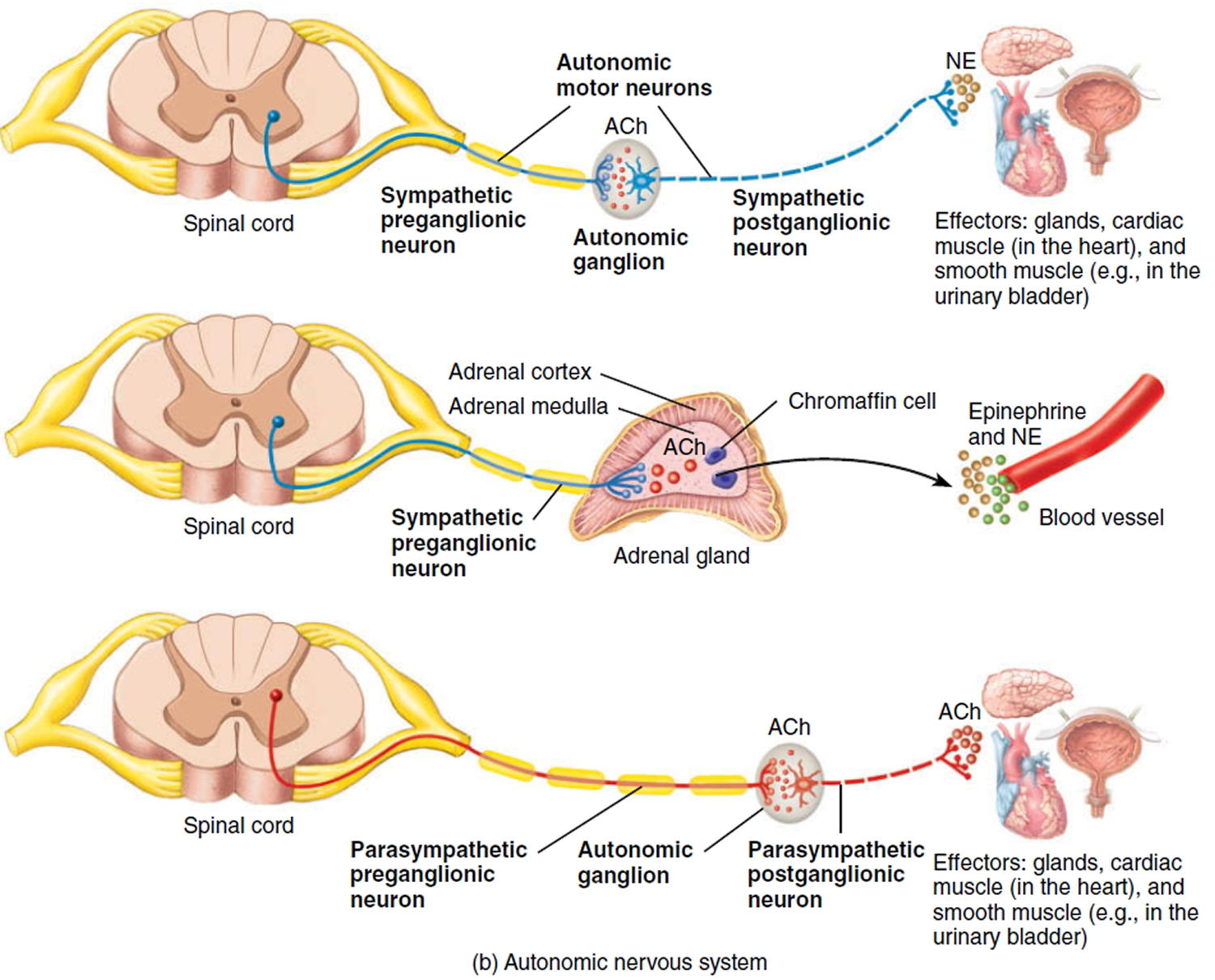
Footnote: Acetylcholine (ACh) and Norepinephrine (NE)
The autonomic nervous system usually operates without conscious control. For example, you probably cannot voluntarily slow down your heart rate; instead, your heart rate is subconsciously regulated. For this reason, some autonomic responses are the basis for polygraph (“lie detector”) tests. However, practitioners of yoga or other techniques of meditation may learn how to regulate at least some of their autonomic activities through long practice. Biofeedback, in which monitoring devices display information about a body function such as heart rate or blood pressure, enhances the ability to learn such conscious control.
The autonomic nervous system can also receive sensory input from sensory neurons associated with interoceptors, sensory receptors located in blood vessels, visceral organs, muscles, and the nervous system that monitor conditions in the internal environment. Examples of interoceptors are chemoreceptors that monitor blood CO2 level and mechanoreceptors that detect the degree of stretch in the walls of organs or blood vessels. Unlike those triggered by a flower’s perfume, a beautiful painting, or a delicious meal, these sensory signals are not consciously perceived most of the time, although intense activation of interoceptors may produce conscious sensations. Two examples of perceived visceral sensations are pain sensations from damaged viscera and angina pectoris (chest pain) from inadequate blood flow to the heart. Signals from the somatic senses and special senses, acting via the limbic system, also influence responses of autonomic motor neurons. Seeing a bike about to hit you, hearing squealing brakes of a nearby car, or being grabbed by an attacker would all increase the rate and force of your heartbeat.
Types of autonomic disorders
The autonomic nervous system regulates the function of the body’s internal organs, such as heart rate, blood pressure, digestion, and body temperature. People with an autonomic disorder have trouble regulating one or more of these systems, which can result in fainting, lightheadedness, fluctuating blood pressure, and other symptoms.
Orthostatic hypotension
Orthostatic hypotension is a sudden drop in blood pressure that occurs when a person stands up, causing low blood pressure in the upright position. This leads to a decrease in blood supply to the brain. The condition usually causes a person to feel dizzy or lightheaded. Sometimes, orthostatic hypotension can cause a person to faint.
Other symptoms of orthostatic hypotension include fatigue, particularly on exertion; vision problems; soreness in the back of the neck and shoulders, sometimes called “coat hanger” pain; or shortness of breath.
Symptoms are worse when people stand up and improve when they sit or lie down. Common causes of orthostatic hypotension include dehydration, hot environments, or standing for long periods of time. Most people feel better with hydration and rest.
Many people occasionally feel dizzy or lightheaded after standing. However, for those who feel lightheaded or lose consciousness every time they stand up, it could be a sign of an autonomic disorder.
Orthostatic hypotension can cause complications—especially in older adults—such as falling down as a result of fainting. People with the condition are at risk for bone fractures, stroke due to the reduced blood supply to the brain, or cardiovascular conditions such as chest pain or heart failure.
Postprandial hypotension
Postprandial hypotension is a sudden drop in blood pressure after a meal, caused by blood pressure changes while you’re digesting food. Symptoms include dizziness, lightheadedness, or fainting about 15 to 90 minutes after eating. The condition is common in adults over the age of 60 and people with other disorders of the autonomic nervous system.
During digestion, extra blood is diverted to the stomach and small intestine, causing the heart to beat faster and harder while blood vessels far from the digestive system narrow. These actions maintain blood pressure and blood flow throughout the body. However, in people with postprandial hypotension, the heart rate doesn’t beat as fast as needed and the blood vessels don’t constrict as they should, so blood pressure drops.
Multiple system atrophy
Multiple system atrophy is a rare autonomic disorder that typically affects men and women in their 50s and advances rapidly over the course of 5 to 10 years. The condition causes a progressive loss of motor function and, eventually, the need to use a wheelchair.
There are two different types of this condition: the cerebellar type and the Parkinsonian type. How a person is diagnosed depends on the most prominent symptoms at the time he or she is evaluated.
People with the Parkinsonian type have symptoms similar to Parkinson’s disease, such as moving slowly, stiffness, tremors, and problems with balance and coordination.
Those with the cerebellar type have loss of coordination, difficulty swallowing, speech problems or a quivering voice, and unusual eye movements.
This condition tends to progress more rapidly than Parkinson’s disease, and most people eventually require an aid for walking, such as a cane, walker, or wheelchair, within a few years of the onset of symptoms.
Pure autonomic failure
Pure autonomic failure is a rare neurodegenerative disease of the autonomic nervous system, which regulates involuntary body processes such as blood pressure and breathing rate. Pure autonomic failure affects only the peripheral autonomic nervous system, which means it does not involve the brain and spinal cord (the central nervous system). Pure autonomic failure usually begins in midlife, although it can begin earlier. The main symptom of pure autonomic failure is orthostatic hypotension, a sudden drop in blood pressure upon standing. This causes a person to feel dizzy and lightheaded, requiring them to sit or lie down to prevent fainting. People with pure autonomic failure also have an abnormal blood pressure response to other common daily activities or exposures, as well as additional symptoms affecting various body systems such as sexual dysfunction, a decreased ability to sweat, elevated blood pressure when lying down, and changes in gastrointestinal and urinary habits. The condition affects men slightly more often than women, and is often found in middle-aged to older adults.
The reason that pure autonomic failure develops is not known. Pure autonomic failure is not known to be inherited. The symptoms are caused by abnormal accumulations of protein, called Lewy bodies, in the cells of autonomic nerves. The Lewy bodies restrict the production and release of norepinephrine from nerve cells, which in turn causes hypotension. Diagnosing pure autonomic failure may involve tilt table testing, 24-hour blood pressure monitoring, hyperventilation testing, and a norepinephrine blood test. Treatment options do not stop pure autonomic failure disease progression but help to control symptoms. Options may include avoiding triggers of symptoms, increasing fluid and salt intake, using compressive garments, and/or various medications. Pure autonomic failure usually has a slowly progressive course and may result in a person being restricted to a reclined position in their home.
Afferent baroreflex failure
Afferent baroreflex failure is an autonomic disorder that causes fluctuations in blood pressure due to a failure of the blood pressure-sensing nerves that relay information to the brain. As a result, blood pressure alternates between being too high and too low. Symptoms include dizziness and fainting as well as headaches, sweating, and skin flushing.
The condition occurs when there is damage to the blood pressure-sensing nerves in the neck following cancer treatment, surgery, or radiation therapy. It can happen in people who have a stroke that affects the areas of the brain where blood pressure information is relayed. It can also be a result of hereditary disorders that affect the development of blood pressure-sensing nerves.
Familial dysautonomia
Familial dysautonomia is a rare inherited condition that affects the development of the autonomic and sensory nervous systems. People with this condition have unstable blood pressure that alternates between being too high and too low. They may also have reduced sensitivity to pain and temperature and an absence of tears when crying.
Other common symptoms include difficulty swallowing, severe vomiting or gastroesophageal reflux, poor muscle tone, excessive sweating, overproduction of saliva and mucus, and blotchy reddening of the skin when excited or eating. People with familial dysautonomia may develop chronic breathing problems due to reflux of stomach acid or food. They may also have vision problems due to progressive damage to the optic nerve in the eyes.
During times of stress, people with familial dysautonomia may experience dramatic high blood pressure and heart rate accompanied by vomiting or retching. This is known as an autonomic crisis.
Autoimmune autonomic ganglionopathy
Autoimmune autonomic ganglionopathy is a rare autoimmune disorder in which the body’s immune system mistakenly attacks and damages certain parts of the autonomic nervous system. Signs and symptoms of the condition vary but may include severe orthostatic hypotension (low blood pressure upon standing); fainting; constipation; fixed and dilated pupils; urinary retention; and/or dry mouth and eyes. The exact underlying cause of autoimmune autonomic ganglionopathy is poorly understood. Treatment depends on many factors including the severity of the condition and the signs and symptoms present in each person. Due to the rarity of autoimmune autonomic ganglionopathy, there are no standard treatment protocols; however, treatment with plasmapheresis, intravenous (IV) immunoglobulin, corticosteroids or immunosuppressive drugs has been reported with variable success. Approximately one third of affected people may improve spontaneously without treatment, but the recovery is often incomplete.
Congenital central hypoventilation syndrome
Congenital central hypoventilation syndrome is a disorder of the autonomic nervous system that affects breathing. It causes a person to hypoventilate (especially during sleep), resulting in a shortage of oxygen and a buildup of carbon dioxide in the blood. It have two forms of presentation, a classic form that usually begin shortly after birth in newborns, and a milder later-onset presentaition in toddlers, children and adults. Affected infants hypoventilate upon falling asleep and exhibit a bluish appearance of the skin or lips (cyanosis). Other features may include difficulty regulating heart rate and blood pressure; decreased perception of pain; low body temperature; sporadic profuse sweating; Hirschsprung disease; constipation; learning difficulties; eye abnormalities; and a characteristic facial appearance (having a short, wide, somewhat flattened face). They can also have tumors of neural crest origin, such as neuroblastoma, ganglioneuroblastoma, and ganglioneuroma. The later-onset form is milder, and some cases may present as infants and children who die suddenly and unexpectedly (“SIDS” and “sudden unexplained death of childhood [SUDC]”).
Congenital central hypoventilation syndrome is caused by a variation (mutation) in the PHOX2B gene and is inherited in an autosomal dominant manner. However, over 90% of cases are due to a new mutation in the affected person and are not inherited from a parent. Diagnosis is made with the clinical symptoms and the genetic test showing the variation in the PHOX2B gene. Treatment typically includes mechanical ventilation or use of a diaphragm pacemaker. People who have been diagnosed as newborns and adequately ventilated throughout childhood may reach the age of 20 to 30 years, and can live independently. In the later-onset form, people who were diagnosed when they were 20 years or older have now reached the age of 30 to 55 years.
Horner’s syndrome
Horner’s syndrome is a rare condition characterized by miosis (constriction of the pupil), ptosis (drooping of the upper eyelid), and anhidrosis (absence of sweating of the face). Horner’s syndrome is caused by damage to the sympathetic nerves of the face. The underlying causes of Horner’s syndrome vary greatly and may include a tumor, stroke, injury, or underlying disease affecting the areas surrounding the sympathetic nerves. In rare cases, Horner’s syndrome is congenital (present from birth) and may be associated with a lack of pigmentation of the iris (colored part of the eye). The abnormalities in the eye area related to Horner syndrome do not generally affect vision or health. However, the nerve damage that causes Horner syndrome may result from other health problems, some of which can be life-threatening. Treatment of Horner’s syndrome depends on the underlying cause.
Holmes-Adie syndrome
Holmes-Adie syndrome is a neurological disorder affecting the pupil of the eye and the autonomic nervous system. It is characterized by one eye with a pupil that is larger than normal and constricts slowly in bright light (tonic pupil), along with the absence of deep tendon reflexes, usually in the Achilles tendon. Holmes-Adie syndrome is thought to be the result of a neurotrophic (acting on neurons, or nerve cells) viral infection that causes inflammation and damage to neurons in the ciliary ganglion, an area of the brain that controls eye movements, and the dorsal root ganglion, an area of the spinal cord involved in the response of the autonomic nervous system. Holmes-Adie syndrome begins gradually in one eye, and often progresses to involve the other eye. At first, it may only cause the loss of deep tendon reflexes on one side of the body, but then progress to the other side. The eye and reflex symptoms may not appear at the same time. People with Holmes-Adie syndrome may also sweat excessively, sometimes only on one side of the body. The combination of these 3 symptoms – abnormal pupil size, loss of deep tendon reflexes, and excessive sweating – is usually called Ross’s syndrome, although some doctors will still diagnose the condition as a variant of Holmes-Adie syndrome. Some individuals will also have cardiovascular abnormalities. The Holmes-Adie syndrome symptoms can appear on their own, or in association with other diseases of the nervous system, such as Sjogren’s syndrome or migraine. It is most often seen in young women. It is rarely an inherited condition.
Doctors may prescribe reading glasses to compensate for impaired vision in the affected eye, and pilocarpine drops to be applied 3 times daily to constrict the dilated pupil. Thoracic sympathectomy, which severs the involved sympathetic nerve, is the definitive treatment for excessive sweating.
Autonomic disorders diagnosis
There are many types of autonomic disorders, some of which occur alone. Others occur as the result of another disease, such as Parkinson’s disease or diabetes. To diagnose the conditions, a doctor performs a physical exam and reviews a person’s medical history.
Neurological examination
A doctor performs a neurological examination to determine whether there are any underlying causes of autonomic dysfunction. He or she may assess how a person moves or walks and his or her ability to sense vibration, touch, or pain.
Autonomic testing
Autonomic testing is designed to determine how well the body regulates the internal organs. During these tests, doctors use an electrocardiogram, or EKG, to monitor electrical activity in the heart and special cuffs on the fingers to continuously measure blood pressure. Doctors may record other physiologic functions, depending on a person’s symptoms, including sweating, respiration, production of carbon dioxide, oxygen saturation, the amount of blood the heart pumps, and the amount of blood going through the brain.
The tests involve performing different breathing exercises and changing position, from lying down to standing upright. These activities are meant to stimulate the autonomic nervous system to produce changes in blood pressure, heart rate, sweating, and blood flow to the brain during a short period of time so the doctor can identify any autonomic disorder.
Doctors may also order blood tests to assess the release of neurotransmitters and hormones that help to control blood pressure.
Valsalva maneuver
To test the body’s ability to compensate for changes in the amount of blood that returns to the heart, a doctor asks a person to perform a test called the Valsalva maneuver. The Valsalva maneuver involves forcefully exhaling against a closed airway. This is usually done by breathing through a mouthpiece and pinching the nose shut while blowing hard, like you’re blowing up a balloon.
During this test, doctors record the strength and depth of respiration and changes in heart rate and blood pressure through electrodes on the chest and cuffs on the fingers. People with autonomic dysfunction have changes in heart rate, blood pressure, or both that are different from those in people who don’t have these disorders.
Deep breathing
A doctor performs the deep breathing test to determine the function of the vagus nerve that controls the heart. The purpose of this test is to examine how much the heart rate changes in response to breathing in and breathing out. The test involves following commands to breathe slowly and deeply for one minute, while expansion of the chest, heart rate, and blood pressure are recorded through electrodes on the chest and cuffs on the fingers.
Tilt table test
A doctor performs a tilt table test to determine whether standing up provokes a drop in blood pressure or fainting. The purpose is to reproduce a person’s symptoms in a controlled laboratory setting.
During this test, a person’s heartbeat, blood pressure, respiration, and sweating are continuously recorded while he or she lies on a stretcher-like table relaxing and breathing normally for five minutes. Seatbelt-like straps are then attached around the abdomen and legs and the table tilts the person upright to a 60-degree angle. The tilting continues for up to 45 minutes or until the person has a drop in blood pressure and experiences low blood pressure symptoms such as dizziness, lightheadedness, or near fainting.
As soon as a person starts to feel symptoms of low blood pressure, the table is tilted back and the person is returned to the lying position, where symptoms get better.
Samples of blood are taken while the person is in the lying and the standing position to check the release of neurotransmitters and hormones that are involved in the control of blood pressure.
Doctors may also measure blood supply to the brain using a small ultrasound probe mounted on a headband. This allows the doctors to see whether symptoms that a person has during a tilt table test are related to changes in blood supply to the brain.
In addition, specialists also measure breathing rate throughout the tilt table test using a small plastic nasal tube called a cannula that monitors the level of carbon dioxide in each breath.
Sweat test
A sweat test evaluates how the nerves that control sweat glands respond to stimulation. During this test, a mild, painless electrical current is passed through the forearms, foot, and leg. A computer analyzes how the nerves and sweat glands react.
These nerves can be affected by different autonomic disorders like pure autonomic failure and Parkinson’s disease. The test can pinpoint where in the autonomic nervous system the problem is.
Ambulatory blood pressure monitoring
An ambulatory blood pressure machine is a portable device that you take home and wear. It is programmed to measure your blood pressure at intervals throughout the day and night. Depending on the results of the ambulatory blood pressure measurements, doctors may adjust any medications you are on, or prescribe different ones to help control blood pressure.
Bladder ultrasound
A bladder ultrasound is an imaging method to study the function of your bladder, which is controlled by autonomic nerves. The painless test is done after you urinate to measure how much urine is left in your bladder.
Autonomic nervous system disorders treatment
For many people with autonomic disorders, medications to regulate blood pressure, improve digestion, and target neurological processes can help reduce symptoms. Doctors may also recommend lifestyle changes to manage some symptoms.
Medication for autonomic disorders
Doctors may prescribe different medications to manage the symptoms of autonomic disorders. Some symptoms may improve when an underlying cause, such as dehydration, is treated.
Blood pressure medication
Physicians typically prescribe medications to regulate blood pressure, which is often too low when people who have autonomic disorders are standing. These medications are used to increase blood pressure and prevent complications, such as dizziness, fainting, or falls. Most blood pressure medications are taken on a long-term basis.
Doctors often prescribe a mineralocorticoid medication called a fludrocortisone to increase water and salt retention and raise blood pressure in people with autonomic disorders. This medication is typically taken once daily by mouth. Side effects include high blood pressure, headaches, swelling of the ankles, low potassium levels, and kidney function problems.
Other medications our doctors prescribe to manage symptoms of orthostatic hypotension include the alpha agonist midodrine and the synthetic amino acid droxidopa. Both medications are short-acting pressor agents, which means they raise blood pressure for two to six hours after they are taken. Side effects include high blood pressure while lying down.
Doctors advise people to take these medications only when they are upright and active—and to avoid lying down after they take them to avoid hypertension.
Parkinson’s disease medications
Your doctor may prescribe medications for Parkinson’s disease if you have Parkinson’s-like symptoms. A combination of two medications—levodopa and carbidopa—can be used to reduce symptoms such as stiffness, balance problems, and slow movement in people with autonomic disorders. These medications are taken daily by mouth. Side effects include nausea and vomiting.
People who use levodopa for long-term treatment may find that the benefits decrease about three to five years after starting the medication. A person may also experience involuntary movements, called dyskinesia, after taking high doses. To control these effects, a doctor may lessen the dose or adjust the timing of doses.
Autonomic nervous system disorders natural treatment
Doctors may recommend lifestyle changes to help people with certain types of autonomic disorders manage their symptoms—in particular, those who experience hypotension, or low blood pressure. If done properly, these measures can lead to a dramatic improvement even without medication.
For orthostatic hypotension
You may find relief by performing physical counter-maneuvers—such as making a fist, crossing your legs, or clenching your buttocks—that can increase standing blood pressure.
Staying adequately hydrated is crucial to avoid a decrease in blood pressure. People with orthostatic hypotension should drink six to eight eight-ounce glasses of water each day.
Adding salt to meals helps the body retain fluids, which is useful to avoid a drop in blood pressure.
Exercise is crucial to keep muscles active. In order to avoid low blood pressure when exercising, people may benefit from performing recumbent exercises such as riding a stationary bicycle, using elastic bands for resistance training, and rowing. One of the best kinds of exercise for people with orthostatic hypotension is doing exercises in a pool. This is because the pressure of the water around the body prevents the fall in blood pressure.
For postprandial hypotension
Drinking 12 to 18 ounces of water 15 minutes before eating and eating smaller meals throughout the day can reduce the chances of triggering postprandial hypotension.
Doctors also recommend eating fewer rapidly digested carbohydrates, such as white bread, white rice, potatoes, muffins, cookies, chocolate, bagels, and sugary beverages. Instead, consume slowly digested foods, such as whole grains, beans, and proteins, which can prevent blood pressure from falling after a meal.
Because blood pressure is usually lowest 30 to 60 minutes after a meal, it can be helpful to sit or lie down after eating. If you need to move around, watch for signs that your blood pressure is low, such as dizziness.
Avoid alcohol, which also contributes to low blood pressure.
For either cause of hypotension
People with both postprandial and orthostatic hypotension may benefit from wearing compression stockings: waist-high elastic garments that are similar to tights. By exerting pressure against the legs, compression stockings reduce the diameter of the veins and increase blood flow in the legs.
Compression stockings may help reduce dizziness, lightheadedness, and fainting. Knee- or thigh-high stockings are not as effective, and, therefore, our doctors don’t recommend them.
Some people find it useful to wear an abdominal binder, which is similar to a girdle. This helps to reduce blood pooling in the abdomen and improves blood pressure upon standing.
Sleeping with the head of the bed elevated in a semi-sitting position can lower blood pressure at night, helping to retain fluid in the body and improving symptoms of orthostatic hypotension in the morning.
Sleeping with the head of the bed raised can also reduce the number of times that you need to get up to urinate at night. There are bed wedge pillows and specially made blocks that can help.
Autonomic neuropathy
Autonomic neuropathy occurs when the nerves that control involuntary bodily functions are damaged. This may affect blood pressure, temperature control, digestion, bladder function and even sexual function.
The nerve damage interferes with the messages sent between the brain and other organs and areas of the autonomic nervous system, such as the heart, blood vessels and sweat glands.
While diabetes is generally the most common cause of autonomic neuropathy, other health conditions — even an infection — may be to blame. Some medications also may cause nerve damage. Symptoms and treatment will vary based on which nerves are damaged.
Autonomic neuropathy causes
Many health conditions can cause autonomic neuropathy. It may also be a side effect of treatments for other diseases, such as cancer. Some common causes of autonomic neuropathy include:
- Abnormal protein buildup in organs (amyloidosis), which affects the organs and the nervous system.
- Autoimmune diseases, in which your immune system attacks and damages parts of your body, including your nerves. Examples include Sjogren’s syndrome, systemic lupus erythematosus, rheumatoid arthritis and celiac disease. Guillain-Barre syndrome is an autoimmune disease that happens rapidly and can affect autonomic nerves. Autonomic neuropathy may also be caused by an abnormal attack by the immune system that occurs as a result of some cancers (paraneoplastic syndrome).
- Diabetes, which is the most common cause of autonomic neuropathy, can gradually cause nerve damage throughout the body.
- Injury to nerves caused by surgery or radiation to the neck.
- Treatment with certain medications, including some drugs used in cancer chemotherapy.
- Other chronic illnesses, such as Parkinson’s disease, multiple sclerosis and some types of dementia.
- Certain infectious diseases. Some viruses and bacteria, such as botulism, Lyme disease and HIV, can cause autonomic neuropathy.
- Inherited disorders. Certain hereditary disorders can cause autonomic neuropathy.
Risk factors for autonomic neuropathy
Factors that may increase your risk of autonomic neuropathy include:
- Diabetes. Diabetes, especially when poorly controlled, increases your risk of autonomic neuropathy and other nerve damage. You’re at greatest risk if you have had the disease for more than 25 years and have difficulty controlling your blood sugar, according to the National Institute of Diabetes and Digestive and Kidney Diseases. Additionally, people with diabetes who are overweight or have high blood pressure or high cholesterol have a higher risk of autonomic neuropathy.
- Other diseases. Amyloidosis, porphyria, hypothyroidism and cancer (usually due to side effects from treatment) may also increase the risk of autonomic neuropathy.
Autonomic neuropathy prevention
While certain inherited diseases that put you at risk of developing autonomic neuropathy can’t be prevented, you can slow the onset or progression of symptoms by taking good care of your health in general and managing your medical conditions.
Follow your doctor’s advice on healthy living to control diseases and conditions, which may include these recommendations:
- Control your blood sugar if you have diabetes.
- Seek treatment for alcoholism.
- Get appropriate treatment for any autoimmune disease.
- Take steps to prevent or control high blood pressure.
- Achieve and maintain a healthy weight.
- Stop smoking.
- Exercise regularly.
Autonomic neuropathy symptoms
Signs and symptoms of autonomic neuropathy vary based on the nerves affected. They may include:
- Dizziness and fainting when standing caused by a sudden drop in blood pressure.
- Urinary problems, such as difficulty starting urination, incontinence, difficulty sensing a full bladder and inability to completely empty the bladder, which can lead to urinary tract infections.
- Sexual difficulties, including problems achieving or maintaining an erection (erectile dysfunction) or ejaculation problems in men and vaginal dryness, low libido and difficulty reaching orgasm in women.
- Difficulty digesting food, such as feeling full after a few bites of food, loss of appetite, diarrhea, constipation, abdominal bloating, nausea, vomiting, difficulty swallowing and heartburn, all due to changes in digestive function.
- Sweating abnormalities, such as sweating too much or too little, which affects the ability to regulate body temperature.
- Sluggish pupil reaction, making it difficult to adjust from light to dark and seeing well when driving at night.
- Exercise intolerance, which may occur if your heart rate stays the same instead of adjusting in response to your activity level.
Autonomic neuropathy diagnosis
Autonomic neuropathy is a possible complication of a number of diseases, and the tests you’ll need often depend on your symptoms and risk factors for autonomic neuropathy.
When you have known risk factors for autonomic neuropathy
If you have conditions that increase your risk of autonomic neuropathy (such as diabetes) and have symptoms of the condition, extensive testing may not be necessary. Your doctor may perform a physical exam and ask about your symptoms.
If you are undergoing cancer treatment with a drug known to cause nerve damage, your doctor will check for signs of neuropathy.
When you don’t have risk factors for autonomic neuropathy
If you have symptoms of autonomic neuropathy but don’t have risk factors, the diagnosis may be more involved. Your doctor will probably review your medical history, discuss your symptoms and do a physical exam.
Your doctor may perform tests to evaluate autonomic functions, which may include:
- Breathing tests. These tests measure how your heart rate and blood pressure respond during exercises such as forcefully exhaling (Valsalva maneuver).
- Tilt-table test. This test monitors the response of blood pressure and heart rate to changes in posture and position, simulating what occurs when you stand up after lying down. You lie flat on a table, which is then tilted to raise the upper part of your body. Normally, your body narrows blood vessels and increases heart rate to compensate for the drop in blood pressure. This response may be slowed or abnormal if you have autonomic neuropathy. A simpler way test for this response involves standing for a minute, then squatting for a minute and then standing again while blood pressure and heart rate are monitored.
- Gastrointestinal tests. Gastric-emptying tests are the most common tests to check for digestive abnormalities such as slow digestion and delayed emptying of the stomach (gastroparesis). These tests are usually done by a doctor who specializes in digestive disorders (gastroenterologist).
- Quantitative sudomotor axon reflex test. This test evaluates how the nerves that regulate your sweat glands respond to stimulation. A small electrical current passes through four capsules placed on your forearm, foot and leg, while a computer analyzes the response of your nerves and sweat glands. You may feel warmth or a tingling sensation during the test.
- Thermoregulatory sweat test. During this test, you’re coated with a powder that changes color when you sweat. While lying in a chamber with slowly increasing temperature, digital photos document the results as you begin to sweat. Your sweat pattern may help confirm a diagnosis of autonomic neuropathy or suggest other causes for decreased or increased sweating.
- Urinalysis and bladder function (urodynamic) tests. If you have bladder or urinary symptoms, a series of urine tests can evaluate bladder function.
- Ultrasound. If you have bladder symptoms, your doctor may do an ultrasound in which high-frequency sound waves create an image of the bladder and other parts of the urinary tract.
Autonomic neuropathy treatment
Treatment of autonomic neuropathy includes:
- Treating the underlying disease. The first goal of treating autonomic neuropathy is to manage the disease or condition damaging your nerves. For example, if the underlying cause is diabetes, you’ll need to tightly control blood sugar to prevent autonomic neuropathy from progressing.
- Managing specific symptoms. Some treatments can relieve the symptoms of autonomic neuropathy. Treatment is based on what part of your body is most affected by nerve damage.
Digestive (gastrointestinal) symptoms
Your doctor may recommend:
- Modifying your diet. You may need to increase dietary fiber and fluids. Fiber supplements, such as Metamucil or Citrucel, also may help. Slowly increase fiber to avoid gas and bloating.
- Medication to help your stomach empty. A prescription drug called metoclopramide (Reglan) helps your stomach empty faster by increasing the contractions of the digestive tract. This medication may cause drowsiness, and its effectiveness wears off over time.
- Medications to ease constipation. Over-the-counter laxatives may help ease constipation. Ask your doctor how often you should use these medications. Increasing dietary fiber also may help relieve constipation.
- Medications to ease diarrhea. Antibiotics can help treat diarrhea by preventing excess bacterial growth in the intestines. Medications usually used to treat high blood pressure and cholesterol may also be prescribed for managing diarrhea.
- Antidepressants. Tricyclic antidepressants, such as imipramine (Tofranil), can help treat nerve-related abdominal pain. Dry mouth and urine retention are possible side effects of these medications.
Urinary symptoms
Your doctor may suggest:
- Retraining your bladder. Following a schedule of when to drink fluids and when to urinate can help increase your bladder’s capacity and retrain your bladder to empty completely at the appropriate times.
- Medication to help empty the bladder. Bethanechol is a medication that helps ensure complete emptying of the bladder. Possible side effects include headache, abdominal cramping, bloating, nausea and flushing.
- Urinary assistance (catheterization). During this procedure, a tube is guided through your urethra to empty your bladder.
- Medications that decrease overactive bladder. These include tolterodine (Detrol) or oxybutynin (Ditropan XL). Possible side effects include dry mouth, headache, fatigue, constipation and abdominal pain.
Sexual dysfunction
For men with erectile dysfunction, your doctor may recommend:
- Medications that enable erections. Drugs such as sildenafil (Viagra), vardenafil (Levitra) or tadalafil (Cialis) can help you achieve and maintain an erection. Possible side effects include mild headache, flushing, upset stomach and changes in color vision. If you have a history of heart disease, arrhythmia, stroke or high blood pressure, use these medications with caution and medical discretion. Also avoid taking these medications if you are taking any type of organic nitrates. Seek immediate medical assistance if you have an erection that lasts longer than four hours.
- An external vacuum pump. This device helps pull blood into the penis using a hand pump. A tension ring helps keep the blood in place, maintaining the erection for up to 30 minutes.
For women with sexual symptoms, your doctor may recommend:
- Vaginal lubricants. Vaginal lubricants may decrease dryness and make sexual intercourse more comfortable and enjoyable.
Heart rhythm and blood pressure symptoms
Autonomic neuropathy can cause a number of heart rate and blood pressure problems. Your doctor may prescribe:
- Medications that help raise your blood pressure. If you feel faint or dizzy when you stand up, your doctor may suggest a drug called fludrocortisone. This medication helps your body retain salt, which helps regulate your blood pressure. Other drugs that can help raise your blood pressure include midodrine and pyridostigmine (Mestinon). Midodrine may cause high blood pressure when lying down.
- Medication that helps regulate your heart rate. A class of medications called beta blockers helps to regulate your heart rate if it goes too high with an activity level.
- A high-salt, high-fluid diet. If your blood pressure drops when you stand up, a high-salt, high fluid diet may help maintain your blood pressure. This is generally only recommended for very severe cases of blood pressure problems, as this treatment may cause blood pressure that is too high or swelling of the feet, ankles or legs.
Sweating
If you experience excessive sweating, your doctor may prescribe:
- A medication that decreases perspiration. The drug glycopyrrolate (Robinul, Robinul Forte) can decrease sweating. Side effects may include diarrhea, dry mouth, urinary retention, blurred vision, changes in heart rate, headaches, loss of taste and drowsiness. Glycopyrrolate may also increase the risk of heat-related illness (such as heatstroke) from a reduced ability to sweat.
Home remedies
- Posture changes. Stand up slowly, in stages, to decrease dizziness. Sit with your legs dangling over the side of the bed for a few minutes before getting out of bed. Flex your feet and grip your hands for a few seconds before standing up, to increase blood flow. Once standing, try tensing your leg muscles while crossing one leg over the other a few times to increase blood pressure.
- Elevate the bed. If you have low blood pressure, it may also help to raise the head of your bed by about 4 inches by placing blocks or risers under the legs at the head of the bed.
- Digestion. Eat small, frequent meals to combat digestive problems. Increase fluids, and opt for low-fat, high-fiber foods, which may improve digestion. You may also want to try restricting foods that contain lactose and gluten.
- Diabetes management. Try to keep your blood sugar as close to normal as possible. Tight blood sugar control can help lessen symptoms and help to prevent or delay the onset of new problems.
Alternative medicine
Several alternative medicine treatments may help people with autonomic neuropathy. Remember to discuss any new treatments with your doctor to ensure that they won’t interfere with treatments you’re already receiving or cause you any harm.
Alpha-lipoic acid
Preliminary research suggests this antioxidant may be helpful in slowing or even reversing neuropathy that’s causing blood pressure or heart rate problems, but more study is needed.
Acupuncture
This therapy, which uses numerous thin needles placed in specific points in the body, may help treat slow stomach emptying. More studies are needed to confirm what acupuncture’s role is in treating autonomic neuropathy.
Electrical nerve stimulation
Some studies have found that this therapy, which uses low-energy electrical waves transmitted through electrodes placed on the skin, may help ease pain associated with diabetic neuropathy.
Coping and support
Living with a chronic condition presents daily challenges. Some of these suggestions may make it easier for you to cope:
- Set priorities. Accomplish the most important tasks, such as paying bills or grocery shopping, and save less important tasks for another day. Stay active, but don’t overdo it.
- Seek and accept help from friends and family. Having a support system and a positive attitude can help you cope with the challenges you face. Ask for or accept help when you need it. Don’t shut yourself off from loved ones.
- Talk to a counselor or therapist. Depression and impotence are possible complications of autonomic neuropathy. Seek help from a counselor or therapist in addition to your primary care doctor to discuss possible treatments.
- Consider joining a support group. Ask your doctor about support groups in your area. If there isn’t a specific group for people with neuropathies, you may find that there’s a support group for your underlying condition, such as diabetes. Some people find it helpful to talk to other people who truly understand what they’re going through. Support group members can offer camaraderie, as well as tips or tricks to make living with autonomic neuropathy easier.
Autonomic nervous system dysfunction
Autonomic nervous system dysfunction also called dysautonomia refers to a disorder of autonomic nervous system function that generally involves failure of the sympathetic or parasympathetic components of the autonomic nervous system, but dysautonomia involving excessive or overactive autonomic nervous system actions also can occur. Dysautonomia can be local, as in reflex sympathetic dystrophy, or generalized, as in pure autonomic failure. It can be acute and reversible, as in Guillain-Barre syndrome, or chronic and progressive. Several common conditions such as diabetes and alcoholism can include dysautonomia. Dysautonomia also can occur as a primary condition such as postural orthostatic tachycardia syndrome (POTS), vasovagal syncope, pure autonomic failure, neurocardiogenic syncope, neurally mediated hypertension, orthostatic hypotension, orthostatic hypertension, autonomic instability, paroxysmal sympathetic hyperactivity and cerebral salt wasting syndrome 1 or in association with degenerative neurological diseases such as Parkinson’s disease. Other diseases with generalized, primary dysautonomia include multiple system atrophy and familial dysautonomia. Hallmarks of generalized dysautonomia due to sympathetic failure are impotence (in men) and a fall in blood pressure during standing (orthostatic hypotension). Excessive sympathetic activity can present as hypertension or a rapid pulse rate (inappropriate sinus tachycardia).
Autonomic nervous system dysfunction treatment
There is usually no cure for dysautonomia. Secondary forms may improve with treatment of the underlying disease. In many cases treatment of primary dysautonomia is symptomatic and supportive. Measures to combat orthostatic hypotension include elevation of the head of the bed, water bolus (rapid infusion of water given intravenously), a high-salt diet, and drugs such as fludrocortisone and midodrine.
Autonomic nervous system dysfunction prognosis
The outlook for individuals with dysautonomia depends on the particular diagnostic category. People with chronic, progressive, generalized dysautonomia in the setting of central nervous system degeneration have a generally poor long-term prognosis. Death can occur from pneumonia, acute respiratory failure, or sudden cardiopulmonary arrest.
References




{kind=link}