
Benzodiazepine withdrawal syndrome
Benzodiazepines withdrawal symptoms may include:
- headaches
- aching or twitching muscles
- dizziness and tremors
- nausea, vomiting and stomach pains
- bizarre dreams, difficulty sleeping and fatigue
- poor concentration
- anxiety and irritability
- altered perception and heightening of senses
- delusions, hallucinations and paranoia
- seizures.
Common physical symptoms of benzodiazepines withdrawal:
- Stiffness
- Weakness
- Stomach problems
- Flu-like symptoms
- Visual problems
Common psychological symptoms of benzodiazepines withdrawal:
- Anxiety
- Insomnia
- Nightmares
- Depersonalization (the persistent feeling of observing oneself from outside one’s body or having a sense that one’s surroundings aren’t real)
- Problems with memory and concentration
- Depression
- Hallucinations. This is when you see, her, smell or feel things that are not there.
- Delusions. This is where you have beliefs that don’t match reality.
Benzodiazepine withdrawal is possible for most people on longer term benzodiazepines, although the process of reduction may be difficult and lengthy 4. Up to 15% of people who experience benzo withdrawal will go on to have protracted symptoms lasting months to years 7. Benzodiazepine withdrawal syndrome can happen if you have been taking benzodiazepine regularly for 4-6 weeks. Benzodiazepine withdrawal symptoms vary from person to person and are different depending on the type of benzodiazepine being taken. The benzodiazepine withdrawal symptoms can last from a few weeks to a year. Talk to your doctor about stopping if you have been taking benzodiazepine regularly for more than 4-6 weeks. They will be able to help you stop taking benzodiazepine. Abruptly discontinuing benzodiazepine after you have been taking it daily for more than one month is potentially dangerous; withdrawal can be severe or even life-threatening 8. It is safer to reduce your benzodiazepine slowly with your doctor’s support and with specialist support where needed. This is because your body will be used to the benzodiazepine and you might experience withdrawal symptoms. It is recommended to withdraw from benzodiazepines slowly, over a period of months, under medical supervision. Benzodiazepine reduction requires a team approach with regular communication between the prescriber and other practitioners involved in the patient’s care (e.g., pharmacist, counsellor, psychiatrist, addiction services).
The clearest strategy for withdrawing benzodiazepines is to taper the medication (Figure 2) 6. Benzodiazepine withdrawal strategies should be individualized, considering factors such as lifestyle, personality, environmental stressors, reasons for taking benzodiazepine, the type of dependence (therapeutic dose, prescribed high dose, recreational high dose or polydrug) and amount of available personal and clinical support. Because anticipatory anxiety is often related to benzo withdrawal syndrome, benzodiazepines are commonly tapered slowly, with psychological support emphasized during the process to help patients learn alternative coping skills 6. A common first step in benzo withdrawal is to substitute diazepam for the benzodiazepine being taken 6. Switching to a longer-acting benzodiazepine equivalent may allow for a smoother taper experience 6. The slower elimination of diazepam creates a smoother taper in blood level 9.
Two-thirds of patients can achieve benzodiazepine cessation with gradual reduction of dose alone. Others need additional psychological therapies and a limited number of patients benefit from additional pharmacotherapy 10. Cognitive behavioral therapy (CBT) performed in a single, extended (20-minute) consultation with a doctor, with a handout, has been shown to increase non-use at 1 year from 15% to 45% 11. A systematic review comparing routine care to brief interventions, gradual dose reduction and psychological interventions found all interventions increased benzodiazepine discontinuation over routine care, with gradual dose reduction plus psychological interventions the most effective 10.
Figure 1. Benzodiazepine withdrawal syndrome symptoms
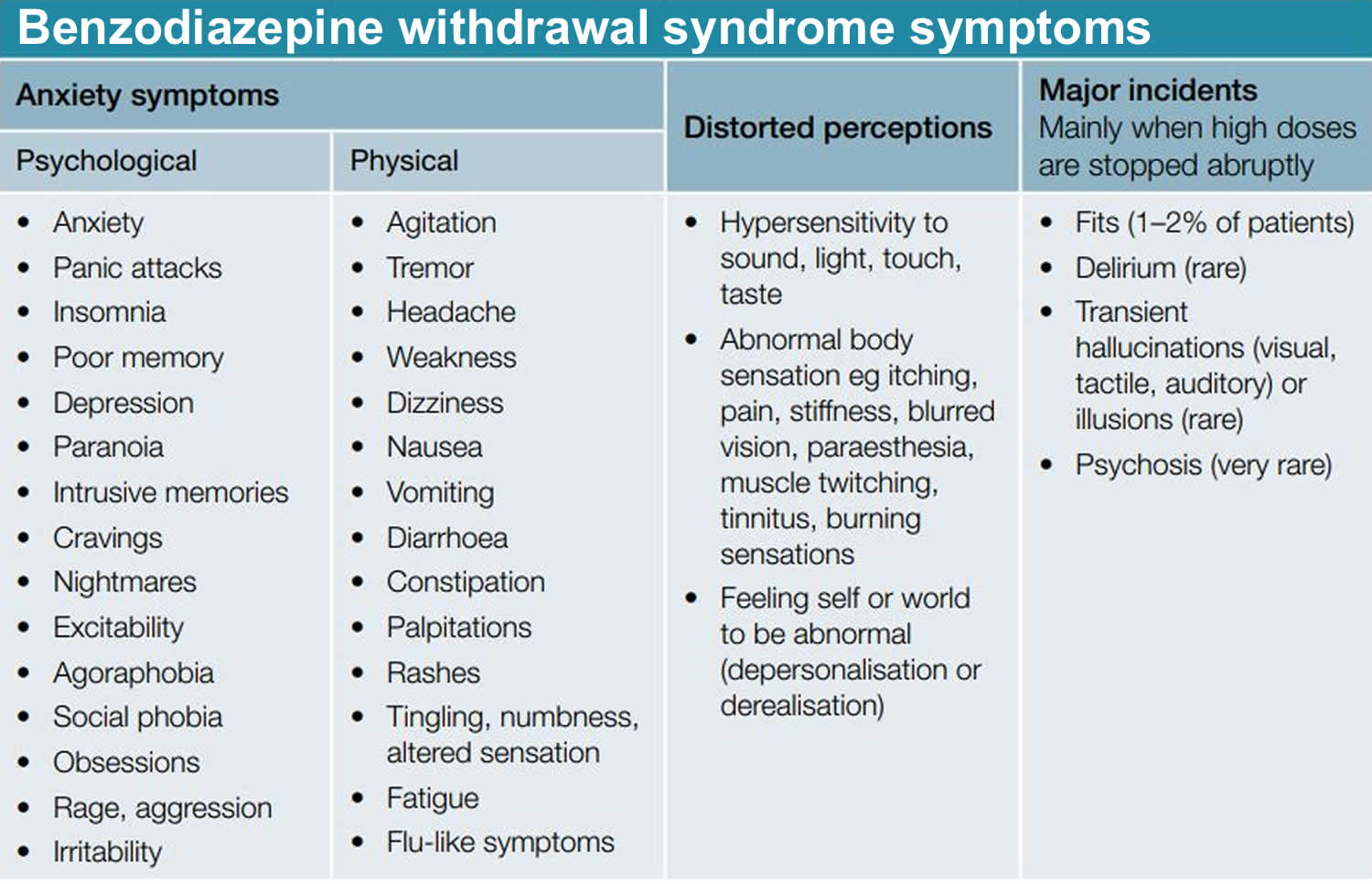
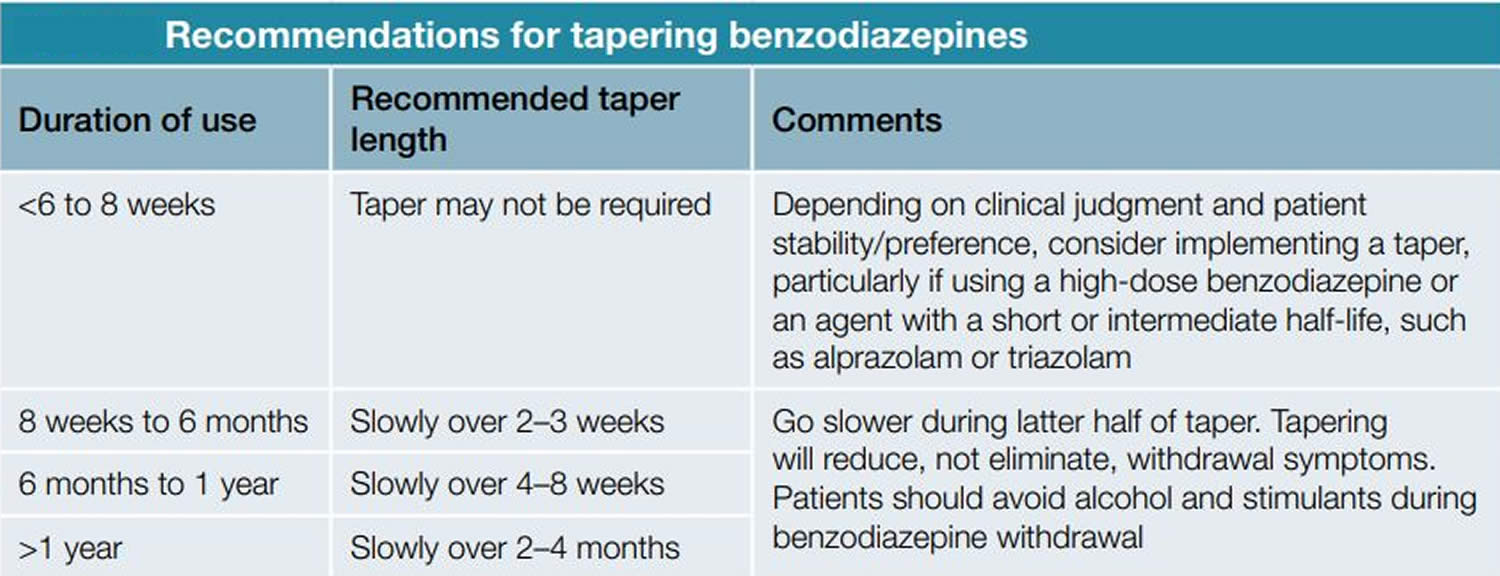
Figure 2. Recommendations for tapering benzodiazepines
When will benzodiazepine withdrawal syndrome stop?
Your benzodiazepine withdrawal syndrome will usually stop after a few weeks. But they can last longer for a small amount of people. You may not get benzodiazepines withdrawal symptoms when you stop your benzodiazepine medication. You should talk to your doctor or local pharmacist if you are worried about the withdrawal effects of benzodiazepines.
Is there anything that can help with my symptoms through benzodiazepine withdrawal?
Antidepressant and mood stabilizing drugs may help with the withdrawal effects of benzodiazepines.
If you have insomnia you may benefit from treatment with melatonin. Melatonin may help benzodiazepine reduction in older people with insomnia 4.
If you have a panic disorder you may benefit from cognitive behavioral therapy (CBT) whilst you are coming off the medication.
Should every patient be withdrawn from benzodiazepine?
There may be a small number of patients whose quality of life improves with the stable use of benzodiazepines 4. This may justify long-term benzodiazepine therapy. The decision to continue long-term benzodiazepine treatment needs to be clearly documented 4. The decision may also involve a second opinion by a specialist in an area relevant to the patient’s needs 4. These patients still require regular, ongoing review and re-assessment of the risks and benefits of benzodiazepine use 4.
Attempts at benzodiazepine withdrawal are more likely to succeed if the patient is able to contemplate the ultimate goal of cessation, and the doctor and patient are able to work together in a productive therapeutic relationship to achieve this.
Some patients struggle to reduce and cease benzodiazepine use. However, this group can often reduce their daily dose markedly and this is accompanied by a decrease in risk and side effects 4. They may continue on low-dose benzodiazepines (e.g., 2 to 5 mg diazepam daily) for an extended period 4. Continued regular review may assist in the majority of patients who will successfully cease benzodiazepines in the longer term 4. This decision should be made on a case-by-case basis 4.
For patients who have complex, multiple morbidities, doctors should seek advice from mental health and addiction specialists, as well as other relevant specialists (eg neurologists) to assist with development of the best plan to assist the patient 4.
What are benzodiazepines?
Benzodiazepines are drugs that belong to the group of medicines called central nervous system (CNS) depressants or sedatives, which are medicines that slows down messages traveling between your brain and your body. Other central nervous system (CNS) depressants include alcohol, cannabis and heroin. The central nervous system (brain and spinal cord) effects of benzodiazepines are believed to be mediated by activation of gamma aminobutyric acid (GABA) A receptors and modulation of their inhibition of neurotransmission 12. Because benzodiazepines are controlled substances with abuse potential, they are available only with your doctor’s prescription with special attention directed toward the patient’s addiction history before these agents are prescribed.
Benzodiazepines are also minor tranquilizers, usually prescribed by doctors to relieve stress and anxiety and to help people sleep. Benzodiazepines can also be used to treat alcohol withdrawal symptoms and epilepsy. However, medical professionals have become concerned about their risks, particularly when they are used for a long time.
Benzodiazepines may be prescribed to:
- treat the symptoms of anxiety disorders
- relieve insomnia
- help with treatment of symptoms experienced by cancer patients
- control epilepsy
- help relax muscles during certain medical procedures (such as endoscopy)
- treat alcohol withdrawal.
Benzodiazepines are relatively safe and, with overdose, rarely result in death. However, used chronically, benzodiazepines can be addicting. These agents are often taken in combination with other drugs of abuse by patients with addiction disorders. Some people misuse benzodiazepines to get high or to help with the ‘come down’ effects of stimulants such as amphetamines or cocaine.
Benzodiazepines can cause a person to overdose, particularly when used with alcohol or other drugs. Benzodiazepines are associated with dependence and withdrawal symptoms, even after a short period of use which is why benzodiazepines are not the first option for pharmacological treatment of insomnia (difficulty falling asleep or staying asleep), anxiety or other health concerns 13.
Benzodiazepines are known by their chemical (generic) name or their brand name. In each case the drug is the same – it’s just made by a different company. Some common benzodiazepines are:
Table 1. Benzodiazepines pharmaceutical names
| Generic name | Brand name | Type |
|---|---|---|
| Diazepam | Ducene®, Valium® | Long-acting |
| Oxazepam | Alepam®, Murelax®, Serepax® | Short-acting |
| Nitrazepam | Alodorm®, Mogadon® | Intermediate-acting |
| Temazepam | Euhypnos®, Normison® | Short-acting |
| Alprazolam | Xanax®, Kalma®, Alprax® | Short-acting |
More than a dozen benzodiazepines are available by prescription. The following is a list of benzodiazepines in current use, with their initial brand name and year of approval: alprazolam (Xanax, 1981), chlordiazepoxide (Librium, 1960), clonazepam (Klonopin, 1997), clorazepate (Tranxene, 1972), diazepam (Valium, 1963), estazolam (ProSom, 1990), flurazepam (Dalmane, 1970), lorazepam (Ativan, 1977), midazolam (Versed, 1985), oxazepam (Serax, 1965), quazepam (Doral, 1985), temazepam (Restoril, 1981), triazolam (Halcion, 1982), and most recently clobazam (2011).
Benzodiazepines all share similar activity and clinical effects, but variability in dosing, pharmacokinetics, rapidity of uptake and half-life make them more suited for one or another of these indications. Thus, estazolam, flurazepam, quazepam, temazepam and triazolam are generally used as sleeping pills, whereas alprazolam, chlordiazepoxide, diazepam, and lorazepam are used largely for the treatment of anxiety. Clobazam, clonazepam, and clorazepate are used as anticonvulsants, and high dose, parenteral diazepam and lorazepam are used for status epilepticus. Parenteral midazolam, diazepam and lorazepam are also used as anesthetics or anesthetic premedications. Alprazolam (Xanax), clonazepam (Klonopin), diazepam (Valium) and lorazepam (Ativan) are listed among the top 100 most commonly prescribed medications in United States 14. According to the American Psychiatric Association report on benzodiazepines, 11 to 15 percent of the adult population has taken a benzodiazepine one or more times during the preceding year, but only 1 to 2 percent have taken benzodiazepines daily for 12 months or longer 15. In psychiatric treatment settings and in substance-abuse populations, however, the prevalence of benzodiazepine use, abuse and dependence is substantially higher than that in the general population 16.
Types of benzodiazepines
There are three types of benzodiazepines: long, intermediate and short-acting. Short-acting benzodiazepines have stronger withdrawal or ‘come down’ effects and can be more addictive than long-acting ones 17.
- Benzodiazepines used as sleeping pills (hypnotics) are shorter acting. They are mostly used for treating sleep problems such as insomnia.
- Benzodiazepines used to treat anxiety (anxiolytics) are longer lasting. They are mostly used for treating anxiety.
Table 2. Benzodiazepines used as sleeping pills (hypnotics)
| Hypnotic Benzodiazepines | ||
| Medicine name | Trade name | Use to treat |
| Flurazepam | Dalmane | Sleep problems |
| Loprazolam | Sleep problems | |
| Lormetazepam | Sleep problems | |
| Nitrazepam | Mogadon | Sleep problems |
| Temazapam | Sleep problems | |
Table 3. Benzodiazepines used to treat anxiety (anxiolytics)
| Anxiolytic Benzodiazepines | ||
| Medicine name | Trade name | Use to treat |
| Alprazolam | Anxiety disorders | |
| Chlordiazepoxide Hydrochloride | Anxiety disorders, alcohol withdrawal | |
| Diazepam | Rimapan | Anxiety disorders, Anxiety with sleep problems, alcohol withdrawal, muscle spasms |
| Lorazepam | Ativan | Anxiety disorders |
| Oxazepam | Anxiety disorders | |
| Clobazam | Tapclob | Anxiety disorder |
High-potency benzodiazepines
- Drugs with a short half-life
- Alprazolam (Xanax)
- Lorazepam (Ativan)
- Triazolam (Halcion)
- Drugs with a long half-life
- Clonazepam (Klonopin)
Low-potency benzodiazepines
- Drugs with a short half-life
- Oxazepam (Serax)
- Temazepam (Restoril)
- Drugs with a long half-life
- Chlordiazepoxide (Librium)
- Clorazepate (Tranxene)
- Diazepam (Valium)
- Flurazepam (Dalmane)
How do benzodiazepines work?
Benzodiazepines are central nervous system depressants and they all increase activity at receptors for the neurotransmitter gamma-aminobutyric acid (GABA). The inhibitory neurotransmitter gamma-aminobutyric acid (GABA) inhibits the activity of neurons, slowing down the workings of your brain and nervous system. Benzodiazepines enhance the affinity of the recognition site for GABA by inducing conformational changes that make GABA binding more efficacious. Activation of the benzodiazepine-GABA-chloride ionophor complex is responsible for producing the therapeutic anxiolytic effects of benzodiazepines and for mediating many of the side effects and, possibly, dependence and withdrawal from these drugs 18.
Similarly, other sites for drug and neurotransmitter binding are associated with the GABA receptor complex, which serves as a primary site of action of benzodiazepines, barbiturates and other sedative-hypnotics, such as alcohol 18. Benzodiazepines and barbiturates act at separate binding sites on the receptor to potentiate the inhibitory action of GABA. They do so by allosterically altering the receptor (changing its conformation) so that it has a greater binding affinity for GABA. Ethanol modifies the receptor by altering the membrane environment so that it has increased affinity for GABA and the other sedative-hypnotic drugs. That benzodiazepines, barbiturates and ethanol all have related actions on a common receptor type, which explains their pharmacologic synergy and cross tolerance. Thus, benzodiazepines are used during alcohol detoxification.
With long-term high-dose use of benzodiazepines (or ethanol), there is an apparent decrease in the efficacy of GABA-A receptors, presumably a mechanism of tolerance 19. When high-dose benzodiazepines or ethanol are abruptly discontinued, this “down-regulated” state of inhibitory transmission is unmasked, leading to characteristic withdrawal symptoms such as anxiety, insomnia, autonomic hyperactivity and, possibly, seizures.
Benzodiazepines differ mainly in how quickly they are absorbed, how long their effects last, and how long they take to leave the body. Benzodiazepines only treat symptoms of anxiety or insomnia, and do not solve the underlying causes of these conditions.
The effects of benzodiazepines depend on the strength of the dose, the physical make-up of the person taking them and their state of mind.
Common effects of benzodiazepines include:
- relief from anxiety
- muscle relaxation
- sleepiness
- a sense of being disconnected or detached from reality
- dizziness
- loss of inhibitions.
Benzodiazepines can be highly addictive, whether they are taken under medical supervision or used recreationally.
Benzodiazepines uses
Benzodiazepines are central nervous system (CNS) depressants that are commonly prescribed in medicine to treat anxiety, stress, panic disorders, insomnia, alcohol withdrawal symptoms, muscle relaxation, epilepsy and to sedate people before certain medical procedures. It is generally recommended that benzodiazepines only be used for a short term – just days or weeks at a time.
Benzodiazepines clinical uses 20
- Anxiety disorders
- Acute anxiety
- Generalized anxiety disorder
- Panic disorder
- Phobias (social, simple)
- Post-traumatic stress disorder (PTSD)
- Obsessive-compulsive disorder (OCD)
- Insomnia
- Anxiety associated with medical illness
- Cardiovascular
- Gastrointestinal
- Somatoform disorder
- Convulsive disorders
- Acute status epilepticus
- Neonatal seizures or febrile convulsions
- Preeclampsia
- Tetanus
- Adjunct to other anticonvulsants
- Amnestic (before surgery or procedure)
- Spastic disorders and other types of acute muscle spasm
- Cerebral palsy
- Multiple sclerosis (MS)
- Paraplegia secondary to spinal trauma
- Involuntary movement disorders
- Restless leg syndrome
- Akathisia associated with neuroleptic use
- Choreiform disorders
- Myoclonus
- Detoxification from alcohol and other substances
- Agitation or anxiety associated with other psychiatric conditions
- Acute mania
- Psychotic illness
- Anxiety associated with depression
- Impulse control disorders
- Catatonia or mutism
- Other adjunctive uses
- Surgery
- Dentistry
- Diagnostic studies, such as computed tomography, magnetic resonance imaging and endoscopy
- Cardioversion
- Chemotherapy
Severe anxiety
You may be given benzodiazepines for the short-term relief of severe anxiety. You should not be given them for long term relief.
Panic disorders
You may be given benzodiazepines:
- When you first start taking antidepressants, OR
- if you don’t respond to antidepressants.
Insomnia
Benzodiazepines can be used to treat insomnia. Insomnia means that you find it difficult to fall asleep or stay asleep.
You should only be offered benzodiazepines to treat insomnia if it is severe, disabling or is causing you a lot of distress.
Benzodiazepines should only be offered for short term use.
Acute alcohol withdrawal
Long acting benzodiazepines are used to help with the effects of acute alcohol withdrawal.
You should stay in hospital during alcohol withdrawal if you have severe alcohol dependence. Alcohol withdrawal without medical support can cause dangerous side effects such as seizures.
Recreational use of benzodiazepines
Some people take benzodiazepines illegally for recreational use. They may use them to feel a sense of euphoria (or high) or mix them with other drugs such as stimulants (cocaine, amphetamines, ecstasy) to ‘come down’. Benzodiazepines can be dangerous when mixed with other drugs (including alcohol) and can put you at risk of overdose or harm.
Some people may give them to others intentionally or without their consent (such as spiking their drink).
Benzodiazepine withdrawal syndrome symptoms
Benzodiazepine withdrawal syndrome symptoms are highly variable, mostly impacted by the level of dose reduction. Other contributing factors can include a history of polydrug dependence, seizures, anxiety, depression or trauma, or when the total daily dose is not clear due to doctor shopping or illegal purchase. Each patient will need tailored withdrawal management plan that will also address any underlying problems and contributing factors. Benzodiazepine withdrawal syndrome symptoms may appear in 1 to 2 days for agents with shorter half-lives, but may not appear until 3 to 7 days for agents with longer half-lives 4.
Benzodiazepines withdrawal symptoms may include:
- headaches
- aching or twitching muscles
- dizziness and tremors
- nausea, vomiting and stomach pains
- bizarre dreams, difficulty sleeping and fatigue
- poor concentration
- anxiety and irritability
- altered perception and heightening of senses
- delusions, hallucinations and paranoia
- seizures.
Common physical symptoms of benzodiazepines withdrawal:
- Stiffness
- Weakness
- Stomach problems
- Flu-like symptoms
- Visual problems
Common psychological symptoms of benzodiazepines withdrawal:
- Anxiety
- Insomnia
- Nightmares
- Depersonalization (the persistent feeling of observing oneself from outside one’s body or having a sense that one’s surroundings aren’t real)
- Problems with memory and concentration
- Depression
- Hallucinations. This is when you see, her, smell or feel things that are not there.
- Delusions. This is where you have beliefs that don’t match reality.
Protracted benzodiazepine withdrawal symptoms may include 21:
- Anxiety
- Depression
- Diarrhea, constipation, bloating
- Insomnia
- Irritability
- Muscle aches
- Poor concentration and memory
- Restlessness
- Less commonly, perceptual disturbances and panic attacks
- Occasionally, seizures and symptoms of psychosis.
These protracted benzodiazepine withdrawal symptoms do not occur in all benzodiazepine patients 22, but have a reported incidence between 15% and 44% among those taking benzodiazepines on a regular rather than an as-needed (PRN) basis 23.
Benzodiazepine withdrawal syndrome treatment
Evidence-based recommendations for general management of benzodiazepine withdrawal are difficult due to a lack of clinical data 4. The following are general principles for managing benzodiazepine withdrawal syndrome 24, 25, 7:
- Review the patients’ prescription records and discuss the situation to those receiving long-term benzodiazepines.
- Send patients letters suggesting methods of tapering off benzodiazepines (this may be enough to motivate them to withdraw).
- Teach patients ways to deal with anxiety and insomnia (either as primary conditions or due to withdrawal).
- Acknowledge that withdrawing from benzodiazepines can be stressful.
- Encourage family and friends to provide encouragement and practical help during withdrawal.
- Refer patients to appropriate services (eg psychologist or support groups). Only refer to drug or alcohol dependence services if the service has shown specific interest in benzodiazepine
- dependence or the patient also has a drug or alcohol problem.
- Advise patients to make changes in lifestyle such as regular exercise.
- Advise patients to avoid alcohol.
- Advise patients to avoid mild stimulants (eg coffee and chocolate [theobromine]) as these can cause anxiety, panic and insomnia.
- Postpone advice on smoking cessation until after the benzodiazepine has been withdrawn 6
Benzodiazepine reduction requires a team approach with regular communication between the prescriber and other practitioners involved in the patient’s care (eg pharmacist, counsellor, psychiatrist, addiction services).
The clearest strategy for withdrawing benzodiazepines is to taper the medication (see Figure 2) 6. There are three basic approaches to taper a benzodiazepine 8, 5:
- Use the same medication for tapering;
- Switch to a longer-acting equivalent; and
- Use add-on medications to help reduce potential withdrawal symptoms.
Slow discontinuation of benzodiazepines is recommended to avoid withdrawal symptoms (e.g., rebound anxiety, agitation, insomnia or seizures) particularly when use exceeds 8 weeks 4. However, clear evidence for the optimal rate of tapering is lacking. The dosage reduction mainly depends on the starting dose and whether the patient is tapering as an inpatient or outpatient. For safety reasons, outpatient tapers usually need to be slower than inpatient tapers. Patients taking higher dosages of benzodiazepines can usually tolerate larger reductions than those taking lower dosages 6, 26. The initial reduction typically ranges between 5% and 25% of the starting dose, with further reductions of 5% to 25% every one to four weeks as tolerated. The British National Formulary recommends a minimum of 6 weeks 27, while Lader recommends a maximum of 6 months 6. The exact rate of benzodiazepine reduction should be individualized according to the drug, dose and duration of treatment. A common first step in benzo withdrawal is to substitute diazepam for the benzodiazepine being taken 6. Switching to a longer-acting benzodiazepine equivalent may allow for a smoother taper experience 6. The slower elimination of diazepam creates a smoother taper in blood level 9. A suggested benzodiazepine taper schedule is available at https://www.va.gov/PAINMANAGEMENT/docs/OSI_6_Toolkit_Taper_Benzodiazepines_Clinicians.pdf
Supratherapeutic doses can initially be reduced by 25% to 30%, then further reduced by 5% to 10% daily, weekly, or monthly as appropriate, based on how well the patient tolerates withdrawal symptoms during the taper. Addition of an anticonvulsant (e.g., gabapentin [Neurontin]) should be considered for high-dosage withdrawal. Studies have shown that add-on medications, such as carbamazepine (Tegretol), imipramine, divalproex (Depakote), and trazodone, can mitigate some of the withdrawal discomfort 6. Use of antidepressants, such as duloxetine (Cymbalta) or amitriptyline, may help patients with chronic pain. There is limited evidence that antidepressants help in benzodiazepine withdrawal, unless depression (or anxiety disorders/panic disorders) are present or emerge during withdrawal 10.
For complex cases, stabilizing the dose at a 50% reduction for several months before resuming the taper may improve tolerability 28. At the end of the taper, some patients may need to reduce the pace with nearly homeopathic dosage reductions to tolerate the withdrawal. Compounding pharmacies can be used to obtain very small doses near the end of the taper.
All patients on a tapering regime must obtain prescriptions from one prescriber and through one pharmacy, where time-limited dispensing may be required (e.g., once or twice a week at a specified time) 4. Plans should be in place to cover absences of the usual prescribing doctor from the practice 4. Consider working closely with the patient’s pharmacist with staged supply or supervised dosing to assist the patient with dose reduction and cessation, if they are unable to manage this themselves 4.
Other considerations
Patients with benzodiazepine use disorder will have more difficulty reducing or stopping the dosage because of cravings. They may report intolerable withdrawal symptoms, request early refills, use benzodiazepines for reasons other than why they were prescribed, or report a need for benzodiazepines to perform normal daily activities. These patients may not be able to taper off without more intensive follow-up and intervention. A taper may be a litmus test for addiction; these patients may benefit from a referral to an addiction specialist 26.
Patients taking ‘therapeutic benzodiazepine doses’
For people who have early or mild benzodiazepine dependence, minimal interventions such as advisory letters, other information provision or doctor advice should be offered. Where benzodiazepine dependence is established, gradual dose reduction of prescribed benzodiazepine is recommended 29.
Switching from a short half-life benzodiazepine to a long half-life benzodiazepine before gradual taper should be reserved for patients having problematic withdrawal symptoms on reduction 29.
Additional psychological therapies increase the effectiveness of gradual dose reduction, particularly in patients with insomnia and panic disorder. Consideration should be given to targeted use of these interventions 29.
Patient taking high doses of benzodiazepines or who are users of illicit drugs (polydrug users)
So called ‘harm-reduction dosing’ or maintenance prescribing of benzodiazepines for patients using polydrugs cannot be recommended on the basis of existing evidence, as prescribing benzodiazepines does not appear to prevent use of other drugs 29. There are some evidence that maintenance dosing of benzodiazepines may reduce high-dose problematic benzodiazepine use in some patients 29.
References- Baldwin DS, Aitchison K, Bateson A, Curran HV, Davies S, Leonard B, Nutt DJ, Stephens DN, Wilson S. Benzodiazepines: risks and benefits. A reconsideration. J Psychopharmacol. 2013 Nov;27(11):967-71. doi: 10.1177/0269881113503509
- Seldenrijk A, Vis R, Henstra M, Ho Pian K, van Grootheest D, Salomons T, Overmeire F, de Boer M, Scheers T, Doornebal-Bakker R, Ruhé HG, Vinkers CH. Aandacht voor bijwerkingen van benzodiazepinen is belangrijk: een systematisch overzicht [Systematic review of the side effects of benzodiazepines]. Ned Tijdschr Geneeskd. 2017;161:D1052. Dutch.
- Janhsen K, Roser P, Hoffmann K. The problems of long-term treatment with benzodiazepines and related substances. Dtsch Arztebl Int. 2015 Jan 5;112(1-2):1-7. doi: 10.3238/arztebl.2015.0001
- Discontinuing benzodiazepines. https://www.racgp.org.au/clinical-resources/clinical-guidelines/key-racgp-guidelines/view-all-racgp-guidelines/drugs-of-dependence/part-b/discontinuing-benzodiazepines
- Guidance for the use and reduction of misuse of benzodiazepines and other hypnotics and anxiolytics in general practice. https://www.addictionprofessionals.org.uk/Handlers/Download.ashx?IDMF=8f776bd7-8127-485f-8550-b93603ea275f
- Lader M, Tylee A, Donoghue J. Withdrawing benzodiazepines in primary care. CNS Drugs. 2009;23(1):19-34. doi: 10.2165/0023210-200923010-00002
- Ashton H. The diagnosis and management of benzodiazepine dependence. Curr Opin Psychiatry. 2005 May;18(3):249-55. doi: 10.1097/01.yco.0000165594.60434.84
- Tapering Patients Off of Benzodiazepines. Am Fam Physician. 2017 Nov 1;96(9):606-608. https://www.aafp.org/afp/2017/1101/p606.html
- Ministry of Health Singapore. Prescribing of Benzodiazepines: MOH Clinical Practice Guidelines 2/2008. Singapore: MOH; 2008.
- Parr JM, Kavanagh DJ, Cahill L, Mitchell G, McD Young R. Effectiveness of current treatment approaches for benzodiazepine discontinuation: a meta-analysis. Addiction. 2009 Jan;104(1):13-24. doi: 10.1111/j.1360-0443.2008.02364.x
- Vicens C, Bejarano F, Sempere E, Mateu C, Fiol F, Socias I, Aragonès E, Palop V, Beltran JL, Piñol JL, Lera G, Folch S, Mengual M, Basora J, Esteva M, Llobera J, Roca M, Gili M, Leiva A. Comparative efficacy of two interventions to discontinue long-term benzodiazepine use: cluster randomised controlled trial in primary care. Br J Psychiatry. 2014 Jun;204(6):471-9. doi: 10.1192/bjp.bp.113.134650
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Benzodiazepines. [Updated 2017 Jan 24]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548298
- Brands B, Sproule B & Marshman J. (eds) (1998) Drugs & Drug Abuse (3rd ed.) Ontario: Addiction Research Foundation.
- American Druggist. Top 200 drugs of 1995. New York, N.Y.: Hearst Corp, 1996:18–26.
- Salzman C, for Task Force on Benzodiazepine Dependency, American Psychiatric Association. Benzodiazepine dependence, toxicity, and abuse: a task force report of the American Psychiatric Association. Washington, D.C.: American Psychiatric Association, 1990.
- Busto UE, Romach MK, Sellers EM. Multiple drug use and psychiatric comorbidity in patients admitted to the hospital with severe benzodiazepine dependence. J Clin Psychopharmacol. 1996;16:51–7.
- Benzodiazepines drug profile. https://www.emcdda.europa.eu/publications/drug-profiles/benzodiazepines_en
- Arana GW, Hyman SE. Handbook of psychiatric drug therapy. 2d ed. Boston: Little, Brown, 1991: 128–61.
- Miller LG. Chronic benzodiazepine administration: from the patient to the gene. J Clin Pharmacol. 1991;31:492–5.
- Hollister L, Muller-Oerlinghausen B, Rickels K, Shader R. Clinical uses of benzodiazepines. J Clin Psychopharmacol 1993;13(suppl 1):1–169.
- Mental Health and Drug and Alcohol Office (MHDAO). NSW Drug and Alcohol Withdrawal Clinical Practice Guidelines. Sydney: MHDAO; 2008.
- Pergolizzi JV Jr, LeQuang JA, Raffa RB. Benzodiazepines: Thinking outside the black box. J Clin Pharm Ther. 2021 Jun;46(3):554-559. doi: 10.1111/jcpt.13333
- Lugoboni F, Quaglio G. Exploring the dark side of the moon: the treatment of benzodiazepine tolerance. Br J Clin Pharmacol. 2014 Feb;77(2):239-41. doi: 10.1111/bcp.12148
- Wright S. Benzodiazepine withdrawal: clinical aspects. In: Peppin J, Pergolizzi J, Raffa R, et al. (eds) The benzodizapeines crisis: the ramifications of an over-used drug class. New York: Oxford University Press, 2020, pp. 117–148.
- Horowitz MA, Taylor D. How to reduce and stop psychiatric medication. Eur Neuropsychopharmacol. 2022 Feb;55:4-7. https://doi.org/10.1016/j.euroneuro.2021.10.001
- Ashton H. The treatment of benzodiazepine dependence. Addiction. 1994;89(11):1535–1541.
- Joint National Formulary Committee. British National Formulary. London: British Medical Association and Royal Pharmaceutical Society of Great Britain; 2011.
- National Center for PTSD. Effective treatments for PTSD: helping patients taper from benzodiazepines. 2013. https://www.va.gov/PAINMANAGEMENT/docs/OSI_6_Toolkit_Taper_Benzodiazepines_Clinicians.pdf
- Lingford-Hughes AR, Welch S, Peters L, Nutt DJ; British Association for Psychopharmacology, Expert Reviewers Group. BAP updated guidelines: evidence-based guidelines for the pharmacological management of substance abuse, harmful use, addiction and comorbidity: recommendations from BAP. J Psychopharmacol. 2012 Jul;26(7):899-952. doi: 10.1177/0269881112444324





{kind=link}