Bloom syndrome
Bloom syndrome also called Bloom-Torre-Machacek syndrome or congenital telangiectatic erythema, is a rare autosomal recessive inherited disorder characterized by short stature, a skin rash that develops after exposure to the sun, and a greatly increased risk of all types of cancer 1. Bloom syndrome is due to mutations in the BLM gene inducing the formation of an abnormal DNA helicase protein. The most prominent features include growth deficiency of prenatal onset, mild immunodeficiency, excessive photosensitivity with facial lupus-like skin lesions, type 2 diabetes mellitus and hypogonadism. The increased risk of malignancy in Bloom syndrome leads to a shortened life expectancy and alters the quality of life of affected persons 2.
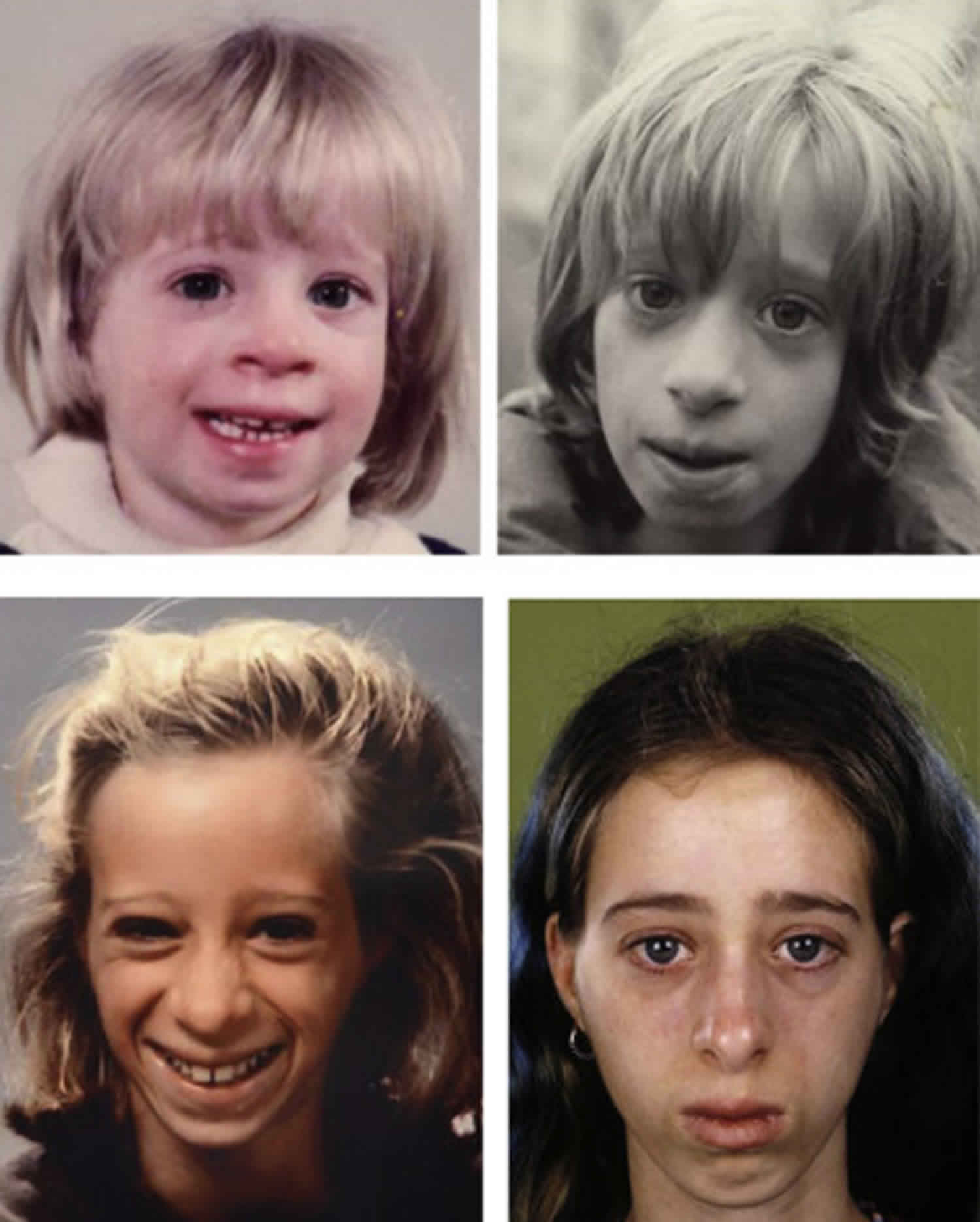
People with Bloom syndrome are usually smaller than 97 percent of the population in both height and weight from birth, and they rarely exceed 5 feet tall in adulthood.
Affected individuals have skin that is sensitive to sun exposure, and they usually develop a butterfly-shaped patch of reddened skin across the nose and cheeks. A skin rash can also appear on other areas that are typically exposed to the sun, such as the back of the hands and the forearms. Small clusters of enlarged blood vessels (telangiectases) often appear in the rash; telangiectases can also occur in the eyes. Other skin features include patches of skin that are lighter or darker than the surrounding areas (hypopigmentation or hyperpigmentation respectively). These patches appear on areas of the skin that are not exposed to the sun, and their development is not related to the rashes.
People with Bloom syndrome have an increased risk of cancer. They can develop any type of cancer, but the cancers arise earlier in life than they do in the general population, and affected individuals often develop more than one type of cancer.
Individuals with Bloom syndrome have a high-pitched voice and distinctive facial features including a long, narrow face; a small lower jaw; and prominent nose and ears. Other features can include learning disabilities, an increased risk of diabetes, chronic obstructive pulmonary disease (COPD), and mild immune system abnormalities leading to recurrent infections of the upper respiratory tract, ears, and lungs during infancy. Men with Bloom syndrome usually do not produce sperm and as a result are unable to father children (infertile). Women with the disorder generally have reduced fertility and experience menopause at an earlier age than usual.
Bloom syndrome is a rare disorder. Only a few hundred affected individuals have been described in the medical literature, about one-third of whom are of Central and Eastern European (Ashkenazi) Jewish background 3.
Treatment of manifestations: Skin protection, including coverage of exposed skin and use of broad-spectrum sunscreen with SPF of at least 30 to reduce the sun-sensitive rash. Increased-calorie-density formulas and foods may promote weight gain. Although growth hormone treatment may improve linear growth, many clinicians caution against its use because of reports of early onset of cancer in some treated children. Developmental services and therapies as needed. Hyperglycemia from insulin resistance is treated as in type 2 diabetes. In persons with Bloom syndrome who have cancer, reduced chemotherapy dosage and duration to reduce risks of severe complications; caution should be exercised with use of ionizing radiation or alkylating agents, particularly busulfan, cyclophosphamide, or melphalan. Individuals with recurrent infections and defects in humoral immunity may be treated with gamma globulin infusions to decrease frequency and severity of infections.
Surveillance: Abdominal ultrasound examination every three months until age eight years for Wilms tumor. Screening and family education regarding signs/symptoms of leukemia and lymphoma at every health visit. Whole-body MRI every one to two years beginning at age 12-13 years for risk of lymphoma. Annual colonoscopy beginning at age 10-12 years. Fecal immunochemical testing every six months beginning at age 10-12 years. Annual breast MRI in women beginning at age 18 years. Annual fasting blood glucose and hemoglobin A1C beginning at age ten years. Annual serum TSH with reflex to T4 beginning at age ten years. Annual lipid profile beginning at age ten years.
Agents and circumstances to avoid: Sun exposure may provoke an erythematous rash, especially on the face. Exposure to ionizing radiation should be minimized.
Is gene therapy available for the treatment of Bloom syndrome?
Gene therapy, a technique for treating disease by altering the patient’s genetic material, is not currently available for individuals with Bloom syndrome. In the United States, The Food and Drug Administration (FDA) has not yet approved any human gene therapy product for sale. Current gene therapy is experimental and has not proven very successful in clinical trials.[2]
ClinicalTrials.gov (https://clinicaltrials.gov/ct2/home) lists trials in the U.S and around the world that are studying the use of gene therapy for a variety of conditions. Although there may not be a trial specific to gene therapy for Bloom syndrome listed at this time, this site is updated regularly and may be checked periodically. To search for trials studying the use of gene therapy for Bloom syndrome, go here (https://clinicaltrials.gov/ct2/results?term=bloom+syndrome+gene+therapy).
I have Bloom syndrome and am I able to become pregnant?
According to the Bloom’s Syndrome Foundation, puberty in people with Bloom syndrome occurs at the usual age and sexual interests and activity are normal 4. This resource, along with others, indicate that women with Bloom syndrome may have reduced fertility, but several women have become pregnant 5. Eleven women with Bloom syndrome (followed through the the Bloom Syndrome Registry) have become pregnant at least once; seven of them have delivered a total of eleven healthy babies of normal size 5. It should be noted that the reproductive span may be shortened in women with Bloom syndrome because menopause tends to occur unusually early 5.
Bloom syndrome causes
Mutations in the BLM gene cause Bloom syndrome. The BLM gene provides instructions for making a member of a protein family called RecQ helicases. Helicases are enzymes that attach (bind) to DNA and unwind the two spiral strands (double helix) of the DNA molecule. This unwinding is necessary for several processes in the cell nucleus, including copying (replicating) DNA in preparation for cell division and repairing damaged DNA. Because RecQ helicases help maintain the structure and integrity of DNA, they are known as the “caretakers of the genome.”
When a cell prepares to divide to form two cells, the DNA that makes up the chromosomes is copied so that each new cell will have two copies of each chromosome, one from each parent. The copied DNA from each chromosome is arranged into two identical structures, called sister chromatids, which are attached to one another during the early stages of cell division. Sister chromatids occasionally exchange small sections of DNA during this time, a process known as sister chromatid exchange. Researchers suggest that these exchanges may be a response to DNA damage during the copying process. The BLM protein helps to prevent excess sister chromatid exchanges and is also involved in other processes that help maintain the stability of the DNA during the copying process.
BLM gene mutations result in the absence of functional BLM protein. As a result, the frequency of sister chromatid exchange is about 10 times higher than average. Exchange of DNA between chromosomes derived from the individual’s mother and father are also increased in people with BLM gene mutations. In addition, chromosome breakage occurs more frequently in affected individuals. All of these changes are associated with gaps and breaks in the genetic material that impair normal cell activities and cause the health problems associated with this condition. Without the BLM protein, the cell is less able to repair DNA damage caused by ultraviolet light, which results in increased sun sensitivity. Genetic changes that allow cells to divide in an uncontrolled way lead to the cancers that occur in people with Bloom syndrome.
Bloom syndrome is of special interest to geneticists because patients with this condition bear chromosomes that are highly unstable so that mutations are frequently encountered. In addition, the recombination of chromosomes of such patients occurs with much greater frequency and seemingly with much greater ease than normal. Most clinicians engaged in studies of Bloom syndrome consider the volatility of the chromosomes to be a major contributor to both short stature and a predisposition to cancer.
One of the types of chromosomal recombination that occurs in Bloom syndrome is known as sister-chromatid exchange (SCE). This means that portions of the chromosomal-DNA are exchanged among paired (sister) chromosomes. Bloom syndrome is the only known human genetic condition in which cells undergo high levels of SCE; and because these SCE’s can be viewed under the microscope, the presence of multiple SCE’s is a diagnostic indicator.
The protein (a RecQ helicase) controlled by the gene for Bloom syndrome is involved in cell repair, cell division, and cell death. Bloom syndrome is presumed to result from a defect of the cell’s DNA repair system. DNA may be damaged during the course of a cell’s life and must be repaired if the cell is to continue to function. If the damaged DNA is not repaired properly, the cells may die and be replaced by others; or in some cases the damaged cells may continue to grow in an abnormal fashion and result in cancer.
Bloom syndrome inheritance pattern
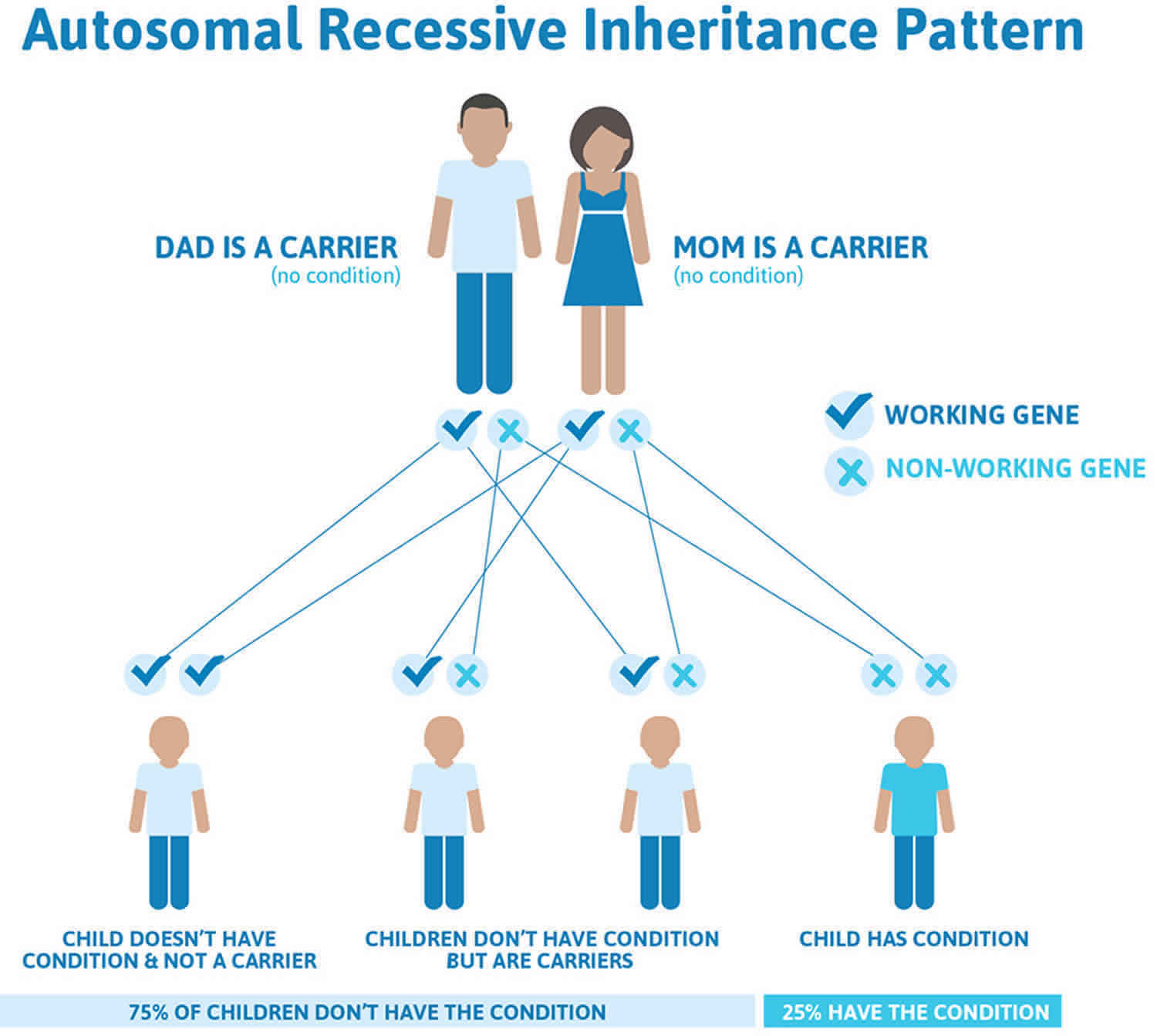
Bloom syndrome is inherited in an autosomal recessive pattern, which means both copies of the gene in each cell have mutations. The parents of an individual with an autosomal recessive condition each carry one copy of the mutated gene, but they typically do not show signs and symptoms of the condition.
It is rare to see any history of autosomal recessive conditions within a family because if someone is a carrier for one of these conditions, they would have to have a child with someone who is also a carrier for the same condition. Autosomal recessive conditions are individually pretty rare, so the chance that you and your partner are carriers for the same recessive genetic condition are likely low. Even if both partners are a carrier for the same condition, there is only a 25% chance that they will both pass down the non-working copy of the gene to the baby, thus causing a genetic condition. This chance is the same with each pregnancy, no matter how many children they have with or without the condition.
- If both partners are carriers of the same abnormal gene, they may pass on either their normal gene or their abnormal gene to their child. This occurs randomly.
- Each child of parents who both carry the same abnormal gene therefore has a 25% (1 in 4) chance of inheriting a abnormal gene from both parents and being affected by the condition.
- This also means that there is a 75% ( 3 in 4) chance that a child will not be affected by the condition. This chance remains the same in every pregnancy and is the same for boys or girls.
- There is also a 50% (2 in 4) chance that the child will inherit just one copy of the abnormal gene from a parent. If this happens, then they will be healthy carriers like their parents.
- Lastly, there is a 25% (1 in 4) chance that the child will inherit both normal copies of the gene. In this case the child will not have the condition, and will not be a carrier.
These possible outcomes occur randomly. The chance remains the same in every pregnancy and is the same for boys and girls.
Figure 1 illustrates autosomal recessive inheritance. The example below shows what happens when both dad and mum is a carrier of the abnormal gene, there is only a 25% chance that they will both pass down the abnormal gene to the baby, thus causing a genetic condition.
Figure 1. Bloom syndrome autosomal recessive inheritance pattern
People with specific questions about genetic risks or genetic testing for themselves or family members should speak with a genetics professional.
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://www.findageneticcounselor.com/) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://www.abgc.net/about-genetic-counseling/find-a-certified-counselor/) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counselors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (http://www.acmg.net/ACMG/Genetic_Services_Directory_Search.aspx) has a searchable database of medical genetics clinic services in the United States.
Bloom syndrome symptoms
Infants and adults with Bloom syndrome are short and underweight and have a small head circumference, but they have normal body proportions. Affected infants and children usually present with a distinctive, narrow, small head and face. Sometimes, these signs are accompanied by a reddish facial rash that is due to the dilation of very small blood vessels (telangiectasia) of the face. The rash typically appears in a “butterfly” pattern on the cheeks and across the nose. Areas of abnormal brown or gray skin coloration (cafe-au-lait spots) may occur on other parts of the body. The skin is highly sensitive to sunlight (photosensitive) and may become very red upon exposure, especially on the face.
At least 50% of people with this disorder eventually develop any one of a variety of malignancies, especially leukemia and cancers of the gastrointestinal tract such as the colon. About 10% of people who have Bloom syndrome will develop diabetes as well.
Male sterility is common because, for reasons that are not well understood, men with Bloom syndrome are unable to produce sperm. Female infertility is also common because menstruation ceases at an abnormally early age among women with Bloom syndrome.
Also, people with Bloom syndrome typically have abnormalities of the immune system that often result in an increased number of middle ear infections (otitis media) and/or pneumonia.
Many persons with Bloom syndrome have a characteristically high-pitched voice, dental abnormalities, prominent ears, cysts at the base of the spine (pilonidal), and/or extra fingers (polydactyly). Occasionally, other abnormalities of the eyes, ears, hands, and/or feet may also be present.
The range of clinical features in persons with Bloom syndrome (Bloom syndrome) has been tracked through the Bloom Syndrome Registry. The clinical and genetic histories have been obtained from registered persons diagnosed between 1954 and 2018 and their clinical courses have been followed [German & Passarge 1989, German 1993, German & Ellis 2002].
The main clinical features of Bloom syndrome are the following 5:
- Size and appearance. The most consistent clinical feature of Bloom syndrome seen throughout all stages of life is growth deficiency affecting height, weight, and head circumference. Body proportions are normal. Subcutaneous adipose tissue is sparse throughout childhood and adolescence, but adults may develop central obesity. Providing increased calories in childhood and adolescence does not usually result in substantial changes in growth parameters, particularly linear growth. Plasma growth hormone concentration is normal.
The affected fetus is smaller than normal for gestational age. The mean birth weight of affected males is 1,760 g (range 900-3,189 g) and of affected females, 1,754 g (range 700-2,892 g). The average adult height of men is 149 cm (range 128-164 cm) and of women, 138 cm (range 115-160 cm).
The facial appearance of people with Bloom syndrome is variable and may be indistinguishable from unaffected persons of similar age and size. More commonly, the face appears narrow, with underdeveloped malar and mandibular prominences and retrognathia or micrognathia. A paucity of subcutaneous fat may cause the nose and/or ears to appear prominent. - Feeding problems. Most parents report that feeding is an issue for their newborns, infants, and young children. The child with Bloom syndrome characteristically feeds slowly, has a decreased appetite, and eats a limited variety of foods. In a minority of infants with Bloom syndrome, nursing and eating are normal. Because of their slow growth and weight gain, many children are prescribed formula with increased caloric density and later are prescribed nutritional supplements that provide extra calories. Many infants have had gastrostomy tubes placed. Despite these maneuvers, weight gain continues to be modest, and children are rarely in the normal range for growth. Gastroesophageal reflux is common and may contribute to the feeding issues.
- Skin lesions. The skin at birth and during early infancy appears normal; however, typically following sun exposure during the first or second year of life, a red, sun-sensitive rash appears on the nose and cheeks and sometimes also on the dorsa of the hands and forearms. This rash varies in severity and extent among affected individuals; in some, it is minimal. It is usually characterized by telangiectasia but in others is described as poikiloderma. In severely affected individuals, the lesion can be bright red and can extend onto adjacent areas. Additional dermatologic manifestations include cheilitis, blistering and fissuring of the lips, eyebrow and eyelash hair loss, alopecia areata, and vesicular and bullous lesions with excessive or intense sun exposure. Café au lait macules and areas of hypopigmented skin are more numerous and larger than in those without Bloom syndrome.
- Immunodeficiency. In children and adults who have had laboratory evaluation of their immune system, the concentration of one or more of the plasma immunoglobulins is usually abnormally low. IgM and IgA levels are most commonly affected. Although the numbers of T and B cells are usually normal, variable abnormalities of the adaptive immune system suggest a possible role in the frequent infections reported in affected individuals.
- Infections. Parents of children with Bloom syndrome report that their affected children have more childhood infections than their sibs and peers; none, however, has had an opportunistic infection, and few persons with Bloom syndrome have had bacterial sepsis, meningitis, or pneumonia.
- Fertility. Most men with Bloom syndrome appropriately examined have had azoospermia or severe oligospermia. There is, however, one confirmed case of paternity [Ben Salah et al 2014]. Women with Bloom syndrome, although often fertile, may enter menopause prematurely. Eleven women with Bloom syndrome followed in the Registry have become pregnant at least once; seven of them have delivered a total of 11 healthy babies of normal size.
- Intelligence. There are no systematic studies of academic achievement or cognitive performance in persons with Bloom syndrome. The great majority appear to perform within the normal range of intellectual development. Some have required academic support for attention-related issues and task orientation, but it is not clear that the prevalence of these problems is different from that seen in the general population. Many others have excelled in school, with some earning graduate degrees.
- Other clinical features. Major anatomic defects are not increased in frequency. In the 281 persons in the Registry as of 2018, only single examples of the following have occurred: tracheoesophageal fistula, cardiac malformation, absent thumbs, and absence of a toe and malformation of a thumb.
Bloom syndrome complications
Medical complications of Bloom syndrome, all serious, in order of increasing frequency are the following:
- Chronic obstructive pulmonary disease (COPD). Chronic bronchitis and bronchiectasis are common, and pulmonary failure has been the cause of death in six persons.
- Myelodysplasia has been diagnosed in 23 persons in the Registry at a median age of 22.1 years (range 3-47), and it has progressed to acute myelogenous leukemia in at least seven. In all but three, the myelodysplasia was preceded by some form of cancer for which chemotherapy and/or radiotherapy had been administered.
- Diabetes mellitus. Abnormalities in insulin release and glucose tolerance have been detected in the eight healthy children (ages 9 months to 13 years) and the three healthy young adults with Bloom syndrome (ages 22, 28, and 28 years) appropriately studied 6. Because of insulin resistance, the diabetes mellitus of Bloom syndrome resembles type 2 diabetes but has a much earlier age of onset than in the general population. Paradoxically, diabetes in persons with Bloom syndrome commonly occurs in the setting of low body mass index (BMI), rather than high BMI. Diabetes has been diagnosed in 47 of 281 persons in the Registry (16.7%) at a mean age of 26.6 years (range 4-45 years). Although most individuals do not have severe complications, 16 have required insulin, and retinopathy has developed in two. Lipid profile abnormalities were also identified by Diaz et al 6 in five of the ten subjects tested.
- Cancer is the most frequent medical complication in Bloom syndrome and the most common cause of death. Although the wide distribution of cell types and anatomic sites of cancer resemble that in the general population, it occurs more frequently and at much earlier ages in Bloom syndrome. Development of multiple cancers in a single individual is also much more common. Table 1 summarizes the cancers diagnosed in individuals followed in the Bloom Syndrome Registry.
Bloom syndrome cancer
Table 1. Bloom syndrome cancer diagnosed in 145 persons in the Bloom Syndrome Registry (1954-2018)
| Malignancy Type / Tissue | Subtype | Frequency | Age at Diagnosis (years) | ||
|---|---|---|---|---|---|
| Median | Mean | Range | |||
| Leukemia | Acute myeloid | 17 | 21 | 19 | 6-32 |
| Acute lymphoblastic | 11 | 14 | 17 | 4-40 | |
| Other/biphenotypic/undefined | 12 | 18 | 19 | 2-40 | |
| Lymphoma | — | 37 | 20 | 21 | 4-49 |
| Oropharyngeal | Tongue | 9 | 37 | 37 | 30-48 |
| Pharynx | 6 | 32 | 34.8 | 31-45 | |
| Tonsil | 4 | 40 | 38 | 25-46 | |
| Other | 5 | NA | NA | NA | |
| Upper gastrointestinal | Esophageal | 5 | 39 | 37 | 25-48 |
| Gastric | 5 | 31 | 29 | 24-33 | |
| Other | 4 | NA | NA | NA | |
| Colorectal | — | 28 | 37 | 35 | 16-49 |
| Genitourinary | Cervical | 5 | 22 | 21 | 19-23 |
| Other | 9 | NA | NA | NA | |
| Breast | — | 24 | 33 | 33 | 21-52 |
| Skin | Basal cell | 13 | 29 | 28 | 18-38 |
| Squamous cell (uncategorized) | 5 | 35 | 35 | 35-36 | |
| Other/undefined | 4 | NA | NA | NA | |
| Wilms tumor | — | 8 | 3 | 3 | 1-8 |
| Lung | — | 4 | 37 | 36 | 32-40 |
| All other | — | 12 | NA | NA | NA |
Bloom syndrome diagnosis
Bloom syndrome should be suspected in an individual with any of the following clinical or cytogenetic findings.
Clinical findings:
- Prenatal-onset growth deficiency that usually includes linear growth, weight gain, and head circumference and that persists into infancy, childhood, and adulthood
- Moderate-to-severe growth deficiency and a sun-sensitive, erythematous rash that commonly involves the face and appears in a butterfly distribution
- Moderate-to-severe growth deficiency and a diagnosis of cancer, usually occurring at an earlier age than in the general population
Cytogenetic findings:
- Increased numbers of sister-chromatid exchanges
- Increased quadriradial configurations (Qrs) in cultured blood lymphocytes (a mean of 1%-2% Qrs are observed in cultured blood lymphocytes from a person with Bloom syndrome vs none in controls)
- Chromatid gaps, breaks, and rearrangements
Bloom syndrome is diagnosed by either cytogenetic analysis or mutation testing. Cytogenetic analysis is used to detect if there is an increased amount of sister chromatid exchange in cells. Genetic testing can reveal if a person has mutations in the BLM gene, which are known to cause Bloom Syndrome 3. If an individual has a family history of Bloom syndrome, one of these two testing methods may be used to find out if the person has also inherited the condition. An unusually low birth weight and short height throughout childhood are suggestive of Bloom syndrome in an individual with an affected sibling 5.
To establish the extent of disease and needs in an individual diagnosed with Bloom syndrome, in addition to the routine medical history, family history, and physical examination, the evaluations summarized in Table 2 (if not performed as part of the evaluation that led to the diagnosis) are recommended.
Table 2. Recommended evaluations following initial diagnosis in individuals with Bloom syndrome
| System/Concern | Evaluation | Comment |
|---|---|---|
| Gastrointestinal | Consultation w/gastroenterologist &/or feeding specialist | Evaluation for gastroesophageal reflux & problem feeding behaviors |
| Colonoscopy & fecal immunochemical testing | In probands age ≥10 yrs | |
| Dermatologic | Careful history & skin examination for sun-sensitive skin rash & for moles or nevi suspicious for basal cell or squamous cell carcinoma | |
| Immune |
| If patient has experienced severe &/or recurrent infections |
| Endocrine | Fasting blood glucose & hemoglobin A1C concentration | In probands age ≥10 yrs to evaluate for evidence of diabetes mellitus |
| Thyroid function testing: TSH w/reflex to T4 | At any age | |
| Lipid profile | Beginning at age 10 yrs | |
| Renal | Abdominal ultrasound examination for Wilms tumor | In probands age ≤8 yrs |
| Lymphoreticular | Whole-body MRI scan for lymphoma | In probands age ≥12 yrs |
| Breast | Breast MRI scan | In female probands age ≥18 yrs |
| Developmental | Developmental assessment | If indicated based on developmental history |
| Other | Consultation w/clinical geneticist &/or genetic counselor |
Bloom syndrome treatment
There is currently no cure for Bloom syndrome, so treatment is generally symptomatic and supportive. Because affected individuals are hypersensitive to DNA-damaging chemicals and ionizing radiation, standard cancer treatment plans often need to be adjusted for affected individuals. Changes may include reducing both the dosage and duration of the treatment; however, the cancers in affected individuals are often unusually responsive to treatment. The wide variety of types of cancer as well as the early development of tumors in affected individuals make life-long cancer surveillance significantly important. Additionally, it is recommended that individuals avoid sun exposure to the face, particularly in infancy and early childhood. Treatment of diabetes is typically the same as for individuals in the general population 5.
- Skin. Reduce excessive exposure to sunlight by seeking shade, particularly between 10 am and 4 pm. Cover exposed skin with clothing, including a broad-brimmed hat and UV-blocking sunglasses. Apply a broad-spectrum sunscreen with SPF of 30 twice daily, or every two to three hours if outdoors.
- Psychosocial. Family and teachers are encouraged to relate to persons with Bloom syndrome appropriately for their chronologic age rather than the younger age suggested by their unusually small size.
- Growth. Growth hormone administration to children with Bloom syndrome has not consistently increased growth rate in most persons, but some have experienced improved linear growth. Use of growth hormone has been approached cautiously in this population because of concerns regarding an increased risk of developing tumors as a result of their treatment. If growth hormone is prescribed, the growth response and serum IGF-1 and IGFBP-3 levels should be closely monitored, and unless there is an increase in growth velocity while under treatment, it should be discontinued.
- Nutrition. Until additional information is available regarding treatment of problematic feeding behaviors and gastrointestinal symptoms, standard treatment for these concerns is recommended. This may include consultation with a gastroenterologist or feeding specialist, use of high-calorie diets, institution of reflux precautions, and use of anti-reflux medications. Studies of small cohorts of individuals with Bloom syndrome have shown that supplemental feeding may result in increased fat deposition but not in improved linear growth. Because abnormalities have been identified in the lipid profile of persons with Bloom syndrome, caution should be exercised in the use of high-fat and/or high-cholesterol diets.
- Cognitive. Infants, toddlers, and preschool-age children with Bloom syndrome should have close developmental monitoring and referral for early intervention services. If developmental delays are present, physical, occupational, and speech therapy can help. School performance should be assessed regularly and parents made aware of available educational support.
- Diabetes mellitus. Treatment of diabetes mellitus in Bloom syndrome is the same as in other persons.
- Hypothyroidism. Thyroid hormone replacement therapy is recommended according to standard protocols.
- Dyslipidemia. Dietary treatment according to standard protocols is recommended.
- Cancer. The hypersensitivity of persons with Bloom syndrome to both DNA-damaging chemicals and ionizing radiation ordinarily necessitates modification of standard cancer treatment regimens, which usually includes a reduction of both dosage and duration. Individuals with Bloom syndrome have usually tolerated doses at or below 50% of the standard chemotherapy dosage, with no clear evidence that this has resulted in poorer outcomes. However, full weight-based dosing may be appropriate for some chemotherapeutic drugs such as steroids and tyrosine kinase inhibitors. Absence of information as to the ideal dosages makes such treatment particularly challenging to the physician; nevertheless, the fact that the cancers themselves often appear unusually responsive to the treatment justifies the special effort.
- Bone marrow transplantation (BMT). Hematopoietic stem cell transplantation (HSCT) has been performed in three persons in the Bloom Syndrome Registry. One person had more than five years of disease-free survival before succumbing to another cancer, and the other two persons died in the immediate post-transplant period. If HSCT is being contemplated, nonmyeloablative transplantation is likely to be tolerated more readily than other regimens. Additionally, the required ablative therapy prior to BMT often may require modification of standard protocols because of the hypersensitivity of persons with Bloom syndrome to DNA-damaging agents.
- Immune. Defects in humoral immunity can be managed with weekly subcutaneous or monthly intravenous infusions of gamma globulin. Cough assist devices, vibration vests, and daily nasal lavage can be used for mucociliary clearance for bronchiectasis. If an individual with Bloom syndrome experiences recurrent, severe, or opportunistic infection, immunodeficiency screening (including immunoglobulin level, antibody responses to vaccines, and quantitative B- and T-lymphocyte measurements) is recommended.
- Fertility
- Men with Bloom syndrome can undergo semen analysis to reveal azoospermia, oligospermia, or asthenospermia. Those who wish to conceive should consider consulting a fertility specialist. It is unclear if assisted reproductive technology (ART) may be helpful in persons with oligospermia or other abnormalities.
- Women with Bloom syndrome should be aware of signs of early menopause. Oocyte cryopreservation can be considered. Additionally, ART may be beneficial if natural conception is not possible; the authors are not aware of any prior use of ART in this population.
Agents and circumstances to avoid
Sun exposure to the face and other exposed areas, particularly in infancy and early childhood, should be avoided.
Exposure to ionizing radiation should be minimized.
Surveillance
Health supervision recommendations for surveillance in persons with Bloom syndrome have been published 7. It should be recognized, however, that these recommendations are based on limited data from the Bloom Syndrome Registry and on expert opinion. There are currently no clinical trials or case-control studies that address outcomes in people with Bloom syndrome. Because of the unusually high risk for early development of cancer, much of the health supervision effort is directed to early detection and treatment.
Table 3. Recommended surveillance for individuals with Bloom syndrome
| Manifestation | Evaluation | Frequency |
|---|---|---|
| Wilms tumor |
| Every 3 mos from time of diagnosis to age 8 yrs |
| Leukemia | Screening & family education on signs/symptoms incl pallor, abnormal bleeding, petechiae, fatigue, unintentional weight loss | Every health visit |
| Lymphoma | Screening & family education on signs/symptoms incl enlarged lymph nodes, unexplained fevers, drenching night sweats, fatigue, unintentional weight loss | Every health visit |
| Whole-body MRI | Every 1-2 yrs from age 12-13 yrs | |
| Colorectal cancer | Colonoscopy | Annually from age 10-12 yrs |
| Fecal immunochemical testing | Every 6 mos from age 10-12 yrs | |
| Breast cancer | Breast MRI in females | Annually from age 18 yrs |
| Skin cancer | Skin examination w/dermatologist for any suspicious skin lesions | On recognition of suspicious lesions & annually thereafter |
| Diabetes mellitus |
| Annually from age 10 yrs |
| Hypothyroidism |
| Annually from age 10 yrs |
| Dyslipidemia | Lipid profile | Annually from age 10 yrs |
- Hafsi W, Badri T. Bloom Syndrome (Congenital Telangiectatic Erythema) [Updated 2019 Nov 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448138
- Gratia M, Rodero MP, Conrad C, Bou Samra E, Maurin M, Rice GI, Duffy D, Revy P, Petit F, Dale RC, Crow YJ, Amor-Gueret M, Manel N. Bloom syndrome protein restrains innate immune sensing of micronuclei by cGAS. J. Exp. Med. 2019 May 06;216(5):1199-1213.
- Bloom syndrome. https://ghr.nlm.nih.gov/condition/bloom-syndrome
- Bloom syndrome. http://www.bloomssyndrome.org/bloomssyndrome.htm
- Flanagan M, Cunniff CM. Bloom Syndrome. 2006 Mar 22 [Updated 2019 Feb 14]. In: Adam MP, Ardinger HH, Pagon RA, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2020. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1398
- Diaz A, Vogiatzi MG, Sanz MM, German J. Evaluation of short stature, carbohydrate metabolism and other endocrinopathies in Bloom’s syndrome. Horm Res. 2006;66:111–7.
- Cunniff C, Djavid AR, Carrubba S, Cohen B, Ellis NA, Fein Levy C, Jeong S, Lederman HM, Vogiatzi M, Walsh MF, Zauber AG. Health supervision for people with Bloom syndrome. Am J Med Genet. 2018;176:1872–81.





{kind=link}