Calcaneovalgus foot
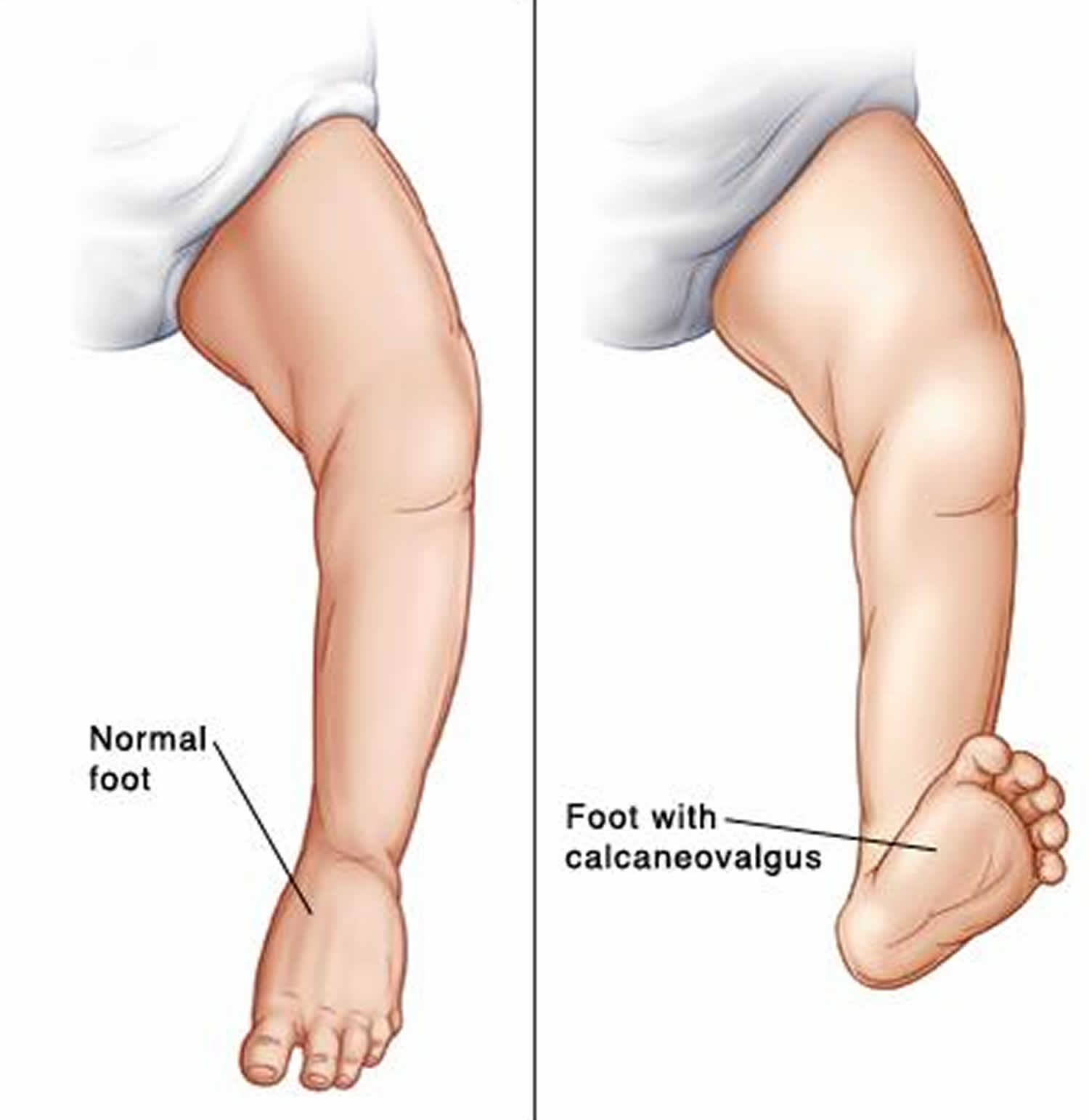
Calcaneovalgus foot is one of the most common deformities of the foot seen in newborns. Babies with calcaneovalgus foot are born with their foot and ankle excessively bent up, where the toes are usually touching the shin (Figure 1). Calcaneovalgus foot deformity may also present in older children, but is usually a manifestation of another condition.
The axis of calcaneovalgus deformity is in the tibiotalar joint, where the foot is positioned in extreme hyperextension, with its dorsum frequently touching the distal leg 1. Females are affected more often than males, and calcaneovalgus foot deformity can be unilateral or bilateral 2. Calcaneovalgus foot occurs in about 5 percent of all newborns 3 and is associated with external rotation of the calcaneus, an overstretched Achilles tendon, and tight anterior leg musculature, all of which warrant treatment 4.
On inspection, the foot has an “up and out” appearance, with the dorsal forefoot practically touching the anterior aspect of the ankle and lower leg (Figure 1). The ankle generally can be plantarflexed to only 90 degrees or less. Radiographs can confirm clinical diagnosis.
Calcaneovalgus is a positional deformity that is highly amenable to treatment. According to some authors 5, it has an excellent natural history and can spontaneously resolve on its own. Others 2 advocate a more aggressive approach because of the possibility of future complications, such as permanent muscle imbalance, peroneal tendon dislocation, and delayed ambulation. Generally, the more severe the limitation of ankle plantar flexion, the more treatment is warranted.
Treatment should begin as early as possible. Mild cases can be treated with stretching exercises performed at each diaper change. Stretching consists of gentle plantarflexion of the foot with mild inversion for a count of 10, repeated three times. In moderate cases or when stretching fails to correct the deformity, splinting or firm, high-top, lace-up shoes that prevent dorsiflexion can be used. For severe deformities with significant limitation of ankle plantarflexion, serial mobilization casting is performed until corrected, followed by nightly maintenance use of a bivalved cast or splinting of the posterior aspect of the leg for a two- to 10-week course 2.
Figure 1. Calcaneovalgus foot (correctable)


Footnote: A big difference between calcaneovalgus and congenital vertical talus is whether the deformity is rigid or flexible. Therefore it is important to examine the flexibility of the foot and write this in the notes. Look at the examination above. Calcaneovalgus foot is usually flexible, vertical talus is rigid.
Calcaneovalgus foot causes
Although the true cause of calcaneovalgus foot is unknown, the theory is that this is part of intrauterine “packaging” disorder, in other words, it reflects the babies foot position in the womb during the last few months of pregnancy. Calcaneovalgus runs in families, and more girls than boys have it.
Calcaneovalgus foot symptoms
Calcaneovalgus foot is obvious at birth. The foot is usually partially corrected, so the foot can be brought to the “normal” 90 degrees ankle position. It can present as unilateral or bilateral and it may be associated with other conditions, namely: posterior-medial bowing of the tibia (the leg is curved and shorter in the affected site), vertical talus (the talus bone is not in its correct position causing the entire foot to look deformed), muscle imbalance or nerve injury (usually seen in older children).
Calcaneovalgus foot diagnosis
While most children with calcaneovalgus outgrow the deformity, it is important for a trained clinician to examine your child to rule out more serious conditions.
Pediatricians and pediatric orthopedic surgeons may examine children with calcaneovalgus foot. Your child’s doctor will perform a complete medical history, physical examination and visual evaluation of your child.
Clinicians will ask if anyone else in your family is affected, look for other associated deformities, and examine your child from head to toes.
If there are any concerns of a more complex cause for calcaneovalgus foot, further investigation may be warranted utilizing:
- X-rays, which produce images of bones.
- Ultrasound, usually used for examination of babies’ hips and spine prior to their ossification/full development
Calcaneovalgus foot treatment
For most children with typical calcaneovalgus foot, no treatment is necessary, except for some home stretching exercises. Calcaneovalgus foot usually improves within the first several weeks of life. If there are other causes or associated conditions, those will be approached and managed as indicated.
It can be hard to treat calcaneovalgus foot in an older child. So it is best if the child is diagnosed as an infant. Here is what you can expect:
- For mild cases. Your child’s doctor will prescribe stretching exercises to be done at each diaper change. The parent gently moves the foot down and in for a count of 10, repeating the stretch 3 times.
- For moderate cases or when stretching does not correct the condition. Your child’s doctor may prescribe splints or firm, high-top, lace-up shoes. These hold the foot in the correct position.
- For severe cases. Your child’s doctor may prescribe casting of the child’s legs and feet for up to several months. The casts move the child’s foot into normal position. Casts are changed every 1 to 2 weeks.
Follow-up care
Most children with calcaneovalgus feet will not need long-term follow-up care. Except for children who present the deformity later in life and have other associated conditions.
What are the long-term concerns of calcaneovalgus feet?
- If diagnosed and treated, the child’s foot often works well and looks normal.
- If it doesn’t go away, calcaneovalgus can cause problems with muscle development and walking. So your child should see their healthcare provider for regular follow-up visits to be sure the problem goes away.
- The Newborn Foot. Am Fam Physician. 2004 Feb 15;69(4):865-872. https://www.aafp.org/afp/2004/0215/p865.html
- Connors JF, Wernick E, Lowy LJ, Falcone J, Volpe RG. Guidelines for evaluation and management of five common podopediatric conditions. J Am Podiatr Med Assoc. 1998;88:206–22.
- Widhe T. Foot deformities at birth: a longitudinal prospective study over a 16-year period. J Pediatr Orthop. 1997;17:20–4.
- Trott AW. Children’s foot problems. Orthop Clin North Am. 1982;13:641–54.
- Wall EJ. Practical primary pediatric orthopedics. Nurs Clin North Am. 2000;35:95–113.





{kind=link}