Congenital torticollis
Congenital muscular torticollis also called congenital torticollis, is a painless form of head tilting due to a muscle of the neck, called the sternocleidomastoid muscle, being shorter on one side of the neck than the other and it is present at birth or develops soon after (see Figure 3). The tight sternocleidomastoid muscle causes the head to tilt toward the side of the neck with the shortened muscle and the head to be turned away from that side. The baby tends to look away from the tight muscle. Congenital muscular torticollis is the most common cause of a wry-neck posture in the infant. Congenital muscular torticollis is often discovered during the first 6 to 8 weeks of life, when a newborn begins to gain more control over the head and neck.
“Congenital” means a condition that is present at birth. Congenital torticollis occurs at or shortly after birth.
In newborns, torticollis can happen due to the baby’s position in the womb or after a difficult childbirth.
Some babies with congenital torticollis also have developmental dysplasia of the hip—a condition in which the head of the thighbone is not held firmly in the hip socket.
It can be upsetting to see that your baby has a tilted head or trouble turning his or her neck. But most with babies don’t feel any pain from torticollis. And the problem usually gets better with simple position changes or stretching exercises done at home.
Torticollis can also develop later in infancy and childhood and even in adults. This type of torticollis is referred to as “acquired” torticollis and may be associated with a variety of conditions that require specialized treatment. Acquired torticollis is not discussed in this post.
Congenital muscular torticollis key points
- Torticollis is when the muscle on one side of the neck is shorter than on the other side. It causes the head to tilt to one side. The baby tends to look away from the tight muscle.
- If your baby only looks in one direction, try to encourage them to look to the less preferred side. A physiotherapist or occupational therapist may need to prescribe specific stretches.
- Torticollis is sometimes associated with a condition called positional plagiocephaly (flattened head syndrome), which is when the skull becomes flattened when a baby lays on their back or looks in one direction too long (see Figure 2).
- During the baby’s first few weeks, a soft lump or bump, which is similar to a “knot” in a tense muscle, may be felt in the affected neck muscle. This lump is not painful and gradually goes away before the baby reaches 6 months of age.
- Both of the tense muscle lump and positional plagiocephaly tend to go away as the torticollis gets better.
Figure 1. Congenital muscular torticollis
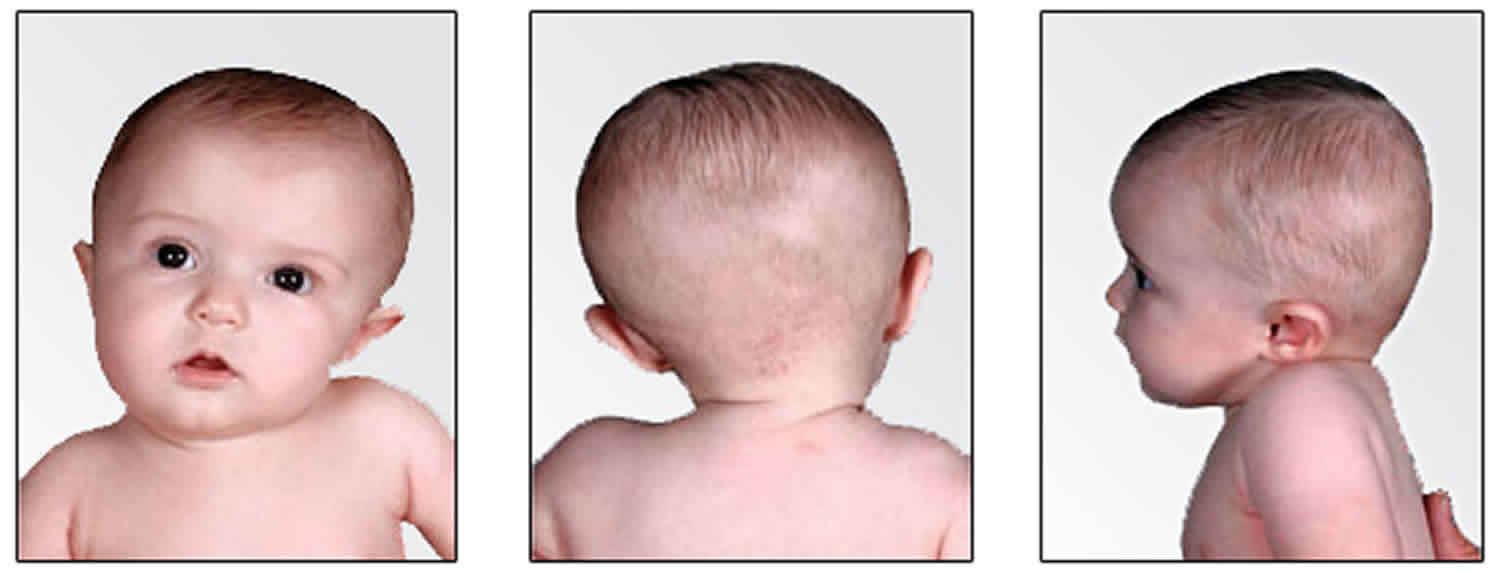

Figure 2. Flattened head syndrome (positional plagiocephaly)
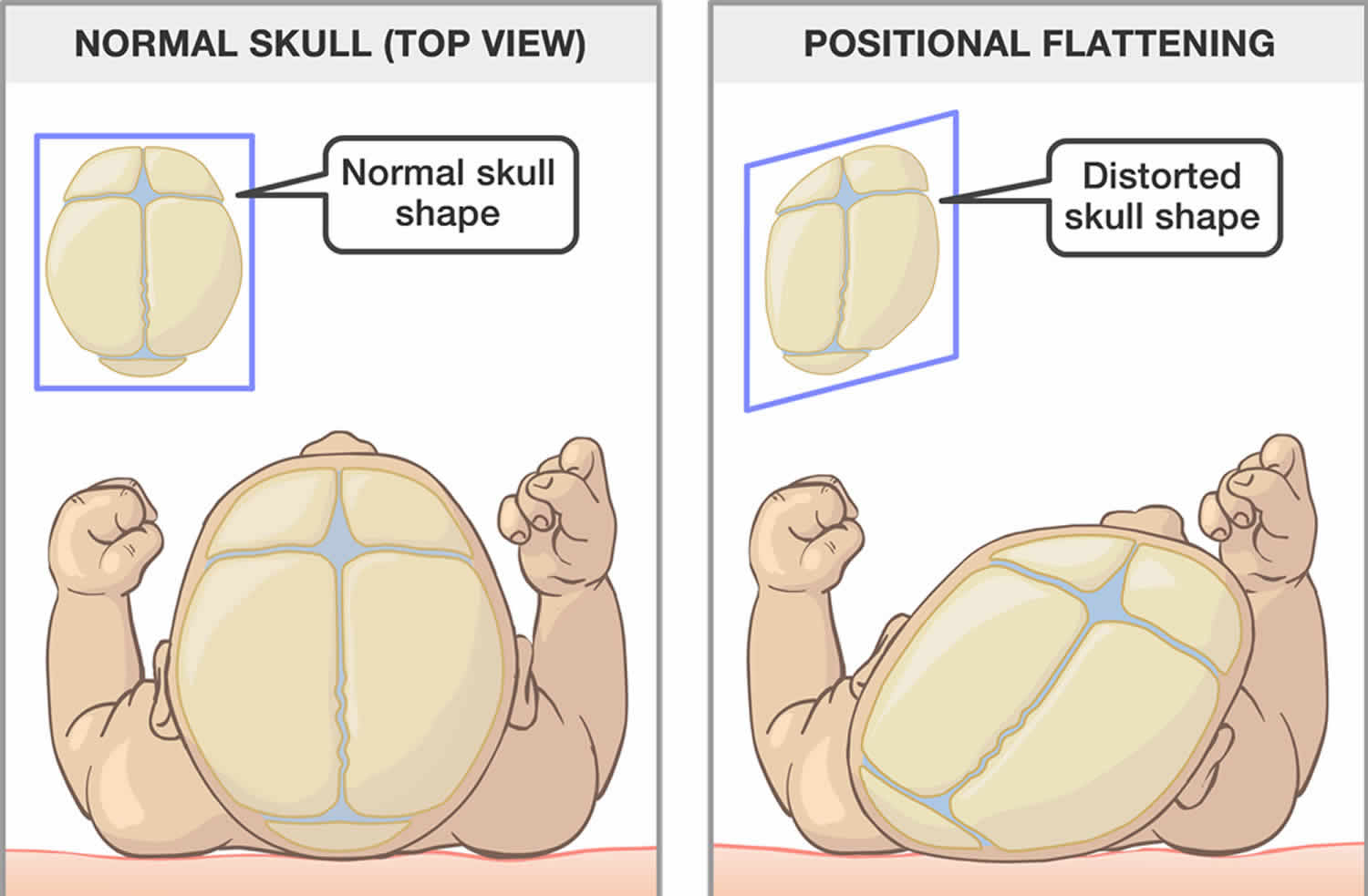
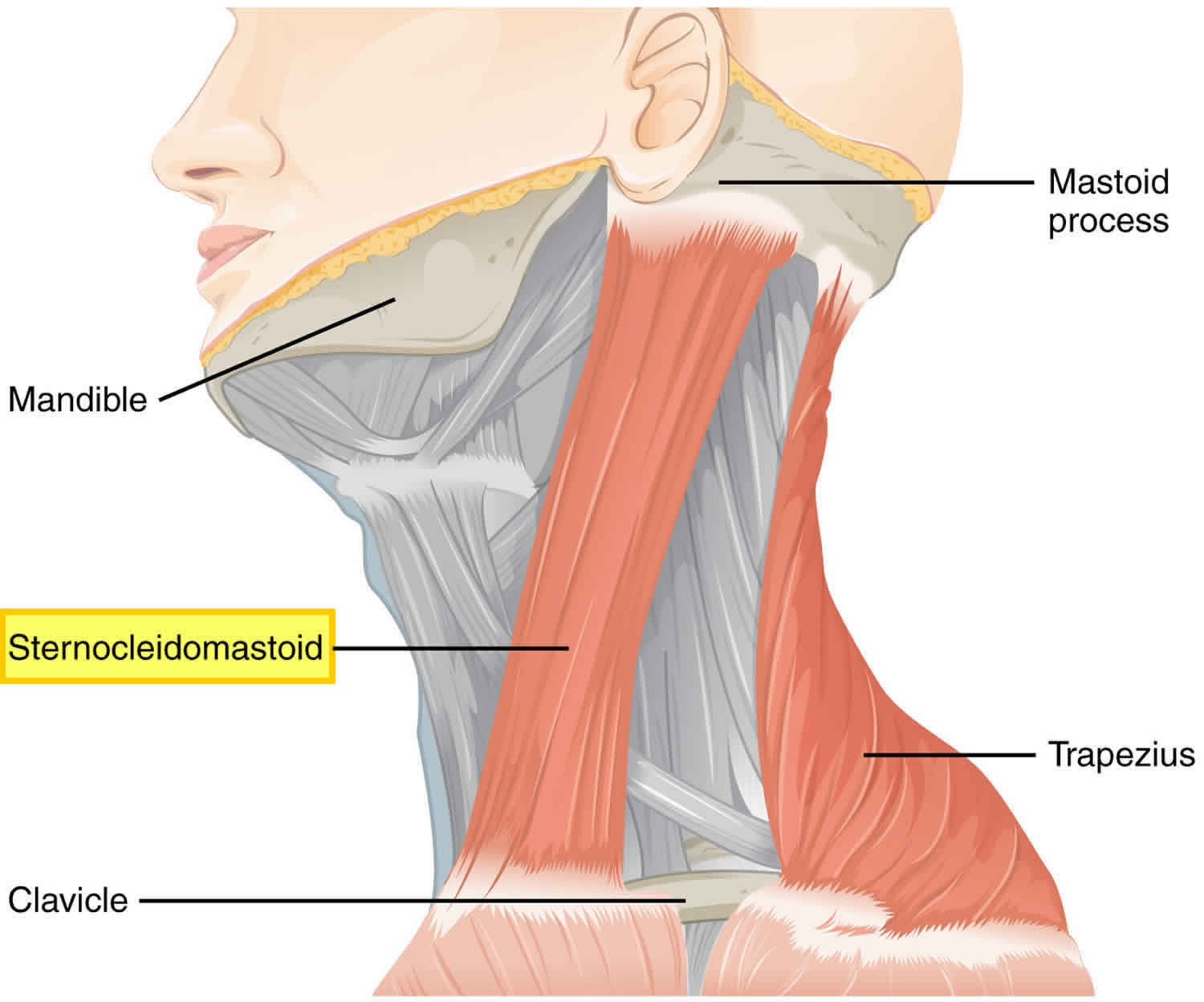
Figure 3. Sternocleidomastoid muscle
If you feel your baby has limited neck movement, see your doctor to learn about other help available. They may refer you to a physiotherapist.
After assessing your child’s head and neck, the therapist will design a home program for your baby. You may be given exercises and other recommendations.
Should I be concerned about the lump on my baby’s neck?
No. The lump that you may be feeling is scar tissue. This is a normal result of the healing process. It is not painful to your child. With specific stretching exercises given to you by a physiotherapist, it should go away in a few months.
Why does my baby prefer to look in one direction?
A baby with torticollis may tend to look in only one direction. The shortened neck muscle causes the head to be tilted towards it. The chin turns away from it. This is why your child prefers to look away from the tight muscle.
If your baby is always on their back or prefers to looks in one direction, part of their skull may become flat. This condition is called positional plagiocephaly. Positional plagiocephaly means flattening of the skull. Torticollis and plagiocephaly are closely associated with one another.
What should I do if my child only looks in one direction?
If your baby prefers to look in one direction, you should encourage them to look to the less-preferred side until they look equally in both directions. Your baby may have a tight muscle in their neck and they may need specific stretches. You should speak to your doctor or to a physiotherapist for more information.
In the meantime, here are some things you can do:
- During playtime, use mobiles or brightly coloured toys to encourage your baby to look in the less-preferred direction.
- When you are holding your baby, hold them in a way to encourage them to look in the less-preferred direction.
- If your baby’s crib is against the wall, put them at opposite ends of the crib each night. Babies prefer to look out into the room.
- If your baby’s crib is not against a wall, move a brightly coloured crib-safe toy to encourage them to look in a different direction each night.
Congenital torticollis causes
Congenital torticollis occurs when the neck muscle, known as the sternocleidomastoid muscle, that runs up and toward the back of the infant’s neck is shortened. This tilts the head down and to one side. This is known as congenital muscular torticollis.
Scientists still don’t know exactly what causes the shortened neck muscle. Researchers think that the sternocleidomastoid muscle may have had a small tear or it may be stretched during the baby’s birth. The tear causes bleeding and swelling. And scar tissue replaces some of the muscle, making it shorter.
More recently, it has been postulated that the sternomastoid muscle shortens as a result of scarring due to a vascular disturbance in the womb. Still others think that it is due to position of the baby’s head in the womb causing fibrosis or shortening of the muscle.
Some cases of congenital torticollis are caused by a bone problem in the neck portion of the spine (cervical spine). This is known as a congenital malformation of the cervical spine.
Torticollis may also occur later in life, but this is not congenital torticollis.
Risk factors for developing congenital torticollis
Risk factors include a breech pregnancy (where the fetus is leg-down instead of face-down) and a difficulty delivery. However, most congenital torticollis occur without any apparent cause in otherwise healthy infants.
Congenital torticollis has been associated with two other birth conditions:
- Developmental dysplasia of the hip – hip joint dislocation present at birth.
- Metatarsus adductus – the front of the foot is bent or angled in toward the middle of the foot.
Congenital torticollis symptoms
Congenital muscular torticollis does not cause pain. Babies with torticollis will act like most other babies except when it comes to activities that involve turning. Either side can be affected although it is often more common in the right (75%). The infant keeps his or her head tilted toward the affected side and the chin rotated toward the opposite shoulder. He or she will also have difficulty turning the head from side to side and up and down.
A olive-shaped lump may be visible or felt on the affected side in the first 3 months of life. The lump may eventually disappear as a tight fibrous band is replaced over the length of the neck muscle.
A baby with congenital torticollis might:
- tilt the head in one direction (this can be hard to notice in very young infants)
- prefer looking at you over one shoulder instead of turning to follow you with his or her eyes
- if breastfed, have trouble breastfeeding on one side (or prefers one breast only)
- work hard to turn toward you and get frustrated when unable turn his or her head completely
Some babies with torticollis develop a flat head (positional plagiocephaly) on one or both sides from lying in one direction all the time. During the baby’s first few weeks, a soft lump or bump, which is similar to a “knot” in a tense muscle, may be felt in the affected neck muscle. This lump is not painful and gradually goes away before the baby reaches 6 months of age. Both of these conditions tend to go away as the torticollis gets better.
Possible results of untreated congenital torticollis
- Plagiocephaly – This is the most common consequence of untreated Torticollis. Plagiocephaly is the mishapening of the bones on the skull, usually resulting in a large flat spot on one side of the back of the head and facial assymetries. Early diagnosis and conservative treatment can be successful in decreasing the severity of the Plagiocephaly. However, late diagnosis must be treated by a helmet or craniofacial surgery.
- Cervical spine contractures into the preferred head rotation and sidebend – These contractures can become ossified over time, significantly impacting functional mobility and ability to interact with peers. Once a contracture is ossified, surgery is required to lengthen the muscle, followed by several sessions of physical therapy to regain full cervical spine range of motion.
- Limited shoulder mobility – Decreased active movement into non-preferred rotation and sidebend can also result in shoulder elevation. This in turn impacts the child’s ability for upper extremity weight-bearing and reaching toward midline with hand.
- Cervical scoliosis – Persistent head tilt in the absence of shoulder elevation can result in a lateral shift of the cervical spine, which leads to cervical scoliosis.
Congenital torticollis complications
If the problem of wry-neck is not corrected, some of the complications that will appear as the child grows include:
- Asymmetry of skull and face – the face of the affected side may remain “flattened”. This is only reversible if the torticollis is corrected before age 1.
- Permanent limtations in head and neck movements.
Congenital torticollis diagnosis
If you notice that your child holds his or her head tilted to one side, consult your pediatrician. He or she will discuss your child’s general health, and will ask specific questions about the torticollis symptoms.
Your baby’s doctor will perform a comprehensive physical examination to see how far your baby can turn their head and check for other conditions that can cause torticollis symptoms. Imaging tests, such as x-rays and ultrasound scans, may be taken of your child’s neck and/or hips.
There is a 20% incidence of hip dysplasia children with muscular torticollis. So your doctor will perform an ultrasound exam of the hips in the first 4 to 6 weeks of life to rule that out.
Congenital torticollis treatment
Initial treatment consists of a massage and stretching program, which is successful in most cases when started in the first 6 months of life. If your baby does have congenital muscular torticollis, your baby’s doctor might teach you neck stretching exercises to practice at home. These help loosen the tight sternocleidomastoid muscle and strengthen the weaker one on the opposite side (which is weaker due to underuse). This will help to straighten out your baby’s neck.
Sometimes, doctors suggest taking a baby to a physical therapist for more treatment.
After treatment starts, the doctor may check your baby every 2 to 4 weeks to see if the torticollis is getting better.
Most babies with torticollis get better through position changes and stretching exercises. It might take up to 6 months to go away completely, and in some cases can take a year or longer.
Stretching exercises to treat torticollis work best if started when a baby is 3–6 months old. If you find that your baby’s torticollis is not improving with stretching, talk to your doctor. Your baby may be a candidate for muscle-release surgery, a procedure that cures most cases of torticollis that don’t improve.
If your child’s head tilt is caused by something other than congenital muscular torticollis, and the X-rays show no spinal abnormality, other treatment involving rest, a special collar, traction, application of heat to the area, medication, or, rarely, surgery may be necessary. To treat Klippel-Feil syndrome, a specialist may recommend treatments ranging from physical therapy to an operation. For treating torticollis due to injury or inflammation, your doctor may recommend applying heat, as well as using massage and stretching to ease head and neck pain. Your pediatrician can refer you to a specialist for a definitive diagnosis and treatment program.
Helping your baby at home
Encourage your baby to turn the head in both directions. This helps loosen tense neck muscles and tighten the loose ones. Babies cannot hurt themselves by turning their heads on their own.
There are other things that you can do at home to help:
- Place toys where your baby must turn his or her head to see them.
- Carry your child so that he or she looks away from the limited side.
- Position the crib and changing table so that your child must look away from the limited side to see you.
- Lay your baby on his or her stomach for brief periods when awake (“tummy time”) to help strengthen the neck muscles.
Congenital torticollis exercises
The standard treatment for congenital muscular torticollis consists of an exercise program to stretch the sternocleidomastoid muscle.
Stretching exercises include turning the baby’s neck side to side so that the chin touches each shoulder, and gently tilting the head to bring the ear on the unaffected side down to the shoulder.
These exercises must be done 4 to 6 times a day. Your doctor or a physical therapist will teach you how to perform the exercises.
Here are some exercises to try:
- When your baby wants to eat, offer the bottle or your breast in a way that encourages your baby to turn away from the favored side.
- When putting your baby down to sleep, position them to face the wall. Since babies prefer to look out onto the room, your baby will actively turn away from the wall and this will stretch the tightened muscles of the neck. Remember — always put babies down to sleep on their back to help prevent Sudden Infant Death Syndrome (SIDS).
- During play, draw your baby’s attention with toys and sounds to make him or her turn in both directions.
Don’t forget “Tummy Time”
Laying your baby on the stomach for brief periods while awake (known as “tummy time”) is an important exercise. It helps strengthen neck and shoulder muscles and prepares your baby for crawling.
This exercise is especially useful for a baby with torticollis and a flat head, and can help treat both problems at once. Here’s how to do it:
- Lay your baby on your lap for tummy time. Position your baby so that his or her head is turned away from you. Then, talk or sing to your baby and encourage him or her to turn and face you. Practice this exercise for 10 to 15 minutes.
For stretching and positioning RIGHT sternomastoid torticollis
Stretching
- For the following stretching exercises, the parent sits with the back against the wall and knees bent.
- Place the child in your lap, with the child on her back and knees tucked.
Sidebending
- Hold the child’s RIGHT shoulder down with your LEFT hand.
- Place your RIGHT hand on top of the RIGHT side of the child’s head, and slowly bend her head towards her LEFT shoulder.
- Hold the position for 10 seconds. Repeat 15 times, 4 to 6 times a day.
Rotation
- Place your RIGHT forearm against the child’s LEFT shoulder, and cup the child’s head with the same hand.
- Use your LEFT hand to hold the child’s chin.
- Slowly rotate the child’s face to her RIGHT.
Hold the position for 10 seconds. Repeat 15 times, 4 to 6 times a day.
Positioning
- Playing on stomach: When the child is on her stomach, position all toys in the crib so that the child has to turn her face to the RIGHT.
Carrying
- Hold the child facing away from you, in a side-lying position, with the child’s RIGHT ear resting against your RIGHT forearm.
- Place your LEFT arm between the child’s legs and support the child’s body.
- Carry the child in this position as much as possible.
Other suggestions
- Hold toys so that the child has to look up and out to her RIGHT.
- Position child in crib so that activities in the room encourage her to look RIGHT.
- While bottle feeding the child, position her to face RIGHT.
- While holding the baby across the shoulder, position her to face RIGHT.
For stretching and positioning LEFT sternomastoid torticollis
Stretching
- For the following stretching exercises, the parent sits with the back against the wall and knees bent.
- Place the child in your lap, with the child on her back and knees tucked.
Sidebending
- Hold the child’s LEFT shoulder down with your RIGHT hand.
- Place your LEFT hand on top of the LEFT side of the child’s head, and slowly bend her head towards her RIGHT shoulder.
- Hold the position for 10 seconds. Repeat 15 times, 4 to 6 times a day.
Rotation
- Place your LEFT forearm against the child’s RIGHT shoulder, and cup the child’s head with the same hand.
- Use your RIGHT hand to hold the child’s chin.
- Slowly rotate the child’s face to her LEFT.
- Hold the position for 10 seconds. Repeat 15 times, 4 to 6 times a day.
Positioning
- Playing on stomach: When the child is on her stomach, position all toys in the crib so that the child has to turn her face to the LEFT.
Carrying
- Hold the child facing away from you, in a side-lying position, with the child’s LEFT ear resting against your LEFT forearm.
- Place your RIGHT arm between the child’s legs and support the child’s body.
- Carry the child in this position as much as possible.
Other suggestions
- Hold toys so that the child has to look up and out to her LEFT.
- Position child in crib so that activities in the room encourage her to look LEFT.
- While bottle feeding the child, position her to face LEFT.
- While holding the baby across the shoulder, position her to face LEFT.
Surgical treatment
If nonsurgical options do not correct the torticollis, your doctor may suggest surgery.
Approximately 10% of children with congenital muscular torticollis require surgery. The operation is typically scheduled once the child reaches preschool years. The procedure will lengthen the short sternocleidomastoid muscle, and may be done as an outpatient surgery, meaning your child could go home the same day.





{kind=link}