
What is calcification
Calcification is a process in which calcium builds up in body tissue, causing the tissue to harden. Calcification can be a normal or abnormal process. Ninety-nine percent of calcium entering your body is deposited in your bones and teeth. The remaining calcium dissolves in your blood.
When a disorder affects the balance between calcium and certain chemicals in your body, calcium can be deposited in other parts of the body, such as the arteries, kidneys, lungs, and brain. Calcium deposits can cause problems with how these blood vessels and organs work. Calcifications can usually be seen on x-rays. A common example is calcium depositing in the arteries as part of atherosclerosis.
Vascular calcification
Vascular calcification or calcification of arteries is a strong predictor of future cardiovascular disease in humans and may contribute directly to the pathogenesis of cardiovascular events 1. There are two main types of vascular calcification that have been reported in adults: intimal calcification, associated with atherosclerosis, and medial also known as Mönckeberg calcification, associated with chronic kidney disease and diabetes 2. Intimal calcification occurs in the setting of lipid accumulation and macrophage infiltration into the vessel wall 2. Intimal calcium deposition in the thin fibrous caps of atherosclerotic disease has been proposed to increase local biomechanical stress and contribute to plaque rupture 3. Medial wall calcification occurs independently of intimal calcification, localizes to elastin fibers or smooth muscle cells, and is not associated with lipid deposition or macrophage infiltration 4. Medial calcification impacts clinical outcomes by increasing arterial stiffness, which can induce cardiac hypertrophy and affect cardiac function 5.
Coronary artery calcification and aortic calcification are hallmarks of atherosclerotic disease and serve as strong predictors of cardiovascular events 6.
Calcification in kidney
Calcification in kidney or nephrocalcinosis refers to generalized calcium deposition in the kidney and does not include the focal calcium deposition associated with focal renal injury 7. Calcification in kidney is caused by diseases that cause hypercalcemia, hyperphosphatemia, hypercalciuria, hyperphosphaturia, and hyperoxaluria.
Calcification in kidney falls into the following classifications:
- Molecular or chemical: an increase in intracellular calcium concentration which is quantifiable but not microscopically or radiologically visible
- Microscopic calcification: Deposits visible by light microscopic examination of kidney biopsy specimen but not radiologically visible
- Macroscopic calcification: calcification visible radiologically
Calcification in kidney usually involves the renal medulla and much less often the cortex.
Conditions associated with cortical nephrocalcinosis are:
- Cortical necrosis such as occurs in pregnancy
Transplant rejection - Chronic glomerulonephritis
- Trauma
- Tuberculosis
- Oxalosis
Oxalosis is one condition which can cause both medullary and cortical nephrocalcinosis.
Calcification in kidney causes
The most common cause of kidney calcification is hypercalciuria with or without hypercalcemia. The metabolic abnormalities of hypercalciuria, hyperphosphaturia, and hyperoxaluria are often associated with kidney calcification and patients often present with both conditions. Calcium phosphate and calcium oxalate crystals form when the concentration of the solutes exceed the saturation limit in the tubular fluid. In a study by Evan AP et al. 8, Randall’s plaques were noted in the inner medullary interstitium as part of the basement membranes of the thin limb of the loop of Henle where the tubular fluid is saturated. Once these calcium phosphate plaques form, they can enlarge into the surrounding interstitial tissue or rupture into the tubular lumen subsequently forming a nidus for luminal calcium oxalate stone.
Light microscopy in nephrocalcinosis shows intracellular, tubular, and interstitial basophilic calcifications. Calcium phosphate deposition is accompanied by lymphocyte predominant interstitial infiltrate and interstitial fibrosis.
Calcium phosphate crystal formation occurs in alkaline urine pH. It has associations with many diseases which operate through the underlying mechanisms.
- Hypercalciuria with hypercalcemia
- Hypercalciuria without hypercalcemia
- Hyper-phosphaturia with hyperphosphatemia
- Hyper-phosphaturia without hyperphosphatemia
1. Conditions causing both hypercalcemia and hypercalciuria
- Primary hyperparathyroidism
- Vitamin D therapy
- Sarcoidosis
- Milk-alkali syndrome
- Congenital hypothyroidism
2. Conditions causing hypercalciuria without hypercalcemia
- Distal renal tubular acidosis
- Medullary sponge kidney
- Neonatal nephrocalcinosis and loop diuretics
- Inherited tubulopathies
- Chronic hypokalemia
- Beta thalassemia
3. Conditions causing Hyper-phosphaturia and hyperphosphatemia
- Tumor lysis syndrome
- Oral sodium phosphate bowel preparations
4. Conditions causing Hyper-phosphaturia without hyperphosphatemia
- Inherited tubulopathies such as Dent disease, Lowe syndrome
- X-linked, autosomal dominant, and autosomal recessive hypophosphatemic rickets.
Calcification in kidney signs and symptoms
Calcification in kidney most commonly presents as asymptomatic, chronic disease process discovered on radiographic imaging of abdomen. However, ordering radiographs might be feasible due to the evaluation of pain caused by coexisting nephrolithiasis. Nephrolithiasis can occur due to chronic hypercalcemia and hypercalciuria. It can cause renal colic. Polyuria and polydipsia can occur with chronic hypercalcemia, medullary nephrocalcinosis, and in Bartter syndrome.
Calcification in kidney can also present acutely with renal failure in instances such as tumor lysis syndrome and acute phosphate nephropathy.
Calcification in kidney complications
X-linked hypophosphatemic rickets if not treated appropriately will cause stunted bone growth. In hypomagnesemia-hypercalciuria syndrome children can present with tetanic seizures, muscle cramps, and weakness. In a subset of patients, sensorineural hearing loss and ocular impairment can occur.
Calcification in kidney diagnosis
Once the radiologic determination of kidney calcification has taken place, the causal investigation should follow. Serum electrolytes, calcium, phosphate should be measured. Measurement of urine pH should help determine the presence of distal renal tubular acidosis. Besides the above, the recommendation is to obtain two 24 hour urine collections for measuring the excretion of calcium, phosphate, oxalate, citrate, and creatinine.
Calcification in kidney treatment
Treatment is directed to treat the underlying cause of kidney calcification. Strategies to reduce the urinary concentration of calcium, phosphate, or oxalate are used. Fluid intake is increased to produce at least 2 Liters of urine a day.
Among patients with hypercalciuria, urinary calcium excretion can be reduced by restricting the amount of animal protein, decreasing the sodium intake to less than 100 milliequivalents /day, increasing the potassium intake, and using a thiazide diuretic to reduce the urinary calcium excretion. However, patients with hypercalcemia should not use a thiazide diuretic.
In kidney calcification due to distal renal tubular acidosis, potassium citrate is used in patients with hypocitraturia and pH less than 7. This not only replenishes the potassium loss but also achieves a normal urinary citrate level, thereby increasing the solubility of calcium.
Calcification in kidney prognosis
Specific causes of kidney calcification such as Dent disease, primary hyperoxaluria, and hypomagnesemic hypercalciuric nephrocalcinosis, if not treated effectively, would progress to chronic renal failure or end stage renal disease 9. Kidney calcification once detected radiologically is rarely reversible.
Heart calcification
In the heart, calcification of cardiac muscle leads to conduction system disturbances and is one of the most common pathologies underlying heart blocks 10. However the cell identity and mechanisms contributing to pathological heart muscle calcification remain unknown 10.
Pathological mineralization of soft tissues, or ectopic calcification, commonly occurs with tissue injury, degeneration and in common diseases such as diabetes and chronic kidney disease. Calcification of soft tissues is a cell mediated process that resembles bone formation in the skeletal system with calcification of the extracellular matrix by cells capable of mineralization 11. Heart muscle calcification is an under-reported and unusual form of soft tissue calcification characterized by calcific deposits within the myocardium, which can occur in the absence of calcification of valves, vessels or other organs 12. Myocardial calcification is observed in the aging heart and in patients with diabetes, renal disease, and myocardial injury secondary to ischemia or inflammation 13. Calcification within the heart muscle is one of the most common underlying causes of heart blocks where calcification and fibrosis of the conduction system interrupt smooth propagation of electrical impulses 14. Cardiac pump dysfunction and arrhythmias can also occur depending on the extent and anatomic site of calcification and calcified myocardial scars have been reported to cause refractory ventricular tachycardia. Cardiac calcification is also a prognostic indicator of poor outcomes following myocardial infarction or myocarditis 15. Even during embryonic development, progressive calcification of myocardial walls can occur and leads to fetal or neonatal demise 16.
Despite the occurrence of heart muscle calcification in a variety of disease conditions, little is known about the identity of cells contributing to pathological myocardial calcification. We have recently demonstrated that cardiac fibroblasts can exhibit plasticity after heart injury and adopt alternative cell fates 17. Ectopic calcification of soft tissues usually occurs in areas of injury associated with fibrosis 18 and this led us to hypothesize that cardiac fibroblasts can adopt osteoblast cell like fates and directly contribute to calcification of the heart muscle.
Calcification in lungs
Calcification in lungs or pulmonary calcification (deposition of calcium salts in lung tissues) and ossification (bone tissue formation) occurs with a number of systemic and pulmonary conditions. The mechanism(s) of lung calcification with or without ossification is not precisely known 19. No single factor is responsible 19. Specific symptoms of lung calcification are often lacking, but lung calcification may be a marker of disease severity and its chronicity. Pathophysiologic states predisposing to lung calcification and ossification include hypercalcemia, a local alkaline environment, and previous lung injury 19. Factors such as enhanced alkaline phosphatase activity, active angiogenesis, and mitogenic effects of growth factors may also contribute. The clinical classification of pulmonary calcification includes both metastatic calcification, in which calcium deposits in previously normal lung or dystrophic calcification, which occurs in previously injured lung. Pulmonary ossification can be idiopathic or can result from a variety of underlying pulmonary, cardiac, or extracardiopulmonary disorders. The diagnosis of pulmonary calcification and ossification requires various imaging techniques, including chest radiography, computed tomographic scanning, and bone scintigraphy. Interpretation of the presence of and the specific pattern of calcification or ossification may obviate the need for invasive biopsy. In this review, specific conditions causing pulmonary calcification or ossification that may impact diagnostic and treatment decisions are highlighted. These include metastatic calcification caused by chronic renal failure and orthotopic liver transplantation, dystrophic calcification caused by granulomatous disorders, DNA viruses, parasitic infections, pulmonary amyloidosis, vascular calcification, the idiopathic disorder pulmonary alveolar microlithiasis, and various forms of pulmonary ossification.
Pathologic soft tissue calcification can be broadly divided into either (1) metastatic calcification, in which calcium deposits in normal tissues, or (2) dystrophic calcification, in which calcification is superimposed on previously injured lung.
Metastatic lung calcification is further subdivided into benign 20 and malignant causes 21 (see causes below). By far the most common cause of metastatic lung calcification is seen in patients on hemodialysis for chronic renal insufficiency. The other causes are uncommon. Dystrophic calcification follows caseation, necrosis, or fibrosis and may complicate pulmonary infections that include (1) granulomatous infections, for example, Histoplasma capsulatum 22, Coccidioides immitis 23, and Mycobacterium tuberculosis 24; (2) viral infections, for example, varicella virus 25 and smallpox virus 26; and (3) parasitic infections, for example, Paragonimus westermani 27 and Pneumocystis carinii 28. In sarcoidosis, pulmonary calcification can result from either dystrophic calcification or metastatic calcification secondary to hypercalcemia 29. Pulmonary vascular calcification is postulated to result from shear stress and is considered to be a variant of dystrophic calcification 30. Dystrophic calcification has also been described in association with amyloidosis and after inhalation exposures in coal workers pneumoconiosis and silicosis. Pulmonary alveolar microlithiasis is a unique idiopathic calcific disorder with distinct histologic and radiographic appearances that do not fit into either metastatic or dystrophic calcification.
Figure 1. Lung calcification

Footnote: Chest radiograph demonstrating the punctate pulmonary calcification as a sequela of adult varicella pneumonia
[Source 31 ]Calcification in lungs causes
Causes of lung calcification:
I. Metastatic calcification
A. Benign causes
- Chronic renal insufficiency on hemodialysis
- Orthotopic liver transplantation
- Primary hyperparathyroidism
- Excess exogenous administration of calcium and vitamin D (milk-alkali syndrome)
- Hypervitaminosis D
- Osteopetrosis
- Osteitis deformans (Paget’s disease)
B. Malignant causes
- Parathyroid carcinoma
- Multiple myeloma
- Lymphoma/leukemia
- Hypopharyngeal squamous cell carcinoma
- Synovial sarcoma
- Breast carcinoma
- Choriocarcinoma
II. Dystrophic calcification
A. Granulomatous disorders
- Histoplasmosis
- Coccidioidomycosis
- Tuberculosis
- Sarcoidosis
B. Viral infections
- Postvaricella pneumonia
- Smallpox handler’s lung
C. Parasitic infections
- Paragonomiasis
- Pneumocystosis
D. Amyloidosis
E. Pulmonary vascular calcifications
- Vascular grafts
- Pulmonary hypertension
- Congenital high flow
- Hemosiderosis
F. Coal worker’s pneumoconiosis
G. Silicosis
Idiopathic
- Pulmonary alveolar microlithiasis
Causes of pulmonary ossification
I. Idiopathic pulmonary ossification
II. Preexisting pulmonary disorder
- Idiopathic pulmonary fibrosis
- Pulmonary amyloidosis
- Chronic busulfan therapy
- Acute respiratory distress syndrome
- Hamman-Rich syndrome
- Sarcoidosis
- Histoplasmosis
- Tuberculosis
- Metastatic breast cancer
- Pulmonary metastases of osteogenic sarcoma
- Metastatic melanoma
III. Preexisting cardiac disorder
- Mitral stenosis
- Chronic left ventricular failure
- Idiopathic hypertrophic subaortic stenosis
IV. Preexisting extracardiopulmonary disorder
- Primary and secondary hyperparathyroidism
- Hypervitaminosis D
- Pyloric stenosis with alkalosis
Calcification in brain
Calcification in brain or intracranial calcification refers to calcification within the cranial cavity, and is generally taken to mean calcification within the parenchyma of the brain or its vasculature 32. The term physiological calcification is used to indicate calcification when seen as part of normal ageing. It is arguable whether physiological calcification occurs anywhere other than in the pineal gland or choroid plexus 32. Therefore, with the exception of calcification in these areas, which rarely manifests in the first two decades of life, brain calcification occurring before the age of 20 years can be regarded as pathological 32.
Traditional pathology teaching distinguishes between metastatic and dystrophic calcification. Metastatic calcification occurs as a result of systemic disorders of calcium metabolism, such as hypo‐ and hyperparathyroidism. All other brain calcification is considered as dystrophic, meaning calcification occurring as a result of pathologies within the brain itself 32.
There is probably no pathological insult that cannot, in some circumstances, result in brain calcification. Thus, there is a potentially endless list of brain calcification causes 32. However, for poorly understood reasons, there are certain disorders in which brain calcification is prominent and/or characteristic, so that its recognition has value for diagnostic purposes.
In 1986, Kendall and Cavanagh 33 reviewed 18,000 computerized tomography (CT) images taken at Great Ormond Street Hospital between 1977 and 1983, and identified ‘pathological’ brain calcification in 1.6%. In just under half (43%) of these the cause was neoplastic. Adult studies of basal ganglia calcification suggest a prevalence of 6.6 per 1000 population 34. In pediatric neurology practice, the identification of brain calcification represents a common diagnostic starting point for investigation of a neurological disorder.
Calcification in brain or intracranial calcification is a common finding on neuroimaging in pediatric neurology practice. In approximately half of all cases the calcification occurs in damaged, neoplastic, or malformed brain 32. For the large number of other disorders in which brain calcification occurs, no common pathogenetic mechanism can be suggested 32. Congenital infection, particularly with cytomegalovirus, accounts for a significant proportion of all brain calcification cases. However, some genetic diseases, in particular Aicardi-Goutières syndrome, Band-like calcification, and RNASET2-related disease, may mimic congenital infection; therefore, a full consideration of the radiological and clinical features is necessary before concluding that congenital infection is the cause. In some disorders brain calcification is a universal finding, in others it is a frequent occurrence, and in some it is only an occasional finding. Characteristic patterns of brain calcification are seen in a number of conditions, and a systematic approach to the identification and description of radiological findings, taken together in the context of the clinical scenario, allows a diagnosis to be made in many cases. Nonetheless, there remain a number of presumed genetic disorders associated with brain calcification for which the underlying molecular cause has not yet been identified 32.
Figure 2. Calcification in brain
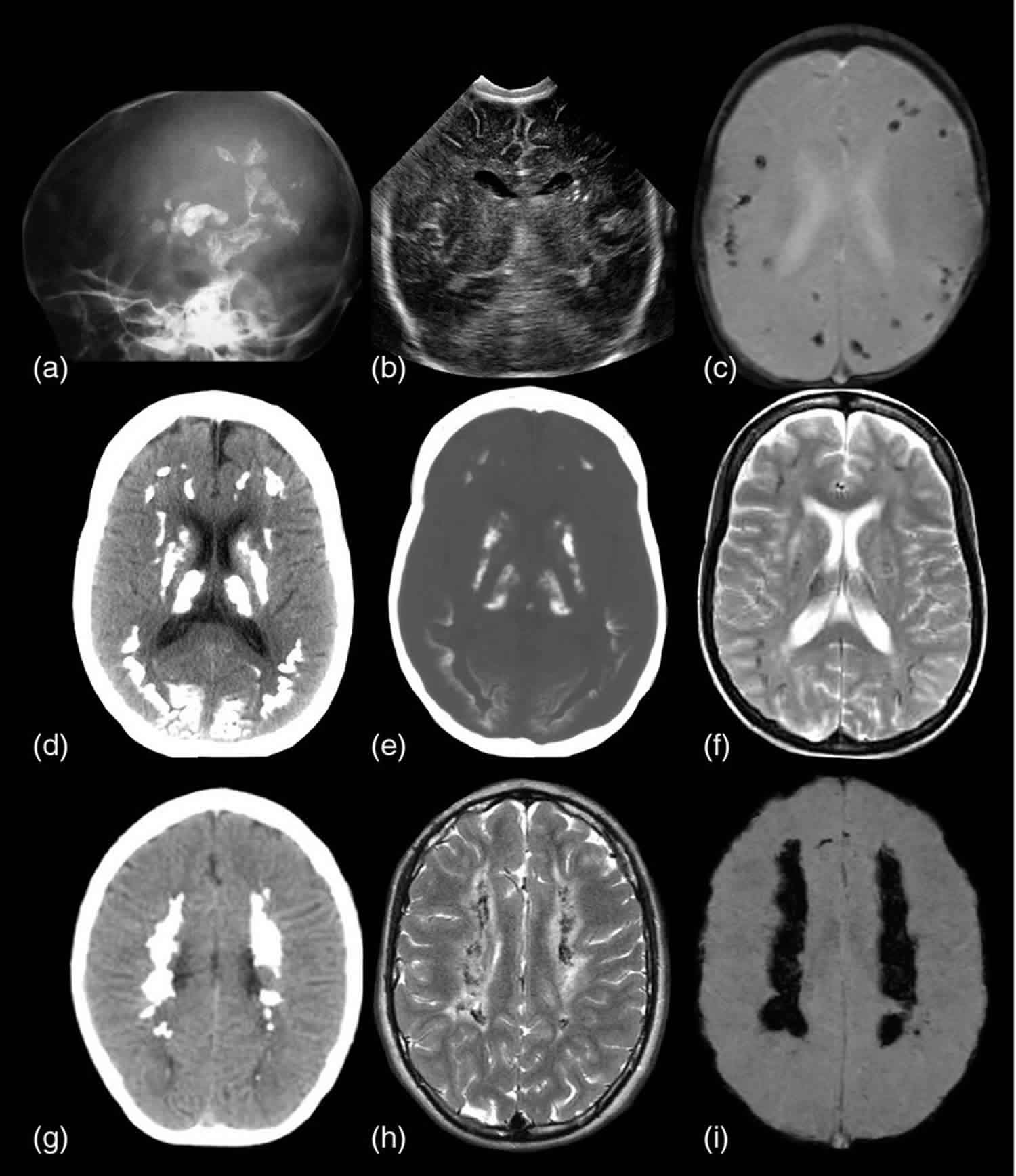
Footnote: The identification of calcification in brain using different imaging modalities. (a) Dense calcification is readily apparent on a plain film skull radiograph. (b) Ultrasound image of a child with congenital cytomegalovirus infection. ICC is readily seen as highly echogenic areas in the left periventricular region. (c) Gradient echo axial MR image of an infant with congenital toxoplasmosis showing multiple low‐signal spots within the cortex and white matter. The spatial resolution is poor in gradient echo images. Different imaging modalities provide complementary information. (d) CT image at normal brain window settings (e) CT image at bony window settings, and (f) T2‐weighted axial MRI of the same patient. The location of brain calcification may be difficult to determine on normal brain window settings (d), whereas on the bone window settings (e) the cortical location is apparent. This is confirmed on the T2‐weighted MR (f) by the low‐signal ribbon seen at the depths of the gyri. (g) CT, (h) T2‐weighted axial MR, and (i) susceptibility‐weighted axial MR images from the same patient, illustrating the differing appearances of brain calcification depending on the modality used.
[Source 32 ]What is calcification in the breast
Mammograms are pictures (x-rays) of the breast, used to check for breast cancer. Possible mammogram findings include:
Calcifications. There are two types of breast calcifications, or calcium deposits:
- Macrocalcifications (large, rounded calcifications), which look like small white dots on a mammogram. Macrocalcifications are often caused by aging being common in women over age 50, an old injury, or inflammation and are usually benign. Macrocalcifications are most likely not related to cancer. You will rarely need more testing.
- Microcalcifications, which look like white tiny calcium specks on a mammogram. Most of the time, they are not cancer. However, these areas may need to be checked more closely if they have a certain appearance on the mammogram. If found in an area of rapidly dividing cells or grouped together in a certain way, microcalcifications may be a sign of ductal carcinoma in situ (DCIS) or breast cancer. In-situ carcinoma or carcinoma in situ (CIS) is used for the earliest stage of breast cancer, when it is confined to the layer of cells where it began. The normal breast is made of tiny tubes (ducts) that end in a group of sacs (lobules). Cancer starts in the cells lining the ducts or lobules, when a normal cell becomes a carcinoma cell. As long as the carcinoma cells are still confined to the breast ducts or lobules, and do not break out and grow into surrounding tissue, it is considered in-situ carcinoma or carcinoma in situ (CIS). Once the carcinoma cells have grown and broken out of the ducts or lobules, it is called invasive or infiltrating carcinoma. In an invasive carcinoma, the tumor cells can spread (metastasize) to other parts of your body. There are 2 main types of in-situ carcinoma of the breast: ductal carcinoma in-situ (DCIS) and lobular carcinoma in situ (LCIS). Intraductal carcinoma is another name for ductal carcinoma in-situ (DCIS). If ductal carcinoma in situ (DCIS) is left untreated, it can go on to become an invasive cancer, so it is often called a pre-cancer. Still, scientists don’t really understand it well. Scientists don’t think that all DCIS would go on to become invasive cancer, but they can’t tell which DCIS would be safe to leave untreated. Treatment is aimed at getting rid of all the DCIS, usually by surgery. In some cases, radiation (radiotherapy) or hormone therapy (like tamoxifen) is given after surgery to lower the chance that it will come back later (recur) or that invasive carcinoma will occur.
Microcalcifications or calcifications are mineral deposits that can be found in both non-cancerous and cancerous breast lesions. They can be seen both on mammograms and under the microscope. Most women who have suspicious calcifications do not have cancer. However, certain types of calcifications are found in areas containing cancer. If these are seen on a mammogram, that area may need to be biopsied. Then, when the biopsy is done, the pathologist looks at the tissue removed to be sure that it contains calcifications. If the calcifications are there, the doctor knows that the biopsy sampled the correct area (the abnormal area with calcifications that was seen on the mammogram).
Microcalcifications and calcifications only matter because they are sometimes found in areas containing cancer. When they are found alone (without worrisome changes in the breast ducts or lobules), they do not affect breast cancer risk.
Calcifications that do not appear to be a problem are called benign. No specific follow-up is needed. But, your health care provider may recommend that you get a mammogram each year.
In some cases, calcifications that are slightly abnormal but do not look like a problem (such as cancer) are also called benign. Most women will need to have a follow-up mammogram in 6 months.
Calcifications that are irregular in size or shape or are tightly clustered together, are called suspicious calcifications. Your provider will recommend a stereotactic core biopsy. This is a needle biopsy that uses a type of mammogram machine to help find the calcifications. The purpose of the biopsy is to find out if the calcifications are benign (not cancer) or malignant (cancer).
References- O’Rourke C, Shelton G, Hutcheson JD, et al. Calcification of Vascular Smooth Muscle Cells and Imaging of Aortic Calcification and Inflammation. J Vis Exp. 2016;(111):54017. Published 2016 May 31. doi:10.3791/54017 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4927747
- Otsuka F, Sakakura K, Yahagi K, Joner M, Virmani R. Has our understanding of calcification in human coronary atherosclerosis progressed?. Arterioscler Thromb Vasc Biol. 2014;34(4):724-36. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4095985
- Maldonado N, et al. A mechanistic analysis of the role of microcalcifications in atherosclerotic plaque stability: potential implications for plaque rupture. Am J Physiol Heart Circ Physiol. 2012;303(5):H619–H628
- Aikawa E, et al. Arterial and aortic valve calcification abolished by elastolytic cathepsin S deficiency in chronic renal disease. Circulation. 2009;119(13):1785–1794.
- Toussaint ND, Kerr PG. Vascular calcification and arterial stiffness in chronic kidney disease: implications and management. Nephrology (Carlton) 2007;12(5):500–509
- Budoff MJ, et al. Assessment of coronary artery disease by cardiac computed tomography: a scientific statement from the American Heart Association on Committee on Cardiovascular Imaging and Intervention, Council on Cardiovascular Radiology and Intervention, and Committee on Cardiac Imaging, Council on Clinical Cardiology. Circulation. 2006;114(16):1761–1791
- Vaidya SR, Aeddula NR. Nephrocalcinosis. [Updated 2019 Jan 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537205
- Evan AP, Lingeman JE, Coe FL, Parks JH, Bledsoe SB, Shao Y, Sommer AJ, Paterson RF, Kuo RL, Grynpas M. Randall’s plaque of patients with nephrolithiasis begins in basement membranes of thin loops of Henle. J. Clin. Invest. 2003 Mar;111(5):607-16.
- Vaidya SR, Aeddula NR. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Dec 19, 2018. Chronic Renal Failure.
- Pillai ICL, Li S, Romay M, et al. Cardiac Fibroblasts Adopt Osteogenic Fates and Can Be Targeted to Attenuate Pathological Heart Calcification. Cell Stem Cell. 2016;20(2):218-232.e5. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5291784/
- Inflammatory, metabolic, and genetic mechanisms of vascular calcification. Demer LL, Tintut Y. Arterioscler Thromb Vasc Biol. 2014 Apr; 34(4):715-23.
- Idiopathic massive myocardial calcification: a case report and review of the literature. Shackley BS, Nguyen TP, Shivkumar K, Finn PJ, Fishbein MC. Cardiovasc Pathol. 2011 Mar-Apr; 20(2):e79-83.
- Myocardial calcification and cardiac dysfunction in chronic renal failure. Rostand SG, Sanders C, Kirk KA, Rutsky EA, Fraser RG. Am J Med. 1988 Nov; 85(5):651-7.
- ANATOMIC BASIS FOR ATRIOVENTRICULAR BLOCK. LEV M. Am J Med. 1964 Nov; 37():742-8.
- Myocardial calcification: a predictor of poor outcome for myocarditis treated with extracorporeal life support. Stallion A, Rafferty JF, Warner BW, Ziegler MM, Ryckman FC. J Pediatr Surg. 1994 Apr; 29(4):492-4.
- Fetal cardiac calcifications: report of four prenatally diagnosed cases and review of the literature. Simchen MJ, Toi A, Silver M, Smith CR, Hornberger LK, Taylor G, Chitayat D. Ultrasound Obstet Gynecol. 2006 Mar; 27(3):325-30.
- Mesenchymal-endothelial transition contributes to cardiac neovascularization. Ubil E, Duan J, Pillai IC, Rosa-Garrido M, Wu Y, Bargiacchi F, Lu Y, Stanbouly S, Huang J, Rojas M, Vondriska TM, Stefani E, Deb A. Nature. 2014 Oct 30; 514(7524):585-90.
- Calcium may preferentially deposit in areas of elastic tissue damage. Pugashetti R, Shinkai K, Ruben BS, Grossman ME, Maldonado J, Fox LP. J Am Acad Dermatol. 2011 Feb; 64(2):296-301.
- Calcium deposition with or without bone formation in the lung. Chan ED1, Morales DV, Welsh CH, McDermott MT, Schwarz MI. Am J Respir Crit Care Med. 2002 Jun 15;165(12):1654-69. https://doi.org/10.1164/rccm.2108054
- Winter EM, Pollard AJ, Chapman S, Kelly D, Spencer D. Case report: pulmonary calcification after liver transplantation in children. Br J Radiol 1995;68:923–925.
- Cohen MC, Drut R. Metastatic pulmonary calcification with ossification in a child with acute lymphoblastic leukemia. Pediatr Pulmonol 1999;27:134–137
- Lace PA. An investigation into the aetiological factors concerned in disseminated calcification of the lungs. Med J Aust 1968;23:951–953.
- Sargent EN, Balchum E, Freed AL, Jacobson G. Multiple pulmonary calcifications due to coccidioidomycosis. Am J Roentgenol Radium Ther Nucl Med 1970;109:500–504.
- Katz S, Stanton J, McCormick G. Miliary calcification of the lungs after treated miliary tuberculosis. N Engl J Med 1955;253:135–137.
- Raider L. Calcification in chickenpox pneumonia. Chest 1971;60:504–507.
- Ross PJ, Seaton A, Foreman HM, Evans WHM. Pulmonary calcification following smallpox handler’s lung. Thorax 1974;29:659–665.
- Chen SZ. An analysis of radiologic signs of typical pulmonary calcification in 8 cases of paragonimiasis. Zhonghua Fang She Xue Za Zhi 1984;18:128–130.
- Lee MM, Schinella RA. Pulmonary calcification caused by Pneumocystis carinii pneumonia: a clinicopathological study of 13 cases in acquired immune deficiency syndrome patients. Am J Surg Pathol 1991;15:376–380.
- Israel HL, Sones M, Roy RL, Stein GN. The occurrence of intrathoracic calcification in sarcoidosis. Am Rev Respir Dis 1961;84:1–11.
- Mendlowitz M. Arterial calcium metabolism, hypertension, and arteriosclerosis. Cardiology 1981;67:81–89.
- Schwarz MI, King TE, editors. Interstitial lung disease, 3rd ed. Hamilton, Ontario: B.C. Decker; 1998.
- Livingston, J. H., Stivaros, S. , Warren, D. and Crow, Y. J. (2014), Intracranial calcification in childhood: a review of aetiologies and recognizable phenotypes. Dev Med Child Neurol, 56: 612-626. doi:10.1111/dmcn.12359 https://onlinelibrary.wiley.com/doi/pdf/10.1111/dmcn.12359
- Kendall B, Cavanagh N. Intracranial calcification in paediatric computed tomography. Neuroradiology 1986; 28: 324–30.
- Manyam BV. What is and what is not ‘Fahr’s disease’? Parkinsonism Relat Disord 2005; 11: 73–80.





{kind=link}