Cardiac asthma
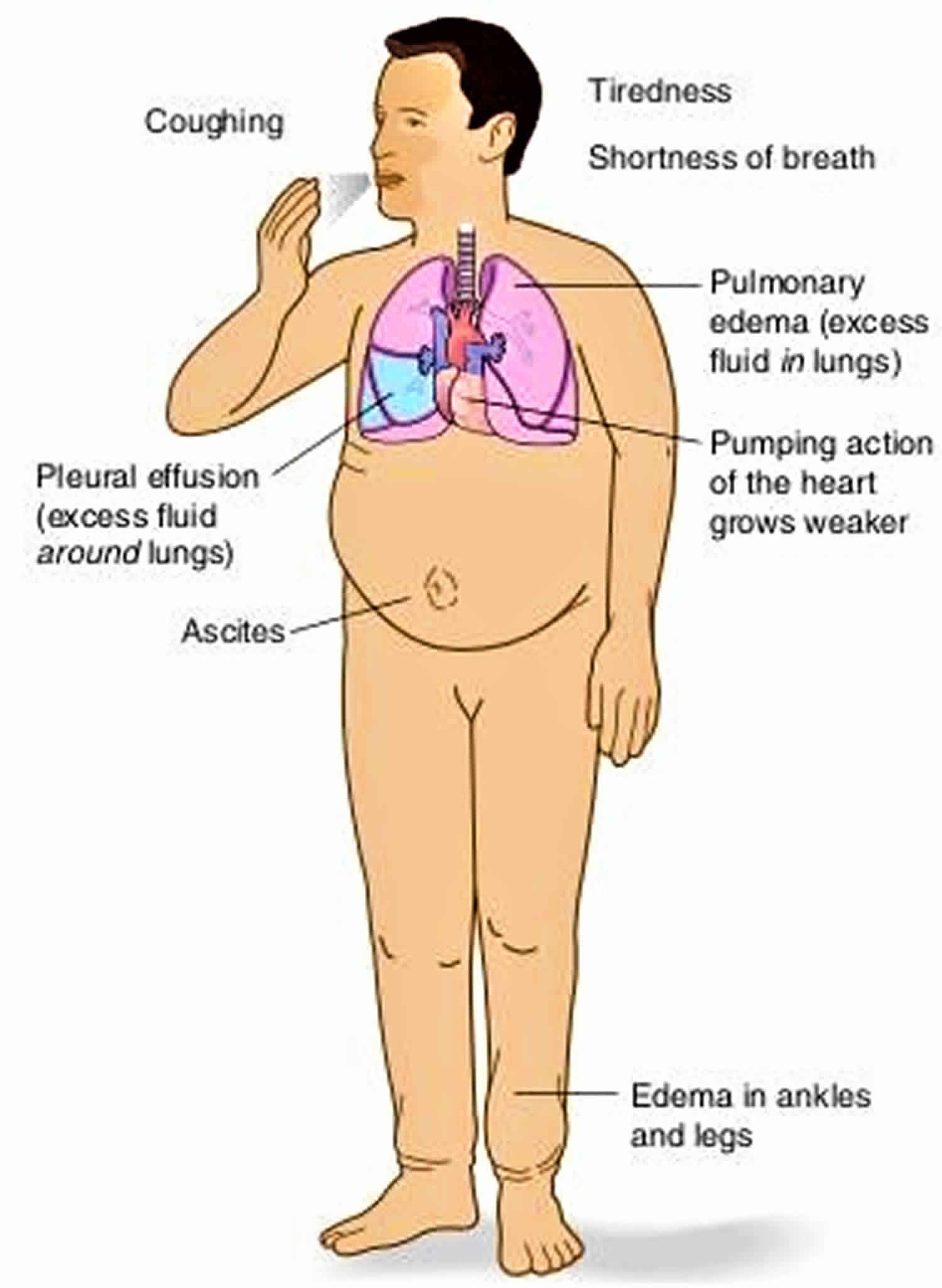
Cardiac asthma is not a form of asthma, but it’s a type of coughing or wheezing that occurs in people with left heart failure. In cardiac asthma, the reduced pumping efficiency of the left side of your heart leads to a build up of fluid in your lungs (pulmonary edema) and in and around your airways. This fluid build-up can cause symptoms such as shortness of breath, coughing and wheezing that may mimic asthma. Cardiac asthma has very similar symptoms to bronchial asthma. Depending on how severe your symptoms are, this wheezing can be a medical emergency.
True asthma is a chronic condition caused by inflammation of the airways, which can narrow them, leading to breathing difficulties. True asthma has nothing to do with fluid in the lungs or heart disease. The distinction is important because treatments for asthma and heart failure are different.
Common causes of heart failure are coronary artery disease, high blood pressure and diabetes. It is more common in people who are 65 years old or older, African Americans, people who are overweight, and people who have had a heart attack. Men have a higher rate of heart failure than women.
Children who have congenital heart defects also can develop heart failure. These defects occur if the heart, heart valves, or blood vessels near the heart don’t form correctly while a baby is in the womb. Congenital heart defects can make the heart work harder. This weakens the heart muscle, which can lead to heart failure. Children don’t have the same symptoms of heart failure or get the same treatments as adults.
About 5.7 million people in the United States have heart failure. The number of people who have this condition is growing.
Heart failure is more common in:
- People who are age 65 or older. Aging can weaken the heart muscle. Older people also may have had diseases for many years that led to heart failure. Heart failure is a leading cause of hospital stays among people on Medicare.
- Blacks are more likely to have heart failure than people of other races. They’re also more likely to have symptoms at a younger age, have more hospital visits due to heart failure, and die from heart failure.
- People who are overweight. Excess weight puts strain on the heart. Being overweight also increases your risk of heart disease and type 2 diabetes. These diseases can lead to heart failure.
- People who have had a heart attack. Damage to the heart muscle from a heart attack and can weaken the heart muscle.
Your doctor will diagnose heart failure by doing a physical exam and heart tests. Treatment includes treating the underlying cause of your heart failure, medicines, and heart transplantation if other treatments fail.
Treatments for heart failure can help improve your symptoms for both the heart failure and the cardiac asthma. Overusing treatments for true asthma, such as rescue inhalers, could be dangerous and lead to a worsening of symptoms.
Cardiac asthma causes
Cardiac asthma it’s a type of coughing or wheezing that occurs in people with left heart failure.
Heart failure is a condition in which the heart can’t pump enough blood to meet your body’s needs. Heart failure does not mean that your heart has stopped or is about to stop working. It means that your heart is not able to pump blood the way it should. It can affect one or both sides of the heart.
Heart failure is a serious condition that requires medical care.
Right-side heart failure occurs if the heart can’t pump enough blood to the lungs to pick up oxygen. Left-side heart failure occurs if the heart can’t pump enough oxygen-rich blood to the rest of the body.
Right-side heart failure may cause fluid to build up in the feet, ankles, legs, liver, abdomen, and the veins in the neck. Right-side and left-side heart failure also may cause shortness of breath and fatigue (tiredness).
The weakening of the heart’s pumping ability causes:
- Blood and fluid to back up into the lungs
- The buildup of fluid in the feet, ankles and legs – called edema
- Tiredness and shortness of breath
Heart failure causes
Conditions that damage or overwork the heart muscle can cause heart failure. Over time, the heart weakens. Your heart isn’t able to fill with and/or pump blood as well as it should. As the heart weakens, certain proteins and substances might be released into the blood. These substances have a toxic effect on the heart and blood flow, and they worsen heart failure.
Causes of heart failure include:
- Ischemic heart disease
- Diabetes
- High blood pressure
- Other heart conditions or diseases
- Other factors
Ischemic heart disease
Ischemic heart disease is a condition in which a waxy substance called plaque builds up inside the coronary arteries. These arteries supply oxygen-rich blood to your heart muscle.
Plaque narrows the arteries and reduces blood flow to your heart muscle. The buildup of plaque also makes it more likely that blood clots will form in your arteries. Blood clots can partially or completely block blood flow. Ischemic heart disease can lead to chest pain or discomfort called angina, a heart attack, and heart damage.
Diabetes
Diabetes is a disease in which the body’s blood glucose (sugar) level is too high. The body normally breaks down food into glucose and then carries it to cells throughout the body. The cells use a hormone called insulin to turn the glucose into energy.
In diabetes, the body doesn’t make enough insulin or doesn’t use its insulin properly. Over time, high blood sugar levels can damage and weaken the heart muscle and the blood vessels around the heart, leading to heart failure.
High blood pressure
Blood pressure is the force of blood pushing against the walls of the arteries. If this pressure rises and stays high over time, it can weaken your heart and lead to plaque buildup.
Blood pressure is considered high if it stays at or above 140/90 mmHg over time. (The mmHg is millimeters of mercury—the units used to measure blood pressure.) If you have diabetes or chronic kidney disease, high blood pressure is defined as 130/80 mmHg or higher.
Other heart conditions or diseases
Other conditions and diseases also can lead to heart failure, such as:
- Arrhythmia. Happens when a problem occurs with the rate or rhythm of the heartbeat.
- Cardiomyopathy. Happens when the heart muscle becomes enlarged, thick, or rigid.
- Congenital heart defects. Problems with the heart’s structure are present at birth.
- Heart valve disease. Occurs if one or more of your heart valves doesn’t work properly, which can be present at birth or caused by infection, other heart conditions, and age.
Other factors
Other factors also can injure the heart muscle and lead to heart failure. Examples include:
- Alcohol abuse or cocaine and other illegal drug use
- HIV/AIDS
- Thyroid disorders (having either too much or too little thyroid hormone in the body)
- Too much vitamin E
- Treatments for cancer, such as radiation and chemotherapy.
Cardiac asthma pathophysiology
In congestive heart failure, the heart’s inability to pump blood out of the left ventricle results in excess fluid in the pulmonary circulation 1. Pulmonary congestion is the consequence of fluid being pushed into the alveolar lumen. Cardiac asthma may be associated with bronchiolar pathology, rather than simply the accumulation of alveolar fluid.
Not only does the presence of fluid in the lungs make breathing difficult, it can cause asthmalike symptoms as well. The wheezing experienced by congestive heart failure patients may be due to a narrowing or obstruction of the bronchioles rather than simply to pulmonary congestion. Various studies have identified bronchial hyperreactivity as the mechanism behind cardiac asthma 2. Patients in these studies inhaled either acetylcholine or methacholine (cholinergic agonists). Compared with patients without cardiac asthma symptoms, those with symptoms demonstrated greater airway narrowing in response to the inhaled drug. The mechanism by which this narrowing occurs is not fully understood. Another study suggested that downregulation of beta2 receptors resulting from excessive adrenergic stimulation might cause bronchoconstriction in heart failure patients 3. Either mechanism is detrimental and undesirable in patients already experiencing pulmonary congestion.
Cardiac asthma may be better attributed to bronchial anatomy. The bronchial blood supply involves a separate vascular system from that which supplies the alveoli. Similar to the mechanism of fluid buildup in the alveoli, the blood supply to the bronchioles may exhibit fluid buildup. Two hypotheses exist regarding the pathophysiology behind this: theory A and theory B 1. Theory A hypothesizes that an increase in blood flow to the bronchial circulation may produce edema in the interstitial space, thereby squeezing the bronchiolar lumen 1. Conversely, theory B posits that certain pathological changes in heart failure, including pulmonary edema (PE), may compete for interthoracic space, compressing the entire airway structure and the bronchiole wall 1.
The pathologic cause of cardiac asthma is not definitively explained. Reflex bronchoconstriction involving the vagus nerve has been suggested. Increased pulmonary vascular pressure may stimulate afferent nerve endings, causing reflex narrowing of large and small airways 4. Reflex bronchoconstriction, in addition to edema and hyperreactivity, can exponentially reduce breathing capability in congestive heart failure patients. The pathophysiology of cardiac asthma may incorporate a combination of mechanisms, creating a number of treatment challenges. The absence of inflammation is the major difference between cardiac asthma and bronchial asthma, even though the symptoms are similar.
Cardiac asthma symptoms
As noted earlier, cardiac asthma involves symptoms of airflow obstruction that are due to heart failure 5. In most cases, the clinical presentation includes severe dyspnea (shortness of breath), cough, frothy or watery sputum, and rales, but the most significant symptom indicative of cardiac asthma is wheezing 6. These symptoms are more prevalent in elderly patients 6.
Cardiac asthma often is characterized by abrupt waking from sleep caused by sudden, severe episodes of dyspnea 6. In a typical attack, the symptoms generally subside after the patient sits upright for 20 to 30 minutes, after which he or she may be able to return to bed without needing medication 7. In severe cases, the patient may experience recurrent episodes in a single night and have cyanosis (blue or purple discoloration of the skin), cold sweats, blood-tinged sputum, and fluid buildup in the lungs 7. Cardiac asthma is difficult to diagnose because its symptoms are similar to those of bronchial asthma 5.
Since cardiac asthma stems from a heart problem, it can be difficult to distinguish its symptoms from those of heart failure. The three cardinal symptoms of heart failure are dyspnea, fatigue, and fluid retention; the presence of wheezing is diagnostic of cardiac asthma 8. Chronic heart failure often is associated with decreased forced expiratory volume in 1 second (FEV1); however, in one study, cardiac asthma patients (defined as having congestive heart failure and wheezing) exhibited lower FEV1 values than patients with congestive heart failure alone 5. Chest x-ray is useful for confirming the presence of pulmonary congestion as well as for identifying cardiomegaly, which also indicates a heart disorder 4. Cardiomegaly often occurs in cardiac asthma patients, but not to the same degree as in strictly heart failure patients 9. Physical examination and lung auscultation may reveal rales, which are attributable to pulmonary edema, but the best way to diagnose heart failure is to obtain a two-dimensional echocardiogram with Doppler, which can identify structural abnormalities and reduced ejection fraction (EF) 10.
The main symptoms and signs of cardiac asthma are:
- shortness of breath with or without wheezing;
- cough;
- rapid and shallow breathing;
- an increase in blood pressure and heart rate; and
- a feeling of apprehension.
The pattern of shortness of breath helps doctors determine which type of asthma you have — people with bronchial asthma tend to experience shortness of breath early in the morning, whereas people with heart failure and cardiac asthma often find they wake up breathless a few hours after going to bed, and have to sit upright to catch their breath. This is because in people with heart failure, lying down for prolonged periods will cause fluid to accumulate in the lungs leading to shortness of breath.
Both bronchial and cardiac asthma can make people short of breath when they exert themselves. In bronchial asthma, symptoms are usually brought on by vigorous exercise and tend to be worse after the exercise than during it. On the other hand, cardiac asthma tends to happen during less vigorous exertion — someone with heart failure can find themselves short of breath while climbing stairs, or in severe cases, while getting dressed.
People with heart failure also often have problems with swollen ankles that worsen during the course of the day. They may also feel very tired, put on weight and have to urinate frequently.
Cardiac asthma can be a life-threatening condition, and you should consult your doctor if you think you have symptoms of cardiac asthma.
Cardiac asthma diagnosis
Your doctor will diagnose heart failure based on your medical and family histories, a physical exam, and test results. The signs and symptoms of heart failure also are common in other conditions. Thus, your doctor will take these steps:
- Find out whether you have a disease or condition that can cause heart failure, such as ischemic heart disease, high blood pressure, or diabetes.
- Rule out other causes of your symptoms.
- Find any damage to your heart and check how well your heart pumps blood.
Early diagnosis and treatment can help people who have heart failure live longer, more active lives.
Medical and family histories
Your doctor will ask whether you or others in your family have or have had a disease or condition that can cause heart failure.
Your doctor also will ask about your symptoms. He or she will want to know which symptoms you have, when they occur, how long you’ve had them, and how severe they are. Your answers will help show whether and how much your symptoms limit your daily routine.
Physical exam
During the physical exam, your doctor will:
- Listen to your heart for sounds that aren’t normal
- Listen to your lungs for the sounds of extra fluid buildup
- Look for swelling in your ankles, feet, legs, abdomen, and the veins in your neck
Diagnostic tests
No single test can diagnose heart failure. If you have signs and symptoms of heart failure, your doctor may recommend one or more tests.
Your doctor also may refer you to a cardiologist. A cardiologist is a doctor who specializes in diagnosing and treating heart diseases and conditions.
EKG (Electrocardiogram)
An EKG is a simple, painless test that detects and records the heart’s electrical activity. The test shows how fast your heart is beating and its rhythm (steady or irregular). An EKG also records the strength and timing of electrical signals as they pass through your heart.
An EKG may show whether the walls in your heart’s pumping chambers are thicker than normal. Thicker walls can make it harder for your heart to pump blood. An EKG also can show signs of a previous or current heart attack.
Chest X Ray
A chest x ray takes pictures of the structures inside your chest, such as your heart, lungs, and blood vessels. This test can show whether your heart is enlarged, you have fluid in your lungs, or you have lung disease.
BNP blood test
This test checks the level of a hormone in your blood called BNP. The level of this hormone rises during heart failure.
Echocardiography
Echocardiography (echo) uses sound waves to create a moving picture of your heart. The test shows the size and shape of your heart and how well your heart chambers and valves work.
Echo also can identify areas of poor blood flow to the heart, areas of heart muscle that aren’t contracting normally, and heart muscle damage caused by lack of blood flow.
Echo might be done before and after a stress test (see below). A stress echo can show how well blood is flowing through your heart. The test also can show how well your heart pumps blood when it beats.
Doppler ultrasound
A Doppler ultrasound uses sound waves to measure the speed and direction of blood flow. This test often is done with echo to give a more complete picture of blood flow to the heart and lungs.
Doctors often use Doppler ultrasound to help diagnose right-side heart failure.
Holter monitor
A Holter monitor records your heart’s electrical activity for a full 24- or 48-hour period, while you go about your normal daily routine.
You wear small patches called electrodes on your chest. Wires connect the patches to a small, portable recorder. The recorder can be clipped to a belt, kept in a pocket, or hung around your neck.
Nuclear Heart Scan
A nuclear heart scan shows how well blood is flowing through your heart and how much blood is reaching your heart muscle.
During a nuclear heart scan, a safe, radioactive substance called a tracer is injected into your bloodstream through a vein. The tracer travels to your heart and releases energy. Special cameras outside of your body detect the energy and use it to create pictures of your heart.
A nuclear heart scan can show where the heart muscle is healthy and where it’s damaged.
A positron emission tomography (PET) scan is a type of nuclear heart scan. It shows the level of chemical activity in areas of your heart. This test can help your doctor see whether enough blood is flowing to these areas. A PET scan can show blood flow problems that other tests might not detect.
Cardiac catheterization
During cardiac catheterization, a long, thin, flexible tube called a catheter is put into a blood vessel in your arm, groin (upper thigh), or neck and threaded to your heart. This allows your doctor to look inside your coronary (heart) arteries.
During this procedure, your doctor can check the pressure and blood flow in your heart chambers, collect blood samples, and use x rays to look at your coronary arteries.
Coronary angiography
Coronary angiography usually is done with cardiac catheterization. A dye that can be seen on x ray is injected into your bloodstream through the tip of the catheter.
The dye allows your doctor to see the flow of blood to your heart muscle. Angiography also shows how well your heart is pumping.
Stress test
Some heart problems are easier to diagnose when your heart is working hard and beating fast. During stress testing, you exercise to make your heart work hard and beat fast.
You may walk or run on a treadmill or pedal a bicycle. If you can’t exercise, you may be given medicine to raise your heart rate.
Heart tests, such as nuclear heart scanning and echo, often are done during stress testing.
Cardiac MRI
Cardiac MRI (magnetic resonance imaging) uses radio waves, magnets, and a computer to create pictures of your heart as it’s beating. The test produces both still and moving pictures of your heart and major blood vessels.
A cardiac MRI can show whether parts of your heart are damaged. Doctors also have used MRI in research studies to find early signs of heart failure, even before symptoms appear.
Thyroid function tests
Thyroid function tests show how well your thyroid gland is working. These tests include blood tests, imaging tests, and tests to stimulate the thyroid. Having too much or too little thyroid hormone in the blood can lead to heart failure.
Classifying heart failure
Results of these tests help doctors determine the cause of your signs and symptoms and develop a program to treat your heart. To determine the most appropriate treatment for your condition, doctors may classify heart failure using two systems:
- New York Heart Association classification. This symptom-based scale classifies heart failure in four categories. In Class I heart failure, you don’t have any symptoms. In Class II heart failure, you can perform everyday activities without difficulty but become winded or fatigued when you exert yourself. With Class III, you’ll have trouble completing everyday activities, and Class IV is the most severe, and you’re short of breath even at rest.
- American College of Cardiology/American Heart Association guidelines. This stage-based classification system uses letters A to D. The system includes a category for people who are at risk of developing heart failure. For example, a person who has several risk factors for heart failure but no signs or symptoms of heart failure is Stage A. A person who has heart disease but no signs or symptoms of heart failure is Stage B. Someone who has heart disease and is experiencing or has experienced signs or symptoms of heart failure is Stage C. A person with advanced heart failure requiring specialized treatments is Stage D. Doctors use this classification system to identify your risk factors and begin early, more aggressive treatment to help prevent or delay heart failure.
These scoring systems are not independent of each other. Your doctor often will use them together to help decide your most appropriate treatment options. Ask your doctor about your score if you’re interested in determining the severity of your heart failure. Your doctor can help you interpret your score and plan your treatment based on your condition.
Cardiac asthma treatment
Currently, no well-defined treatment plans exist for cardiac asthma in the acute or chronic setting 11. Discussions of cardiac asthma management target the pathophysiology of the underlying condition (i.e., pulmonary edema and heart failure). The use and efficacy of bronchodilators such as albuterol and ipratropium, which are used to relieve symptoms of bronchial asthma, have not been established in cardiac asthma 9.
Traditional medications used in the acute treatment of cardiac asthma include furosemide, morphine, and nitrates (see medicines below) 12. Supplemental oxygen, noninvasive ventilation and proper positioning of the patient also are important 13. Each treatment has a unique benefit and may work synergistically with other treatments. Because patients presenting with an acute episode of cardiac asthma usually are hypoxic, the initial use of oxygen and/or noninvasive ventilation is recommended and has been shown to decrease mortality 14. If the patient shows no signs of hypoxia, oxygen and noninvasive ventilation are not recommended. A patient who awakens at night with shortness of breath (dyspnea) may alleviate symptoms by remaining awake for 20 to 30 minutes 11. Proper positioning, in which the patient stands erect or sits upright with feet hanging off the side of the bed, will result in decreased venous return. The amount of blood to the bronchioles is thereby lessened, interstitial-space edema is reduced, and the squeezing effect of the bronchiolar lumen described in theory A is diminished 13. Theory A hypothesizes that an increase in blood flow to the bronchial circulation may produce edema in the interstitial space, thereby squeezing the bronchiolar lumen 1.
Patients experiencing an acute cardiac asthma episode likely will require fluid removal. In such cases, gradual diuresis using a loop diuretic is warranted. Furosemide, which acts at the ascending portion of the loop of Henle and at the distal tubule, inhibits the reabsorption of sodium and chloride and causes diuresis 14. This improves symptoms by reducing preload in the heart. Symptomatic improvement in patients with pulmonary congestion is seen with an initial recommended furosemide dosage of 40 mg IV 14. The dose may be increased based on clinical response but must remain gradual to avoid hypotension, electrolyte disturbances, gout exacerbations, hearing loss (reversible), and worsening renal function 14.
Some patients may exhibit persistent pulmonary congestion despite aggressive diuresis. In these instances, an IV nitrate (e.g., nitroglycerin) may be used adjunctively in both hypertensive and normotensive patients. Acting as a venodilator, nitroglycerin will lessen the pressure in the left ventricle, thereby reducing pulmonary congestion 14. Nitroglycerin should be started at a dosage of 5 mcg/min; it may be titrated to 200 mcg/min. Nitroglycerin dosing beyond 200 mcg/min is not recommended, and the patient requiring it should be considered a nonresponde 14. Some side effects associated with nitroglycerin use are hypotension, headache, and abdominal pain.
IV morphine ameliorates symptoms in patients with pulmonary congestion 15. Morphine used in the setting of cardiac asthma enables easier breathing and reduces a patient’s anxiety level during the episode 14. The mechanism by which easier breathing occurs is believed to involve venodilation and reduction in preload 14. The morphine dosage commonly used is 1 to 3 mg IV every 5 minutes until relief occurs without inducing respiratory depression 14.
Once the acute cardiac asthma episode is resolved, heart failure therapy should be initiated or optimized to prevent future occurrences. The use of ACE inhibitors and beta-blockers in heart failure patients is recommended to decrease morbidity and mortality rates 14. The continuance of diuretics postepisode will help maintain a normal volume status in this patient population and prevent future cardiac asthma occurrences. Digoxin, although not shown to reduce mortality, may be used to improve congestive symptoms in patients with heart failure. Additional information about chronic heart failure management, including anticoagulation, amiodarone use, alternative treatments, dosing, and so on, may be found in current heart failure practice guidelines 14.
Heart failure treatment
Early diagnosis and treatment can help people who have heart failure live longer, more active lives. Treatment for heart failure depends on the type and severity of the heart failure.
The goals of treatment for all stages of heart failure include:
- Treating the condition’s underlying cause, such as ischemic heart disease, high blood pressure, or diabetes
- Reducing symptoms
- Stopping the heart failure from getting worse
- Increasing your lifespan and improving your quality of life
Treatments usually include heart-healthy lifestyle changes, medicines, and ongoing care. If you have severe heart failure, you also may need medical procedures or surgery.
Heart-healthy lifestyle changes
Your doctor may recommend heart-healthy lifestyle changes if you have heart failure. Heart-healthy lifestyle changes include:
- Heart-healthy eating
- Aiming for a healthy weight
- Physical activity
- Quitting smoking
Medicines
Your doctor will prescribe medicines based on the type of heart failure you have, how severe it is, and your response to certain medicines. The following medicines are commonly used to treat heart failure:
- Angiotensin-converting enzyme (ACE) inhibitors. ACE inhibitors lower blood pressure and reduce strain on your heart. These drugs help people with systolic heart failure live longer and feel better. ACE inhibitors also may reduce the risk of a future heart attack. ACE inhibitors are a type of vasodilator, a drug that widens blood vessels to lower blood pressure, improve blood flow and decrease the workload on the heart. Examples include enalapril (Vasotec), lisinopril (Zestril) and captopril (Capoten).
- Aldosterone antagonists. These drugs include spironolactone (Aldactone) and eplerenone (Inspra). Aldosterone antagonists trigger the body to remove excess sodium through urine. This lowers the volume of blood that the heart must pump. Aldosterone antagonists are potassium-sparing diuretics, which also have additional properties that may help people with severe systolic heart failure live longer. Unlike some other diuretics, spironolactone and eplerenone can raise the level of potassium in your blood to dangerous levels, so talk to your doctor if increased potassium is a concern, and learn if you need to modify your intake of food that’s high in potassium.
- Angiotensin II receptor blockers. Angiotensin receptor blockers, which include losartan (Cozaar) and valsartan (Diovan), have many of the same benefits as ACE inhibitors. They may be an alternative for people who can’t tolerate ACE inhibitors. Angiotensin receptor blockers relax your blood vessels and lower blood pressure to decrease your heart’s workload.
- Beta blockers. Beta blockers not only slow your heart rate and reduce blood pressure to decrease your heart’s workload but also limit or reverse some of the damage to your heart if you have systolic heart failure. Examples include carvedilol (Coreg), metoprolol (Lopressor) and bisoprolol (Zebeta). These medicines reduce the risk of some abnormal heart rhythms and lessen your chance of dying unexpectedly. Beta blockers may reduce signs and symptoms of heart failure, improve heart function, and help you live longer.
- Digoxin (Lanoxin). Digoxin also referred to as digitalis, increases the strength of your heart muscle contractions, making your heart beat stronger and pump more blood. Digoxin also tends to slow the heartbeat. Digoxin reduces heart failure symptoms in systolic heart failure. Digoxin may be more likely to be given to someone with a heart rhythm problem, such as atrial fibrillation.
- Diuretics. Often called water pills, diuretics make you urinate more frequently and keep fluid from collecting in your lungs and swelling in your feet and ankles. Diuretics, such as furosemide (Lasix), also decrease fluid in your lungs so you can breathe more easily. Because diuretics make your body lose potassium and magnesium, your doctor may also prescribe supplements of these minerals. If you’re taking a diuretic, your doctor will likely monitor levels of potassium and magnesium in your blood through regular blood tests.
- Inotropes. These are intravenous medications used in people with severe heart failure in the hospital to improve heart pumping function and maintain blood pressure.
- Isosorbide dinitrate/hydralazine hydrochloride helps relax your blood vessels so your heart doesn’t work as hard to pump blood. Studies have shown that this medicine can reduce the risk of death in blacks. More studies are needed to find out whether this medicine will benefit other racial groups.
Take all medicines regularly, as your doctor prescribes. Don’t change the amount of your medicine or skip a dose unless your doctor tells you to. You should still follow a heart healthy lifestyle, even if you take medicines to treat your heart failure.
Ongoing care
You should watch for signs that heart failure is getting worse. For example, weight gain may mean that fluids are building up in your body. Ask your doctor how often you should check your weight and when to report weight changes.
Getting medical care for other related conditions is important. If you have diabetes or high blood pressure, work with your health care team to control these conditions. Have your blood sugar level and blood pressure checked. Talk with your doctor about when you should have tests and how often to take measurements at home.
Try to avoid respiratory infections like the flu and pneumonia. Talk with your doctor or nurse about getting flu and pneumonia vaccines.
Many people who have severe heart failure may need treatment in a hospital from time to time. Your doctor may recommend oxygen therapy, which can be given in a hospital or at home.
Medical procedures and surgery
As heart failure worsens, lifestyle changes and medicines may no longer control your symptoms. You may need a medical procedure or surgery.
In heart failure, the right and left sides of the heart may no longer contract at the same time. This disrupts the heart’s pumping. To correct this problem, your doctor might implant a cardiac resynchronization therapy device (a type of pacemaker) near your heart. This device helps both sides of your heart contract at the same time, which can decrease heart failure symptoms.
Some people who have heart failure have very rapid, irregular heartbeats. Without treatment, these heartbeats can cause sudden cardiac arrest. Your doctor might implant an implantable cardioverter defibrillator (ICD) near your heart to solve this problem. An ICD checks your heart rate and uses electrical pulses to correct irregular heart rhythms.
People who have severe heart failure symptoms at rest, despite other treatments, may need:
- A mechanical heart pump, such as a left ventricular assist device. This device helps pump blood from the heart to the rest of the body. You may use a heart pump until you have surgery or as a long-term treatment.
- Heart transplant. A heart transplant is an operation in which a person’s diseased heart is replaced with a healthy heart from a deceased donor. Heart transplants are done as a life-saving measure for end-stage heart failure when medical treatment and less drastic surgery have failed.
Living with heart failure
Currently, heart failure has no cure. You’ll likely have to take medicine and follow a treatment plan for the rest of your life.
Despite treatment, symptoms may get worse over time. You may not be able to do many of the things that you did before you had heart failure. However, if you take all the steps your doctor recommends, you can stay healthier longer.
Researchers also might find new treatments that can help you in the future.
Follow your treatment plan
Treatment can relieve your symptoms and make daily activities easier. It also can reduce the chance that you’ll have to go to the hospital. Thus, it’s important that you follow your treatment plan.
- Take your medicines as your doctor prescribes. If you have side effects from any of your medicines, tell your doctor. He or she might adjust the dose or type of medicine you take to relieve side effects.
- Make all of the lifestyle changes that your doctor recommends.
- Get advice from your doctor about how active you can and should be. This includes advice on daily activities, work, leisure time, sex, and exercise. Your level of activity will depend on the stage of your heart failure (how severe it is).
- Keep all of your medical appointments, including visits to the doctor and appointments to get tests and lab work. Your doctor needs the results of these tests to adjust your medicine doses and help you avoid harmful side effects.
Take steps to prevent heart failure from getting worse
Certain actions can worsen your heart failure, such as:
- Forgetting to take your medicines
- Not following your diet (for example, eating salty foods)
- Drinking alcohol
These actions can lead to a hospital stay. If you have trouble following your diet, talk with your doctor. He or she can help arrange for a dietitian to work with you. Avoid drinking alcohol.
People who have heart failure often have other serious conditions that require ongoing treatment. If you have other serious conditions, you’re likely taking medicines for them as well as for heart failure.
Taking more than one medicine raises the risk of side effects and other problems. Make sure your doctors and your pharmacist have a complete list of all of the medicines and over-the-counter products that you’re taking.
Tell your doctor right away about any problems with your medicines. Also, talk with your doctor before taking any new medicine prescribed by another doctor or any new over-the-counter medicines or herbal supplements.
Try to avoid respiratory infections like the flu and pneumonia. Ask your doctor or nurse about getting flu and pneumonia vaccines.
Plan ahead
If you have heart failure, it’s important to know:
- When to seek help. Ask your doctor when to make an office visit or get emergency care.
- Phone numbers for your doctor and hospital.
- Directions to your doctor’s office and hospital and people who can take you there.
- A list of medicines you’re taking.
Emotional issues and support
Living with heart failure may cause fear, anxiety, depression, and stress. Talk about how you feel with your health care team. Talking to a professional counselor also can help. If you’re very depressed, your doctor may recommend medicines or other treatments that can improve your quality of life.
Joining a patient support group may help you adjust to living with heart failure. You can see how other people who have the same symptoms have coped with them. Talk with your doctor about local support groups or check with an area medical center.
Support from family and friends also can help relieve stress and anxiety. Let your loved ones know how you feel and what they can do to help you.
Palliative care and end-of-life care
Your doctor may recommend including palliative care in your treatment plan. Palliative care is specialized medical care that focuses on easing your symptoms and improving your quality of life. Anyone who has a serious or life-threatening illness can benefit from palliative care, either to treat symptoms of the disease, such as pain or shortness of breath, or to ease the side effects of treatment, such as fatigue or nausea.
It’s possible that your heart failure may worsen to the point where medications are no longer working and a heart transplant or device isn’t an option. If this occurs, you may need to enter hospice care. Hospice care provides a special course of treatment to terminally ill people.
Hospice care allows family and friends — with the aid of nurses, social workers and trained volunteers — to care for and comfort a loved one at home or in hospice residences. Hospice care provides emotional, psychological, social and spiritual support for people who are ill and those closest to them.
Although most people under hospice care remain in their own homes, the program is available anywhere — including nursing homes and assisted living centers. For people who stay in a hospital, specialists in end-of-life care can provide comfort, compassionate care and dignity.
Although it can be difficult, discuss end-of-life issues with your family and medical team. Part of this discussion will likely involve advance directives — a general term for oral and written instructions you give concerning your medical care should you become unable to speak for yourself.
If you have an implantable cardioverter-defibrillator (ICD), one important consideration to discuss with your family and doctors is turning off the defibrillator so that it can’t deliver shocks to make your heart continue beating.
References- Ceridon M, Wanner A, Johnson BD. Does the bronchial circulation contribute to congestion in heart failure? Med Hypotheses. 2009;73:414-419.
- Nishimura Y, Yu Y, Kotani Y, et al. Bronchial hyperresponsiveness and exhaled nitric oxide in patients with cardiac disease. Respiration. 2001;68:41-45.
- Borst M, Beuthien W, Schwencke C, et al. Desensitization of the pulmonary adenylyl cyclase system: a cause of airway hyperresponsiveness in congestive heart failure? J Am Coll Cardiol. 1999;34:848-856.
- Snashall PD, Chung KF. Airway obstruction and bronchial hyperresponsiveness in left ventricular failure and mitral stenosis. Am Rev Respir Dis. 1991;144:945-956.
- Tanabe T, Kanoh S, Moskowitz WB, Rubin BK. Cardiac asthma: transforming growth factor-ß from the failing heart leads to squamous metaplasia in human airway cells and in the murine lung. Chest. 2012;142:1274-1283.
- Lombardo TA, Harrison TR. Cardiac asthma. Circulation. 1951;4:920-929.
- Hamilton JG. Cardiac asthma. Br Med J. 1955;1:39-41.
- Hunt SA, Abraham WT, Chin MH, et al. 2009 focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation. 2009;119:e391-e479
- Jorge S, Becquemin MH, Delerme S, et al. Cardiac asthma in elderly patients: incidence, clinical presentation and outcome. BMC Cardiovasc Disord. 2007;7:16.
- Jessup M, Abraham WT, Casey DE, et al. 2009 focused update: ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation. 2009;119:1977-2016.
- Cardiac Asthma: Not Your Typical Asthma. https://www.uspharmacist.com/article/cardiac-asthma-not-your-typical-asthma
- National Asthma Education and Prevention Program. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. Bethesda, MD: National Heart, Lung, and Blood Institute; 2007. NIH Publication No. 08-5846.
- Sabatine M. Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011:15.
- Lindenfeld J, Albert NM, Boehmer JP, et al. HFSA 2010 Comprehensive Heart Failure Practice Guideline. J Card Fail. 2010;16:e1-194.
- Nieminen MS, Böhm M, Cowie MR, et al. Executive summary of the guidelines on the diagnosis and treatment of acute heart failure. Eur Heart J. 2005;26:384-416.





{kind=link}