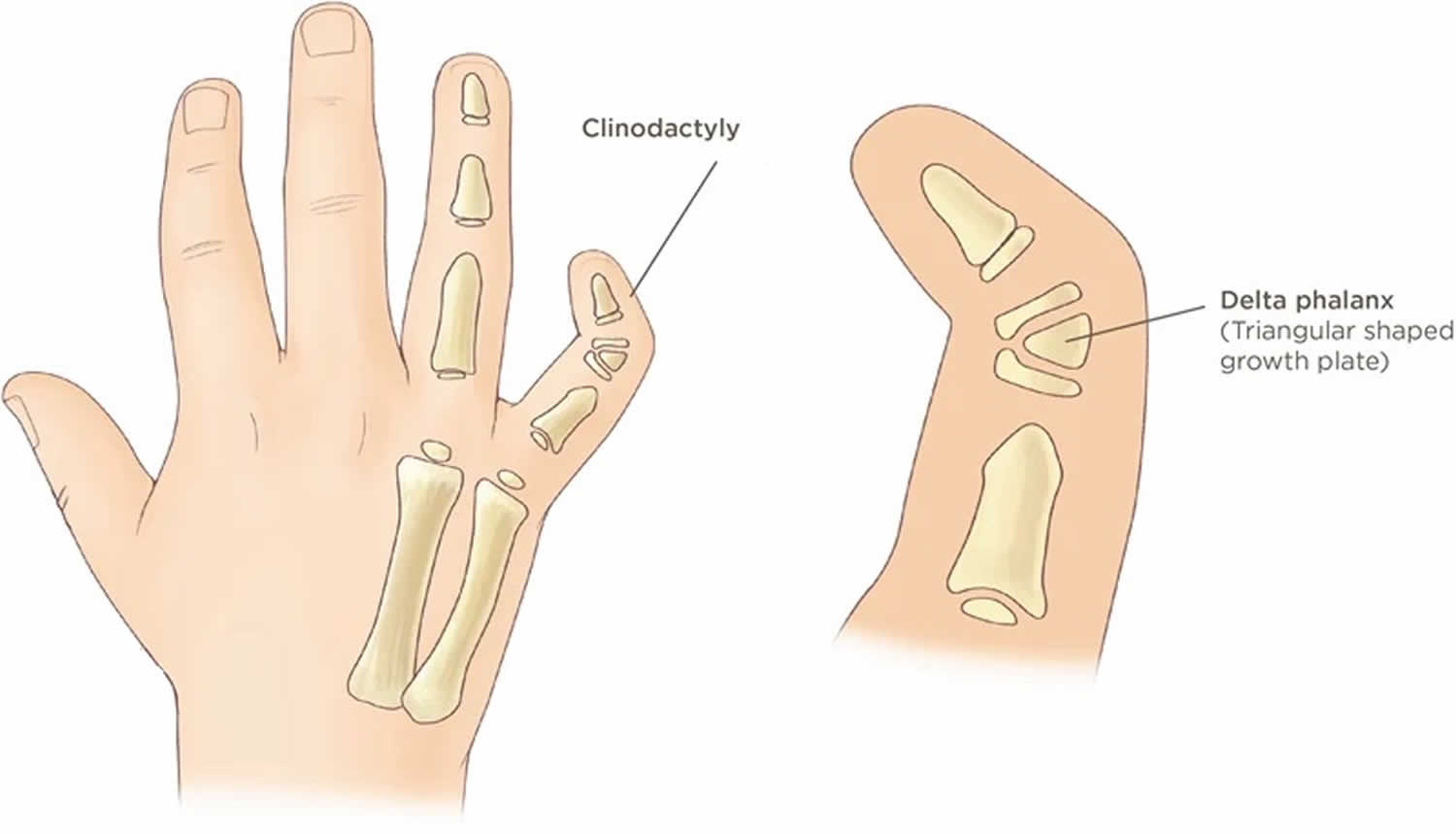
Clinodactyly
Clinodactyly is when a finger or toe curves toward the finger or toe next to it, not up or down. Clinodactyly is a medical term that refers to a radial angulation at an interphalangeal joint in the radio-ulnar or palmar planes 1. Clinodactyly can happen in any finger or toe, but the most common type is when the 5th finger curves toward the ring finger. Clinodactyly may get worse with age. The estimated incidence of clinodactyly is highly variable dependent on sampling and has been reported to range between 1% to 18%. Clinodactyly affects about one in four children born with Down syndrome (trisomy 21).
Unless the curved finger is severe, clinodactyly may go unnoticed for years. The condition doesn’t cause pain and in most cases, does not affect hand function.
Clinodactyly is a congenital condition, meaning it is present at birth even if it is not discovered until later. Clinodactyly can be inherited or your child may be the first person in your family to have the condition. Clinodactyly can also be a symptom of an associated syndrome.
Clinodactyly is typically caused by the growth of an abnormally shaped bone in your child’s finger, which causes the finger to curve to the side. It may also be due to an irregular growth plate in one of the bones of your child’s finger.
Treatment for clinodactyly varies depends on the severity of the condition, but can include ongoing monitoring and surgery.
Figure 1. Clinodactyly pinky finger

Clinodactyly causes
Clinodactly can result from vast number pathologies ranging from congenital to acquired. There may be a growth plate on one side of the bone that causes the bone to grow longer on one side than the other. The bone doesn’t grow in the normal shape of a rectangle, but rather more like a triangle.
- Clinodactyly might be a genetic condition (it can run in families with an autosomal recessive inheritance).
- Clinodactyly might be a part of a syndrome (a specific group of symptoms):
- Aneuploidic syndrome
- Down syndrome: About 35-70% of children with Down syndrome have clinodactyly 2
- Klinefelter syndrome
- trisomy 18
- Turner syndrome
- Non aneupliodic syndrome
- Cornelia de Lange syndrome
- Feingold syndrome
- Roberts syndrome
- Russell-Silver syndrome 2
- Fanconi anemia
- Non syndromic
- macrodystrophia lipomatosa
- brachydactyly type A3
- Aneuploidic syndrome
Clinodactyly signs and symptoms
The primary symptom of clinodactyly is a finger that is abnormally curved in the middle. It may overlap with other fingers on the hand. In most cases, the condition does not cause pain, swelling or inflammation.
If your child’s clinodactyly finger includes a curve of more than 30 degrees, it may affect their hand function.
Clinodactyly diagnosis
Clinodactyly is diagnosed by examination. In most cases, clinicians will recommend an X-ray to look at the bones of the fingers/toes and to confirm the diagnosis. X-rays produce images of bones and help doctors identify the underlying structure of the hand. In the case of clinodactyly, a distinctive c-shaped bone can typically be seen in the middle bone of the affected finger.
In addition to a physical exam and X-rays, your child may also undergo:
- Range of motions tests to determine if the condition is affecting movement and dexterity
Accurate diagnosis helps us determine the best course of treatment for your child.
Clinodactyly treatment
Most children with clinodactyly don’t need surgery to fix the condition. Surgery is usually only done if your child can’t use his/her hands normally.
Clinodactyly surgery
If your child’s clinodactyly is severe (more than 30-degree curvature) or significantly affecting her daily activities, surgery may be recommended. Surgery is most effective if performed while your child is still young and her bones are not fully matured.
If surgery is recommended:
- The surgery will be done in the operating room under general anesthesia (the child is put to sleep).
- Small cuts are made in the fingers to get to the bone.
- A cut in the bone is made to straighten the bones of the fingers.
- The fingers are put in the correct position. Small pins, wires or screws are used to hold the bone straight.
- After surgery, the hand will be bandaged and most likely put in a cast.
- Once the bandages are taken off, your surgeon might suggest working with a hand therapist.
Surgery for clinodactyly typically involves a phalanx-opening wedge osteotomy procedure. During this multi-step procedure, doctors will:
- Remove a wedge-shaped portion of the curved bone in the affected finger
- Stabilize the finger
- Ensure the bones and soft tissues are lined up properly within the finger
- Ensure the corrected finger lines up with the other fingers on the hand
After surgery, your child’s finger will be immobilized with a cast or splint. Doctors may also recommend a sling for your child’s arm to further protect the hand and finger as it heals.
Nonsurgical treatment
If your child’s finger is only slightly curved — and there is no problem using the fingers — clinicians will usually recommend ongoing observation to ensure the condition doesn’t worsen.
In most cases, splinting or stretching the finger is not recommended.
Follow-up care
Follow-up care for clinodactyly will depend on the treatment needed. If your child received nonsurgical treatment, they should be monitored regularly to ensure the condition does not begin to significantly affect his daily activities.
If your child had surgery, they will be examined at 2 weeks and 6 weeks post-operatively, then monitored regularly. Your child’s doctor will give you specific information about a recovery program for your child and how soon they can return to daily activities.
Clinodactyly prognosis
The long-term outlook for children with clinodactyly is very good. Many children with clinodactyly can avoid surgery. For children with more severe curvature of the finger, surgery can improve hand function and help children better manage their daily activities.
References




{kind=link}