Cornea verticillata
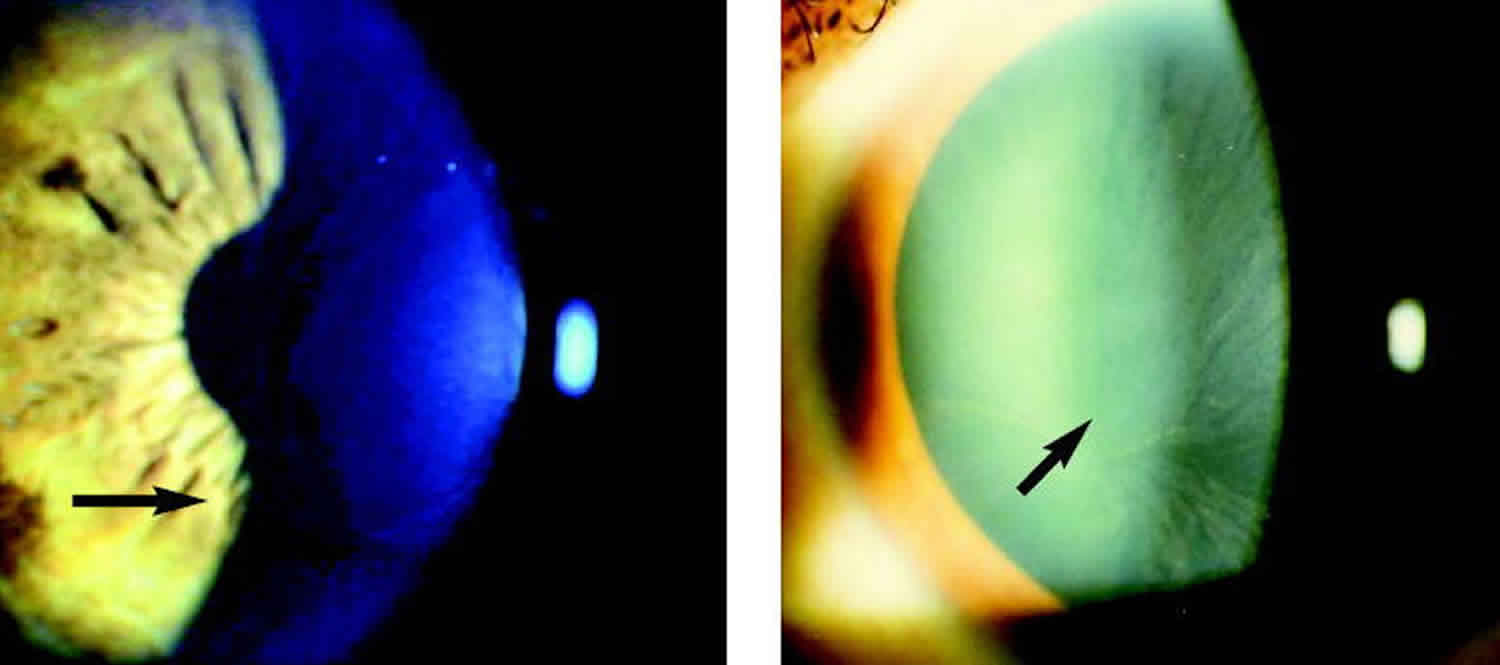
Cornea verticillata also called vortex keratopathy, whorl keratopathy or Fleischer vortex, describes a whorl-like pattern of golden brown or gray opacities in the cornea. It is termed cornea verticillata from the Latin noun “verticillus,” meaning “whorl”. Usually asymptomatic, it is caused by the deposition of medication, material, and disease byproducts in the basal epithelial layer of the cornea. Corneal verticillata is recognizable as fine golden-brown or gray opacities in the basal epithelium that branch out from a central whorl, usually across the inferior cornea. The deposits do not stain and are almost always bilateral 1. The whorl-like pattern of cornea verticillata results from the centripetal migration of deposit-laden limbal stem cells as the corneal epithelium undergoes natural growth and repair 2.
The medications that produce cornea verticillata share cationic, amphiphilic properties that allow them to penetrate lysosomes in the basal epithelial layer of the cornea, where they bind to cellular lipids. These medication-lipid complexes are resistant to enzymatic degradation and accumulate as deposits in the cornea 3.
Cornea verticillata is seen in 90% of patients with Fabry disease, a rare X-linked lysosomal storage disorder 4. Unlike that seen with medications, the cornea verticillata in Fabry disease is caused by a deficiency in alpha-galactosidase A, a lysosomal enzyme. This results in the accumulation of glycosphingolipids in lysosomes throughout body tissues, including the cornea 5.
Cornea verticillata, the most typical ocular sign in Fabry disease, was first described by Fleischer in 1910 6, but it was only in 1925 that Weicksel recognized cornea verticillata as being related to Fabry disease 7. In 1968, while studying a family with various cases of cornea verticillata, Franceschetti found that several members were affected by Fabry disease and reported an X-linked recessive model of inheritance for this metabolic disorder 8. Subsequent investigators have reported that Fabry disease has significant clinical effects in female heterozygotes 1. This is possibly due to the process of random X-inactivation.
Figure 1. Cornea verticillata Fabry disease
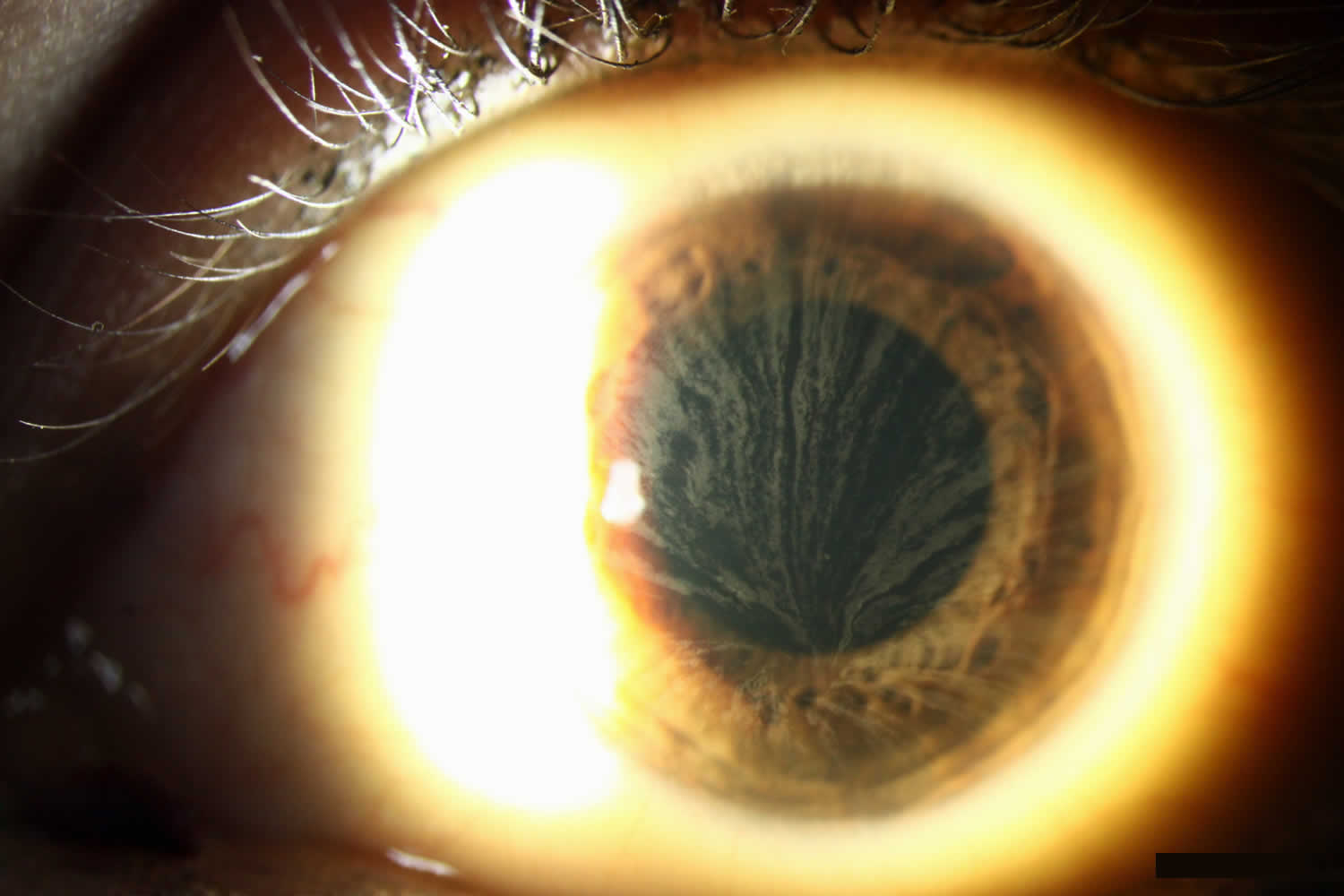
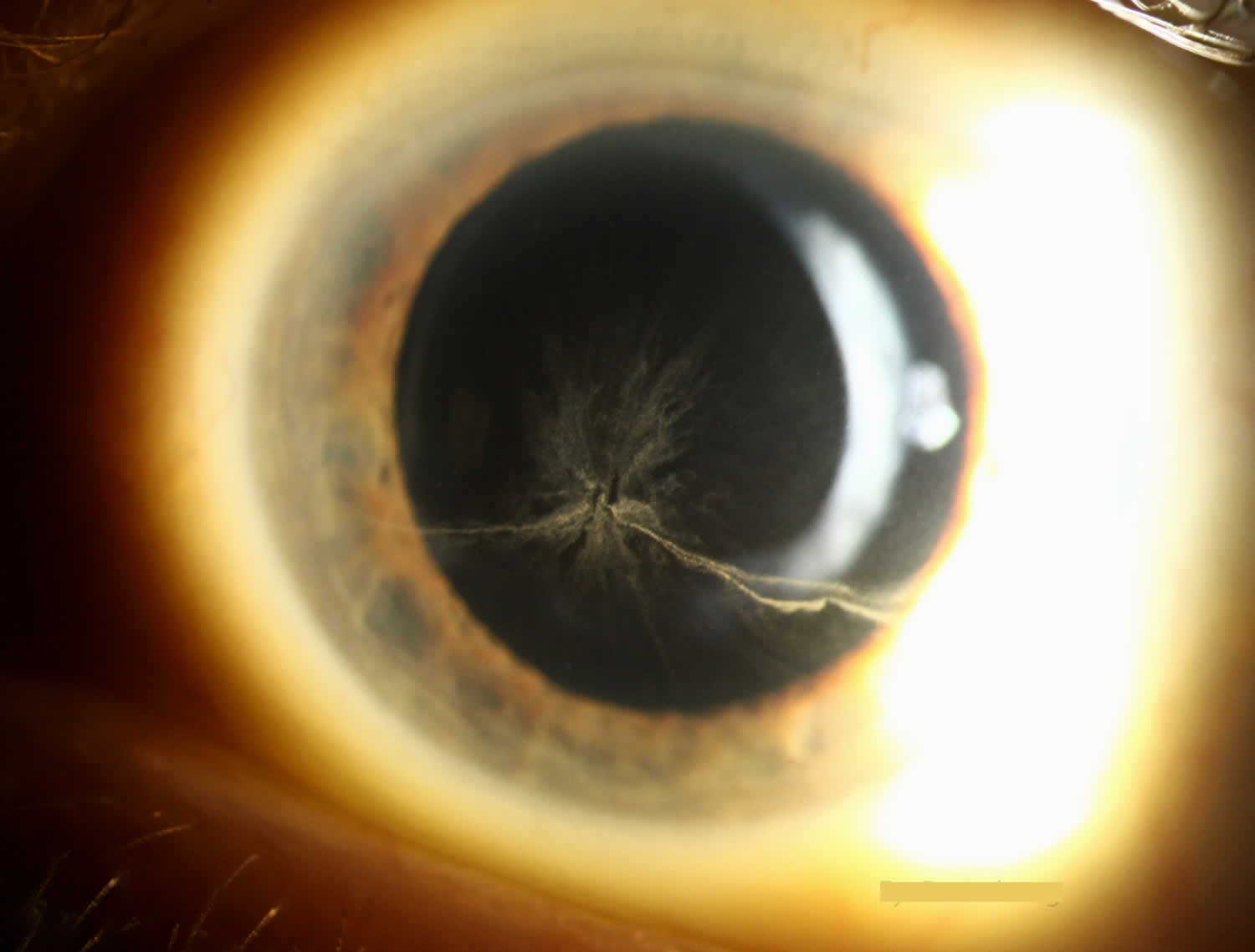
Figure 2. Cornea verticillata in a patient taking amiodarone
Cornea verticillata causes
Cornea verticillata is most commonly associated with amiodarone and Fabry disease 9.
Cornea verticillata can be caused by a variety of other medications, the most common of which include 3:
- Chloroquine and Hydroxychloroquine
- Indomethacin
- Phenothiazines
Other agents implicated in cornea verticillata include gentamicin, tamoxifen, meperidine, chlorpromazine, atovaquone, suramin, tilorone, perhexiline maleate, and the tyrosine kinase inhibitors vandetanib and osimertinib 3.
Other non-pharmacologic causes include 10:
- Multiple myeloma
- Neurotrophic keratitis
- Lisch corneal dystrophy
- Epidemic keratoconjunctivitis
- Iron lines (i.e., after radial keratotomy)
- Stromal deposits (gold, silver, antacid, retinoid depositions)
Corneal verticillata symptoms
Patients with cornea verticillata typically have no visual complaints or eye discomfort. Rarely, patients may see blue-green rings in their vision or halos around lights 3.
Occasionally, slight differences on slit-lamp microscopy can be seen in the opacities due to medications compared to those seen in Fabry disease. Drug-related opacities may appear as horizontal lines with fine branching at the extremities 11, while Fabry disease-related opacities may appear as curving lines that form whorls before becoming almost straight at the periphery 1.
Corneal verticillata diagnosis
Although the diagnosis of cornea verticillata can typically be made with a thorough review of the patient’s medical history and medications combined with slit-lamp microscopy, if this is insufficient, the microstructure of the deposits can be viewed with confocal laser scanning microscopy to differentiate drug-induced cornea verticillata from Fabry disease-associated cornea verticillata 12. However, this is not a routine part of the diagnostic evaluation.
Cornea verticillata treatment
There is no recommended treatment for cornea verticillata. The deposits typically resolve with cessation of the responsible agent, and no alteration in medication regimen or further work-up is required 5. Several case reports have described the resolution of cornea verticillata with the use of topical heparin 13.
If cornea verticillata is associated with a drug that is known to produce retinal toxicities, most notably hydroxychloroquine, chloroquine, chlorpromazine, and tamoxifen, patients should be routinely monitored with automated visual fields plus spectral-domain optical coherence tomography (SD OCT) 14. The presence of cornea verticillata does not correlate with retinal toxicity 15. The possibility of optic neuropathy should also be considered if patients taking amiodarone and tamoxifen present with reduced vision. For these patients, a reduction in dose or a switch to a different medication may be necessary 16.
References- Sodi A, Ioannidis A, Pitz S. Ophthalmological manifestations of Fabry disease. In: Mehta A, Beck M, Sunder-Plassmann G, editors. Fabry Disease: Perspectives from 5 Years of FOS. Oxford: Oxford PharmaGenesis; 2006. Chapter 26. Available from: https://www.ncbi.nlm.nih.gov/books/NBK11599
- Bron AJ. Vortex patterns of the Corneal epithelium. Trans ophthalmol SOC UK. 1973; 93(0):455-72
- Raizman M. B., Hamrah P., Holland E. J., Kim T., Mah F. S., Rapuano C. J., & Ulrich R. G. (2017). Drug-induced corneal epithelial changes. Survey of ophthalmology, 62(3), 286–301. 10.1016/j.survophthal.2016.11.008
- Eng CM, Germain DP, Banikazemi M, et al. Fabry disease: guidelines for the evaluation and management of multi-organ system involvement. Genet Med, 8 (9) (2006), pp. 539-548.
- Raizman M. B., Hamrah P., Holland E. J., Kim T., Mah F. S., Rapuano C. J., & Ulrich R. G. (2017). Drug-induced corneal epithelial changes. Survey of ophthalmology, 62(3), 286–301. 10.1016/j.survophthal.2016.11.008.
- Fleischer B. Uber eine eigenartige bisher nicht bekannte Hornhauttrubung [On an unusual thus far unknown type of corneal cloudiness] Graefes Arch Ophthalmol. 1910;77:136–40.
- Weicksel J. Angiomatosis bzw Angiokeratosis universalis (eine sehr seltene Haut-und Gefasserkrankung) [Angiomatosis or angiokeratosis universalis (a very rare disease of the skin and blood and lymphatic vessels)] Deutsch Med Wschr. 1925;51:898.
- Franceschetti AT. La cornea verticillata at ses relations avec la maladie de Fabry [Cornea verticillata (Gruber) and its relation to Fabry disease (angiokeratoma corporis diffusum)] Ophthalmologica. 1968;156:232–8.
- Koh S, Hamano T, Ichii M, Yatsui K, Maeda N, Nishida K. Transient Cornea Verticillata of Unknown Etiology. Cornea. 2019; 38 (5): e16–e17. doi: 10.1097/ICO.0000000000001913
- King JA, Affeldt JC, Agarwal MR. Etiologic profile of vortex keratopathy. Investigative Ophthalmology and Visual Science. 2003;44(13):1381.
- Mäntyjärvi M, Tuppurainen K, Ikäheimo K. Ocular side effects of amiodarone. Surv Ophthalmol, 42 (4) (1998), pp. 360-366.
- Wasielica-Poslednik J, Pfeiffer N, Reinke J, Pitz S. Confocal laser-scanning microscopy allows differentiation between Fabry disease and amiodarone-induced keratopathy. Graefes Arch Clin Exp Ophthalmol, 249 (11)(2011), pp. 1689-1696.
- Frings A, Schargus M. Recovery From Amiodarone-Induced Cornea Verticillata by Application of Topical Heparin. Cornea. 2017 Nov;36(11):1419-1422.
- Drug induced maculopathy. https://eyewiki.aao.org/Drug_induced_maculopathy
- Marmor MF, Kellner U, Lai TY, et al. Recommendations on screening for chloroquine and hydroxychloroquine retinopathy (2016 revision). Ophthalmology, 123 (6) (2016), pp. 1386-1394.
- Hui Jen Ding, Alastair K. Denniston, Vijay K. Rao, Caroline Gordon, Hydroxychloroquine-related retinal toxicity, Rheumatology, Volume 55, Issue 6, June 2016, Pages 957–967, https://doi.org/10.1093/rheumatology/kev357





{kind=link}