
What is Cyclospora
Cyclospora is an infection of the bowel caused by a tiny parasite called Cyclospora cayetanensis. Cyclospora cayetanensis parasite is usually caught from eating raw fruit and vegetables contaminated with human feces (poop). Cyclospora cayetanensis is a coccidian protozoan composed of one cell, too small to be seen without a microscope and appears to be involved in all human intestinal illness cases. Because cyclospora is a coccidian parasite, infected people shed oocysts (rather than cysts) in their feces. These oocysts must mature (sporulate) in the environment for days to weeks to become infective; therefore, direct person-toperson (fecal-oral) transmission is unlikely. Cyclosporiasis (cyclospora infection) has been reported in many countries, but is most common in tropical and subtropical areas. Since 1990, at least 11 foodborne outbreaks of cyclosporiasis, affecting approximately 3600 persons, have been documented in the United States and Canada.
People can become infected with Cyclospora by consuming food or water contaminated with the Cyclospora cayetanensis parasite. People living or traveling in countries where cyclosporiasis is endemic may be at increased risk for cyclospora infection (cyclosporiasis). Symptoms usually appear about a week after catching the Cyclospora cayetanensis parasite from ingestion of sporulated oocysts (the infective form of the parasite) usually from eating contaminated food or drinking contaminated water.
Cyclospora infects the small intestine and typically causes watery diarrhea, with frequent, sometimes explosive, diarrhea. And diarrhea, which can often be severe, is the most common symptom of cyclospora infections.
Other symptoms can include:
- Loss of appetite
- Weight loss
- Stomach cramps or pain
- Bloating
- Increased gas (flatulence)
- Feeling sick (nausea)
- Prolonged fatigue or tiredness
- Less common symptoms include vomiting, body aches, headache, fever, and other flu-like symptoms.
Although these symptoms are often unpleasant, cyclospora doesn’t usually pose a serious threat to health and can be easily treated using antibiotics. The recommended treatment is a combination of two antibiotics, trimethoprim-sulfamethoxazole, also known as Bactrim, Septra or Cotrim. People who have diarrhea should also rest and drink plenty of fluids.
To prevent or treat mild to moderate fluid loss from the severe diarrhea associated with cyclospora infection, it’s generally adequate for healthy adults to drink water. For children and infants, you may want to use an oral rehydration solution, such as Pedialyte. Sports drinks and carbonated beverages don’t offer the right balance of nutrients that children need.
If untreated, the illness may last for a few days to a month or longer, and may have a remitting-relapsing course.
Food safety precautions may help prevent the disease.
The following hygiene measures will help reduce your risk of catching cyclospora when traveling to affected areas:
- wash your hands (with soap and water) after going to the toilet
- wash your hands before preparing or eating food
- make sure food is steaming hot
- avoid raw fruit and vegetables that haven’t been washed in clean water
- only drink bottled water and avoid ice in drinks
- beware of any product that you suspect may have been tampered with, including bottled water
Some people with cyclospora don’t have any symptoms. These are usually people who have grown up in a developing country and been previously exposed to the parasite.
Many conditions can cause diarrhea and other gastrointestinal signs and symptoms. If you develop persistent diarrhea that lasts several days or recurs, contact your doctor so that he or she can identify the cause and recommend treatment. If you’ve eaten a food that’s been recalled because of a cyclospora outbreak or traveled in an area where parasites such as cyclospora are common, be sure to tell your doctor.
If you experience dehydration due to diarrhea, see your doctor. Warning signs of dehydration include:
- Sunken eyes
- Dry mouth and tongue
- Reduced production of tears
- Decreased urine output
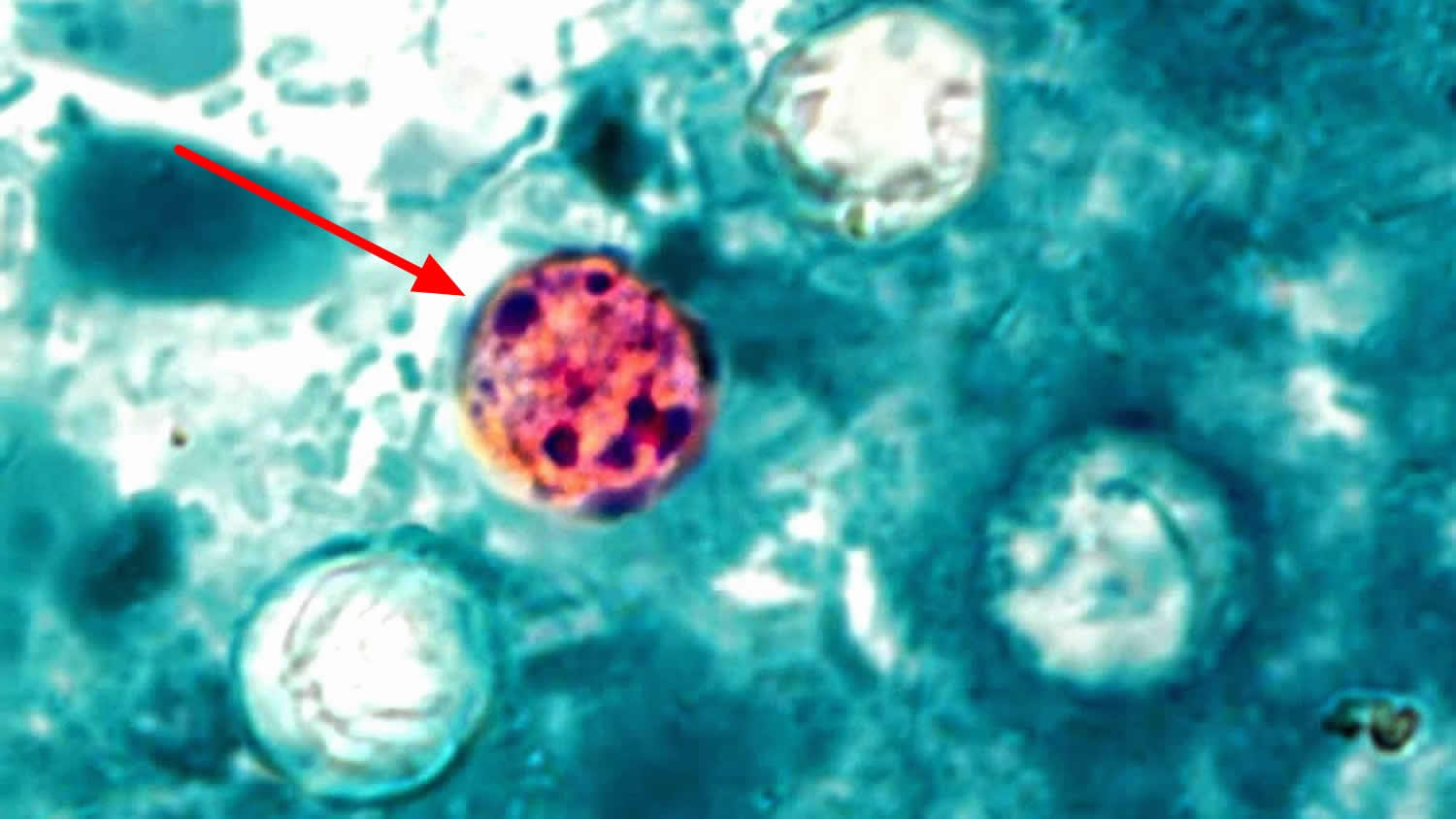
Figure 1. Cyclospora parasite
What is Cyclospora cayetanensis?
Cyclospora cayetanensis is a human parasite, which means it must live inside a human host to survive and multiply. The parasite can cause an infection, called cyclosporiasis. A person may become infected after ingesting food or water contaminated with the parasite. Infected people, even if showing no symptoms of infection, may shed the parasite in their feces, which can contaminate food and water, leading to the infection of other people. Cyclosporiasis outbreaks have been associated with the consumption of fresh fruits and vegetables around the world, including in the U.S.
Where is Cyclospora parasite found?
- Cyclosporiasis is endemic or commonly found among the population in certain countries/regions 1.
- Since the infection occurs only in humans, the parasite originates from the feces of ill people.
- The parasite may also be found in water and food, if it has been contaminated by human feces.
- No non-human host (animals) for this parasite has been identified.
- Cyclospora cayetanensis is not limited to imported foods. In July 2018, FDA found the first confirmed evidence of the presence of Cyclospora cayetanensis in domestic produce when two cilantro samples tested positive for the parasite 2.
What else do we know about Cyclospora parasite?
- Although clinical testing for the parasite in human feces has been available since the 1970s, FDA recently improved the method for the detection of this parasite on some fresh fruits and vegetables.
- The parasite needs to spend some time in the environment to later cause cyclosporiasis, therefore, Cyclospora cayetanensis is unlikely to be transmitted directly from person-to-person and still cause illness.
- The parasite needs specific environmental conditions to become infectious. Under experimental conditions, a combination of time and temperature (temperatures from 73° to 77 °F during 7 – 15 days) were required for Cyclospora cayetanensis to become infectious 3.
- Although chlorine and other antimicrobial washes are effective at reducing harmful populations of bacteria and viruses, they are not as effective on Cyclospora cayetanensis. In countries/regions where cyclosporiasis is endemic, microfiltration, ozone, or UV treatments may be effective at decreasing populations of Cyclospora cayetanensis in irrigation waters.
How long can the symptoms last?
If not treated, the illness may last from a few days to a month or longer. Symptoms may seem to go away and then return one or more times (relapse). It’s common to feel very tired.
How is Cyclospora infection diagnosed?
Your health care provider will ask you to submit stool specimens to see if you are infected. You might be asked to submit more than one specimen from different days. Identification of this parasite in stool requires special laboratory tests that are not routinely done. Therefore, if indicated, your health care provider should specifically request testing for Cyclospora. In addition, your health care provider might have your stool checked for other organisms that can cause similar symptoms.
What are Cyclospora infection complications?
The prolonged diarrhea of untreated cyclospora infection can cause dehydration. If you’re an otherwise healthy adult, you can treat dehydration by drinking more fluids. Some people may need to be hospitalized to receive intravenous fluids because they’re at higher risk of severe dehydration. Examples include:
- People with other serious illnesses
- Infants and young children
- Older adults
How is Cyclospora spread?
Cyclospora is spread by people ingesting something—such as food or water—that was contaminated with feces (stool). Cyclospora needs time (typically, at least 1–2 weeks) after being passed in a bowel movement to become infectious for another person. Therefore, it is unlikely that Cyclospora is passed directly from one person to another.
Who’s at risk cyclospora infection (cyclosporiasis)?
People traveling to tropical or subtropical countries may be at increased risk of infection because cyclospora is common in many developing countries.
Most of the cases reported in United States involve people who have returned from trips to:
- the Caribbean and Mexico
- Central and South America
- south and east Asia
- the Middle East
- Africa
People become infected with Cyclospora by ingesting sporulated oocysts, which are the infective form of the Cyclospora parasite. This most commonly occurs when food or water contaminated with feces is consumed. An infected person sheds unsporulated (immature, non-infective) Cyclospora oocysts in the feces. The oocysts are thought to require at least 1–2 weeks in favorable environmental conditions to sporulate and become infective (see Cyclospora life cycle Figure 1 below). Therefore, direct person-to-person transmission is unlikely, as is transmission via ingestion of newly contaminated food or water.
Cyclospora Geographic Distribution
Cyclosporiasis occurs in many countries, but it seems to be most common in tropical and subtropical regions. In areas where cyclosporiasis has been studied, the risk for infection is seasonal. However, no consistent pattern has been identified regarding the time of year or the environmental conditions, such as temperature or rainfall.
In the United States, foodborne outbreaks of cyclosporiasis have been linked to various types of imported fresh produce, such as raspberries, basil, snow peas, mesclun lettuce, and cilantro; no commercially frozen or canned produce has been implicated to date.
U.S. cases of infection also have occurred in persons who traveled to Cyclospora-endemic areas. Travelers should be aware that treatment of water or food by routine chemical disinfection or sanitizing methods is unlikely to kill Cyclospora oocysts.
Cyclospora life cycle
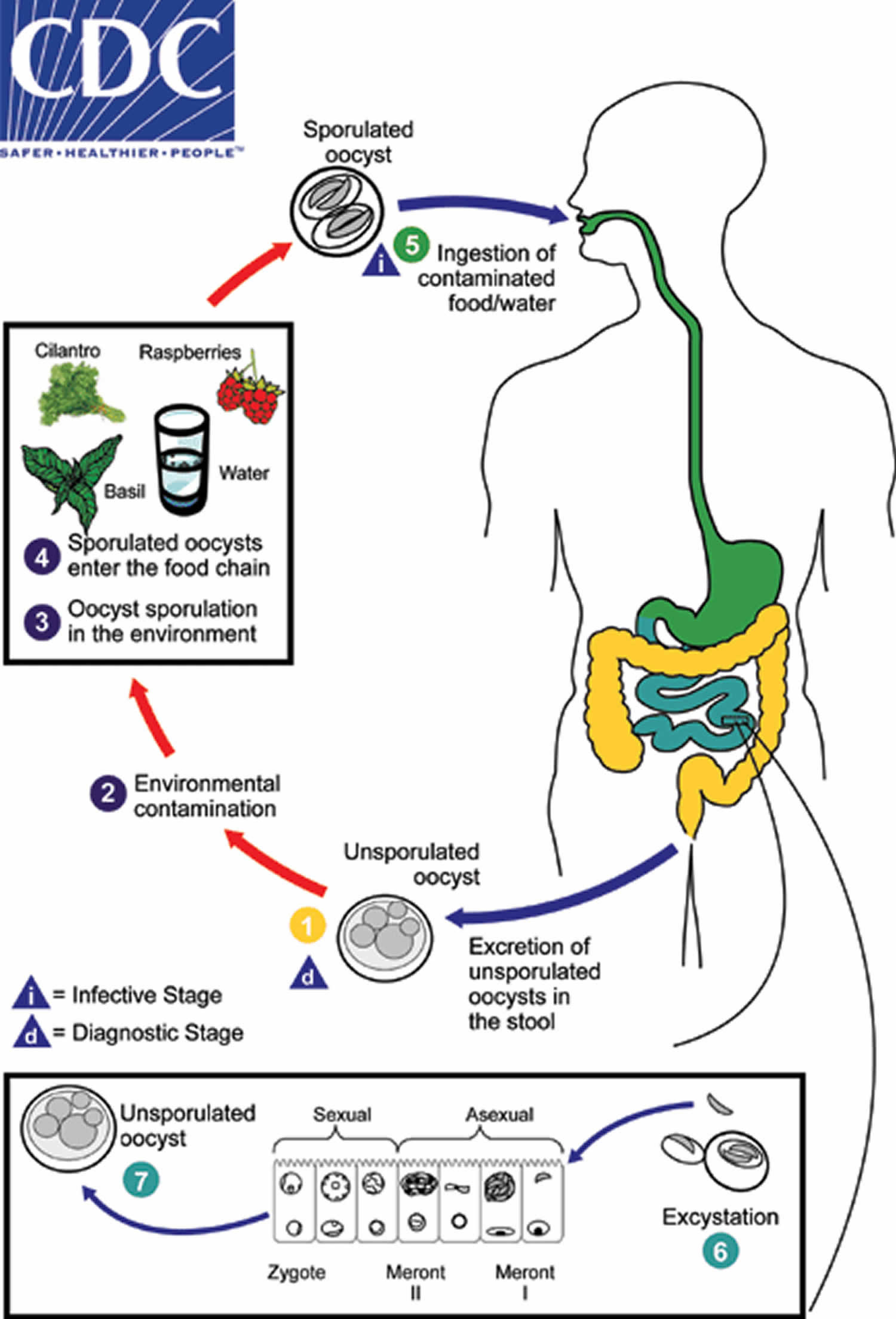
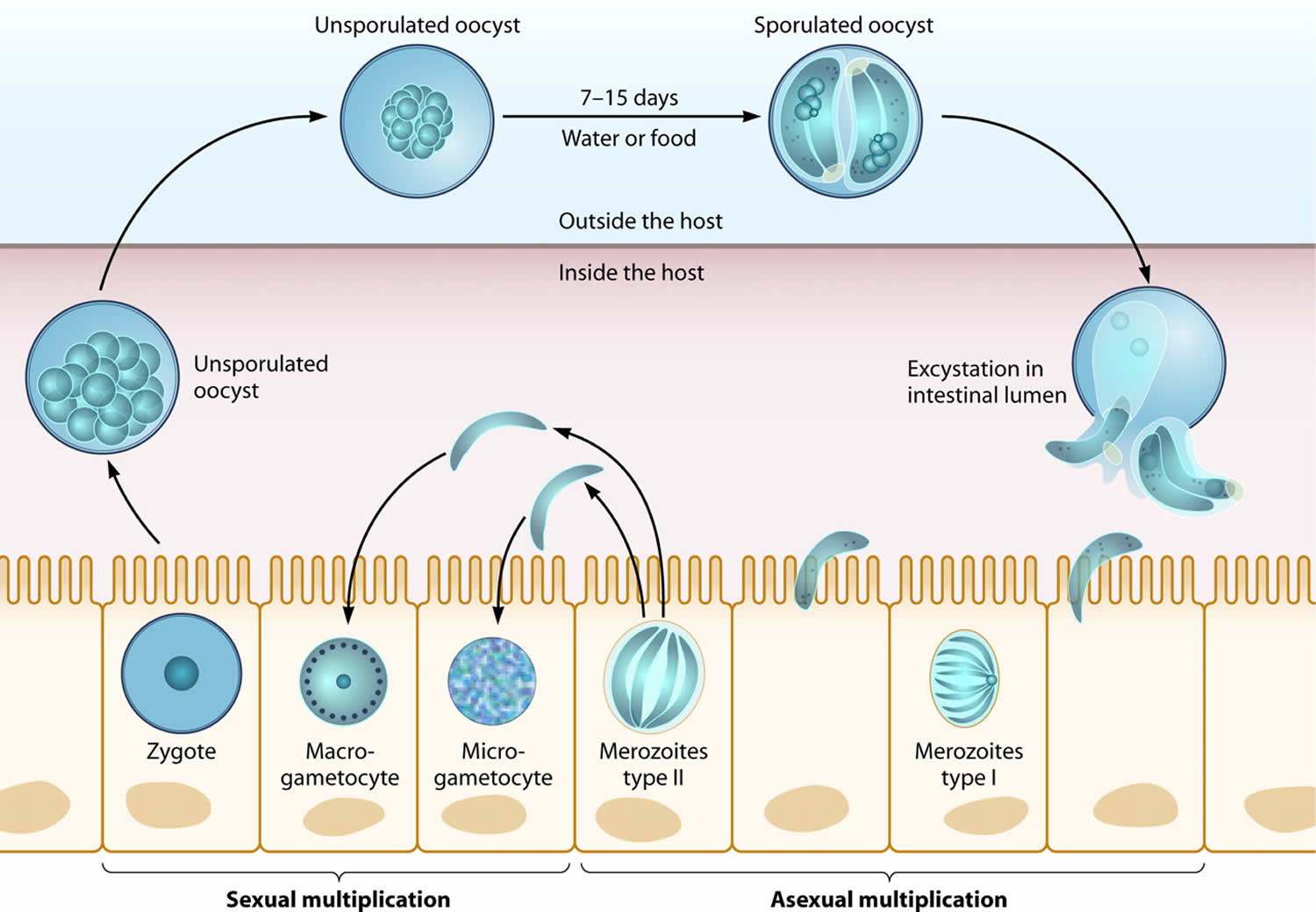
When freshly passed in stools, the oocyst is not infective (1) (thus, direct fecal-oral transmission cannot occur; this differentiates Cyclospora from another important coccidian parasite, Cryptosporidium). In the environment (2), sporulation occurs after days or weeks at temperatures between 22°C to 32°C, resulting in division of the sporont into two sporocysts, each containing two elongate sporozoites (3). Fresh produce and water can serve as vehicles for transmission (4) and the sporulated oocysts are ingested (in contaminated food or water) (5). The oocysts excyst in the gastrointestinal tract, freeing the sporozoites which invade the epithelial cells of the small intestine (6). Inside the cells they undergo asexual multiplication and sexual development to mature into oocysts, which will be shed in stools (7). The potential mechanisms of contamination of food and water are still under investigation.
After an average incubation period of 1 week, symptomatic infections typically manifest as watery diarrhea, which can be severe. Other symptoms include anorexia, weight loss, abdominal pain, nausea and vomiting, myalgias, low-grade fever, and fatigue. Untreated infections typically last for 10-12 weeks and may follow a relapsing course. Infections, especially in disease-endemic settings can be asymptomatic.
Figure 2. Cyclospora life cycle
Cyclospora infections causes
A one-celled parasite, Cyclospora cayetanensis, causes cyclospora infection. You get it by drinking water or eating food that’s been contaminated by a person infected with the parasite.
A person infected with cyclospora passes the parasite in stool. However, unlike some other foodborne parasites, cyclospora doesn’t become infectious until days or weeks after it’s passed in a bowel movement. So it’s unlikely that you can get the infection directly from a person infected with cyclospora, such as a restaurant worker who doesn’t wash his or her hands adequately after using the toilet.
Before the 1990s, sporadic cases of cyclospora infection turned up only in people who traveled in developing countries and in those with HIV or another condition that caused a weakened immune system. However, since the 1990s, lettuce, fresh basil and imported raspberries have been implicated in cyclospora outbreaks in the United States and Canada.
Risk factors for cyclospora infection
In the past, people who traveled in developing countries were more likely to get cyclospora infection. These days, the infection is found worldwide, and anyone who ingests contaminated food or water can get it.
Cyclospora infection prevention
Avoiding food or water that might have been contaminated with stool (feces) may help prevent Cyclospora infection.
When traveling to developing nations, it’s essential to be careful about what you eat and drink. However, recent cyclospora infection outbreaks have been linked to foods imported to or grown in the United States and Canada. Unfortunately, even careful washing of foods isn’t enough to eliminate the parasite that causes the infection.
Food and water while abroad
Many illnesses are contracted through contaminated food and water.
Reduce your risk of diseases like travelers’ diarrhea by following these basic guidelines.
Drinking water
In countries with poor sanitation, don’t drink tap water or use it to brush your teeth unless it’s been treated.
Filtered, bottled, boiled or chemically treated water should be used. Bottled fizzy drinks with an intact seal are usually safe, as are boiled water and hot drinks made with boiled water. Ice in drinks should be avoided.
The most reliable way to purify water is by boiling it, but this isn’t always possible.
Chemical disinfectants, such as iodine and chlorine, will usually kill bacteria and viruses, and can easily be obtained from larger pharmacies or specialist travel shops.
However, some parasites aren’t reliably killed with iodine or chlorine preparations.
Combining iodine or chlorine with filtration using a specialist filter bought from a travel shop should be effective.
Domestic water filters designed for use in the US aren’t suitable.
Foods to avoid
Foods to avoid in countries where sanitation is poor:
- salads, such as lettuce
- uncooked fruits and vegetables, unless they’ve been washed in safe water and peeled by the traveler
- fresh or cooked food that’s been allowed to stand at room temperature in warm environments or exposed to flies, such as in an open buffet
- unpasteurized milk, cheese, ice cream and other dairy products
- raw or undercooked shellfish or seafood
- food from street traders, unless it’s been recently prepared and is served hot on clean crockery
Food served in good-standard hotels or restaurants may not always be safe as it may have been contaminated during preparation.
Try to pick places to eat that have a reputation for serving safe food.
As a rule, only eat freshly prepared food that’s thoroughly cooked and served steaming hot.
Always wash your hands after going to the toilet and before preparing or eating food.
Consumers and retailers should always follow safe fruit and vegetable handling recommendations:
- Wash: Wash hands with soap and warm water before and after handling or preparing fruits and vegetables. Wash cutting boards, dishes, utensils, and counter tops with soap and hot water between the preparation of raw meat, poultry, and seafood products and the preparation of fruits and vegetables that will not be cooked.
- Prepare: Wash all fruits and vegetables thoroughly under running water before eating, cutting, or cooking. Fruits and vegetables that are labeled “prewashed” do not need to be washed again at home. Scrub firm fruits and vegetables, such as melons and cucumbers, with a clean produce brush. Cut away any damaged or bruised areas on fruits and vegetables before preparing and eating.
- Store: Refrigerate cut, peeled, or cooked fruits and vegetables as soon as possible, or within 2 hours. Store fruits and vegetables away from raw meat, poultry, and seafood.
Fast Facts for Farmers:
- Cyclosporiasis is an intestinal illness caused by the parasite Cyclospora cayetanensis (C. cayetanensis), which only occurs in humans, and the most common symptom is diarrhea.
- Infected people shed the parasite in their feces.
- When the parasite is found in water or food, it means that the water or food has been contaminated with human feces.
- Other people may become sick by ingesting water or food contaminated with the parasite.
- Good hygiene (including proper handwashing) is a critical component of ensuring the safety of fresh produce, but by itself it may not be enough to prevent infected employees from contaminating fresh produce.
- The FSMA Produce Safety Rule requires that personnel on farms use hygienic practices and that ill employees are excluded from handling fresh produce and food contact surfaces.
Cyclospora outbreak
Cyclospora outbreaks in the United States and Canada have been linked to imported fresh produce. Cyclospora is spread by eating food, especially raw berries, herbs and salad, or drinking water contaminated with human feces (poop) carrying the parasite.
To keep track of what foods have been linked to recent outbreaks of cyclospora infection, you may want to periodically check the food safety alert section of the Food and Drug Administration’s website. The Latest Cyclospora Outbreak Investigations and Updates can be found here: https://www.cdc.gov/parasites/cyclosporiasis/outbreaks/index.html
- On July 30, 2018, the U.S. Department of Agriculture’s Food Safety and Inspection Service (FSIS) issued a public health alert on beef, pork and poultry salad and wrap products potentially contaminated with Cyclospora that were distributed by Caito Foods LLC, of Indianapolis, IN. The products were produced between July 15 and 18, 2018, with either “Best By,” “Enjoy by,” “Best if Sold By” or “Sell By” dates ranging from July 18 through July 23, 2018. Caito Foods had received notification from Fresh Express that the chopped romaine in these products was being recalled 5.
- As of September 11, 2018, this outbreak appears to be over. A total of 511 laboratory-confirmed cases of Cyclospora infection were reported in people who consumed salads from McDonald’s restaurants; the cases were reported by 15 states and New York City. The FDA investigated distribution and supplier information for romaine and carrots but did not identify a single source or potential point of contamination for this outbreak 5.
What Do Restaurants and Retailers Need To Do?
Based on current information available Cyclospora may be resistant to routine chemical disinfection methods such as those using chlorine. However, restaurants and retailers should still follow basic food safety practices:
- Retailers, restaurants, and other food service operators should always practice safe food handling and preparation measures. It is recommended that they wash utensils, and surfaces with hot, soapy water before and after handling food. Wash and sanitize display cases and refrigerators where potentially contaminated products were stored.
- Wash and sanitize cutting boards, surfaces, and utensils used to prepare, serve, or store potentially contaminated products.
- Wash hands with warm water and soap following the cleaning and sanitation process.
- Regular frequent cleaning and sanitizing of food contact surfaces and utensils used in food preparation may help to minimize the likelihood of cross-contamination.
What Do Consumers Need To Do?
Consumers who have symptoms of cyclosporiasis should contact their health care provider to report their symptoms and receive care. Most people infected with Cyclospora develop diarrhea, with frequent, sometimes explosive, bowel movements. Other common symptoms include loss of appetite, weight loss, stomach cramps/pain, bloating, increased gas, nausea, and fatigue. Vomiting, body aches, headache, fever, and other flu-like symptoms may be noted.
What are some steps that farms are required to take by the FSMA Produce Safety Rule?
Farms covered by the Produce Safety Rule must do the following:
- Train farm workers who handle produce or food contact surfaces on how to properly wash their hands with soap and running water, properly dry hands, and properly dispose of the paper towels. Free videos and training materials exist in multiple languages online here (https://www.cdc.gov/cdctv/spanish/healthyliving/acabe-con-los-microbios.html).
- Make sure toilets and handwashing stations are maintained, cleaned, and emptied in a way that prevents human waste and/or gray water from contaminating fresh produce, food contact surfaces, and adjacent areas.
- Train farm workers to self-report applicable symptoms and illnesses to the appropriate responsible person, and don’t allow ill farm workers to handle fresh produce or touch food contact surfaces.
What can I do to reduce the likelihood of contaminating fresh produce with Cyclospora cayetanensis?
Controlling sources of contamination in the field, in the packinghouse, and from farm workers is key to preventing illnesses. Farms can do the following to minimize the chance of contaminating fresh produce with Cyclospora cayetanensis:
- Train farm workers on how to properly use toilet facilities provided by the farm, including the sanitary disposal of toilet paper.
- Consider the varying cultural practices of farm workers when providing training on produce safety.
- If utilizing a contractor for cleaning and sanitizing the portable toilets, consider using reputable companies that dispose of human waste into an adequate sewage system or through other adequate means. Municipal wastewater treatment incorporates disinfection processes designed to kill or inactivate Cyclospora cayetanensis.
What happens if infected farm workers handle produce?
Workers infected with C. cayetanensis can transmit the parasite to fresh produce, which can cause people to get sick if the contaminated produce is consumed. Therefore, it is essential that ill employees be excluded from handling fresh produce and food contact surfaces. If you have reason to suspect a cyclosporiasis infection, consider working with your public health agency. Identifying and treating Cyclospora infection is essential.
Cyclospora symptoms
Symptoms of cyclosporiasis (cyclospora infection) begin an average of 7 days (range, 2 days to ≥2 weeks) after ingestion of sporulated oocysts (the infective form of the parasite) by eating contaminated food or drinking contaminated water. Some people infected with the microscopic parasite that causes cyclospora infection develop no signs or symptoms.
Symptoms of cyclosporiasis may include the following:
- Frequent, watery diarrhea (most common)
- Bouts of diarrhea alternating with bouts of constipation
- Loss of appetite
- Weight loss
- Stomach cramps
- Bloating
- Increased gas (flatulence) and burping
- Nausea and vomiting
- Fatigue — this symptom may last long after the active infection has gotten better
- Muscle aches
- General feeling of unwellness (malaise)
Other symptoms that may occur but are less common include the following:
- Vomiting
- Low-grade fever
If a person ill from cyclosporiasis is not treated, symptoms can persist for several weeks to a month or more. Some symptoms, such as diarrhea, can return; and some symptoms, such as fatigue, may continue after the gastrointestinal symptoms have gone away. The infection usually is not life threatening. Some infected persons do not have any symptoms, particularly persons from areas where cyclosporiasis is endemic, such as tropical and subtropical regions.
If you have HIV or another condition that compromises your immune system, the infection can last for months if not treated.
Cyclospora diagnosis
Because diarrhea can be caused by many things, it can be difficult to diagnose cyclospora infection (cyclosporiasis) unless a specialized stool test is done. Health care providers should consider Cyclospora as a potential cause of prolonged diarrheal illness, particularly in patients with a history of recent travel to Cyclospora-endemic areas, such as tropical and subtropical regions. Testing for Cyclospora is not routinely conducted in most U.S. laboratories, even when stool is tested for parasites 6. Similarly, not all gastrointestinal polymerase chain reaction (PCR) panels include a target for Cyclospora. Therefore, if indicated, health care providers should specifically request testing for Cyclospora.
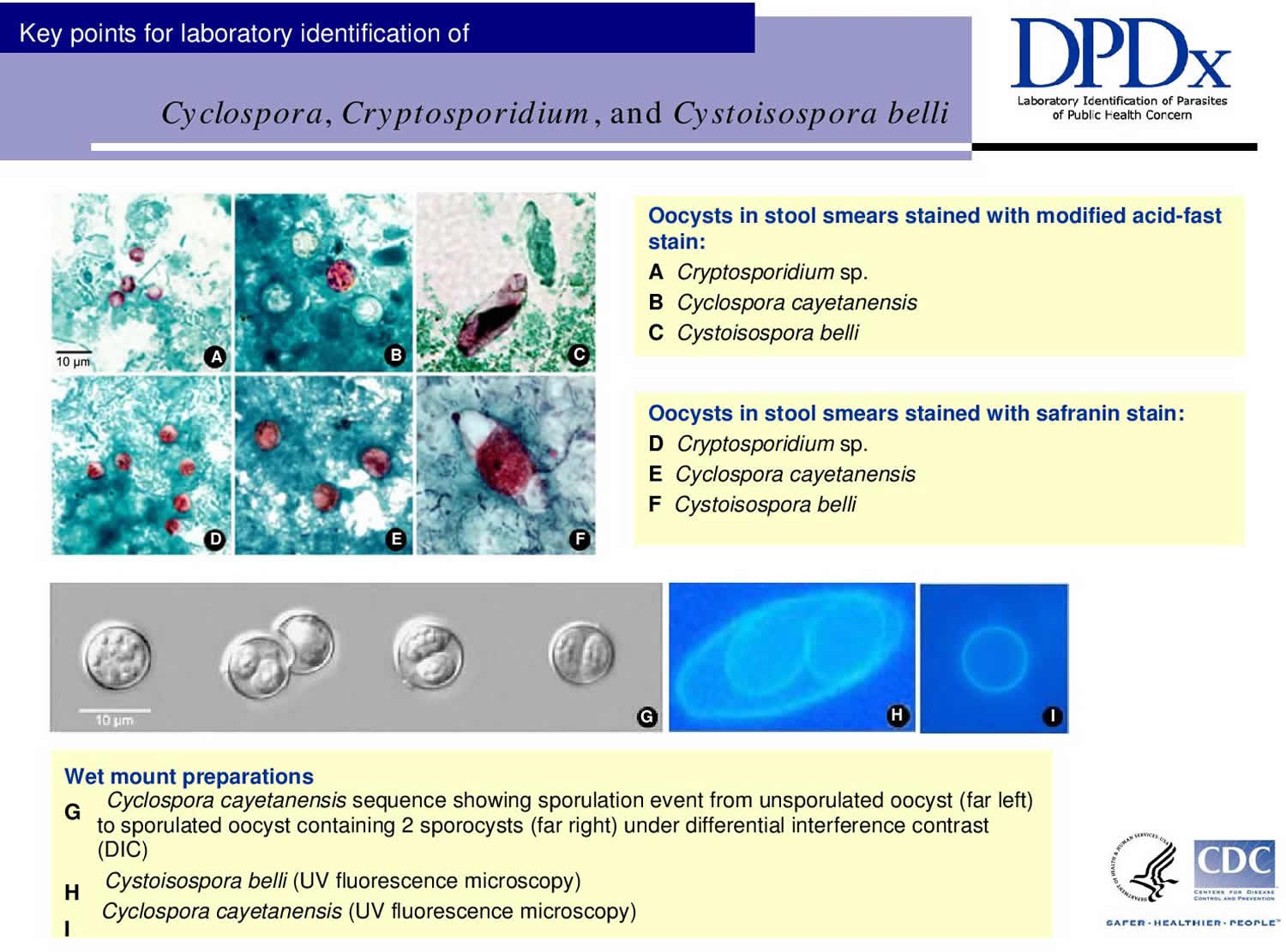
Cyclospora infection is diagnosed by examining stool specimens. Diagnosis can be difficult in part because even patients who are symptomatic might not shed enough oocysts in their stool to be readily detectable by laboratory examinations. Therefore, patients might need to submit several specimens collected on different days. In addition, the laboratory should use sensitive recovery methods (concentration procedures) and detection methods that highlight Cyclospora oocysts. The oocysts can be stained with modified acid-fast or modified (“hot”) safranin techniques. Cyclospora oocysts also are autofluorescent, meaning that when stool containing the parasite is viewed under an ultraviolet (UV) fluorescence microscope the oocysts appear blue or green (see image above) against a black background. Molecular diagnostic methods, such as polymerase chain reaction (PCR) analysis, are used to look for the parasite’s DNA in the stool.
Additional perspective about laboratory testing for Cyclospora:
- Cyclospora oocysts are easily overlooked; low-level shedding (~1–2 logs lower than for Cryptosporidium species) is common. To maximize recovery of Cyclospora oocysts, first concentrate the stool specimen—such as by the formalin-ethyl acetate technique (centrifuge for 10 minutes at 500 x g)—and then examine a wet mount and/or a stained slide of the sediment.
- Cyclospora oocysts are ~8–10 micrometers in diameter (in contrast, Cryptosporidium parvum/hominis oocysts are ~4–6 micrometers in diameter).
Ultraviolet fluorescence microscopy (UV excitation filter set at 330–365 nm or 450–490 nm) is a sensitive technique for rapidly examining stool sediments for Cyclospora oocysts, which stand out because they autofluoresce (Cryptosporidium parvum/hominis oocysts do not). If suspect Cyclospora oocysts are found, bright-field, phase contrast, or differential interference contrast microscopy can then be used to confirm that the structures have the characteristic morphologic features of Cyclospora oocysts (i.e., are nonrefractile spheres that contain undifferentiated cytoplasm or refractile globules). - On a modified acid-fast—stained slide of stool, Cyclospora oocysts typically are variably acid fast (i.e., in the same field, oocysts may be unstained or stain from light pink to deep red or purple). Unstained oocysts characteristically have a wrinkled (hyaline) appearance.
- If a “hot” modified safranin technique is used, Cyclospora oocysts uniformly stain a brilliant reddish orange.
Laboratory Diagnosis
Currently, the most practical diagnostic method consists of the identification of Cyclospora oocysts in stool specimens by light microscopy. Although microscopy remains the method of choice in most clinical laboratories, molecular diagnosis using culture-independent diagnostic tests, such as the FilmArray Gastrointestinal Panel by BioFire, has become increasingly more common.
Specimen Processing
Specimens should be preserved as soon as possible after collection. Various fixatives can be used depending on what tests will be performed.
- Stool fixed in 10% formalin is recommended for direct microscopy, concentration procedures, and preparation of stained smears; Specimens fixed in sodium acetate-acetic acid formalin can be handled in the same manner as specimens fixed in 10% formalin.
- Stool fixed in formalin-free fixatives, such as polyvinyl alcohol or one-vial fixatives (e.g., TotalFix and EcoFix) is suitable for polymerase chain reaction (PCR)-based detection and UV microscopy.
Unpreserved stool collected in enteric transport media (e.g., Cary-Blair) is commonly used for culture-independent diagnostic tests and can be used for confirmatory testing by microscopy and/or polymerase chain reaction (PCR) if needed. Unpreserved specimens must be refrigerated and sent to the diagnostic laboratory as rapidly as possible.
Cyclospora oocysts can be excreted intermittently and in small numbers. Thus:
- A single negative stool specimen does not rule out the diagnosis; three or more specimens at 2- or 3-day intervals may be required
- Concentration procedures should be used to maximize recovery of oocysts. The method most familiar to laboratorians is the formalin-ethyl acetate sedimentation technique (centrifuge for 10 minutes at 500 × g). Other methods can also be used (such as the Sheather’s flotation procedure).
Microscopic Examination
The sediment can be examined microscopically with different techniques:
- Wet mounts (by conventional light microscopy, which can be enhanced by UV fluorescence microscopy or differential interference contrast [DIC, Nomarsky])
- Stained smears (using modified acid-fast stain or a modified safranin stain)
Molecular diagnosis
Several conventional and real-time polymerase chain reaction (PCR) protocols have been developed to specifically detect Cyclospora cayetanensis in stool. The Centers for Disease Control and Prevention (CDC) utilizes a real-time polymerase chain reaction (PCR) that targets a region of the 18S rRNA gene using a species-specific TaqMan probe. When detecting Cyclospora cayetanensis in stool using PCR it is important to choose an appropriate DNA extraction technique that will adequately break open the oocysts; methods that include a vigorous bead beating step generally perform best.
Figure 3. Cyclospora diagnosis
Cyclospora treatment
Trimethoprim-sulfamethoxazole (Bactrim, Septra, or Cotrim), is the treatment of choice. The typical regimen for immunocompetent adults is trimethoprim 160 mg plus sulfamethoxazole 800 mg (one double-strength tablet), orally, twice a day, for 7–10 days. HIV-infected patients may need longer courses of therapy 7.
No highly effective alternatives have been identified yet for persons who are allergic to (or are intolerant of) trimethoprim-sulfamethoxazole. Approaches to consider for such persons include observation and symptomatic treatment, use of an antibiotic whose effectiveness against Cyclospora is based on limited data, or desensitization to trimethoprim-sulfamethoxazole. The latter approach should be considered only for selected patients who require treatment, have been evaluated by an allergist, and do not have a life-threatening allergy.
Anecdotal or unpublished data suggest that the following drugs are ineffective: albendazole, trimethoprim (when used as a single agent), azithromycin, nalidixic acid, tinidazole, metronidazole, quinacrine, tetracycline, doxycycline, and diloxanide furoate. Although data from a small study among HIV-infected patients in Haiti suggested that ciprofloxacin might have modest activity against Cyclospora, substantial anecdotal experience among many immunocompetent persons suggests that ciprofloxacin is ineffective.
Treatment in Pregnancy
Trimethoprim–sulfamethoxazole is in pregnancy category C.
- Pregnancy Category C: Either studies in animals have revealed adverse effects on the fetus (teratogenic or embryocidal, or other) and there are no controlled studies in women or studies in women and animals are not available. Drugs should be given only if the potential benefit justifies the potential risk to the fetus.
Trimethoprim–sulfamethoxazole should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Trimethoprim–sulfamethoxazole should be avoided near-term because of the potential for hyperbilirubinemia and kernicterus in the newborn.
Treatment During Breastfeeding
Trimethoprim–sulfamethoxazole is excreted in breast milk. Trimethoprim–sulfamethoxazole generally is compatible with breastfeeding of healthy, full-term infants after the newborn period. However, trimethoprim–sulfamethoxazole generally should be avoided by women when nursing infants who are premature, jaundiced, ill, or stressed, or who have glucose-6-phosphate dehydrogenase deficiency.
Treatment in Pediatric Patients
The safety of trimethoprim–sulfamethoxazole in children has not been systematically evaluated. Use in children less than 2 months of age generally is not recommended.
I am allergic to sulfa drugs; is there another drug I can take?
No highly effective alternative drugs have been identified yet for people with Cyclospora infection who are unable to take sulfa drugs. See your health care provider to discuss potential options, your doctor may prescribe ciprofloxacin or nitazoxanide (Alinia).
References- Bangladesh, Brazil, Chile, China, Cuba, Dominican Republic, Egypt, Guatemala, Haiti, India, Indonesia, Jordan, Mexico, Morocco, Nepal, Nigeria, Pakistan, Peru, Puerto Rico, Romania, Saudi Arabia, Tanzania, Thailand, Turkey, Venezuela, Viet Nam, and Zimbabwe; (Ortega, et al. Clinical Microbiology Reviews, 2010 Jan; 23(1):218-234.
- Cyclosporiasis and Fresh Produce. https://www.fda.gov/Food/FoodborneIllnessContaminants/Pathogens/ucm621533.htm
- Ortega, et al. Clinical Microbiology Reviews, 2010 Jan; 23(1):218-234.
- Update on Cyclospora cayetanensis, a Food-Borne and Waterborne Parasite. Clinical Microbiology Reviews Jan 2010, 23 (1) 218-234; DOI: 10.1128/CMR.00026-09 https://cmr.asm.org/content/23/1/218
- FDA Investigation of a Multistate Outbreak of Cyclospora Illnesses Linked to Fresh Express Salad Mix Served at McDonald’s Ends. https://www.fda.gov/Food/RecallsOutbreaksEmergencies/Outbreaks/ucm613513.htm
- Diagnosis of Cyclosporiasis. https://www.cdc.gov/parasites/cyclosporiasis/health_professionals/dx.html
- Treatment for Cyclosporiasis. https://www.cdc.gov/parasites/cyclosporiasis/health_professionals/tx.html





{kind=link}