What is dextrocardia
Dextrocardia is a rare condition in which the heart is located in the right side of the chest instead of the left. Dextrocardia is usually present from birth (congenital). There are several types of dextrocardia. The simplest type occurs when the shape and structure of the heart is a mirror image of a normal heart. Other types of dextrocardia may involve defects of the walls of the heart, nearby blood vessels, or other organs in the abdomen. Chest X-raxys and echocardiograms can be used to determine which type of dextrocardia is present.
Dextrocardia is believed to occur in approximately 1 in 12,000 people 1.
Figure 1. Dextrocardia chest x-ray

Footnote: 30 year old female complaining of chest pain. Gastric bubble on the left, liver shadow on the right. Lungs and pleural spaces are clear. No cardiac silhouette enlargement.
[Source 2 ]Is there any case where a pacemaker has been placed in a dextrocardia patient?
There have been several reports of the successful placement of a pacemaker in individuals with dextrocardia 3. It has been suggested that standard surgical techniques may be used, though careful imaging of the heart is encouraged due to the unusual anatomy 3.
Types of dextrocardia
There are several types of dextrocardia. Many types involve other defects of the heart and abdomen area.
In the simplest type of dextrocardia, the heart is a mirror image of the normal heart and there are no other problems. This condition is rare. When this occurs, the organs of the abdomen and the lungs will often also be arranged in a mirror image. For example, the liver will be on the left side instead of the right.
Some people with mirror-image dextrocardia have a problem with the fine hairs (cilia) that filter the air going into their nose and air passages. This condition is called Kartagener syndrome.
In the more common types of dextrocardia, other heart defects are also present. The most common of these include:
- Double outlet right ventricle (the aorta connects to the right ventricle instead of to the left ventricle)
- Endocardial cushion defect (the walls separating all 4 chambers of the heart are poorly formed or absent)
- Pulmonary stenosis (narrowing of the pulmonary valve) or atresia (pulmonary valve does not form properly)
- Single ventricle (instead of two ventricles, there is a single ventricle)
- Transposition of the great vessels (the aorta and pulmonary artery are switched)
- Ventricular septal defect (hole in the wall that separates the right and left ventricles of the heart)
The abdominal and chest organs in babies with dextrocardia may be abnormal and may not work correctly. A very serious syndrome that appears with dextrocardia is called heterotaxy. In this condition, many of the organs are not in their usual places and may not work properly. For example, the spleen may be completely missing. The spleen is an important part of the immune system, so babies born without this organ are in danger of severe bacterial infections and death. In another form of heterotaxy, several small spleens exist, but they may not work correctly.
Heterotaxy may also include:
- Abnormal gallbladder system
- Problems with the lungs
- Problems with the structure or position of the intestines
- Severe heart defects
- Abnormalities of the blood vessels
Dextrocardia with situs inversus
Dextrocardia with situs inversus is a condition that is characterized by abnormal positioning of the heart and other internal organs. In people affected by dextrocardia, the tip of the heart points towards the right side of the chest instead of the left side. Situs inversus refers to the mirror-image reversal of the organs in the chest and abdominal cavity. Some affected people have no obvious signs or symptoms. However, a small percentage of people also have congenital heart defects, usually transposition of the great vessels. Dextrocardia with situs inversus can also be associated with primary ciliary dyskinesia (also known as Kartagener syndrome). Treatment typically depends on the heart or physical problems the person may have in addition to dextrocardia with situs inversus 4.
Situs inversus is present in 0.01% of the population 4. Situs describes the position of the cardiac atria and viscera. Situs solitus is the normal position, and situs inversus is the mirror image of situs solitus (see Figure 2 below). Cardiac situs is determined by the atrial location. In situs inversus, the morphologic right atrium is on the left, and the morphologic left atrium is on the right. The normal pulmonary anatomy is also reversed, so that the left lung has 3 lobes and the right lung has 2 lobes. In addition, the liver and gallbladder are located on the left, whereas the spleen and stomach are located on the right. The remaining internal structures are also a mirror image of the normal.
Situs inversus can be classified further into situs inversus with levocardia and situs inversus with dextrocardia. The classification of situs is independent of the cardiac apical position. The terms levocardia and dextrocardia indicate only the direction of the cardiac apex at birth; they do not imply the orientation of the cardiac chambers. In levocardia, the base-to-apex axis points to the left, and in dextrocardia, the axis is reversed. Isolated dextrocardia is also termed situs solitus with dextrocardia. The cardiac apex points to the right, but the viscera are otherwise in their usual positions. Situs inversus with dextrocardia is also termed situs inversus totalis because the cardiac position, as well as the atrial chambers and abdominal viscera, is a mirror image of the normal anatomy. Situs inversus totalis has an incidence of 1 in 8,000 births. Situs inversus with levocardia is less common, with an incidence of 1 in 22,000 births 5.
Situs inversus occurs more commonly with dextrocardia 6. A 3-5% incidence of congenital heart disease is observed in situs inversus with dextrocardia, usually with transposition of the great vessels. Of these patients, 80% have a right-sided aortic arch. Situs inversus with levocardia is rare 7 and it is almost always associated with congenital heart disease 8.
When situs cannot be determined, the patient has situs ambiguous or heterotaxy. In these patients, the liver may be midline, the spleen absent or multiple, the atrial morphology unclear, and the bowel malrotated. Often, normally unilateral structures are duplicated or absent. The 2 primary subtypes of situs ambiguous include (1) right isomerism, or asplenia syndrome, and (2) left isomerism, or polysplenia syndrome. Heterotaxy syndromes have an incidence of 1 in 10,000 newborn births but account for about 4% of all congenital heart disease 5.
In classic right isomerism, or asplenia, bilateral right-sidedness occurs. These patients have bilateral right atria, a centrally located liver, and an absent spleen, and both lungs have 3 lobes. The descending aorta and inferior vena cava are on the same side of the spine. Right isomerism has an incidence of between 1 in 10,000 and 1 in 20,000 births, male predominance, and a nearly 100% incidence of congenital heart disease. It often presents in childhood with a cyanotic heart defect such as a common AV canal, univentricular heart, transposition of the great arteries, or total anomalous pulmonary venous return 5.
In left isomerism, or polysplenia, bilateral left-sidedness occurs. These patients have bilateral left atria and multiple spleens, and both lungs have 2 lobes. Interruption of the inferior vena cava with azygous or hemiazygous continuation is often present. Left isomerism has an incidence of between 1 in 10,000 and 1 in 20,000 births and a female predominance. Associated cardiac malformations include partial anomalous pulmonary venous return, atrial septal defect (ASD), and a common atrioventricular (AV) canal 5.
The features of situs ambiguous are inconsistent; therefore, situs ambiguous cases are challenging and require thorough evaluation of the viscera 9. The location and relationships of the following should be reviewed carefully: abdominal viscera, hepatic veins, superior vena cava, inferior vena cava, coronary sinus, pulmonary veins, cardiac atria, atrioventricular connections and valves, cardiac ventricles, position of the cardiac apex, and aortic arch and great vessels.
Figure 2. Dextrocardia situs inversus
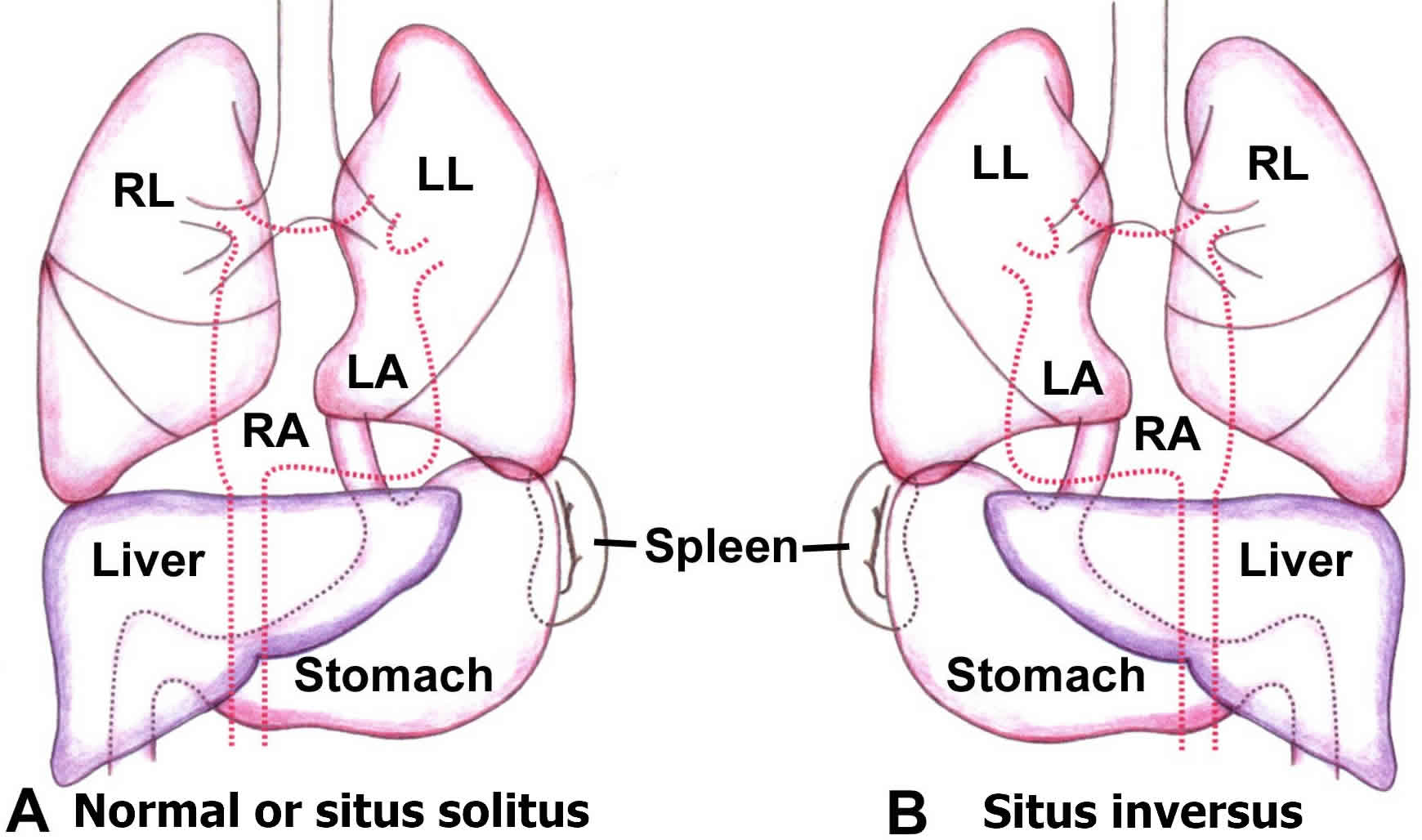
Footnote: Schematic drawings illustrate the standard anatomy of situs solitus (A) and the mirror image of situs inversus (B). The right lung (RL), left lung (LL), right atrium (RA), and left atrium (LA) are shown.
What causes dextrocardia with situs inversus?
The exact cause of dextrocardia with situs inversus is not known, but the condition results from the abnormal positioning of the internal organs during fetal development. More than 60 known genes are important for the proper positioning and patterning of the organs in the body. However, a specific genetic cause of dextrocardia with situs inversus has not been identified and inheritance patterns have not been confirmed in most cases 10.
Some people have dextrocardia with situs inversus as part of an underlying condition called primary ciliary dyskinesia. Primary ciliary dyskinesia can result from changes (mutations) in several different genes, including the DNAI1 and DNAH5 gene; however, the genetic cause is unknown in many families 11.
What other features may be associated with dextrocardia with situs inversus?
Situs inversus with dextrocardia can occur in association with syndromes such as Kartagener syndrome or another primary ciliary dyskinesia. Kartagener syndrome affects about 20% of people with situs inversus; however, only about half of people with Kartagener syndrome have situs inversus. Kartagener syndrome can be diagnosed after birth. Primary ciliary dyskinesia is present in about one fourth of people with situs inversus totalis, and situs inversus totalis is present in nearly half of people with primary ciliary dyskinesia 10
Specific abnormalities that have been associated with situs inversus include incomplete transposition of thoracic (chest) or abdominal organs, various congenital heart defects, polysplenia (more than one spleen), asplenia (absent spleen), annular (ring-shaped) pancreas, horseshoe kidney, and diaphragmatic hernia 12.
The incidence of congenital heart defects is increased to up to 5% in people with situs inversus. Associated heart abnormalities may include ventricular septal defect, tetralogy of Fallot, double outlet right ventricle, and/or complete or corrected transposition of the arteries. Extra-cardiac malformations (affecting parts of the body other than the heart) are not typically found in people with situs inversus with dextrocardia 13.
Are the brains of individuals with situs inversus turned around or otherwise affected by the disease?
Findings from several articles support the concept that brain abnormalities (specifically asymmetry) may be found in individuals who have situs inversus 14. At least one study found evidence which supported the concept that a reversal of more commonly found intracranial anatomy may occur in situs inversus totalis 15.
Dextrocardia causes
The cause of dextrocardia is unclear. Possible risk factors for dextrocardia include a family history of the condition.
Causes of dextrocardia:
- Kartagener syndrome: Also known as primary ciliary dyskinesia. A rare ciliopathic, autosomal recessive genetic disorder that causes defects in the action of cilia lining of the respiratory tract, this is characterized by enlarged bronchial tubes, chronic sinusitis in the lower and upper sinuses, Eustachian tube, middle ear.
- Marden-Walker Syndrome: A rare genetic disorder characterized by blepharophimosis, joint contractures and fixed facial expression.
- Campomelia Cumming type: A rare syndrome characterized by limb and multiple abdominal organ abnormalities. The disorder results in death before birth or soon after.
Dextrocardia prevention
Some syndromes that include dextrocardia may run in families. If you have a family history of heterotaxy, talk to your provider before becoming pregnant.
There are no known ways to prevent dextrocardia. However, avoiding the use of illegal drugs (especially cocaine) before and during pregnancy may lower the risk of this problem.
Talk to your provider if you have diabetes. This condition may contribute to your risk of having a child with certain forms of dextrocardia.
Dextrocardia ECG
The most prominent abnormality recognized is often the “global inversion” of standard (limb) lead I, with inversion of the P wave, QRS complex, and T wave, suggestive of either dextrocardia or limb lead misplacement (the RA, or right arm, lead was placed on the left and vice versa). Use of the precordial leads allows discrimination of these two entiries, specifically by observing the precordial R wave progression.
As one progresses from the right (represented by leads V1-V3) through the left precordium (leads V4-6), a progressive increase in the amplitude of the (first positive QRS deflection) R wave is expected, with poor R wave progression diagnosed when the amplitude of the R wave in V3 is < 3mm (often suggestive of an anteroseptal myocardial infarction of indeterminate age).
Misplaced limb leads will not affect the precordium, therefore a normal R wave progression is expected. Dextrocardia, however, will demonstrate either loss of normal R wave progression (and consequently, PRWP) or a reversal of the normal progression, with dominant S waves present throughout the precordium and R waves decreasing in positivity progressively from right to left.
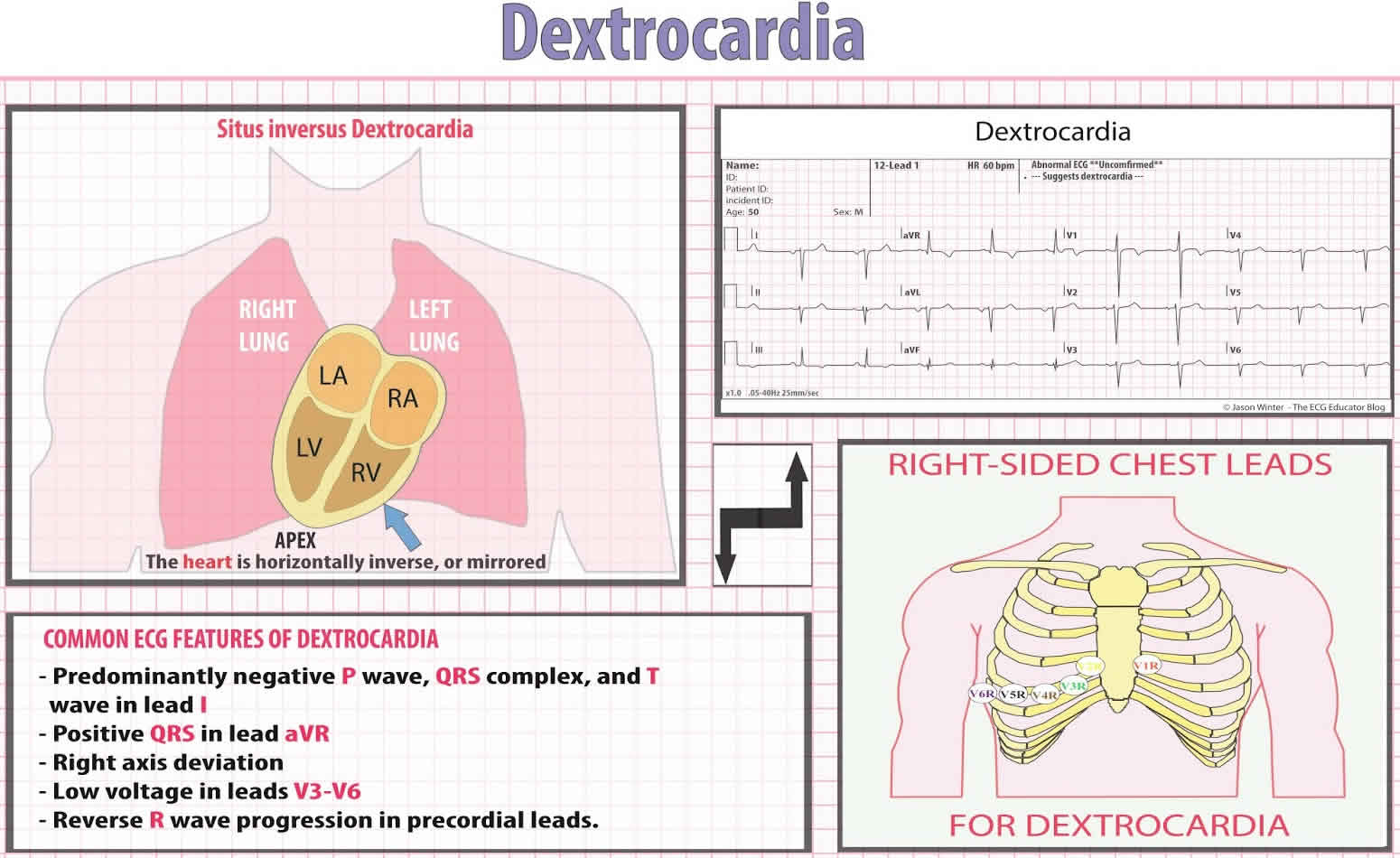
Other common ECG features include:
- Right axis deviation (RAD) (normal axis between -30 and +90)
- Positive QRS complexes (with upright P and T waves) in aVR (usually predominantly negative)
- Lead I: inversion of all complexes, aka ‘global negativity’ (inverted P wave, negative QRS, inverted T wave)
- Absent R-wave progression in the chest leads (dominant S waves throughout)
- Reversal of pattern with inversion of limb leads and precordial leads
Note: ECG leads must be placed in reversed positions on a person with dextrocardia. In addition, when defibrillating someone with dextrocardia, the pads should be placed in reverse positions. That is, instead of upper right and lower left, pads should be placed upper left and lower right.
Things to consider if your patient has dextrocardia and needs pacing/cardioversion or is in cardiac arrest and you have a shockable rhythm.
When defibrillating or pacing the patient with dextrocardia, its is suggested that you place the pads opposite of normal showed in the diagram below. It is suggested that traditional pad placement should be mirrored to the right chest. Anterior/posterior placement should be just right of the mediastinum.
Figure 3. Dextrocardia ECG (situs inversus dextrocardia)
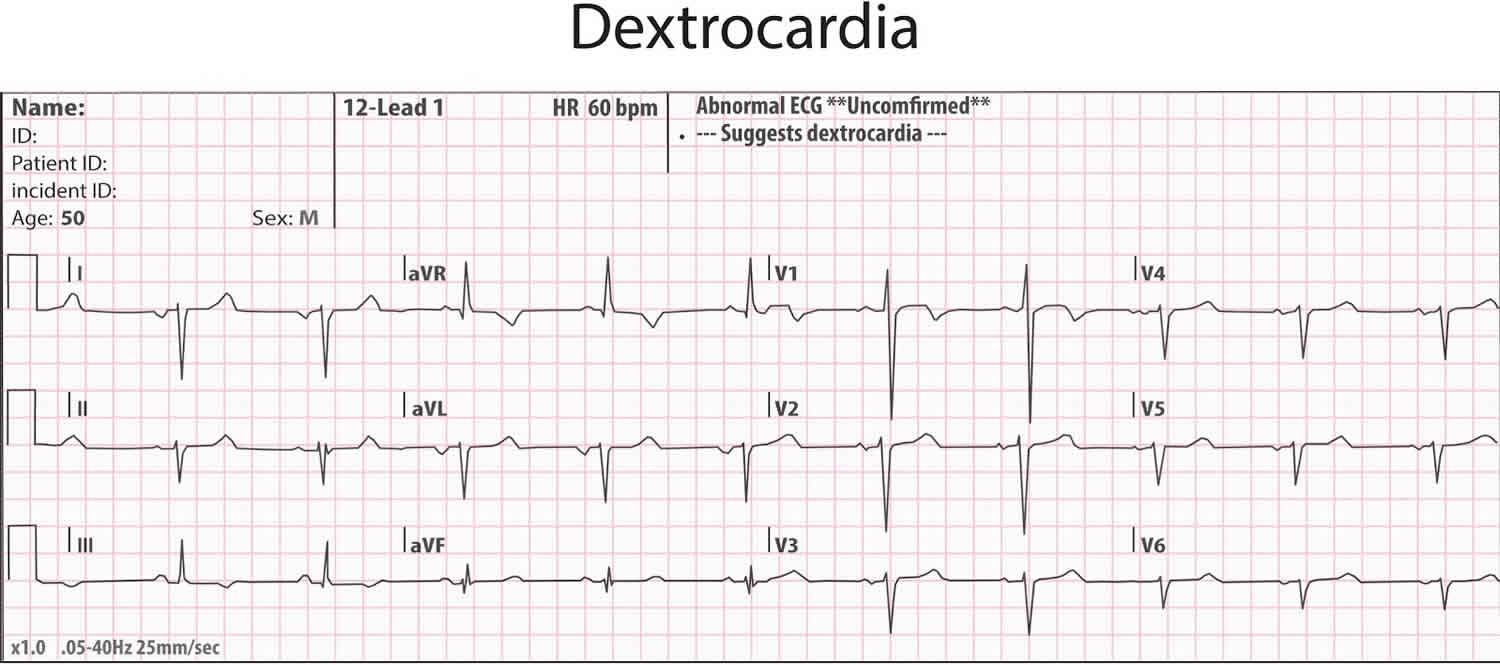
Figure 4. Dextrocardia ECG leads placement
Dextrocardia symptoms
There are no symptoms of dextrocardia if the heart is normal.
Conditions that may include dextrocardia may cause the following symptoms:
- Bluish skin
- Difficulty breathing
- Failure to grow and gain weight
- Fatigue
- Jaundice (yellow skin and eyes)
- Pale skin (pallor)
- Repeated sinus or lung infections
Dextrocardia complications
Complications depend on whether dextrocardia is part of a larger syndrome, and whether other problems exist in the body. Complications include:
- Blocked intestines (due to a condition called intestinal malrotation)
- Heart failure
- Infection (heterotaxy with no spleen)
- Infertility in males (Kartagener syndrome)
- Repeated pneumonias
- Repeated sinus infections (Kartagener syndrome)
- Death
Dextrocardia diagnosis
Your health care provider will perform a physical exam and ask about your symptoms.
Tests to diagnose dextrocardia include:
- Chest x-ray
- CT scan of the heart
- Electrocardiogram
- MRI of the heart
- Echocardiogram
Dextrocardia treatment
A complete mirror image dextrocardia with no heart defects requires no treatment. It is important, however, to let the child’s health care provider know the heart is on the right side of the chest. This information can be important in some exams and tests.
The type of treatment needed depends on the heart or physical problems the infant may have in addition to dextrocardia.
If heart defects are present with dextrocardia, the baby will most likely need surgery. Babies who are very ill may need to take medicines before they can have surgery. These medicines help the baby grow larger so surgery is easier to perform.
Medicines include:
- Water pills (diuretics)
- Drugs that help the heart muscle pump more forcefully (inotropic agents)
- Drugs that lower blood pressure and ease the workload on the heart (ACE inhibitors)
The baby might also need surgery to correct problems in the organs of the abdomen.
Children with Kartagener syndrome will need repeated treatment with antibiotics for sinus infections.
Children with a missing or abnormal spleen need long-term antibiotics.
All children with heart defects may need to take antibiotics before surgeries or dental treatments.
Dextrocardia prognosis
Babies with simple dextrocardia have a normal life expectancy and should have no problems related to the location of the heart.
When dextrocardia appears with other defects in the heart and elsewhere in the body, how well the baby does depends on the severity of the other problems.
Babies and children without a spleen may have frequent infections. This is at least partially preventable with daily antibiotics.
A retrospective review of all diagnoses of dextrocardia due to embryologic development at a tertiary care hospital from 1985 to 2001 was performed 16. Eighty-one cases were identified (48 antenatally). The incidence of dextrocardia was estimated to be 1 in 12,019 pregnancies. Twenty-seven cases were situs solitus, 30 situs inversus, and 24 situs ambiguous or isomerism. Cardiac malformations were found in 26 of 27 cases of situs solitus, 7 of 30 cases of situs inversus, and 24 of 24 cases of isomerism. Noncardiac malformations were identified in 10 of 27 cases of situs solitus, 6 of 30 cases of situs inversus, and 14 of 24 cases of isomerism. Twelve pregnancies were terminated, 3 fetuses were stillborn, and 2 women chose compassionate care. All terminated fetuses were diagnosed with dextrocardia before termination, and all had >1 cardiac anomaly; 7 also had noncardiac anomalies. There were 43 subjects in the intention-to-treat group (20 situs solitus, 10 solitus inversus, 13 isomerism). Thirty-two had ≥1 cardiac operation, and 21 had ≥3. Thirty-nine subjects were alive at most recent follow-up. In conclusion, in this cohort study, the numbers of cases of situs solitus, situs inversus, and isomerism were similar. Cardiac and noncardiac malformations were most common in the isomerism group. Cardiac malformations were often complex in the situs solitus and isomerism groups. Ninety-one percent of those in the intention-to-treat cohort were alive at follow-up 16.
References- Bohun CM, Potts JE, Casey BM et-al. A population-based study of cardiac malformations and outcomes associated with dextrocardia. Am. J. Cardiol. 2007;100 (2): 305-9. doi:10.1016/j.amjcard.2007.02.095
- Dextrocardia. https://radiopaedia.org/cases/dextrocardia-7?lang=us
- Bindra PS, Lin D, Brozena S, Marchlinski F, Dixit S. Case report: Placement of a coronary sinus lead in a patient with dextrocardia and situs inversus. Journal of Interventional Cardiac Electrophysiology. 2006; 16:93-95.
- Situs Inversus Imaging. https://emedicine.medscape.com/article/413679-overview
- Mujo T, Finnegan T, Joshi J, Wilcoxen KA, Reed JC. Situs ambiguous, levocardia, right sided stomach, obstructing duodenal web, and intestinal nonrotation: a case report. J Radiol Case Rep. 2015 Feb. 9 (2):16-23.
- Maldjian PD, Saric M. Approach to dextrocardia in adults: review. AJR Am J Roentgenol. 2007 Jun. 188(6 suppl):S39-49; quiz S35-8.
- Gindes L, Hegesh J, Barkai G, Jacobson JM, Achiron R. Isolated levocardia: prenatal diagnosis, clinical importance, and literature review. J Ultrasound Med. 2007 Mar. 26(3):361-5.
- Schrott-Fischer A, Rieger G, Morass B, Bitsche M, Horak E, Riechelmann H, et al. [Diagnostics of primary ciliary dyskinesia]. Laryngorhinootologie. 2008 Nov. 87(11):809-20; quiz 821-5.
- Lee SE, Kim HY, Jung SE, et al. Situs anomalies and gastrointestinal abnormalities. J Pediatr Surg. 2006 Jul. 41(7):1237-42.
- Heterotaxy Syndrome and Primary Ciliary Dyskinesia. https://emedicine.medscape.com/article/896757-overview
- Primary ciliary dyskinesia. https://ghr.nlm.nih.gov/condition/primary-ciliary-dyskinesia
- Dextrocardia with Situs Inversus. https://rarediseases.org/rare-diseases/dextrocardia-with-situs-inversus
- Alfred Z. Abuhamad, Rabih Chaoui. Fetal Heterotaxy, Left Atrial Isomerism, Right Atrial Isomerism, and Situs Inversus. A Practical Guide to Fetal Echocardiography: Normal and Abnormal Hearts. Philadelphia, PA: Lippincott Williams & Wilkins; 2010
- Masayuki Hirata, Norio Fujimaki, Tetsy Goto, Yuka Umekawa, Norihiko Fujita, Yasushi Terazao, Aumu Matani, Qiang Wei, Toshiki Yoshimine, Shiro Yorifuji, Tsutomu Murata. Neuroimaging study on brain asymmetries in situs inversus totalis. Journal of Neurological Science. January 15, 2010; 288(1-2):72-78. http://www.ncbi.nlm.nih.gov/pubmed/19897211
- Tubbs RS, Wellons JC, Salter G, et al.. Anat Embryol (Berl). 2003; http://www.ncbi.nlm.nih.gov/pubmed/12592571
- A population-based study of cardiac malformations and outcomes associated with dextrocardia. Am J Cardiol. 2007 Jul 15;100(2):305-9. Epub 2007 May 25. https://www.ajconline.org/article/S0002-9149(07)00720-5/fulltext





{kind=link}