What is estradiol
Estradiol (E2) is an estrogen, which is a steroid sex hormone vital for the maintenance of fertility and responsible for the development and function of reproductive organs and the formation of secondary sex characteristics in women. Along with another hormone, progesterone, they help regulate the menstrual cycle, are involved in the growth of breasts and the uterus, and help maintain a healthy pregnancy. Though considered the main sex hormone for women, estradiol is also found in men and play a role in bone metabolism and growth in both sexes. Estradiol also plays a critical role in male sexual function. Estradiol in men is essential for modulating libido, erectile function, and spermatogenesis 1. Estrogen receptors, as well as aromatase, the enzyme that converts testosterone to estrogen, are abundant in brain, penis, and testis, organs important for sexual function in men.
Estradiol (E2) is primarily produced in the ovaries in pre-menopausal women and in the testicles in men. Estradiol (E2) is converted from estrone in post-menopausal women. Estradiol (E2) is the most potent estrogen and the one that is present in the highest concentration in non-pregnant, pre-menopausal women. Estradiol (E2) levels vary depending on a woman’s age and reproductive status. Estradiol (E2) levels are a good marker of ovarian function.
As the primary, most potent estrogen hormone produced by the ovaries, estradiol binds to and activates specific nuclear receptors. Estradiol (E2) exhibits mild anabolic and metabolic properties, and increases blood coagulability.
What is estrogen?
Estrogens are a group of steroids that are responsible for the development and function of reproductive organs and the formation of secondary sex characteristics in women. Along with another hormone, progesterone, they help regulate the menstrual cycle, are involved in the growth of breasts and the uterus, and help maintain a healthy pregnancy. Though considered the main sex hormones for women, estrogens are also found in men and play nongender-specific processes in bone metabolism/remodeling, growth, nervous system maturation and endothelial responsiveness in both sexes.
The 2 major biologically active estrogens in nonpregnant humans are estrone (E1) and estradiol (E2). A third bioactive estrogen, estriol (E3), is the main pregnancy estrogen, but plays no significant role in nonpregnant women or men.
- Estrone (E1) is directly converted from androstenedione (from the adrenal gland) or indirectly from other androgens. Estrone (E1) can also be produced by the ovaries and placenta, testicles, and adipose (fat) tissues. Estradiol (E2) and estrone (E1) can be converted into each other as needed. Estrone (E1) is the primary estrogen in men and in post-menopausal women.
- Estradiol (E2) is primarily produced in the ovaries in pre-menopausal women and in the testicles in men. Estradiol (E2) is converted from estrone (E1) in post-menopausal women. It is the most potent estrogen and the one that is present in the highest concentration in non-pregnant, pre-menopausal women. Estradiol (E2) levels vary depending on a woman’s age and reproductive status. They are a good marker of ovarian function.
- Estriol (E3) is produced by the placenta, with concentrations rising throughout a woman’s pregnancy. Increasing levels are an indication of the health of the pregnancy and developing baby. Estriol (E3) is part of the second trimester maternal serum screen, a test performed to evaluate fetal risk due to certain chromosomal abnormalities. Very low levels of estriol (E3) are present in non-pregnant women or men.
Estradiol (E2) is produced primarily in ovaries and testes by aromatization of testosterone. Small amounts are produced in the adrenal glands and some peripheral tissues, most notably fat. By contrast, most of the circulating estrone (E1) is derived from peripheral aromatization of androstenedione (mainly adrenal). Estradiol (E2) and estrone (E1) can be converted into each other, and both can be inactivated via hydroxylation and conjugation. Estradiol (E2) demonstrates 1.25 to 5 times the biological potency of estrone (E1). Estradiol (E2) circulates at 1.5 to 4 times the concentration of estrone (E1) in premenopausal, nonpregnant women. Estradiol (E2) levels in men and postmenopausal women are much lower than in nonpregnant women, while estrone (E1) levels differ less, resulting in a reversal of the premenopausal E2:E1 ratio. Estradiol (E2) levels in premenopausal women fluctuate during the menstrual cycle. They are lowest during the early follicular phase. Estradiol (E2) levels then rise gradually until 2 to 3 days before ovulation, at which stage they start to increase much more rapidly and peak just before the ovulation-inducing luteinizing hormone (LH)/follicle stimulating hormone (FSH) surge at 5 to 10 times the early follicular levels. This is followed by a modest decline during the ovulatory phase. Estradiol (E2) levels then increase again gradually until the midpoint of the luteal phase and, thereafter, decline to trough, early follicular levels.
Measurement of serum estradiol (E2) forms an integral part of the assessment of reproductive function in females, including assessment of infertility, oligo-amenorrhea, and menopausal status. In addition, it is widely used for monitoring ovulation induction, as well as during preparation for in vitro fertilization (IVF). For these applications estradiol (E2) measurements with modestly sensitive assays suffice. However, extra sensitive estradiol (E2) assays, simultaneous measurement of estrone (E1), or both are needed in a number of other clinical situations. These include inborn errors of sex steroid metabolism, disorders of puberty, estrogen deficiency in men, fracture risk assessment in menopausal women, and increasingly, therapeutic drug monitoring, either in the context of low-dose female hormone replacement therapy or antiestrogen treatment.
Do all men have estrogens?
Yes. Although they are present in amounts far less than in women, they are present and are needed for hormonal balance and the function of other glands.
What are estrogen receptors?
Estrogen receptors are proteins in cells from certain tissues that bind with estrogen. This binding allows estrogen to act on these tissues. Tumors can also have estrogen receptors. Estrogen can stimulate the growth of estrogen receptor-positive tumors in women who have breast cancer. Drugs that block the effect of estrogen may slow the rate of growth of such cancers.
What are phytoestrogens and environmental estrogens?
Phytoestrogens are estrogen-like compounds from plant sources. The two main classes are isoflavones, found in soy products, and lignans, found in whole grains and some fruits and vegetables. It has been proposed that these products could be used as an alternative to hormone replacement therapy (HRT). Initial studies have shown the relief of some menopausal symptoms, such as hot flashes, but there is more research yet to be done.
Environmental estrogens are chemicals, either natural (such as plant sources) or man-made (such as the insecticide DDT), that mimic the effect of estrogen and may cause disorders such as infertility, overgrowth of the endometrial lining, premature breast development, and feminization in young males. They tend to stay in the body for long periods of time and are being studied for their long-term effects.
Normal estradiol levels
Children
The reference ranges for children are based on the published literature 2.
- 1-14 days: Estradiol levels in newborns are very elevated at birth but will fall to prepubertal levels within a few days.
Table 1. Males estradiol level chart
| Tanner Stages# | Mean Age | Reference Range |
| Stage I (>14 days and prepubertal) | 7.1 years | Undetectable-13 pg/mL |
| Stage II | 12.1 years | Undetectable-16 pg/mL |
| Stage III | 13.6 years | Undetectable-26 pg/mL |
| Stage IV | 15.1 years | Undetectable-38 pg/mL |
| Stage V | 18 years | 10-40 pg/mL |
#Puberty onset (transition from Tanner stage I to Tanner stage II) occurs for boys at a median age of 11.5 (+/- 2) years. For boys, there is no proven relationship between puberty onset and body weight or ethnic origin. Progression through Tanner stages is variable. Tanner stage V (adult) should be reached by age 18.
Table 2. Females estradiol level chart
| Tanner Stages# | Mean Age | Reference Range |
| Stage I (>14 days and prepubertal) | 7.1 years | Undetectable-20 pg/mL |
| Stage II | 10.5 years | Undetectable-24 pg/mL |
| Stage III | 11.6 years | Undetectable-60 pg/mL |
| Stage IV | 12.3 years | 15-85 pg/mL |
| Stage V | 14.5 years | 15-350 pg/mL** |
#Puberty onset (transition from Tanner stage I to Tanner stage II) occurs for girls at a median age of 10.5 (+/- 2) years. There is evidence that it may occur up to 1 year earlier in obese girls and in African American girls. Progression through Tanner stages is variable. Tanner stage V (adult) should be reached by age 18.
Adults
- Males: 10-40 pg/mL
- Females
- Premenopausal: 15-350 pg/mL. Estradiol (E2) levels vary widely through the menstrual cycle.
- Postmenopausal: <10 pg/mL
Conversion factor
Estradiol (E2): pg/mL x 3.676=pmol/L (molecular weight=272)
Estrogen in Girls and Women
The types and amounts of estrogen normally present in a woman’s blood will vary throughout her lifetime. Levels vary during each menstrual cycle, during pregnancy, and on a daily basis.
At Birth
Estradiol (E2) and estrone (E1) are high but fall within a few days. Concentration levels are minimal during early childhood.
At Puberty
Concentrations of estradiol (E2) and estrone (E1) begin to rise as puberty approaches. These estrogens are responsible for the development of breasts, uterine growth, and (with other hormones) the onset and regulation of menstruation. A moderate amount of estrone (E1) is present from puberty to menopause. This concentration will vary during the day but is otherwise relatively stable.
During Menstruation
The menstrual cycle is approximately 28 days long and consists of two phases, follicular phase and luteal phase. During each cycle, estradiol (E2) and several other hormones normally rise and then fall in a specific sequence.
Figure 1. Ovarian activity during the Menstrual cycle
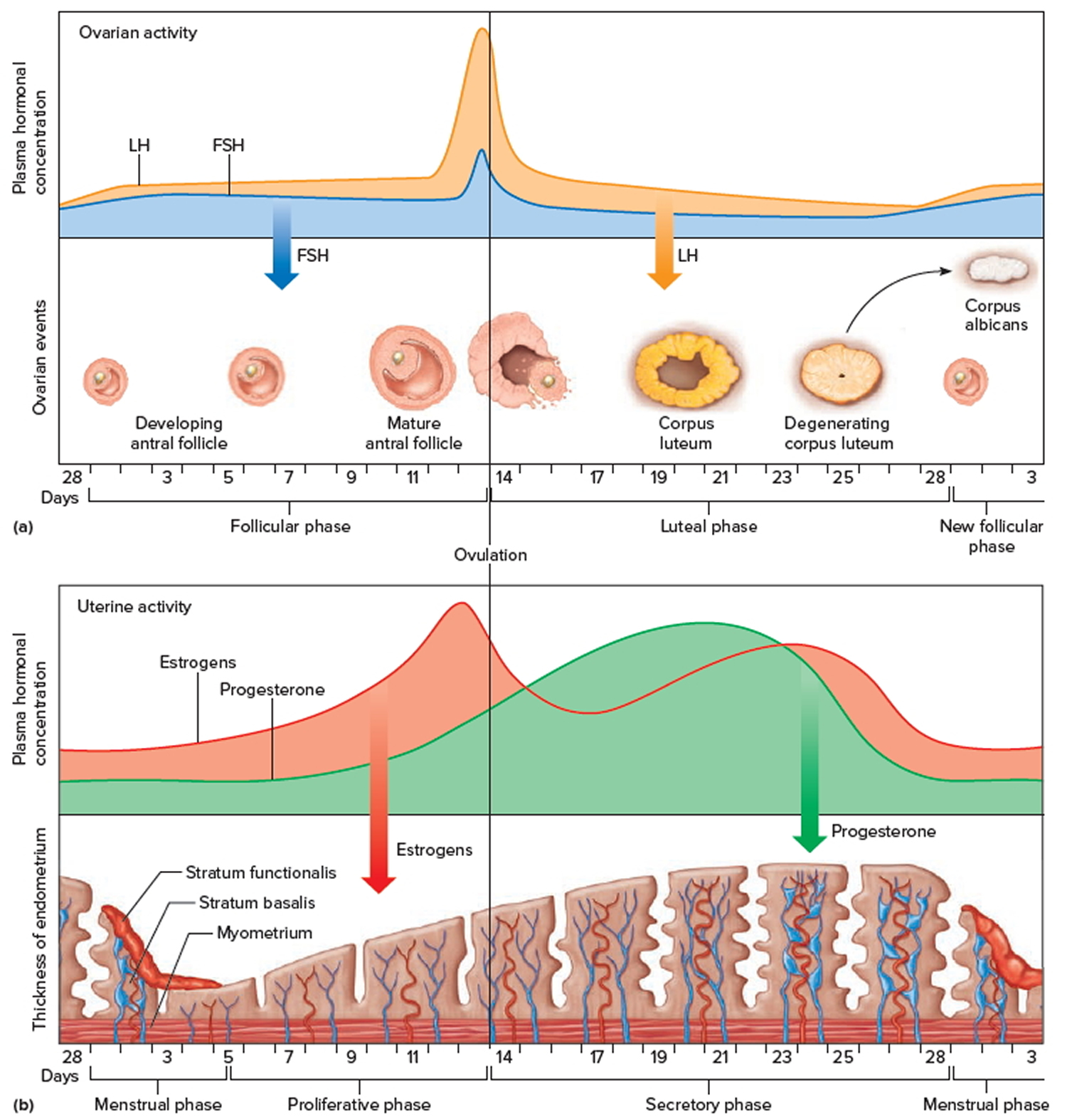
Note: Major events in the female menstrual cycle. (a) Plasma hormonal concentrations of follicle-stimulating hormone (FSH) and luteinizing hormone (LH) affect follicle maturation in the ovaries. (b) Plasma hormonal concentrations of estrogen and progesterone influence changes in the uterine lining.
Estradiol (E2) levels change during the menstrual cycle, as follows:
- Post-menses, levels may be as low as 15 pg/mL
- Levels then rise during the follicular phase to a preovulatory peak, typically in the 300+ pg/mL range
- Levels fall in the luteal phase
- Menses typically occur when Estradiol (E2) levels are in the 50 to 100 pg/mL range
Estradiol (E2) analysis may be helpful in establishing time of ovulation and optimal time for conception. Optimal time for conception is within 48 to 72 hours following the midcycle estradiol (E2) peak. Serial specimens must be drawn over several days to evaluate baseline and peak total estrogen [Estrone (E1) + Estradiol (E2)] levels. Low baseline levels and a lack of rise, as well as persistent high levels without midcycle rise, are indicative of anovulatory cycles.
For determining the timing of initiation of ovarian stimulation in invitro-fertilization (IVF) studies, low levels (around 30 pg/mL) before stimulation, are critical, as higher values often are associated with poor stimulation cycles.
Estrogen replacement in reproductive-age women should aim to mimic natural estrogen levels as closely as possible. Estradiol (E2) levels should be within the reference range for premenopausal women, LH/FSH should be within the normal range, and Estradiol (E2) levels should ideally be higher than Estrone (E1) levels.
During Pregnancy
Estriol (E3) is the primary estrogen present during pregnancy. It is produced by the placenta, starts to rise in the eighth week of pregnancy, and continues to rise throughout the pregnancy. A sharp increase of estriol (E3) occurs approximately 4 weeks prior to the onset of labor. Estriol (E3) circulating in maternal blood is quickly cleared out of the body. Each measurement of estriol is a snapshot of what is happening with the placenta and fetus, but there is also natural daily variation in estriol concentrations.
Estrone (E1) also rises during pregnancy, increasing as much as 10 fold between weeks 24 and 41. After delivery, estrone (E1) falls and estriol (E3) again becomes essentially undetectable.
During Menopause
Estrone (E1) is the primary estrogen present during menopause. Estradiol (E2) concentrations significantly decrease as ovarian production wanes and eventually stabilize at a low level.
The current recommendations for postmenopausal female hormone replacement are to administer therapy in the smallest beneficial doses for as briefly as possible. Ideally, Estradiol (E2) and Estrone (E1) levels should be held below, or near, the lower limit of the premenopausal female reference range.
Postmenopausal women and older men in the lowest quartile of Estradiol (E2) levels are at increased risk of osteoporotic fractures. Estradiol (E2) levels are typically less than 5 pg/mL in these patients.
Estrogen in Boys and Men
The types and amounts of estrogen normally present in a man’s blood change, but they vary much less over time than a woman’s and they are much lower.
Estradiol test
Estrogen tests are used to detect a deficiency or excess in a woman and to help diagnose a variety of conditions associated with this imbalance. Estrogen tests may also be used to help determine the timing of a woman’s ovulation and may be ordered to monitor the health status of the developing baby and placenta during pregnancy. In a man, estrogen testing may be performed to detect a hormone excess and its cause.
Estrogen tests measure one of three components: estrone (E1), estradiol (E2), or estriol (E3) in the blood or urine. These tests each have different uses.
Blood and urine results are not interchangeable. Your health practitioner will choose which estrogen and sample type to test. In addition to blood and urine, estrogen testing is occasionally also performed on saliva or on amniotic fluid.
Beyond daily and cycle variations, illnesses such as high blood pressure (hypertension), anemia, and impaired liver and kidney function can affect estrogen levels.
Some drugs, such as glucocorticosteroids, ampicillin, estrogen-containing drugs, phenothiazines, and tetracyclines, can increase estrogen levels in the blood. Glucose in the urine and urinary tract infections can increase levels in the urine. Drugs that may decrease levels include clomiphene and oral contraceptives.
Cautions
Fulvestrant is a member of a new class of drugs called “selective estrogen receptor degraders” (SERDS).
Fulvestrant has modest cross reactivity (1%-5%) in estradiol immunoassays, but because the peak dose levels of this drug are between 10-fold (reproductive age women) and greater than 200-fold (postmenopausal women) higher than the naturally circulating estradiol concentrations in the treated women, this causes dramatically false-high estradiol results in immunoassays, when blood sampling occurs in close temporal proximity to dosing.
By contrast, estradiol measurements by mass spectrometry display greater than 1000-fold lower cross reactivity (<0.001%), meaning that the impact of Fulvestrant on serum estradiol measurements by mass spectrometry is negligible, even if blood sampling occurs at peak dose.
In Girls and Women
Estradiol (E2) and/or estrone (E1) testing may be ordered to:
- Help diagnose early-onset puberty, when a young girl develops secondary sex characteristics sooner than expected;
- As part of the diagnosis and workup of precocious and delayed puberty, when a girl shows delayed development of secondary sex characteristics or start of menstruation
- Investigate menstrual abnormalities, such as lack of menstrual periods (amenorrhea), infertility, and abnormal vaginal bleeding
- As part of the diagnosis and workup of suspected disorders of sex steroid metabolism (e.g, aromatase deficiency and 17 alpha-hydroxylase deficiency)
- Evaluation of hypogonadism and oligo-amenorrhea in females
- Evaluate the function of the ovaries and detect ovarian failure
- Assessing ovarian status, including follicle development, for assisted reproduction protocols (e.g, in vitro fertilization)
- Monitor follicle development in the ovary in the days prior to in vitro fertilization (IVF) by making serial measurements of estradiol
- Monitor hormone replacement therapy that is given to assist fertility
- In conjunction with luteinizing hormone (LH) measurements, monitoring of estrogen replacement therapy in hypogonadal premenopausal women
- Monitor menopausal hormone replacement therapy that is given to alleviate symptoms associated with estrogen deficiency in postmenopausal women
- As an adjunct to clinical assessment, imaging studies and bone mineral density measurement in the fracture risk assessment of postmenopausal women, and, to a lesser degree, older men
- Detect estrogen-producing tumors
- Monitor anti-estrogen therapy (e.g, aromatase inhibitor therapy), as in breast cancer
Estriol (E3) testing:
- May sometimes be ordered serially to help monitor a high-risk pregnancy; when it is used this way, each sample should be drawn at the same time each day.
- An unconjugated estriol test is one of the components of second trimester maternal serum screening. Decreased levels have been associated with various genetic disorders, including Down syndrome, neural tube defects, and adrenal abnormalities.
In Boys and Men
Estradiol (E2) and/or estrone (E1) testing in boys or men may be ordered to:
- Help diagnose delayed puberty
- Help diagnose the cause of enlarged breasts (gynecomastia) or other signs of feminization
- Detect a relative estrogen excess that is due to a testosterone or androgen deficiency
- Detect estrogen-producing tumors
When is estrogen test ordered?
In Girls and Women
Estradiol (E2) and/or estrone (E1) testing in girls and women may be ordered when:
- A girl’s sex organs develop earlier or later than normally expected
- A woman has symptoms such as abnormal vaginal bleeding after menopause or abnormal or lack of menstrual cycles
- A woman is experiencing infertility; a series of estradiol measurements over the course of a woman’s menstrual cycle may be done to monitor follicle development prior to in vitro fertilization techniques (timed with a surge in estradiol).
- A woman is having symptoms of menopause, including hot flashes, night sweats, insomnia, and/or irregular or lack of menstrual periods
- A menopausal woman is taking hormone replacement therapy; her health practitioner may periodically order estrone levels to monitor treatment.
Estriol (E3) testing in women may be ordered:
- During pregnancy, a health practitioner may order serial estriol samples to look for a trend, whether there is a rise or fall in the estriol level over time.
- Unconjugated estriol is often measured in the 15th to 20th week of gestation as part of the triple/quad screen.
In Boys and Men
Estradiol (E2) and/or estrone (E1) testing in boys and men may be ordered when:
- A boy has delayed puberty, characterized by delayed development of muscle mass, lack of deepening of the voice or growth of body hair, slow or delayed growth of testicles and penis
- A man shows signs of feminization, such as enlarged breasts
What does abnormal estrogen test result mean?
Normal estrogen results depend upon the sex and age of the person being tested. With women, it also depends upon their menstrual cycle or whether they are pregnant. Reference ranges will vary somewhat between laboratories, both in normal values listed and in units used.
Increased or decreased levels of estrogens are seen in many metabolic conditions. Care must be used in the interpretation of estrone, estradiol, and estriol results because the levels vary on a day-to-day basis and throughout a woman’s menstrual cycle.
A health practitioner who is monitoring a woman’s hormones will be looking at trends in the levels, rising or lowering over time in conjunction with the menstrual cycle or pregnancy rather than evaluating single values. Test results are not diagnostic of a specific condition but give the health practitioner information about the potential cause of a person’s symptoms or status.
Below are conditions with which one might see an increase or decrease of estrogen levels.
Increased levels of estradiol or estrone
Girls and Women:
- Early (precocious) puberty
- Tumors of the ovary or adrenal glands
The gonadotrophin-releasing hormone stimulation test remains the central part of the workup for precocious puberty. However, baseline sex steroid and gonadotrophin measurements also are important. Prepubertal girls have estradiol (E2) levels below 10 pg/mL (most <5 pg/mL). Levels in prepubertal boys are less than half the levels seen in girls. LH/FSH are very low or undetectable. Estrone (E1) levels also are low, but may rise slightly in obese children after onset of adrenarche. Estradiol (E2), which is produced in the gonads, should remain low in these children. In true precocious puberty, both estradiol (E2) and LH/FSH levels are elevated above the prepubertal range. Elevation of estradiol (E2) or estrone (E1) alone suggests pseudo-precocious puberty, possibly due to a sex steroid-producing tumor.
Boys and Men:
- Enlarged breasts (gynecomastia)
- Tumors of the testicles (testicular cancer) or adrenal glands
- Delayed puberty
Gynecomastia or other signs of feminization in males may be due to an absolute or relative (in relation to androgens) surplus of estrogens. Gynecomastia is common during puberty in boys. Unless estradiol (E2), estrone (E1), or testosterone levels exceed the adult male reference range, the condition is usually not due to hormonal disease (though it sometimes may still result in persistent breast tissue, which later needs to be surgically removed). For adults with gynecomastia, the workup should include testosterone and adrenal androgen measurements, in addition to estradiol (E2) and estrone (E1) measurements. Causes for increased estrone (E1) or estradiol (E2) levels include:
- High androgen levels caused by tumors or androgen therapy (medical or sport performance enhancing), with secondary elevations in estradiol (E2) and estrone (E1) due to aromatization
- Obesity with increased tissue production of estrone (E1)
- Decreased estradiol (E2) and estrone (E1) clearance in liver disease
- Estrogen producing tumors
- Estrogen ingestion
Normal male estradiol (E2) and estrone (E1) levels also may be associated with feminization or gynecomastia, if bioavailable testosterone levels are low due to primary/secondary testicular failure. This may occur, for example, when patients are receiving antiandrogen therapy or other drugs with antiandrogenic effects (e.g, spironolactone, digitalis preparations).
Both Women and Men:
- Hyperthyroidism
- Cirrhosis
In women, decreased levels of estrogen
- Turner syndrome, an inherited condition in women caused by a missing or abnormal X chromosome and characterized by underdeveloped female sex characteristics
- Low level of pituitary hormones (hypopituitarism)
- Dysfunction of the ovaries (female hypogonadism)
- Failing pregnancy (estriol)
- Eating disorders such as anorexia nervosa
- After menopause (estradiol)
- PCOS (Polycystic ovarian syndrome, Stein-Levanthal syndrome)
- Extreme endurance exercise
Girls with delayed puberty
In delayed puberty, estrogens and gonadotrophins are in the prepubertal range. A rise over time predicts the spontaneous onset of puberty. Persistently low estrogens and elevated gonadotrophins suggest primary ovarian failure, while low gonadotrophins suggest hypogonadotrophic hypogonadism. In this latter case, Kallmann syndrome (or related disorders) or hypothalamic/pituitary tumors should be excluded in well-nourished children.
Both Women and Men:
Inherited disorders of sex steroid metabolism are usually associated with production abnormalities of other steroids, most notably a lack of cortisol. Aromatase deficiency is not associated with cortisol abnormalities and usually results in some degree of masculinization in affected females, as well as primary failure of puberty. Males may show delayed puberty and delayed epiphyseal closure, as well as low bone-density. Estradiol (E2) and estrone (E1) levels are very low or undetectable. Various forms of testicular feminization are due to problems in androgen signaling pathways and are associated with female (or feminized) phenotypes in genetic males. Estradiol (E2) and estrone (E1) levels are above the male reference range, usually within the female reference range, and testosterone levels are very high.
Interpretation of abnormal estrogen test results
Estradiol (E2) levels below the premenopausal reference range in young females indicate hypogonadism. If luteinizing hormone (LH) and follicle stimulating hormone (FSH) levels are elevated, primary gonadal failure is diagnosed. The main causes are genetic (e.g, Turner syndrome, familial premature ovarian failure), autoimmune (eg, autoimmune ovarian failure, possibly as part of autoimmune polyglandular endocrine failure syndrome type II), and toxic (eg, related to chemotherapy or radiation therapy for malignant disease). If LH/FSH levels are low or inappropriately “normal,” a diagnosis of hypogonadotrophic hypogonadism is made. This can have functional causes, such as starvation, overexercise, severe physical or emotional stress, and heavy drug and/or alcohol use. It also can be caused by organic disease of the hypothalamus or pituitary. Further workup is usually necessary, typically including measurement of pituitary hormones (particularly prolactin), and possibly imaging.
Irregular or absent menstrual periods with normal or high estradiol (E2) levels (and often high estrone E1 levels) are indicative of possible polycystic ovarian syndrome (PCOS), androgen producing tumors, or estrogen producing tumors. Further workup is required and usually includes measurement of total and bioavailable testosterone, androstenedione, dehydroepiandrosterone (sulfate), sex hormone-binding globulin, and possibly imaging.
Antiestrogen therapy with central or peripheral acting agents that are not pure receptor antagonists usually aims for complete suppression of estradiol (E2) production, and in the case of aromatase inhibitors, complete estrone (E1) and estradiol (E2) suppression.
Estradiol in men
Estradiol also plays a critical role in male sexual function. Estradiol in men is essential for modulating libido, erectile function, and spermatogenesis 1. Estrogen receptors, as well as aromatase, the enzyme that converts testosterone to estrogen, are abundant in brain, penis, and testis, organs important for sexual function. In the brain, estradiol synthesis is increased in areas related to sexual arousal. In addition, in the penis, estrogen receptors are found throughout the corpus cavernosum with high concentration around neurovascular bundles. Low testosterone and elevated estrogen increase the incidence of erectile dysfunction independently of one another. In the testes, spermatogenesis is modulated at every level by estrogen, starting with the hypothalamus-pituitary-gonadal axis, followed by the Leydig, Sertoli, and germ cells, and finishing with the ductal epithelium, epididymis, and mature sperm. Regulation of testicular cells by estradiol shows both an inhibitory and a stimulatory influence, indicating an intricate symphony of dose-dependent and temporally sensitive modulation.
Role of estradiol in the brain
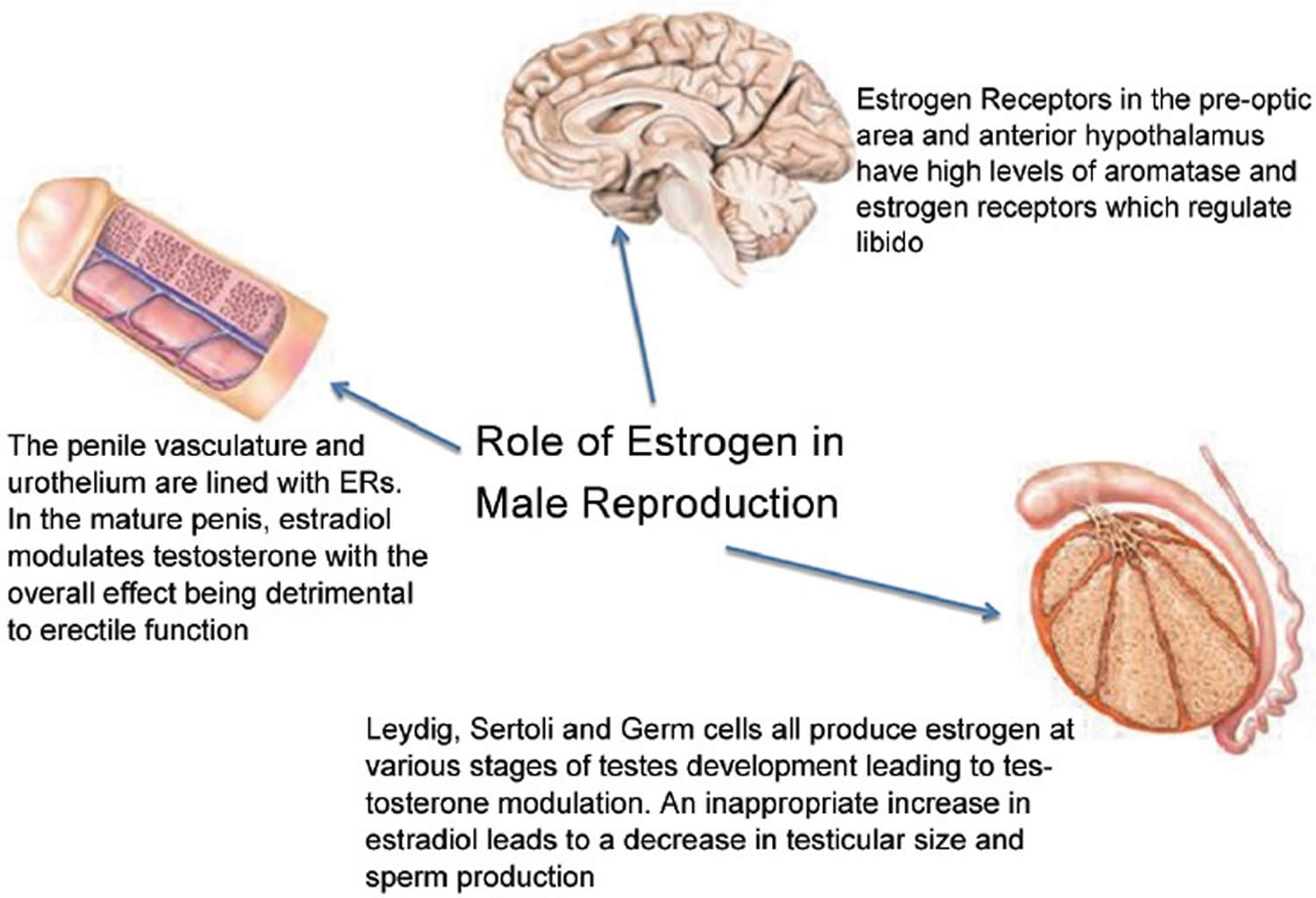
The effect of estradiol on libido is seen at various levels of regulation, starting with direct effects in the brain (Figure 2). Areas of the brain that control sexual behavior in mammals are thought to do so via pheromones that induce specific sexual effects on the autonomic nervous system, including changes in mood and sexual arousal 1. Pheromones produce increased activity in the medial preoptic area/anterior hypothalamus 3. Neurons, the most basic electrical information-transmitting cells in the central nervous system and peripheral nervous system, as well as astrocytes, star-shaped glial cells which fulfill a number of functions in the central nervous system, both convert testosterone to estrogen with aromatase 1. The preoptic area and anterior hypothalamus contain the highest levels of aromatase and estrogen receptors (ERs) in male rodents 4. Similarly, it is well known that selective serotonin reuptake inhibitors (SSRIs) diminish libido. Serotonin receptors follow a pattern of distribution similar to that of estrogen receptors (ERs) in the brain 5. However, the interaction of estradiol and serotonin is complex. Finally, aromatase activity is highest in the brain during development. Thus, not only does estradiol modulate sexual behavior in the adult male, it also appears to organize the early brain to program sexual behavior 6.
Figure 2. Estrogen role in male reproduction
 [Source 1]
[Source 1]
Role of estradiol in hypogonadal men treated with testosterone supplementation therapy
Perhaps, most relevant to the discussion is the use of testosterone supplementation therapy. The goal of testosterone supplementation therapy, regardless of the method used, should be to maintain not only physiologic levels of testosterone, but also its metabolites, including estradiol which optimizes libido 7.
In men with secondary hypogonadism (functioning testes and relatively low levels of luteinizing hormone [LH] and testosterone), clomiphene citrate was used to increase testosterone by acting centrally on the estrogen receptor weakly. Clomiphene citrate administration raised endogenous testosterone while increasing the testosterone to estradiol (T/E) ratio 8. Also, in a later study, clomiphene citrate administered to hypogonadal men produced an increase in libido, energy, and sense of well-being 9.
In 2013, Finkelstein et al. 10 looked at the effects of testosterone and estrogen on male sexual function. They found that the administration of testosterone with and without aromatase inhibitors markedly impaired sexual function when aromatization was inhibited. In addition, a study by Ramasamy et al. 11 in 2014 showed that libido was increased in men receiving testosterone supplementation therapy when testosterone levels were >300 ng/dl and estradiol levels were >5 ng/dl. Most compelling is the fact that in men with serum testosterone <300 ng/dl, sexual drive was seen to be markedly higher when estradiol levels were >5 ng/dl. In addition, when patients with low testosterone were treated with letrozole, a potent aromatase inhibitor, libido was decreased, suggesting that complete elimination of estradiol and decreasing the testosterone/estradiol ratio too severely, adversely affects sexual desire in men 12. These studies provide evidence that both estrogen and testosterone are necessary for normal libido in testosterone-deficient men. Clinically, the dependence of libido in hypogonadal men on both testosterone and estrogen indicates that a cautious approach to the use of aromatase inhibitors is warranted and that the testosterone/estradiol ratio has an impact. It might be reasonable that while prescribing testosterone supplementation therapy one should monitor the levels of both testosterone and estrogen and their relationship to each other.
Clearly, the effect of estradiol on male sexual desire is linked to testosterone levels, as there are different outcomes when estrogen is administered at low and normal testosterone levels. Another example of this duality is seen in men with androgen resistance, where unfettered estrogen is able to stimulate subsequent breast development. However, in men with normal androgen receptor activity, estradiol is unable to stimulate breast development 13. This is thought to be due to an imbalance between the inhibitory and stimulatory effect of these hormones 14. Whatever the pathophysiology in breast development or libido, these hormones seem to be inextricably linked in the complicated physiology of male sexuality and development.
Finally, the effect of estradiol on mood must be considered. As mood can correlate with sexual interest, it is reasonable to consider these data when discussing the role of estradiol on libido. While cognition, well-being, and depressive symptoms improve in men whose low testosterone levels were corrected 15, higher levels of estrogen also have been associated with less depression in older patients of both sexes 16. In addition, estrogen supports serotonin levels and affects the amount of serotonin (5-HT) receptors in the brain, and depending on receptor subtype, there is sexual inhibition or facilitation 17. A recent study showed a significant positive correlation between endogenous plasma estradiol levels and cortical serotonin 2A (5-HT2A) binding in men, with no independent effects on these receptors from testosterone 18. In addition, when serotonin binds to these serotonin 2A (5-HT2A) receptors in the cortex, limbic system, hypothalamus, and midbrain, sexual desire is inhibited with subsequent induction of refractoriness and sexual satiety 19. The interaction of estrogen with serotonin is complex, with overlapping influences that reaches beyond sexual desire including mood regulation and cognition 20. This fact makes its true impact on sexual desire and behavior difficult to fully elucidate.
Estradiol in men summary
The exact role of estradiol in each area of male sexual function including libido, erectile function, and spermatogenesis, is difficult to determine 1. A complex balance of testosterone, estradiol, aromatase, and estrogen receptors (ERs) in the testes, penis, and brain confirms an indispensable and highly regulated hormonal interaction of estrogen in the male. Estrogen receptors (ERs) and aromatase share topographic locations with pheromones in the brain, making it clear that estrogen contributes to early sexual development as well as sexual behavior in adulthood. Estrogen can sustain libido as well as affect the amount of serotonin receptors in the brain modulating mood, mental state, cognition, and emotion. Erectile function is adversely affected by estrogen exposure in early penile development, and exposure to estradiol in the mature penis leads to increased vascular permeability with increased erectile dysfunction (ED). Erectile dysfunction (ED) from increased estradiol exposure is independent of testosterone level 1. In addition, spermatogenesis is dependent upon estradiol to some extent, as all cells involved in the process of sperm production contain aromatase and express estrogen receptors (ERs). Finally, estradiol levels should be considered when treating men with testosterone supplementation therapy, as estradiol levels below 5 ng/dl correlate to a decrease in libido. Considering the complexity and taking into account some conflicting data, more research is necessary so that when better understood, estradiol can become clinically useful in treating diminished libido, erectile dysfunction (ED), and perhaps even oligospermia.
Estradiol dosage
Estrogen increases the risk that you will develop endometrial cancer (cancer of the lining of the uterus [womb]). The longer you take estrogen, the greater the risk that you will develop endometrial cancer. If you have not had a hysterectomy (surgery to remove the uterus), you should be given another medication called a progestin to take with estrogen. This may decrease your risk of developing endometrial cancer, but may increase your risk of developing certain other health problems, including breast cancer. Before you begin taking estrogen, tell your doctor if you have or have ever had cancer and if you have unusual vaginal bleeding. Call your doctor immediately if you have abnormal or unusual vaginal bleeding during your treatment with estrogen. Your doctor will watch you closely to help ensure you do not develop endometrial cancer during or after your treatment.
In a large study, women who took estrogen with progestins had a higher risk of heart attacks, strokes, blood clots in the lungs or legs, breast cancer, and dementia (loss of ability to think, learn, and understand). Women who take estrogen alone may also have a higher risk of developing these conditions. Tell your doctor if you smoke or use tobacco, if you have had a heart attack or a stroke in the past year, and if you or anyone in your family has or has ever had blood clots or breast cancer. Also tell your doctor if you have or have ever had high blood pressure, high blood levels of cholesterol or fats, diabetes, heart disease, lupus (a condition in which the body attacks its own tissues causing damage and swelling), breast lumps, or an abnormal mammogram (x-ray of the breast used to find breast cancer).
The following symptoms can be signs of the serious health conditions listed above. Call your doctor immediately if you experience any of the following symptoms while you are taking estrogen: sudden, severe headache; sudden, severe vomiting; speech problems; dizziness or faintness; sudden complete or partial loss of vision;double vision; weakness or numbness of an arm or a leg; crushing chest pain or chest heaviness; coughing up blood; sudden shortness of breath; difficulty thinking clearly, remembering, or learning new things; breast lumps or other breast changes; discharge from nipples; or pain, tenderness, or redness in one leg.
You can take steps to decrease the risk that you will develop a serious health problem while you are taking estrogen. Do not take estrogen alone or with a progestin to prevent heart disease, heart attacks, strokes, or dementia. Take the lowest dose of estrogen that controls your symptoms and only take estrogen as long as needed. Talk to your doctor every 3 to 6 months to decide if you should take a lower dose of estrogen or should stop taking the medication.
You should examine your breasts every month and have a mammogram and a breast exam performed by a doctor every year to help detect breast cancer as early as possible. Your doctor will tell you how to properly examine your breasts and whether you should have these exams more often than once a year because of your personal or family medical history.
Tell your doctor if you are having surgery or will be on bed rest. Your doctor may tell you to stop taking estrogen 4 to 6 weeks before the surgery or bed rest to decrease the risk that you will develop blood clots.
Talk to your doctor regularly about the risks and benefits of taking estrogen.
Adult Dose for Postmenopausal Symptoms
- Depo-estradiol (estradiol cypionate) for injection: Usual dose: 1 to 5 mg intramuscularly every 3 to 4 weeks
- Injectable estradiol valerate: Usual dose: 10 to 20 mg intramuscularly every 4 weeks
- Oral tablets: Initial dose: 1 to 2 mg orally once a day. Administration should be cyclic (e.g. 3 weeks on, 1 week off)
- Topical gel: 1 pump of gel once a day, applied as a thin layer
- Topical spray: Initial dose: 1 spray once a day, to the inner surface of the forearm, starting near the elbow
- Maintenance dose: 1 to 3 sprays once a day to adjacent, non-overlapping areas on the inner surface of the forearm
- Application site should not be washed for at least 1 hour
- Transdermal film: 1 film, applied twice weekly
- Transdermal patches: 1 patch, applied weekly
- Some patches are applied twice a week: the manufacturer product information should be consulted.
- Vaginal insert: Initial dose: 10 mcg; 1 insert intravaginally daily for 2 weeks, followed by 1 insert twice weekly (e.g. Tuesday and Friday)
Comments:
- When prescribed for a woman with a uterus, consider adding a progestin to reduce endometrial cancer risk.
- Women without uteruses generally do not need a progestin, but those with a history of endometriosis may need a progestin.
- Estrogens, with or without progestins, should be prescribed at the lowest effective dose for the shortest duration consistent with treatment goals and risks.
- Attempt to discontinue or taper at 3 to 6 month intervals.
Adult Dose for Atrophic Urethritis
- Depo-estradiol (estradiol cypionate) for injection: Usual dose: 1 to 5 mg intramuscularly every 3 to 4 weeks
- Attempt to discontinue or taper at 3 to 6 month intervals
- Injectable estradiol valerate: Usual dose: 10 to 20 mg intramuscularly every 4 weeks
- Attempt to discontinue or taper at 3 to 6 month intervals
- Oral tablets: Initial dose: 1 to 2 mg orally once a day
- Administration should be cyclic (e.g. 3 weeks on, 1 week off)
- Topical gel: 1.25 grams of gel once a day, applied as a thin layer over the entire arm, inside and outside, from wrist to shoulder
- Transdermal patches: 1 patch, applied weekly
- Some patches are applied twice a week: the manufacturer product information should be consulted.
- Vaginal cream: Initial dose: 2 to 4 grams intravaginally once a day for 2 weeks, then reduce dose by half for a similar period.
- Maintenance dose: 1 gram, three times a week – use after restoration of vaginal mucosa has been achieved
- Vaginal tablets and inserts: Initial dose: 10 mcg
- 1 tablet/insert intravaginally once a day for 2 weeks, followed by 1 tablet/insert twice weekly (e.g. Tuesday and Friday)
- Vaginal ring: Initial dose: 0.05 mg/day ring, intravaginally; change every 90 days
Comments:
Estrogens, with or without progestins, should be prescribed at the lowest effective dose for the shortest duration consistent with treatment goals and risks.
Adult Dose for Atrophic Vaginitis
- Depo-estradiol (estradiol cypionate) for injection: Usual dose: 1 to 5 mg intramuscularly every 3 to 4 weeks
- Attempt to discontinue or taper at 3 to 6 month intervals
- Injectable estradiol valerate: Usual dose: 10 to 20 mg intramuscularly every 4 weeks
- Attempt to discontinue or taper at 3 to 6 month intervals
- Oral tablets: Initial dose: 1 to 2 mg orally once a day
- Administration should be cyclic (e.g. 3 weeks on, 1 week off)
- Topical gel: 1.25 grams of gel once a day, applied as a thin layer over the entire arm, inside and outside, from wrist to shoulder
- Transdermal patches: 1 patch, applied weekly
- Some patches are applied twice a week: the manufacturer product information should be consulted.
- Vaginal cream: Initial dose: 2 to 4 grams intravaginally once a day for 2 weeks, then reduce dose by half for a similar period.
- Maintenance dose: 1 gram, three times a week – use after restoration of vaginal mucosa has been achieved
- Vaginal tablets and inserts: Initial dose: 10 mcg
- 1 tablet/insert intravaginally once a day for 2 weeks, followed by 1 tablet/insert twice weekly (e.g. Tuesday and Friday)
- Vaginal ring: Initial dose: 0.05 mg/day ring, intravaginally; change every 90 days
Comments:
Estrogens, with or without progestins, should be prescribed at the lowest effective dose for the shortest duration consistent with treatment goals and risks.
Adult Dose for Hypoestrogenism
Uses: Treatment of female hypoestrogenism due to hypogonadism, castration, or primary ovarian failure.
- Depo-estradiol (estradiol cypionate) for injection: Usual dose: 1.5 to 2 mg intramuscularly every 4 weeks
- Oral tablets: Initial dose: 1 to 2 mg orally once a day
- Transdermal patches: 1 patch, applied weekly
- Some patches are applied twice a week: the manufacturer product information should be consulted.
- Injectable estradiol valerate: Usual dose: 10 to 20 mg intramuscularly every 4 weeks
Comments:
- Adjust dose as needed to control symptoms.
Adult Dose for Oophorectomy
- Oral tablets: Initial dose: 1 to 2 mg orally once a day
- Injectable estradiol valerate: Usual dose: 10 to 20 mg intramuscularly every 4 weeks
- Transdermal patches: 1 patch, applied weekly
- Some patches are applied twice a week: the manufacturer product information should be consulted.
Adult Dose for Primary Ovarian Failure
- Oral tablets: Initial dose: 1 to 2 mg orally once a day
- Injectable estradiol valerate: Usual dose: 10 to 20 mg intramuscularly every 4 weeks
- Transdermal patches: 1 patch, applied weekly
- Some patches are applied twice a week: the manufacturer product information should be consulted.
Adult Dose for Breast Cancer-Palliative
- Oral tablets: 10 mg orally 3 times a day for at least 3 months
Adult Dose for Osteoporosis
- Transdermal film: 1 film, applied twice weekly
- Transdermal patches: 1 patch, applied weekly
- Some patches are applied twice a week: the manufacturer product information should be consulted.
- Oral tablets – lowest effective dose has not been determined
Comments:
If using solely for postmenopausal osteoporosis prevention, use only for significant risk when non-estrogen medications are not appropriate.
Adult Dose for Prostate Cancer
Use: Palliation of advanced androgen-dependent prostate carcinoma
- Oral tablets: 1 to 2 mg orally 3 times a day
- Injectable estradiol valerate: Usual dose: 30 mg or more intramuscularly every 1 to 2 weeks
Comments:
- For palliation only.
- Effectiveness of therapy can be judged by phosphatase determinations and symptomatic improvement.
Renal Dose Adjustments
- Data not available
- Carefully observe patients with renal impairment.
Liver Dose Adjustments
- Contraindicated
Estradiol side effects
Estrogen may cause side effects. Tell your doctor if any of these symptoms are severe or do not go away:
- breast pain or tenderness
- upset stomach
- vomiting
- heartburn
- constipation
- diarrhea
- gas
- weight gain or loss
- leg cramps
- nervousness
- depression
- dizziness
- burning or tingling in the arms or legs
- tight muscles
- hair loss
- unwanted hair growth
- spotty darkening of the skin on the face
- difficulty wearing contact lenses
- swelling, redness, burning, itching, or irritation of the vagina
- vaginal discharge
- change in sexual desire
- cold symptoms
Some side effects can be serious. If you experience any of these symptoms or those listed in the IMPORTANT WARNING section, call your doctor immediately:
- bulging eyes
- sore throat, fever, chills, cough, and other signs of infection
- pain, swelling, or tenderness in the stomach
- loss of appetite
- weakness
- yellowing of the skin or eyes
- joint pain
- movements that are difficult to control
- rash or blisters
- hives
- itching
- swelling of the eyes, face, tongue, throat, hands, arms, feet, ankles, or lower legs
- hoarseness
- difficulty breathing or swallowing
Estrogen may increase your risk of developing cancer of the ovaries or gallbladder disease that may need to be treated with surgery. Talk to your doctor about the risks of taking estrogen.
Estrogen may cause growth to slow or stop early in children who take large doses for a long time. Estrogen may also affect the timing and speed of sexual development in children. Your child’s doctor will monitor him or her carefully during his or her treatment with estrogen. Talk to your child’s doctor about the risks of giving this medication to your child.
Estrogen may cause other side effects. Call your doctor if you have any unusual problems while taking this medication.
Symptoms of overdose may include:
- upset stomach
- vomiting
- vaginal bleeding
Genitourinary
- Very common (10% or more): Breast pain (29%)
- Common (1% to 10%): Vulvovaginal pruritus, leukorrhea, vaginal hemorrhage, vaginal discharge, vaginal discomfort, menopause symptoms, breakthrough bleeding or spotting, dysmenorrhea, breast swelling, menorrhagia, metrorrhagia, endometrial hyperplasia
- Uncommon (0.1% to 1%): Urinary problems
- Rare (less than 0.1%): Galactorrhea
- Postmarketing reports: Vaginal irritation, vaginal pain, genital pruritus, changes in bleeding pattern, pelvic pain, breast tenderness, vaginal ulceration, uterine fibroids
Gastrointestinal
- Very common (10% or more): Abdominal pain (16%),
- Common (1% to 10%): Flatulence, nausea, diarrhea
- Uncommon (0.1% to 1%): Vomiting
- Postmarketing reports: Abdominal distension
Musculoskeletal
- Very common (10% or more): Back pain (11%), arthralgia (11%)
- Common (1% to 10%): Leg cramps
Cardiovascular
- Common (1% to 10%): Varicose veins, cardiac symptoms (e.g. palpitations)
- Uncommon (0.1% to 1%): Hot flush, hypertension, venous thromboembolic disease
- Rare (less than 0.1%): Arterial hypertension
- Postmarketing reports: Deep vein thrombosis, changes in blood pressure
Nervous system
- Very common (10% or more): Headache (18%)
- Uncommon (0.1% to 1%): Vertigo, migraine
- Rare (less than 0.1%): Aggravation of epilepsy
- Postmarketing reports: Migraine aggravated, paresthesia, dizziness
Oncologic
- Uncommon (0.1% to 1%): Benign breast neoplasm, increased volume of uterine leiomyoma
- Postmarketing reports: Endometrial cancer, breast cancer
Other
- Very common (10% or more): Pain (11%)
- Common (1% to 10%): Edema
- Uncommon (0.1% to 1%): Weight increased, asthenia
- Postmarketing reports: Drug ineffectiveness, blood estrogen increase, fatigue, exacerbation of hereditary angioedema
Psychiatric
- Common (1% to 10%): Depression
- Uncommon (0.1% to 1%): Sleep disorders, nervousness, mood swings
- Rare (less than 0.1%): Change in libido
- Postmarketing reports: Vaginismus, insomnia, anxiety, irritability
Dermatologic
- Common (1% to 10%): Pruritus
- Uncommon (0.1% to 1%): Rash
- Rare (less than 0.1%): Skin discoloration, acne
- Postmarketing reports: Urticaria, erythematous or pruritic rash, alopecia, hyperhidrosis, night sweats, contact dermatitis, eczema
Ocular
- Uncommon (0.1% to 1%): Vision abnormal
- Postmarketing reports: Visual disturbances, contact lens intolerance
Hepatic
- Rare (less than 0.1%): Liver function tests abnormalities
- Postmarketing reports: Cholestatic jaundice
Metabolic
- Rare (less than 0.1%): Glucose intolerance
- Postmarketing reports: Fluid retention
Hypersensitivity
- Rare (less than 0.1%): Anaphylactic reaction (with a past history of allergic reaction)
- Postmarketing reports: Anaphylactic reactions, hypersensitivity
Immunologic
- Very common (10% or more): Upper respiratory tract infection (17%)
- Common (1% to 10%): Vulvovaginal mycotic infection, pharyngitis, rhinitis, sinusitis, moniliasis genital
- Uncommon (0.1% to 1%): Vaginitis/vaginal candidosis
Local
- Common (1% to 10%): Skin irritation (topical gel)
- Postmarketing reports: Application site reaction
- Schulster M, Bernie AM, Ramasamy R. The role of estradiol in male reproductive function. Asian Journal of Andrology. 2016;18(3):435-440. doi:10.4103/1008-682X.173932. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4854098/
- Elmlinger MW, Kuhnel W, Ranke MB: Reference ranges for serum concentrations of lutropin (LH), follitropin (FSH), estradiol (E2), prolactin, progesterone, sex hormone-binding globulin (SHBG), dehydroepiandrosterone sulfate (DHEAS), cortisol and ferritin in neonates, children and young adults. Clin Chem Lab Med 2002;40(11):1151-1160
- Savic I, Berglund H, Lindstrom P. Brain response to putative pheromones in homosexual men. Proc Natl Acad Sci U S A. 2005;102:7356–61
- Gillies GE, McArthur S. Estrogen actions in the brain and the basis for differential action in men and women: a case for sex-specific medicines. Pharmacol rev. 2010;62:155–98.
- Simpson ER, Davis SR. Another role highlighted for estrogens in the male: sexual behavior. Proc Natl Acad Sci U S A. 2000;97:14038–40. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC34093/
- McCarthy MM. The two faces of estradiol: effects on the developing brain. Neuroscientist. 2009;15:599–610 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2795061/
- Basson R. Re: andropause: a misnomer for a true clinical entity. J Urol. 2000;164:1319.
- Shabsigh A, Kang Y, Shabsign R, Gonzalez M, Liberson G, et al. Clomiphene citrate effects on testosterone/estrogen ratio in male hypogonadism. J Sex Med. 2005;2:716–21.
- Katz DJ, Nabulsi O, Tal R, Mulhall JP. Outcomes of clomiphene citrate treatment in young hypogonadal men. BJU Int. 2012;110:573–8.
- Finkelstein JS, Yu EW, Burnett-Bowie SA. Gonadal steroids and body composition, strength, and sexual function in men. N Engl J Med. 2013;369:2457. https://www.nejm.org/doi/10.1056/NEJMc1313169
- Ramasamy R, Scovell JM, Kovac JR, Lipshultz LI. Elevated serum estradiol is associated with higher libido in men on testosterone supplementation therapy. Eur Urol. 2014;65:1224–5. https://www.europeanurology.com/article/S0302-2838(14)00024-4/fulltext
- Schlegel PN. Aromatase inhibitors for male infertility. Fertil Steril. 2012;98:1359–62 https://www.fertstert.org/article/S0015-0282(12)02335-7/fulltext
- Hughes IA, Davies JD, Bunch TI, Pasterski V, Mastroyannopoulou K, et al. Androgen insensitivity syndrome. Lancet. 2012;380:1419–28.
- Johnson RE, Murad MH. Gynecomastia: pathophysiology, evaluation, and management. Mayo Clin Proc. 2009;84:1010–5
- Khera M. Patients with testosterone deficit syndrome and depression. Arch Esp Urol. 2013;66:729–36. https://www.ncbi.nlm.nih.gov/pubmed/24047633
- Kulkarni J, Gavrilidis E, Worsley R, Van Rheenen T, Hayes E. The role of estrogen in the treatment of men with schizophrenia. Int J Endocrinol Metab. 2013;11:129 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3860106/
- Fink G, Sumner B, Rosie R, Wilson H, McQueen J. Androgen actions on central serotonin neurotransmission: relevance for mood, mental state and memory. Behav Brain Res. 1999;105:53–68.
- Frokjaer VG, Erritzoe D, Juul A, Nielsen FÅ, Holst K, et al. Endogenous plasma estradiol in healthy men is positively correlated with cerebral cortical serotonin 2A receptor binding. Psychoneuroendocrinology. 2010;35:1311–20
- Pfaus JG. Reviews: pathways of sexual desire. J Sex Med. 2009;6:1506–33.
- Amin Z, Canli T, Epperson CN. Effect of estrogen-serotonin interactions on mood and cognition. Behav Cogn Neurosci Rev. 2005;4:43–58.





{kind=link}