
Heart rate recovery
Heart rate recovery is defined decrease of heart rate at 1 minute after cessation of physical exercise and is an important predictor of all‐cause mortality and death associated with coronary artery disease 1 and reflects the dynamic balance and coordinated interplay between parasympathetic nervous system reactivation and sympathetic nervous system withdrawal 2. Heart rate recovery is a noninvasive assessment of autonomic dysfunction, reflecting complex interactions between the autonomic nervous system, metabolic system, and neuroendocrine system, has emerged as an important prognostic factor associated with all‐cause mortality and has been implicated with risk of cardiovascular events 3 or urgent cardiac transplantation in ambulatory patients with chronic heart failure referred for exercise testing 4. Even after adjusting for other exercise-derived predictor variables and previously validated heart failure survival scores, post-exercise heart rate recovery remained an independent predictor of adverse clinical events 4. Empirical evidence supports the link between blunted heart rate recovery after exercise and total and cardiovascular mortality and sudden cardiac death in diverse cohorts 5. Patients with preserved heart rate recovery had a low rate of adverse outcomes regardless of their multivariate prognostic score. In a subset of patients, reduced heart rate recovery was significantly associated with increased serum markers of inflammation. Poor autonomic nervous system control of the cardiovascular system is a plausible mechanism underlying the factors associated with reduced heart rate recovery and increased risk for cardiac events and mortality 3.
Recently, a study by McCrory et al 6 described heart rate recovery within a 1‐minute interval after an orthostatic challenge, and found that speed of heart rate recovery in the immediate 20 seconds was the strongest predictor of all‐cause mortality. And van de Vegte et al 7 provided evidence that decreased heart rate recovery at 10 seconds after cessation of exercise is a superior predictor of outcome compared with heart rate recovery at later time intervals. This observation might have important implications for the future reporting and interpretation of exercise tests.
The mechanisms by which impaired heart-rate recovery confers an increased risk of death, even among patients without heart failure or myocardial perfusion defects, are not clear. Imai et al. 8 examined the physiologic characteristics of heart-rate recovery after exercise in healthy adults, athletes, and patients with chronic heart failure. They demonstrated that, in all three groups, vagal reactivation was the principal determinant of the decrease in heart rate during the first 30 seconds of recovery and that this mechanism was independent of age and the intensity of exercise. Heart-rate recovery was rapid in athletes but was blunted in patients with heart failure and was completely abolished by the administration of atropine. In Cole et al study 9, they also found a marked inverse association between heart-rate recovery and exercise capacity. Because increased vagal activity has been associated with a reduction in the risk of death 10, they hypothesized that the heart rate after exercise may be an important predictor of mortality.
Figure 1. Heart rate recovery chart showing relative risk of death within six years
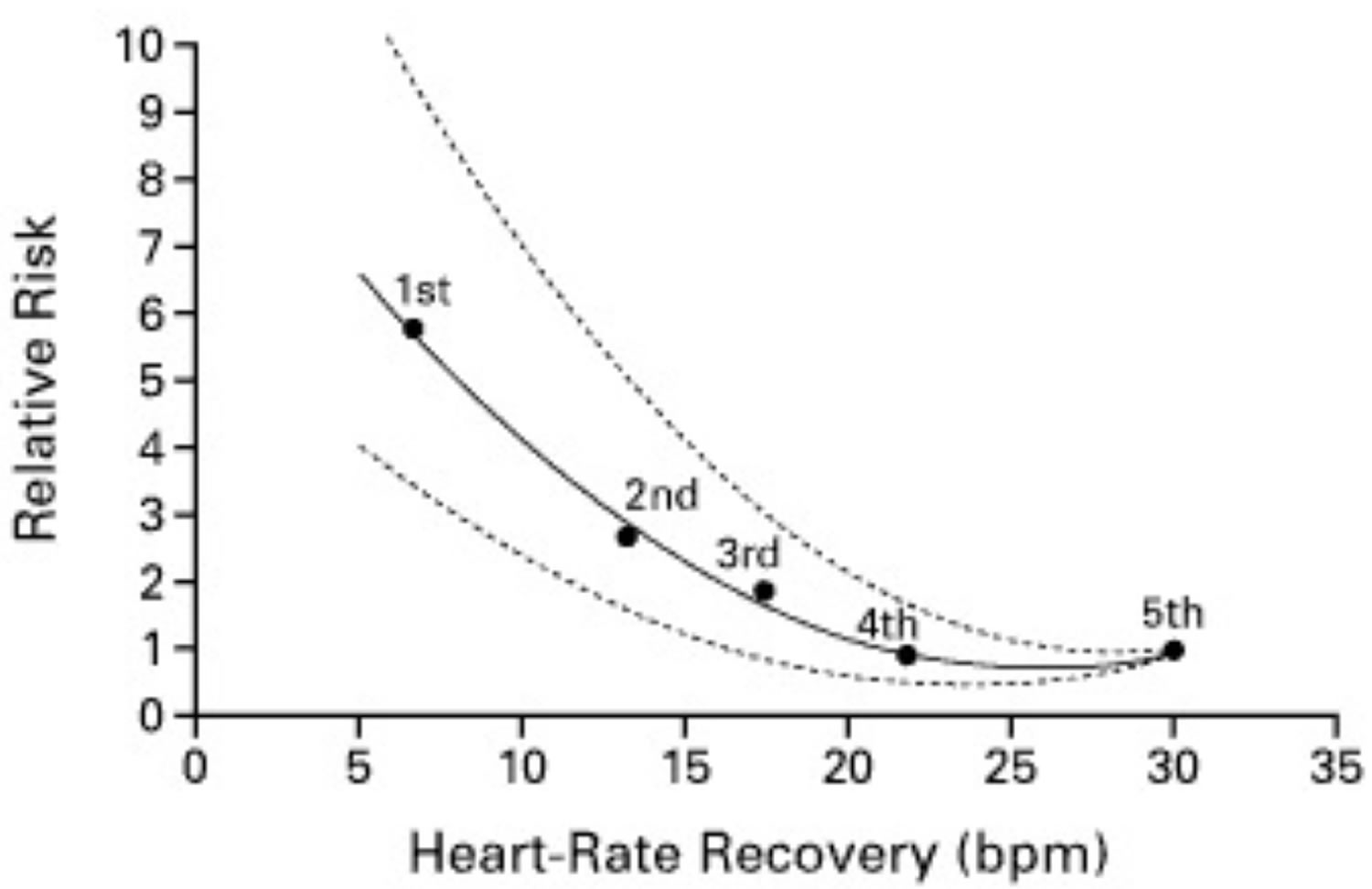
Footnote: Estimates of the Relative Risk of Death within Six Years According to Heart-Rate Recovery One Minute after Cessation of Exercise. Circles represent the relative risk of death for each of the quintiles as compared with the quintile with the greatest reduction (5th). Dashed lines represent the 95 percent confidence interval. The abbreviation bpm denotes beats per minute.
[Source 9 ]The rate of heart rate return to baseline after exercise has also been proposed to be associated with fitness and good health 11, and is usually calculated from peak exercise to minute 1 or 2 of recovery 11. Small studies 12, 13 have found that heart rate recovery can be improved with cardiac rehabilitation. Heart rate recovery improved after phase 2 cardiac rehabilitation in the overall cohort. There was a strong association of abnormal heart rate recovery at exit with all-cause mortality. Patients with abnormal heart rate recovery at baseline who normalized heart rate recovery with exercise had a mortality similar to that of individuals with baseline normal heart rate recovery 14.
In recent years, there has been a large body of epidemiological evidence that heart rate recovery might also be a potential prognostic marker for predicting health outcomes including cardiovascular disease 15, since autonomic dysfunction as signified by attenuated heart rate recovery has been suggested to be a precursor to hyperglycemia as well as an indicator of cardiovascular dysfunction 16. In addition, evidence has also indicated that heart rate recovery may assist in predicting the risk of all‐cause mortality 17. However, findings regarding its prognostic power from current available studies varied substantially among the studies. For instance, some studies observed that attenuated heart rate recovery might be associated with an increased risk of incident cardiovascular disease and all‐cause mortality 18, whereas others stated that the strength of the associations was diluted or even became no longer statistically significant after controlling for confounders 19. Furthermore, differences in the target populations (eg, healthy versus diseased adults) and variations in the recovery time points following the cessation of exercise (eg, 1‐minute versus 2‐minute heart rate recovery) might also contribute to the inconsistent findings 20.
Findings from 2017 meta‐analysis 21 provided evidence that reduced heart rate recovery is consistently associated with increased risk of cardiovascular events and all‐cause mortality in the general population. These results support the recommendation of recording heart rate recovery for risk assessment in routine clinical practice, which would enable the implementation of timely preventive interventions. Future studies are required to determine the normal reference range of heart rate recovery across different recovery time points among ethnic‐specified populations, to evaluate the cost‐effectiveness of exercise stress testing for assessing heart rate recovery with regard to the primary prevention of chronic disease morbidity and mortality, and to assess whether heart rate recovery has any therapeutic implications.
Heart rate recovery as a predictor of mortality
The association between heart rate recovery and all‐cause and coronary artery disease mortality are presented in Table 1 7 and Table 2 9. Heart rate recovery was associated with all‐cause and coronary heart disease mortality in the univariate Cox regression analyses. Heart rate recovery in the early phase after exercise cessation was a stronger predictor of mortality, compared with heart rate recovery measured at later time points. In multivariate analysis, heart rate recovery remained predictive of all‐cause mortality after correction for cardiovascular risk factors (model 2 and 3). In multivariate analyses, in which we corrected for both traditional cardiovascular risk factors as well as for risk factors for mortality in general and cardiovascular medicine use (model 4), only heart rate recovery-10, heart rate recovery-20, and heart rate recovery-30 remained predictive of all‐cause mortality. Table 1 shows a time trend in heart rates for the multivariate models, with heart rates increasing for every 10‐second increase in heart rate recovery. Heart rate recovery-10 was the most significant risk predictor and conferred the lowest heart rate. In general, P values and heart rates increased incrementally with every 10‐second increase of heart rate recovery in all multivariable models.
The predictive value of heart rate recovery on coronary artery disease mortality follows the same trend as all‐cause mortality 7. All univariate associations were significant, with lower heart rates and P values early after cessation of exercise across all models. Only heart rate recovery10 remained predictive of coronary artery disease mortality after multivariable correction. Heart rate recovery was most strongly associated with death when measured early, at 10 seconds after exercise cessation, compared with heart rate recovery measured at later time points 7.
After adjustments were made for age; sex; resting heart rate; heart-rate increase during exercise; exercise capacity; the presence or absence of hypertension, smoking, chronic lung disease, diabetes, Q waves on the electrocardiogram, a history of coronary artery disease, right bundle-branch block, and angina during treadmill testing; the use or nonuse of beta-blockers, nondihydropyridine calcium-channel blockers, lipid-lowering therapy, and vasodilator medications; and perfusion defects on thallium scintigraphy, a low value for heart-rate recovery emerged as the strongest predictor of death (adjusted relative risk, 2.0; 95 percent confidence interval, 1.5 to 2.7; P<0.001) 9. Other independent predictors included decreased exercise capacity (P<0.001), male sex (P<0.001), increased age (P<0.001), the presence of perfusion defects on thallium scintigraphy (P=0.006), and a smaller increase in heart rate during exercise (P=0.006) 9.
Table 1. Associations of heart rate recovery with all‐cause and coronary artery disease mortality
| All‐Cause Mortality | Coronary artery disease Mortality | |||
|---|---|---|---|---|
| Heart Rate (confidence interval) | P Value | Heart Rate (confidence interval) | P Value | |
| Heart rate recovery-10 | ||||
| Model 1 | 0.651 (0.591–0.718) | 5.1×10−18 | 0.398 (0.264–0.598) | 9.6×10−06 |
| Model 2 | 0.758 (0.684–0.839) | 1.1×10−07 | 0.505 (0.328–0.777) | 1.9×10−03 |
| Model 3 | 0.783 (0.707–0.867) | 2.7×10−06 | 0.540 (0.351–0.831) | 5.1×10−03 |
| Model 4 | 0.827 (0.742–0.921) | 5.8×10−04 | 0.524 (0.329–0.833) | 6.3×10−03 |
| Heart rate recovery-20 | ||||
| Model 1 | 0.643 (0.585–0.707) | 6.0×10−20 | 0.481 (0.332–0.696) | 1.1×10−04 |
| Model 2 | 0.769 (0.695–0.852) | 4.5×10−07 | 0.637 (0.428–0.949) | 2.7×10−02 |
| Model 3 | 0.802 (0.724–0.888) | 2.1×10−05 | 0.684 (0.459–1.019) | 6.2×10−02 |
| Model 4 | 0.848 (0.760–0.946) | 3.1×10−03 | 0.680 (0.440–1.051) | 8.2×10−02 |
| Heart rate recovery-30 | ||||
| Model 1 | 0.635 (0.577–0.698) | 6.0×10−21 | 0.478 (0.330–0.691) | 8.7×10−05 |
| Model 2 | 0.773 (0.697–0.857) | 1.1×10−06 | 0.646 (0.432–0.966) | 3.3×10−02 |
| Model 3 | 0.809 (0.729–0.897) | 6.0×10−05 | 0.697 (0.466–1.043) | 7.9×10−02 |
| Model 4 | 0.857 (0.766–0.959) | 7.3×10−03 | 0.691 (0.444–1.076) | 1.0×10−01 |
| Heart rate recovery-40 | ||||
| Model 1 | 0.643 (0.585–0.707) | 6.0×10−20 | 0.466 (0.323–0.674) | 4.8×10−05 |
| Model 2 | 0.799 (0.720–0.887) | 2.5×10−05 | 0.640 (0.426–0.961) | 3.1×10−02 |
| Model 3 | 0.836 (0.753–0.927) | 7.2×10−04 | 0.690 (0.460–1.037) | 7.4×10−02 |
| Model 4 | 0.894 (0.798–1.001) | 5.2×10−02 | 0.680 (0.435–1.065) | 9.2×10−02 |
| Heart rate recovery-50 | ||||
| Model 1 | 0.644 (0.586–0.708) | 8.0×10−20 | 0.475 (0.330–0.685) | 6.7×10−05 |
| Model 2 | 0.809 (0.729–0.899) | 7.3×10−05 | 0.664 (0.443–0.996) | 4.8×10−02 |
| Model 3 | 0.844 (0.761–0.937) | 1.4×10−03 | 0.714 (0.476–1.072) | 1.0×10−01 |
| Model 4 | 0.898 (0.802–1.007) | 6.5×10−02 | 0.707 (0.452–1.105) | 1.3×10−01 |
Footnote: Hazard ratios for all‐cause and coronary artery disease (CAD) mortality were estimated using a Cox proportional hazard model. Hazard ratio (HR) and confidence interval (CI) are shown per SD (standard deviation) increase in heart rate recovery. Four regression models were used to study the association between heart rate recovery and mortality.
- Model 1: univariate.
- Model 2: age, sex, body mass index (BMI), and exercise capacity.
- Model 3: age, sex, BMI, exercise capacity, exercise duration, systolic blood pressure (SBP), diabetes mellitus, hyperlipidemia, smoking behavior, current physical activity behavior, and a family history of cardiovascular disease (CVD).
- Model 4: age; sex; BMI; exercise capacity; exercise duration; SBP; hyperlipidemia; use of diuretics, beta‐blockers, calcium channel blockers, or angiotensin‐converting enzyme inhibitors; ever received a doctor diagnosis of cancer, lung disease, or diabetes mellitus; smoking behavior; physical activity behavior; a family history of cardiovascular disease; Townsend deprivation index; and resting heart rate.
Table 2. Associations between a low value for heart rate recovery and mortality in prespecified subgroups (see Table 3 below).

Characteristics of the patients at base line and during exercise
There were 2428 patients who met all inclusion criteria. The median value for heart-rate recovery was 17 beats per minute, with a range from the 25th to the 75th percentile of 12 to 23 beats per minute. A cutoff value of 12 beats per minute was found to maximize the log-rank test statistic. An abnormal value for heart-rate recovery was found in 639 patients (26 percent) 9.
The base-line characteristics of the patients according to whether their heart-rate recovery was normal or abnormal are summarized in Table 3. As compared with the patients with a normal value for heart-rate recovery, those with an abnormal value (≤12 beats per minute) were older, had higher resting heart rates, were more likely to have hypertension or diabetes, were more likely to smoke, and were more likely to have Q waves on the electrocardiogram or a history of coronary artery disease. They were also more likely to take nondihydropyridine calcium-channel blockers or vasodilators. There were no marked differences between the groups in the use of beta-blockers 9.
During exercise, the patients with an abnormal value for heart-rate recovery, as compared with those with a normal value, had lower increases in heart rate from base line (an increase of 61±21 beats per minute vs. an increase of 81±20 beats per minute, P<0.001) and were more likely to have an impaired chronotropic response during exercise (45 percent vs. 23 percent of patients, P<0.001). They were also more likely to have perfusion defects on thallium scintigraphy (23 percent vs. 19 percent, P=0.01). There were no differences between the groups in the percentage of patients with abnormal ST-segment response (19 percent vs. 21 percent, P=0.2) or angina during treadmill testing (15 percent vs. 14 percent, P=0.6).
During six years of follow-up, there were 213 deaths from all causes (9 percent). An abnormal value for heart-rate recovery was strongly predictive of death (mortality at six years, 19 percent vs. 5 percent; relative risk, 4.0; 95 percent confidence interval, 3.0 to 5.2; P<0.001). Of the 213 patients who died, 120 (56 percent) had an abnormally low value for heart-rate recovery.
As a predictor of death, an abnormally low value for heart-rate recovery had a sensitivity of 56 percent, a specificity of 77 percent, a positive predictive value of 19 percent, and a negative predictive value of 95 percent. When the value for the 10th percentile (a decrease of eight beats per minute) was used as a cutoff, the sensitivity was 33 percent, the specificity 90 percent, the positive predictive value 24 percent, and the negative predictive value 90 percent; the relative risk was 4.1 (95 percent confidence interval, 3.0 to 5.4; P<0.001).
Analyses stratified according to age, sex, history of coronary disease, the chronotropic response during exercise, the presence or absence of perfusion defects on thallium scintigraphy, and the use or nonuse of medications are presented in Table 2. A low value for heart-rate recovery was predictive of death in all subgroups, although the association was weaker among the patients with an impaired chronotropic response during exercise and those taking vasodilators or nondihydropyridine calcium-channel blockers.
A low value for heart-rate recovery was predictive of death when considered as a continuous variable, especially after logarithmic transformation; a decrease in exercise capacity, the presence of perfusion defects on thallium scintigraphy, and an impaired chronotropic response during exercise were also predictive of death (Table 3). Figure 1 shows the relative risk of death according to the quintile of heart-rate recovery; once this value dropped below 10 to 15 beats per minute there was a marked increase in the risk of death. Values above 15 to 20 beats per minute, however, were not associated with further improvements in prognosis.
Table 3. Base-line characteristics of the patients subgroups in the heart rate recovery study.
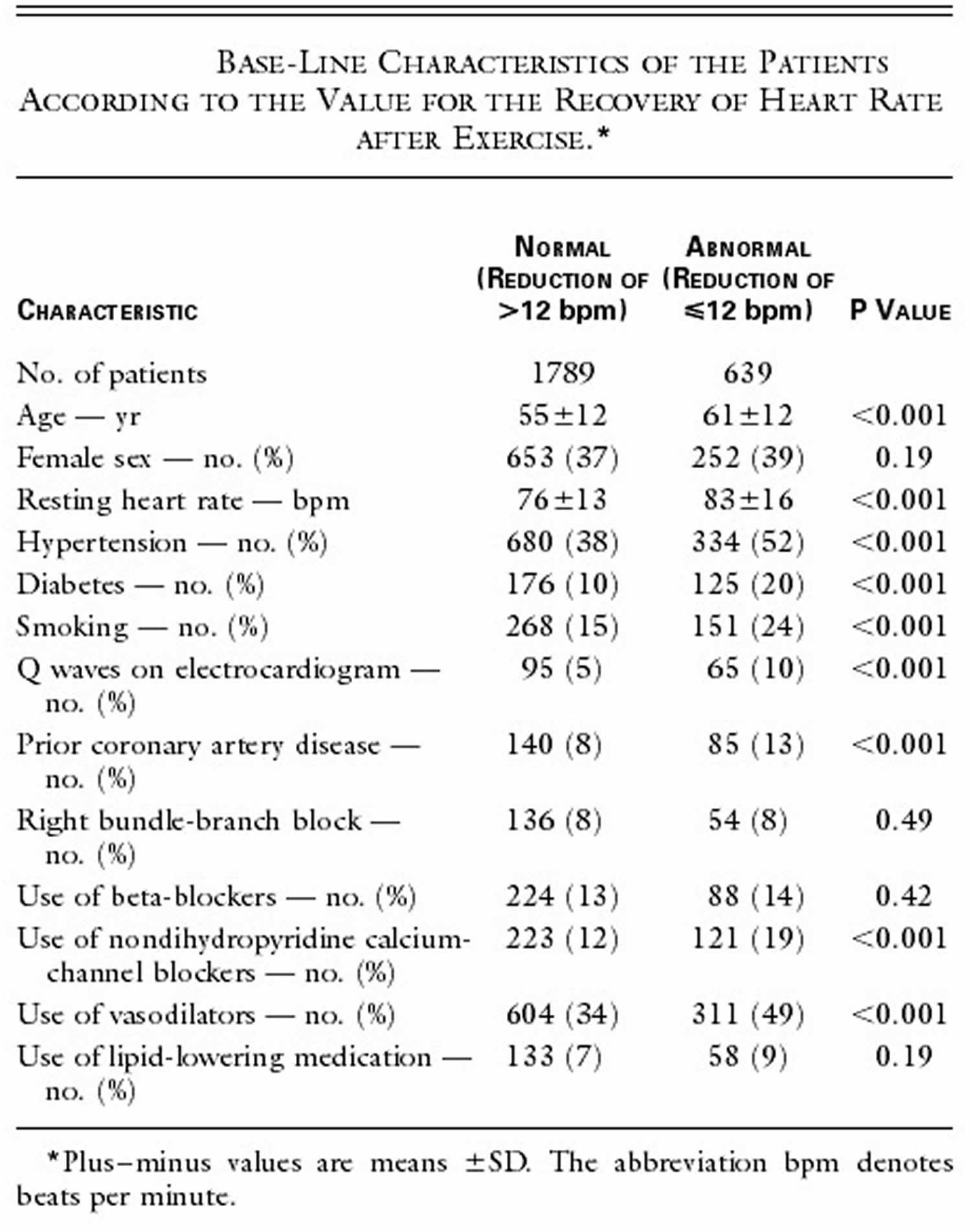
Table 4. Heart rate recovery risk of death according to univariable analysis.

- Clinician’s Guide to cardiopulmonary exercise testing in adults: a scientific statement from the American Heart Association. Balady GJ, Arena R, Sietsema K, Myers J, Coke L, Fletcher GF, Forman D, Franklin B, Guazzi M, Gulati M, Keteyian SJ, Lavie CJ, Macko R, Mancini D, Milani RV, American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee of the Council on Clinical Cardiology., Council on Epidemiology and Prevention., Council on Peripheral Vascular Disease., Interdisciplinary Council on Quality of Care and Outcomes Research. Circulation. 2010 Jul 13; 122(2):191-225.
- Assessment of autonomic function in cardiovascular disease: physiological basis and prognostic implications. Lahiri MK, Kannankeril PJ, Goldberger JJ. J Am Coll Cardiol. 2008 May 6; 51(18):1725-33.
- Beckie TM, Beckstead JW, Kip KE, Fletcher G. Improvements in heart rate recovery among women after cardiac rehabilitation completion. J Cardiovasc Nurs. 2014;29(1):38–47. doi:10.1097/JCN.0b013e31827324e2 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4108986
- Tang YD, Dewland TA, Wencker D, Katz SD. Post-exercise heart rate recovery independently predicts mortality risk in patients with chronic heart failure. J Card Fail. 2009;15(10):850–855. doi:10.1016/j.cardfail.2009.06.437 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2786814
- Johnson NP, Goldberger JJ. Prognostic value of late heart rate recovery after treadmill exercise. Am J Cardiol. 2012;110(1):45–49.
- McCrory C, Berkman LF, Nolan H, O’Leary N, Foley M, Kenny RA. Speed of heart rate recovery in response to orthostatic challenge. Circ Res. 2016; 119:666–6
- Heart Rate Recovery 10 Seconds After Cessation of Exercise Predicts Death. Journal of the American Heart Association. ;7:e008341 https://www.ahajournals.org/doi/full/10.1161/JAHA.117.008341
- Imai K, Sato H, Hori M, et al. Vagally mediated heart rate recovery after exercise is accelerated in athletes but blunted in patients with chronic heart failure. J Am Coll Cardiol 1994;24:1529-1535
- Heart-Rate Recovery Immediately after Exercise as a Predictor of Mortality. N Engl J Med 1999; 341:1351-1357 DOI: 10.1056/NEJM199910283411804 https://www.nejm.org/doi/full/10.1056/NEJM199910283411804
- Schwartz PJ, La Rovere MT, Vanoli E. Autonomic nervous system and sudden cardiac death: experimental basis and clinical observations for post-myocardial infarction risk stratification. Circulation 1992;85:Suppl I:I-77
- Chapter 13 – Exercise and the autonomic nervous system. Handbook of Clinical Neurology Volume 117, 2013, Pages 147-160 https://doi.org/10.1016/B978-0-444-53491-0.00013-4
- The effect of cardiac rehabilitation on recovery of heart rate over one minute after exercise in patients with coronary artery bypass graft surgery. Tsai SW, Lin YW, Wu SK. Clin Rehabil. 2005 Dec; 19(8):843-9.
- Exercise and heart rate recovery. MacMillan JS, Davis LL, Durham CF, Matteson ES. Heart Lung. 2006 Nov-Dec; 35(6):383-90.
- Impact of Exercise on Heart Rate Recovery. Circulation. 2011;124:1520–1526 https://www.ahajournals.org/doi/pdf/10.1161/CIRCULATIONAHA.110.005009
- Ho JS, Fitzgerald SJ, Barlow CE, Cannaday JJ, Kohl HW III, Haskell WL, Cooper KH. Risk of mortality increases with increasing number of abnormal non‐ST parameters recorded during exercise testing. Eur J Cardiovasc Prev Rehabil. 2010;17:462–468.
- Buchheit M, Papelier Y, Laursen PB, Ahmaidi S. Noninvasive assessment of cardiac parasympathetic function: postexercise heart rate recovery or heart rate variability? Am J Physiol Heart Circ Physiol. 2007;293:H8–H10.
- Carnethon MR, Sternfeld B, Liu K, Jacobs DR Jr, Schreiner PJ, Williams OD, Lewis CE, Sidney S. Correlates of heart rate recovery over 20 years in a healthy population sample. Med Sci Sports Exerc. 2012;44:273–279.
- Savonen KP, Kiviniemi V, Laaksonen DE, Lakka TA, Laukkanen JA, Tuomainen TP, Rauramaa R. Two‐minute heart rate recovery after cycle ergometer exercise and all‐cause mortality in middle‐aged men. J Intern Med. 2011;270:589–596.
- Mora S, Redberg RF, Cui Y, Whiteman MK, Flaws JA, Sharrett AR, Blumenthal RS. Ability of exercise testing to predict cardiovascular and all‐cause death in asymptomatic women: a 20‐year follow‐up of the lipid research clinics prevalence study. JAMA. 2003;290:1600–1607.
- Peçanha T, Silva‐Junior ND, Forjaz CL. Heart rate recovery: autonomic determinants, methods of assessment and association with mortality and cardiovascular diseases. Clin Physiol Funct Imaging. 2014;34:327–339.
- Qiu S, Cai X, Sun Z, et al. Heart Rate Recovery and Risk of Cardiovascular Events and All-Cause Mortality: A Meta-Analysis of Prospective Cohort Studies. J Am Heart Assoc. 2017;6(5):e005505. Published 2017 May 9. doi:10.1161/JAHA.117.005505 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5524096





{kind=link}