Hepatectomy
Hepatectomy consists on the surgical resection of the liver. While the term hepatectomy is often employed for the removal of the liver from a liver transplant recipient, hepatectomy could also mean partial hepatectomy or liver resection, which is the surgical removal of part of the liver. Partial hepatectomy or liver resection operation is for some types of liver cancer and for certain cases of metastatic colorectal cancer. Up to half of your liver can be removed as long as the rest is healthy. During a partial hepatectomy or liver resection, a wedge of tissue, an entire lobe, or a larger part of the liver that contains cancer is removed, along with some healthy liver tissue on either side. If the right side of your liver is removed, your gallbladder, which is attached to the liver, is also taken out. The remaining liver tissue takes over the functions of the liver and may regrow. Right hepatectomy for hepatocellular carcinoma is the most common major operation in liver surgery.
In a liver transplant, the entire liver is removed and replaced with a healthy donated liver. A liver transplant may be done when the disease is in the liver only and a donated liver can be found. If the patient has to wait for a donated liver, other treatment is given as needed.
Partial hepatectomy or liver resection is used to treat colorectal cancer that has spread to the liver (liver metastasis). Removing the cancer from the liver helps to keep it from spreading farther. Sometimes all the cancer in the liver can be removed with this surgery. But even when this surgery cannot remove all the cancer from the liver, it usually helps people live longer.
Partial hepatectomy may not be a good choice if you have areas of metastatic colorectal cancer in both lobes of your liver or if you have metastatic disease in other parts of your body.
Chemotherapy and radiation therapy may be needed after a liver resection. Sometimes chemotherapy may be given before surgery to shrink a tumour in the liver. If it becomes small enough, it can be removed with surgery.
Partial hepatectomy or liver resection requires general anesthesia. The operation can take 2 to 5 hours. A blood transfusion is not usually needed for this operation. You may stay in the hospital for 5 to 7 days or as long as 2 weeks after surgery. Follow-up care is needed because of the possibility that colorectal cancer will return, even if the surgery was successful. Treatment following liver resection may include chemotherapy or radiation treatments.
Partial hepatectomy or liver resection increases a person’s chances of living longer. About 25% to 40% of people (25 to 40 out of 100 people) who have this surgery are still alive after 5 years (5-year survival rate) 1.
Hepatectomy indications
Most hepatectomies are performed for the treatment of hepatic neoplasms, both benign or malignant. Benign neoplasms include hepatocellular adenoma, hepatic hemangioma and focal nodular hyperplasia.
The most common malignant neoplasms (cancers) of the liver are liver metastases; those arising from colorectal cancer are among the most common, and the most amenable to surgical resection. The most common primary malignant tumor of the liver is the hepatocellular carcinoma.
Hepatectomy may also be the procedure of choice to treat intrahepatic gallstones or parasitic cysts of the liver.
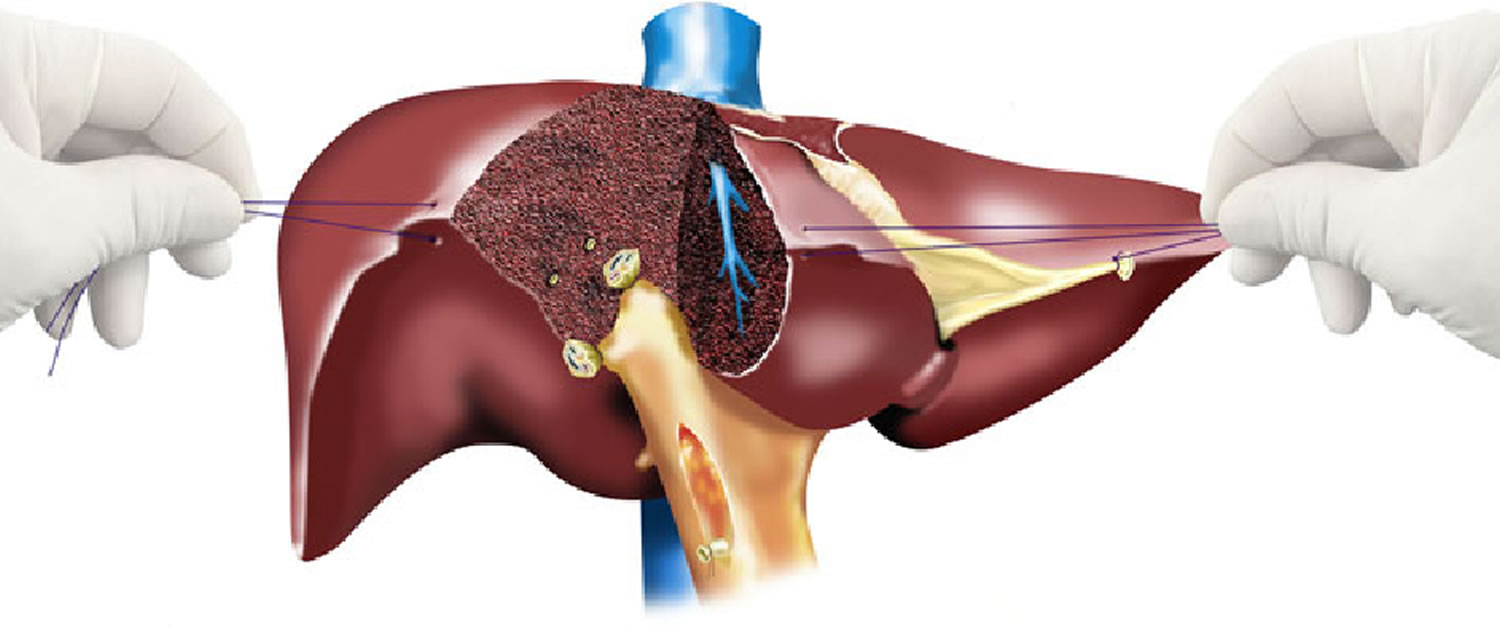
Hepatectomy technique
In the 1990s, the use of laparoscopic hepatectomy for benign and malignant tumors was independently reported by Katkhouda 2, Reich, and others 3. Access is accomplished by laparotomy, typically by a bilateral subcostal (“chevron”) incision, possibly with midline extension (Calne or “Mercedes-Benz” incision).
Hepatectomies may be anatomic, i.e. the lines of resection match the limits of one or more functional segments of the liver as defined by the Couinaud classification 4; or they may be non-anatomic, irregular or “wedge” hepatectomies.
Anatomic resections are generally preferred because of the smaller risk of bleeding and biliary fistula; however, non-anatomic resections can be performed safely as well in selected cases.
Hepatectomy complications
Possible complications after a hepatectomy include:
- Infection.
- Bleeding.
- Scar tissue from the surgery.
Bleeding is the most feared technical complication and may be grounds for urgent reoperation. Biliary fistula is also a possible complication, albeit one more amenable to nonsurgical management. Pulmonary complications such as atelectasis and pleural effusion are commonplace, and dangerous in patients with underlying lung disease. Infection is relatively rare.
Liver failure poses a significant hazard to patients with underlying hepatic disease; this is a major deterrent in the surgical resection of hepatocellular carcinoma in patients with cirrhosis. It is also a problem, to a lesser degree, in patients with previous hepatectomies (e.g. repeat resections for reincident colorectal cancer metastases).
References- Colon Cancer Treatment (PDQ®)–Health Professional Version. https://www.cancer.gov/types/colorectal/hp/colon-treatment-pdq
- Katkhouda N, Fabiani P, Benizri E, Mouiel J. Laser resection of a liver hydatid cyst under videolaparoscopy. Br J Surg. 1992;79:560–561.
- Reich H, McGlynn F, DeCaprio J, Budin R. Laparoscopic excision of benign liver lesions. Obstet Gynecol. 1991;78:956–958.
- Couinaud C. Surgical anatomy of the liver revisited. Paris: Self‐printed; 1989.





{kind=link}