What is a horseshoe kidney
Horseshoe kidneys are the most common fusion defect of the kidneys, but this still amounts to only about 0.25% of the population 1. Horseshoe kidney occurs in about 1 in 500 children. It occurs during fetal development as the kidneys move into their normal position. With horseshoe kidney, as the kidneys of the fetus rise from the pelvic area, they become attached (“fuse”) together at the lower end or base. By fusing, they form into a U shape, like a horseshoe. This is thought to happen more often in males than in females (M:F 2:1) 1. Horseshoe kidneys were initially described during autopsies by da Carpi performed in 1522, they are characterized by abnormalities in the position, rotation, and vascular supply of the kidney 2. Horseshoe kidneys are identified as having functioning renal masses present on both sides of the vertebral column fused together with ureters that remain uncrossed from the renal hilum to the urinary bladder 3. The isthmus connecting the two renal masses may be positioned in the midline or laterally resulting in asymmetric horseshoe kidney, 70% of which are left dominant, and consists of renal parenchyma in about 80% of cases with the remainder being composed of a fibrous band. In more than 90% of cases, fusion occurs at the lower pole, although fusion may occur at the upper pole in a minority of cases 4.
Most people are born with 2 kidneys. But sometimes the kidneys form fused together. A horseshoe kidney consists of two normal functioning kidneys attached by a band of tissue called the isthmus. The kidneys are normally located in the retroperitoneum between the transverse processes of T12 and L3 with the left kidney slightly more superior than the right 5. The upper poles are normally positioned slightly medially and posteriorly relative to the lower poles. Horseshoe kidneys are different in three main ways: location, orientation, and vasculature 2. The horseshoe kidney’s ascent is often quoted to be held back by the inferior mesenteric artery at L3 however, the horseshoe kidney can also be found lower in the abdomen and pelvis. During weeks six to eight of development, the renal ascent is coupled with a 90-degree medial rotation. Due to the isthmus, however, horseshoe kidneys experience malrotation, and consequently, the ureters need to either pass over the isthmus or down the anterior surface of the kidneys which can cause urinary drainage problems and stasis 6. Horseshoe kidneys also show a greater variation in the origin and number of renal arteries and veins 7. These are largely dependent on where during development ascent has terminated. In one study of 90 horseshoe kidneys, 387 arteries were identified 7. Despite this, the normal intra-renal vascular segmental pattern remains, and the ligation or division of any of these arteries results in ischemic segmental renal necrosis due to their poor collateral arterial supply 8. The incidence of renal vein anomalies in horseshoe kidneys is also high (23%) 7.
Horseshoe kidney render the kidneys susceptible to trauma and are an independent risk factor for the development of renal calculi and transitional cell carcinoma of the renal pelvis.
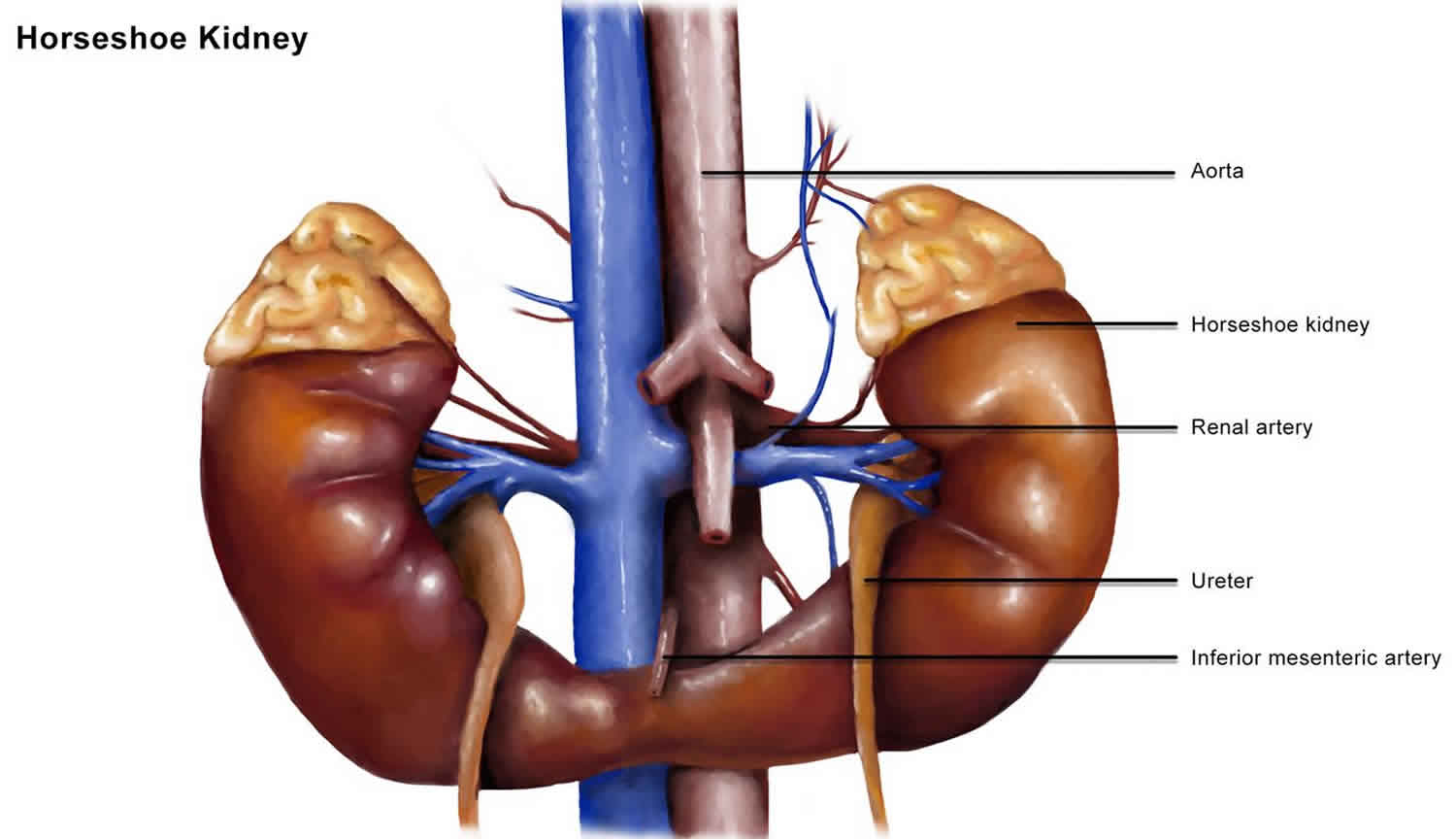
Figure 1. Horseshoe kidney

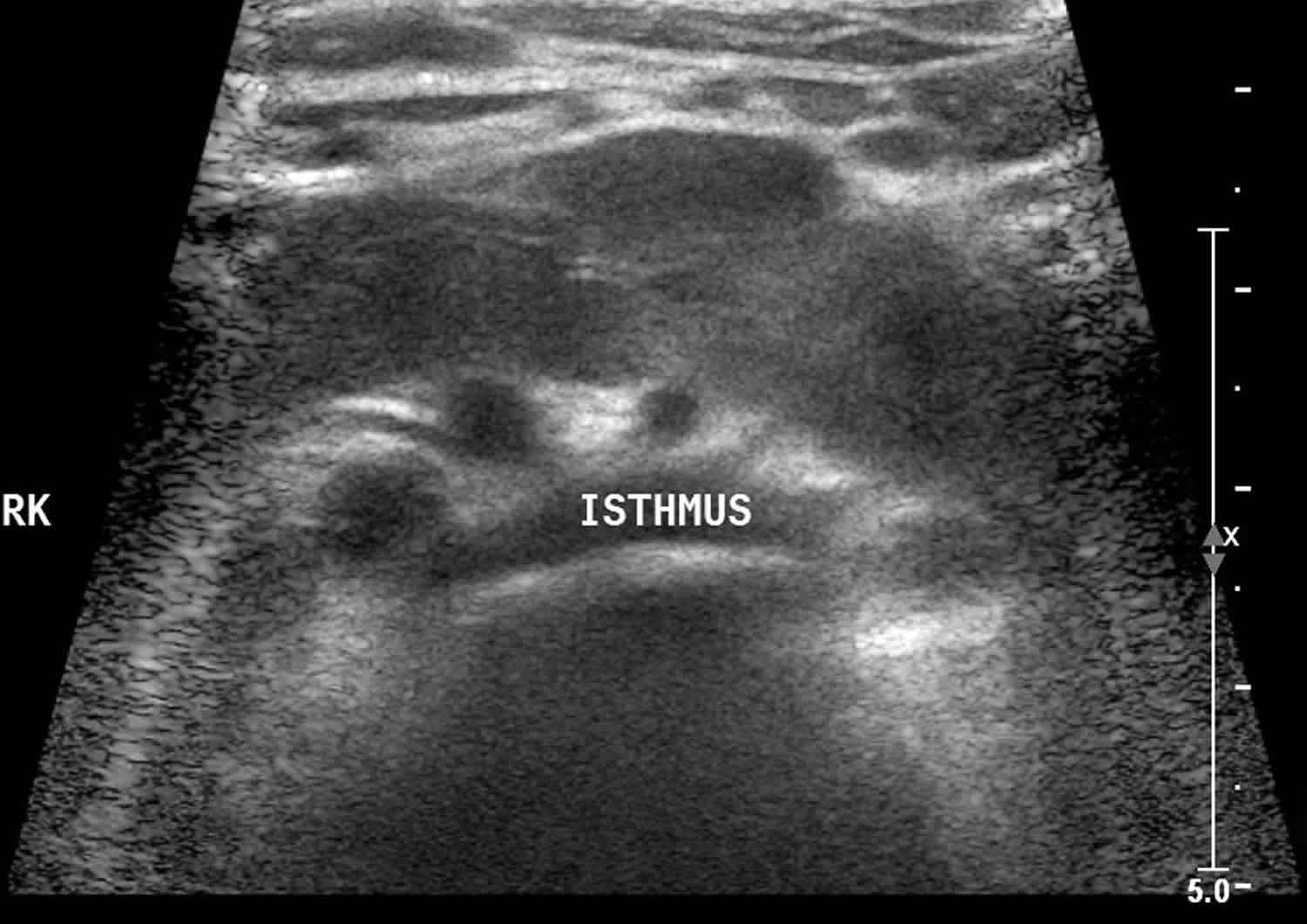
Figure 2. Horseshoe kidney ultrasound
What happens under normal conditions?
The urinary tract is the body’s drainage system. It includes two kidneys, two ureters, a bladder, and a urethra.
Healthy kidneys work day and night to clean our blood. These 2 bean-shaped organs are found near the middle of the back, just below the ribs. One kidney sits on each side of the spine.
Our kidneys are our body’s main filter. They clean about 150 quarts of blood daily. Every day, they form about 1-2 quarts of urine by pulling extra water and waste from the blood. Urine normally travels from the kidneys down to the bladder and out through the urethra.
As a filter, the kidney controls many things to keep us healthy:
- Fluid balance
- Electrolyte levels (e.g., sodium, potassium, calcium, magnesium, acid)
- Waste removal in the form of urine
- The regulation of blood pressure and red blood cell counts
As a child develops in the mother’s uterus, the kidneys form first in the child’s lower belly. They slowly move up to their final position on both sides of the spine as they develop.
Can a horseshoe kidney be separated?
Yes. Symphysiotomy or division of the fused isthmus, was previously recommended when doing a pyeloplasty in patients with a horseshoe kidney, but this has changed due to the increased risk of infection, fistulas, leakages, and bleeding 9. It has also been noted that the kidneys return to their original location after such surgery, so symphysiotomy is no longer recommended.
Horseshoe kidney causes
Despite cases of familial clustering, no clear genetic cause has been described for horseshoe kidneys, although several etiological factors may contribute to their development 10. These include abnormal migration of nephrogenic cells across the primitive streak, alterations in the intrauterine environment with teratogenic drugs such as thalidomide, alcohol consumption and glycemic control causing an increase in incidence and structural factors such as flexion/rotation of the caudal spine and narrowed arterial forks during migration 11. Traditionally textbooks quote fusion as occurring between weeks four and six of development, although there is some evidence for later fusion, particularly when the isthmus is fibrous rather than renal parenchyma.
The incidence for horseshoe kidney is higher in those who present to urology clinics (1 in 304), and with some chromosomal disorders. These include Edward syndrome at approximately 67%, Turner syndrome at 14% to 20%, and Down syndrome at about 1% 12.
Horseshoe kidney symptoms
Even though a horseshoe kidney is congenital (present at birth), one-third of children will have no symptoms and the condition often goes undetected. Up to 7 out of 10 children and adults with horseshoe kidney will have symptoms. In patients who do have symptoms, horseshoe kidney is often diagnosed as the result of an urinary tract infection (UTI), an obstruction or a kidney stone. These can include 13:
- Pain in the belly
- Nausea
- Kidney stones
- Urinary Tract Infections
Horseshoe kidneys have symptoms much more often than do other types of abnormal kidneys.
Kidney cancer is rare in children, but cancer tumors are somewhat more likely to occur in horseshoe kidneys than in normal kidneys. Some symptoms of a kidney tumor are:
- Blood in the urine (hematuria)
- Mass in the belly
- Flank pain
Horseshoe kidney complications
An isolated finding of a horseshoe kidney is generally considered benign 3. About a third of all patients with horseshoe kidneys remain completely asymptomatic and are often found incidentally during imaging. The intrinsic anatomical defects present within horseshoe kidneys do however predispose individuals to a number of urological sequelae due to the associated ureteric obstruction and impaired urinary drainage 14. Ureteropelvic junction obstruction (UPJ) is the most common abnormality associated with horseshoe kidneys, individuals are also predisposed to hydronephrosis, infection, vesicoureteral reflux 6. One study showed that over half of the individuals who are symptomatic had either ureteropelvic junction obstruction or vesicoureteral reflux 15. A recent meta-analysis suggested that 36% of patients with horseshoe kidney will develop kidney stones (nephrolithiasis) at some stage 16. Due to their ectopic position, horseshoe kidneys are also particularly susceptible to blunt abdominal trauma and can be compressed or fractured against the lumbar vertebrae 17.
Horseshoe kidneys also have an increase in frequency for some common renal cancers including transitional cell tumors (three to four times more common), Wilms tumor (twice as frequently), and an extremely large increase in very rare tumors such as carcinoid (62 to 82 times) 18.
Horseshoe kidney diagnosis
Often, health care providers find horseshoe kidneys while treating other conditions. A health care provider may also find them when looking for the cause of symptoms mentioned earlier. These imaging tests could help your health care provider find a horseshoe kidney:
- Ultrasound
- Intravenous pyelogram (IVP)
- Voiding Cystourethrogram (VCUG)
- Radionuclide Scan
- Magnetic Resonance Imaging (MRI)
Horseshoe kidneys can be identified using most abdominal imaging modalities. The diagnosis of a horseshoe kidney is most commonly made using either ultrasound or intravenous urography 14. CT and MRI are the best for demonstrating the anatomy and can detect accessory vasculature and surrounding structures 19. It is also possible to identify horseshoe kidneys on plain radiography through visualization of the perinephric fat in association with an altered renal axis. The lower poles are positioned more medial than normal and because the kidneys sit lower in the abdomen than expected 14. Nuclear medicine radionuclide renal scans can be helpful in differentiating true obstruction from passively dilated systems.
Your health care provider may also order blood tests to see how well the kidney(s) are working.
Horseshoe kidney treatment
Horseshoe kidney treatment may not be needed if there are no symptoms. There isn’t a cure for horseshoe kidney, but the symptoms can be treated if they cause problems (“supportive treatment”).
Blockage of urine flow (“obstruction”) and urine flowing backwards from the bladder (“vesicoureteral reflux”) are very common in patients with horseshoe kidney. These can both be fixed with surgery.
Pre-procedural imaging such as CT is essential during the workup for any surgery required. This is due not only to the highly variable nature of the blood supply but also the association of horseshoe kidneys with having a segment of colon posteriorly and the corresponding increases in risk of incidental bowel injury 20.
A horseshoe kidney is most often set lower and much closer to the front of the body than a normal kidney. It’s also more likely to be hurt when there’s trauma to the abdomen than is a normal kidney. Wearing a medical alert bracelet will let emergency care providers know to be aware of the chance of kidney damage. Children with a horseshoe kidney should avoid contact sports.
Horseshoe kidneys can become blocked just as any normal kidney can. Surgery to remove blockages or kidney stones in the ureter is usually successful.
Shockwave lithotripsy for nephrolithiasis is less effective in horseshoe kidneys due to problems localizing the energy for pelvic stones and poor stone fragment clearance due to impaired renal drainage 21. Larger renal stones, those greater than 2.5 cm, or those not allowing ureteroscopic approaches, can be removed via minimally invasive percutaneous surgery 22.
If the only complaint from the horseshoe kidney is pain, surgery will often not ease the pain.
References- Schiappacasse G, Aguirre J, Soffia P, Silva CS, Zilleruelo N. CT findings of the main pathological conditions associated with horseshoe kidneys. Br J Radiol. 2015 Jan;88(1045):20140456
- Natsis K, Piagkou M, Skotsimara A, Protogerou V, Tsitouridis I, Skandalakis P. Horseshoe kidney: a review of anatomy and pathology. Surg Radiol Anat. 2014 Aug;36(6):517-26.
- Cook WA, Stephens FD. Fused kidneys: morphologic study and theory of embryogenesis. Birth Defects Orig. Artic. Ser. 1977;13(5):327-40.
- Glodny B, Petersen J, Hofmann KJ, Schenk C, Herwig R, Trieb T, Koppelstaetter C, Steingruber I, Rehder P. Kidney fusion anomalies revisited: clinical and radiological analysis of 209 cases of crossed fused ectopia and horseshoe kidney. BJU Int. 2009 Jan;103(2):224-35.
- Kirkpatrick JJ, Leslie SW. Horseshoe Kidney. [Updated 2019 Jun 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK431105
- Lallas CD, Pak RW, Pagnani C, Hubosky SG, Yanke BV, Keeley FX, Bagley DH. The minimally invasive management of ureteropelvic junction obstruction in horseshoe kidneys. World J Urol. 2011 Feb;29(1):91-5
- Glodny B, Petersen J, Hofmann KJ, Schenk C, Herwig R, Trieb T, Koppelstaetter C, Steingruber I, Rehder P. Kidney fusion anomalies revisited: clinical and radiological analysis of 209 cases of crossed fused ectopia and horseshoe kidney. BJU Int. 2009 Jan;103(2):224-35
- O’Hara PJ, Hakaim AG, Hertzer NR, Krajewski LP, Cox GS, Beven EG. Surgical management of aortic aneurysm and coexistent horseshoe kidney: review of a 31-year experience. J. Vasc. Surg. 1993 May;17(5):940-7.
- Boatman DL, Kölln CP, Flocks RH. Congenital anomalies associated with horseshoe kidney. J. Urol. 1972 Feb;107(2):205-7
- David RS. Horseshoe kidney: a report of one family. Br Med J. 1974 Dec 07;4(5944):571-2
- Glodny B, Petersen J, Hofmann KJ, Schenk C, Herwig R, Trieb T, Koppelstaetter C, Steingruber I, Rehder P. Kidney fusion anomalies revisited: clinical and radiological analysis of 209 cases of crossed fused ectopia and horseshoe kidney. BJU Int. 2009 Jan;103(2):224-35
- Cereda A, Carey JC. The trisomy 18 syndrome. Orphanet J Rare Dis. 2012 Oct 23;7:81
- Cascio S, Sweeney B, Granata C, Piaggio G, Jasonni V, Puri P. Vesicoureteral reflux and ureteropelvic junction obstruction in children with horseshoe kidney: treatment and outcome. J. Urol. 2002 Jun;167(6):2566-8
- O’Brien J, Buckley O, Doody O, Ward E, Persaud T, Torreggiani W. Imaging of horseshoe kidneys and their complications. J Med Imaging Radiat Oncol. 2008 Jun;52(3):216-26.
- Cascio S, Sweeney B, Granata C, Piaggio G, Jasonni V, Puri P. Vesicoureteral reflux and ureteropelvic junction obstruction in children with horseshoe kidney: treatment and outcome. J. Urol. 2002 Jun;167(6):2566-8.
- Pawar AS, Thongprayoon C, Cheungpasitporn W, Sakhuja A, Mao MA, Erickson SB. Incidence and characteristics of kidney stones in patients with horseshoe kidney: A systematic review and meta-analysis. Urol Ann. 2018 Jan-Mar;10(1):87-93
- Chopra P, St-Vil D, Yazbeck S. Blunt renal trauma-blessing in disguise? J. Pediatr. Surg. 2002 May;37(5):779-82
- Lallas CD, Pak RW, Pagnani C, Hubosky SG, Yanke BV, Keeley FX, Bagley DH. The minimally invasive management of ureteropelvic junction obstruction in horseshoe kidneys. World J Urol. 2011 Feb;29(1):91-5.
- Lee CT, Hilton S, Russo P. Renal mass within a horseshoe kidney: preoperative evaluation with three-dimensional helical computed tomography. Urology. 2001 Jan;57(1):168.
- Skoog SJ, Reed MD, Gaudier FA, Dunn NP. The posterolateral and the retrorenal colon: implication in percutaneous stone extraction. J. Urol. 1985 Jul;134(1):110-2
- Stein RJ, Desai MM. Management of urolithiasis in the congenitally abnormal kidney (horseshoe and ectopic). Curr Opin Urol. 2007 Mar;17(2):125-31
- Rais-Bahrami S, Friedlander JI, Duty BD, Okeke Z, Smith AD. Difficulties with access in percutaneous renal surgery. Ther Adv Urol. 2011 Apr;3(2):59-68.





{kind=link}