
What are razor bumps
Razor bumps is also known as pseudofolliculitis barbae or “shaving rash.” Razor bumps is a common, chronic foreign-body inflammatory reaction surrounding ingrown facial hairs, which results from shaving. Razor bumps can also occur on any body site where hair is shaved or plucked, including armpit, bikini area, pubic area, and legs. Razor bumps is associated with improper shaving practices. Razor bumps can also occur in skin folds and scars. Razor bumps occurs mainly in people with curly hair, because the curl of the hair means that the sharp pointed end of a recently shaved hair comes out from the skin and re-enters the skin close by causing a foreign body inflammatory reaction (causing a small, tender bump). Razor bumps are not infected (if the bump becomes infected, it is called folliculitis barbae), but they are irritated. A “close shave” increases the risk of getting razor bumps, so if you are prone to this condition you should minimize frequency of shaving and avoid close shaving. Allowing razor bumps to go untreated may result in scarring, which is difficult to treat. Treatment of razor bumps involves allowing the inflammation to settle down, which may simply involve not shaving for a while to allow the bumps to go away. Your doctor may also be able to prescribe a cream to help the inflammation.
Razor bumps is appropriately called pseudofolliculitis barbae when it affects the beard area, which is perhaps the most common area of involvement. Razor bumps is more common in men and darkly pigmented individuals with tight, curly hair. Prevalence of razor bumps (pseudofolliculitis) is higher among males of African ancestry than among Caucasian men. However, razor bumps (pseudofolliculitis) can also occur in women and in other shaved areas such as the neck, pubic, and armpit regions.
Recent research has confirmed a genetic predisposition to razor bumps (pseudofolliculitis) in the African population. A single nucleotide substitution in the hair follicle companion layer-specific keratin (K6hf) is shown to increase the chance of razor bumps (pseudofolliculitis).
Whereas folliculitis represents an infection of the hair follicle, pseudofolliculitis is caused by inflammation secondary to trauma. Interestingly, this trauma is caused by the hairs themselves. When tight, curly hairs are shaved, they are cut at an oblique angle that allows the sharp tip to penetrate the skin as it curves. This re-entry of hair into the skin causes a significant degree of inflammation. Close shaves are particularly problematic because they leave a sharp tip beneath the surface of the skin that is primed for re-entry.
Razor bumps (pseudofolliculitis) presents as red bumps in the beard (or other shaved) area that are often painful and/or itchy. Sometimes, pustules or deep boils develop. These red bumps eventually turn dark and firm as they heal, often appearing much darker than the surrounding skin. Some people develop abnormally large scars or keloids. Unfortunately, in chronic or untreated cases, the post-inflammatory hyperpigmentation may be difficult to treat and scarring/keloid development permanent.
- Razor bumps (pseudofolliculitis) is a chronic condition. The only way to stop the inflammatory cycle is to stop shaving, and most people do not like to hear this!
Although total abstinence from shaving may (ultimately and with great care) be avoided, it is very important to at least temporarily stop shaving so that healing may occur. Resolution of active inflammation can take anywhere from a few months to one year (in the case of very severe disease), so patience is required. Continuing to shave over inflamed skin can cause the development of permanent scars or keloids, as well as permanent changes to the hair. An alternate to shaving during this time is to use electric clippers or scissors, leaving at least ½ cm of hair present at all times.
Medical evaluation should be sought during the period of acute inflammation. Depending on the degree of inflammation, oral antibiotics, topical corticosteroids, or even oral corticosteroids may become necessary.
A number of options are available to treat this condition. Tretinoins, alpha-hydroxy acids, and benzoyl peroxide work well in mild to moderate disease by exfoliating the areas involved and removing excess skin. A bleaching agent such as hydroxyquinone may be useful in improving the appearance of post-inflammatory hyperpigmentation. Some patients choose to undergo hair removal (via creams or lasers) to reduce hair density and thus decrease the risk of hair penetration.
Once the acute inflammation resolves and all of the ingrown hairs are gone, shaving can be attempted for those who cannot abstain from shaving forever. This will likely lead to the recurrence of lesions, but the following steps may help to minimize this risk:
- Before shaving, wash the area to be shaved with a gentle acne soap and a rough washcloth.
- Soak the face with a moist hot towel, and apply a shaving cream, gel, or foam prior to shaving.
- Always use a sharp blade and avoid cutting too close to the skin.
- Use a single blade razor.
- Shave in the direction of the hair with short strokes.
- Do not shave over one area more than once.
- After shaving, apply soothing aftershave lotion.
Although razor bumps can be quite bothersome, there are a number of preventative methods that can be taken to improve its appearance. In addition, multiple treatment modalities are available and should be chosen with the help of a skin specialist who can discuss their associated risks and benefits.
Figure 1. Razor bumps on neck

Figure 2. Hair structure
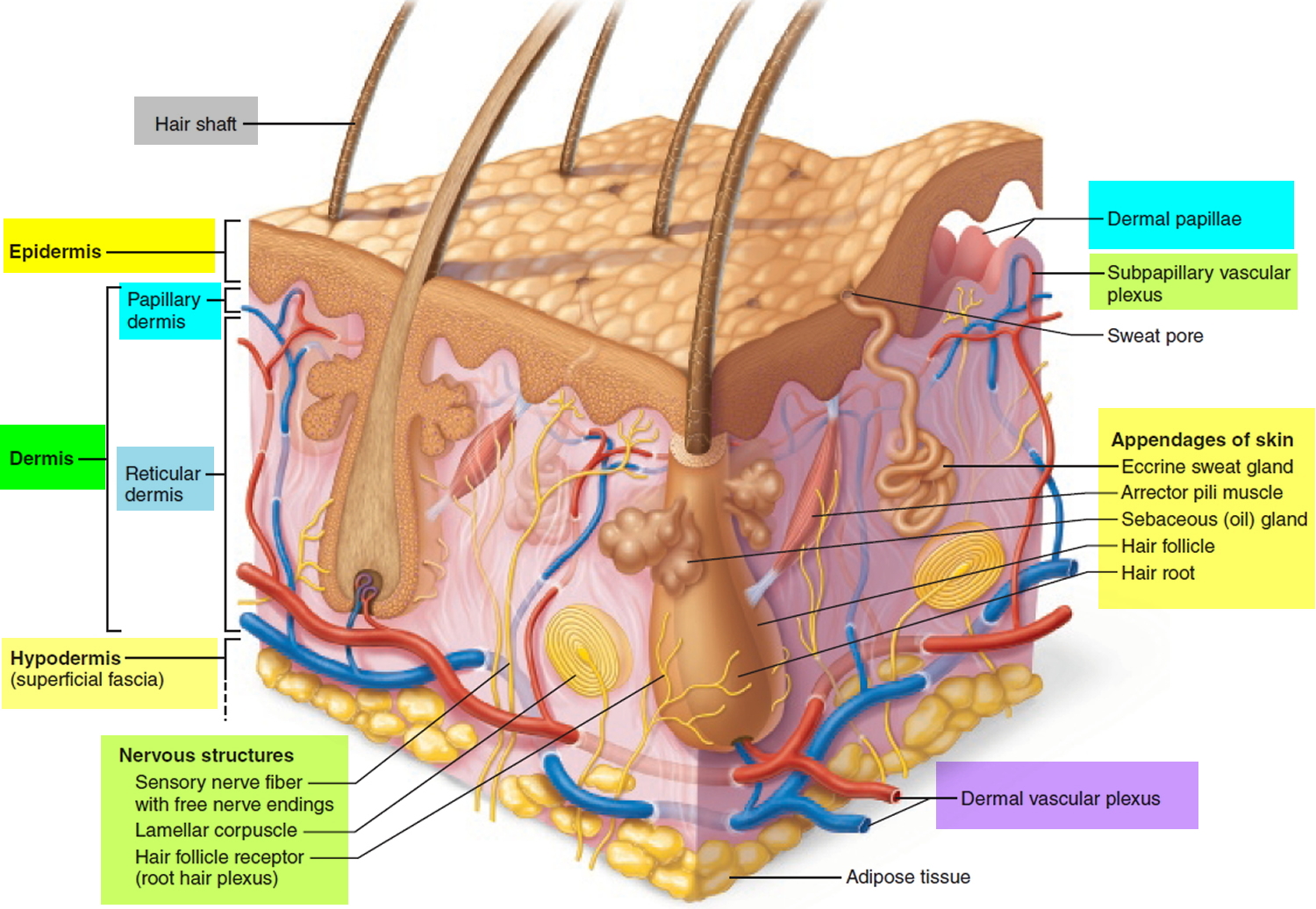
Figure 3. Hair follicle
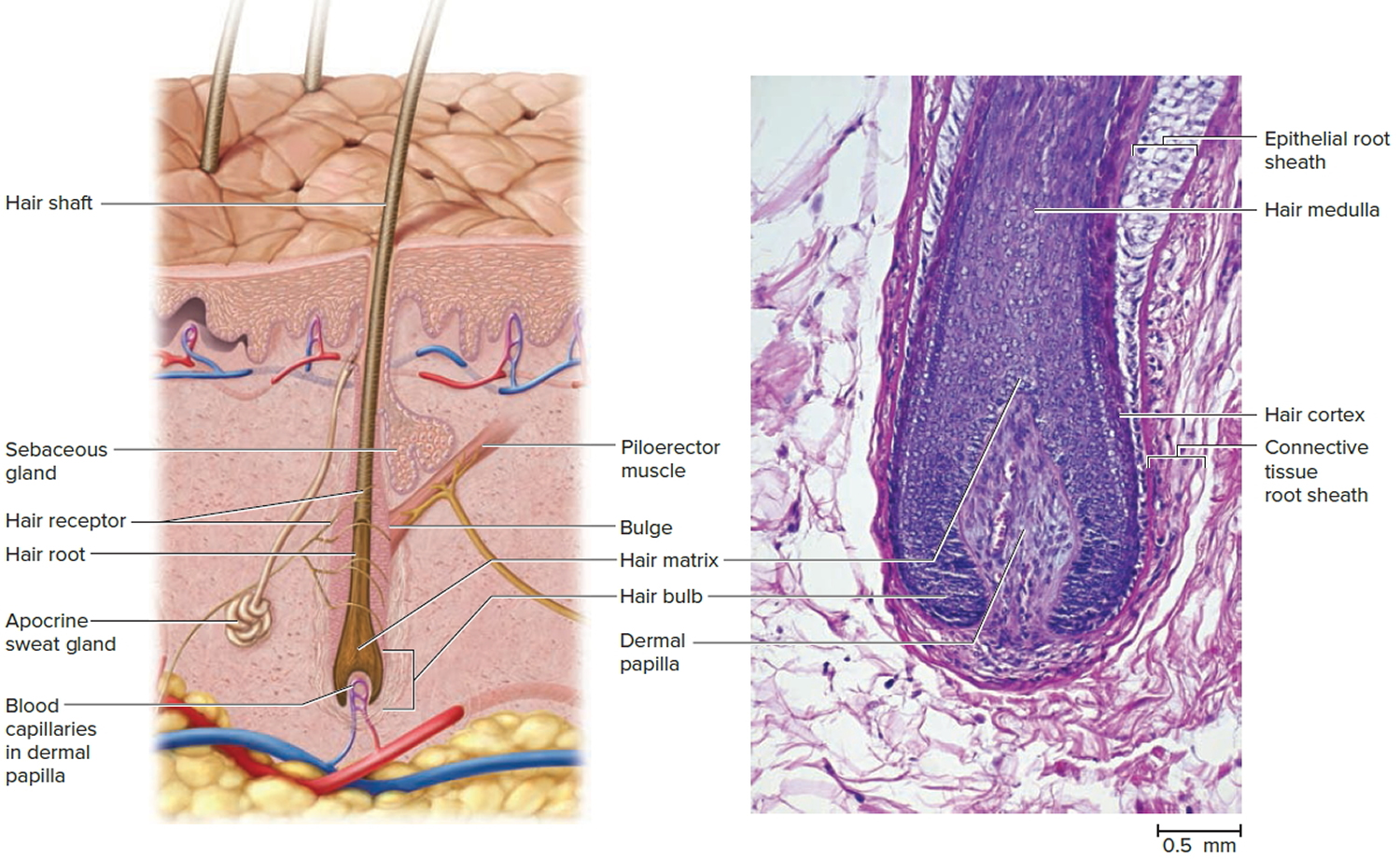 Figure 4. Razor bumps
Figure 4. Razor bumps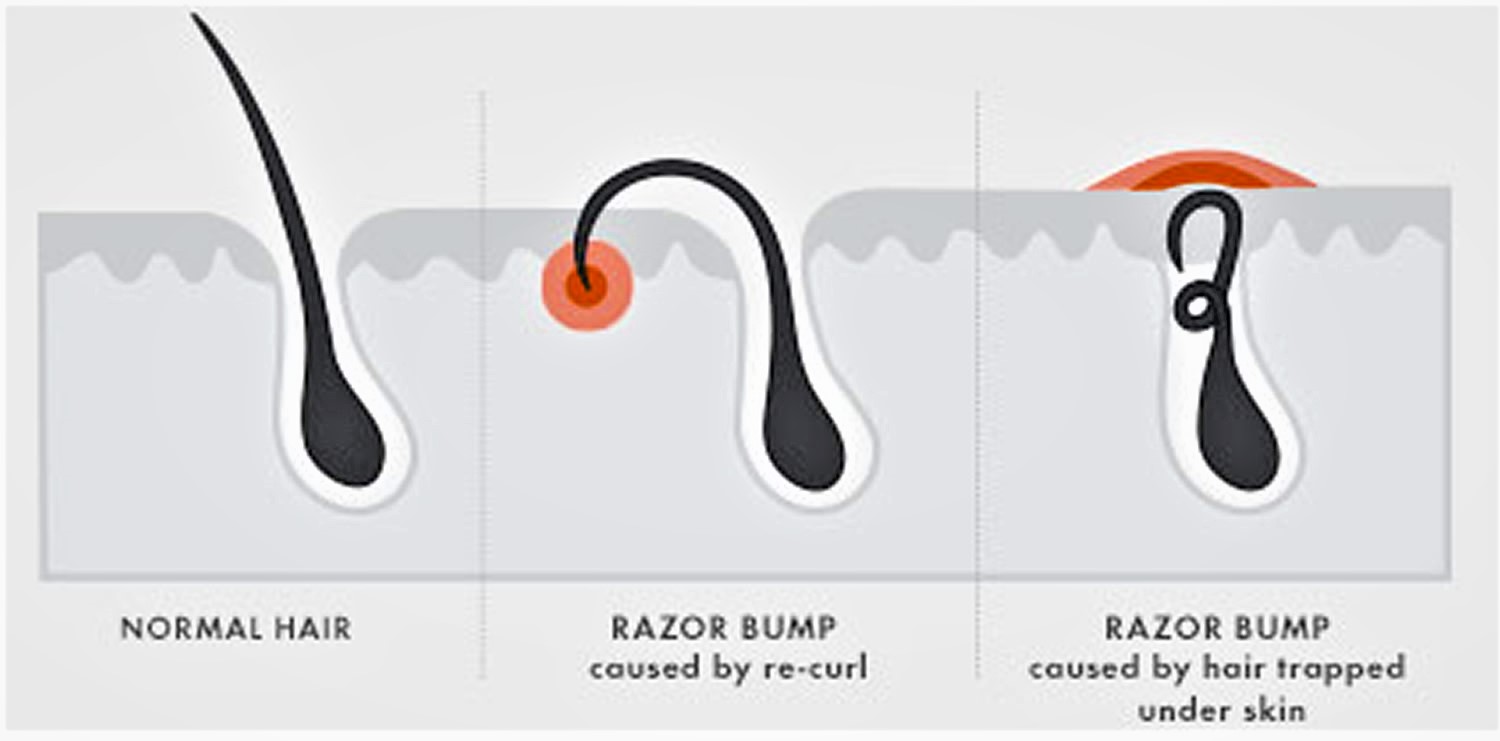
Figure 5. Ingrown hair – note multiple pustules in the beard secondary to ingrowing hairs.

What causes razor bumps
Razor bumps (pseudofolliculitis) is due to shaving, particularly close shaving—because the cut hair may retract beneath the skin surface.
Hair grows inside tubes in the skin called “follicles.” When shaved, the tip of the hair is left with a sharp point. As curly hair grows, this sharp tip may curve back and re-enters the skin close by causing a foreign body inflammatory reaction. The medical term for this cause of razor bumps is “extrafollicullar penetration.”
Razor bumps can also form when shaving too close to the skin, which causes the whiskers to be clipped off below the skin surface. This allows the hair to penetrate the side of the follicle instead of following it’s normal path to the skin’s surface. This can occur more often with curly hair. The medical term for this cause of razor bumps is “transfollicular penetration.”
Razor bumps are not infected (if the bump becomes infected, it is called folliculitis barbae), but they are irritated.
The injured follicles are highly susceptible to become infected, causing folliculitis barbae. Folliculitis barbae is a type of folliculitis affecting the beard area due to infection with the bacteria Staphylococcus aureus. It occurs in men who shave and in men that do not shave. Deep-seated folliculitis barbae is called sycosis barbae, and leads to scarring and areas of permanent hair loss.
After shaving, you may experience an acne-like eruption on the area that has been shaved, usually the face and neck of men or bikini and pubic area of women.
- Razor bumps (pseudofolliculitis) presents as ingrown hairs associated with flesh-coloured or red follicular papules, which may be itchy or tender.
- Folliculitis barbae presents as painful pustules and can discharge pus.
- Lesions may bleed when they are shaved.
Folliculitis barbae and razor bumps (pseudofolliculitis) are aggravated by co-existent eczema/dermatitis.
What are the complications of razor bumps
Complications of razor bumps include:
- Postinflammatory hyperpigmentation
- Hypertrophic scarring and keloid formation
- Temporary and permanent hair loss
- Sycosis barbae – sinuses, abscesses and spreading infection due to infection and autoinflammatory reaction
How to prevent razor bumps
To prevent razor bumps recurrence, follow a proper shaving regimen long term and consider hair removal. Methods may include:
- If you don’t mind growing your hair, do so. This is curative!
- The chances of having razor bumps is greatly reduced if the hairs are kept at least a few millimeters long.
- If shaving is a must, please try the following shaving regimen:
- Apply a warm compress to the area for a few minutes prior to shaving.
- Ensure the skin is well moisturized, for example using a lotion containing glycolic acid to the affected areas. This exfoliates the surface skin cells and reduces the likelihood of new inflamed spots.
- Use a mild exfoliant, such as a extra gentle Buf-Puf facial sponge or loofah or better still a soft bristle (clean) toothbrush. Massage the area that is prone to ingrown hairs prior to shaving. Massage in a circular motion to help release the hairs that have curled inward. Some even use a toothpick to release hairs that have grown back on themselves.
- Cleanse the skin using a polyester skin-cleansing pad or a moisturizing shaving foam.
- Use a shaving gel designed for sensitive skin.
- Do not pull the skin taut when shaving.
- Either use a single blade disposable razor, or use electric hair clippers or a razor with an attachment that leaves the cut hairs long.
- Sterilize metal hair clippers and electric razors using boiling water, and plastic items should be soaked in antiseptic solution.
- Shave in the direction of hair growth (hairs pointing down, shave with a downward stroke). Do not shave against the direction of hair growth. Shaving against “the grain” will worsen the condition. On the neck, shave with the grain in a downward stroke only, never up.
- Take short strokes and do not shave back and forth over the same areas. One or two strokes in each area will suffice. Remember you do not want too close of a shave.
- After shaving, use a Hydrocortisone 1% lotion (available over-the-counter) to soothe any “razor burn” or irritation if needed.
- At night use any medication prescribed by your doctor e.g. Eflornithine cream. Eflornithine hydrochloride applied topically as a cream twice daily is the first agent known to help slow the rate of excessive hair growth. It is marketed under the brand name Vaniqa® and comes as eflornithine hydrochloride 13.9% cream. Eflornithine works by blocking the enzyme ornithine decarboxylase that stimulates hair growth. Eflornithine HCl cream 13.9% has been shown to slow the rate of hair growth in animal and human studies. Studies with eflornithine cream have been limited to treating unwanted hair on the face, around the lips and chin. Eflornithine hydrochloride is available on prescription from a doctor in the United States and elsewhere. Eflornithine HCl cream is very well tolerated. Some women may experience minor and temporary skin irritations including:
- redness
- stinging
- burning
- tingling
- rash
- ingrown hairs (pseudofolliculitis barbae)
- acne
- If skin irritation develops, the Eflornithine HCl cream dose may be reduced to once a day. If irritation continues you should stop using the cream.
- A laser beam can be used to get rid of hair by destroying the hair at its base. This procedure has to be done by a dermatologist (a skin doctor). It is probably the most expensive way to get rid of hair. In the future, it may become a permanent way to remove facial hair. Laser hair removal, especially Nd:YAG and diode lasers, but there is a risk of causing white or dark marks in skin of color.
- Electrolysis is the only permanent way to remove hair. A thin metal probe is inserted in the opening in the skin where the hair grows. An electric current destroys the hair at its base. You may need to get this treatment more than once to get rid of the hair for good. Electrolysis is more expensive. It isn’t done by a doctor. If you have a pacemaker, you can’t use this method.
- Chemical depilatories such as barium sulfide paste and calcium thioglycolate; these can be irritating
- Intense pulsed light (IPL)
How to get rid of razor bumps
Medical treatment of razor bumps:
- Hydrocortisone cream can reduce mild inflammation and itching.
- Topical acne treatments such as benzoyl peroxide and tretinoin are used to suppress follicular hyperkeratosis.
- A combination of tretinoin, low-potency topical corticosteroid, and hydroquinone may be selected to decrease inflammation, hyperkeratosis and pigment production.
- Oral tetracyclines are used to reduce inflammation.
- Photodynamic therapy has been successful.
- Infected ingrown hair are treated with topical or oral anti-staphylococcal antibiotics.
Any plucking should stop. The tip of the hair may be teased out, releasing the hair. Laser hair removal may be a permanent solution for problematic areas.
- Growing your hair is curative.
- Release hairs. Hair releasing is critically important and must be done instead of plucking hairs. Hair releasing means removing the end of any hair buried in papules or pustules. Hair releasing may be done with a toothpick or a needle yourself or by your physician. Use a sterile needle to gently lift embedded hair tips. You may need to release your hairs every two to three days.
- Laser ablation.
- Shave carefully (see prevention above).
- Depilatories may work for some.
Growing hair is curative. Even a short hair is excellent. If this is not possible, various tips may allow for a relatively close shave.
- Use a shaving gel and a sharp razor.
- Don’t pull the skin taut.
- Shave with the direction of hair growth
- Shave each area only once.
- After shaving, apply a soothing after shave or hydrocortisone 1% lotion (available over-the-counter) to soothe any “razor burn” or irritation if needed.
A depilatory may be used, but many find these too irritating.
Laser hair removal may be helpful. For darker-skinned patients, the longer pulsed lasers (e.g. 1064 nm or 810 nm) may be used.
If inflammatory pustules or papules are present, topical benzoyl peroxide or a combination benzoyl peroxide with clindamycin product may be recommended. Topical retinoid every night at bedtime may be helpful, especially if there is post inflammatory hyperpigmentation.
Eflornithine 12% topically twice daily for 16 weeks was shown in one study to work synergistically with laser hair removal 1.
References




{kind=link}