What is the hyoid bone
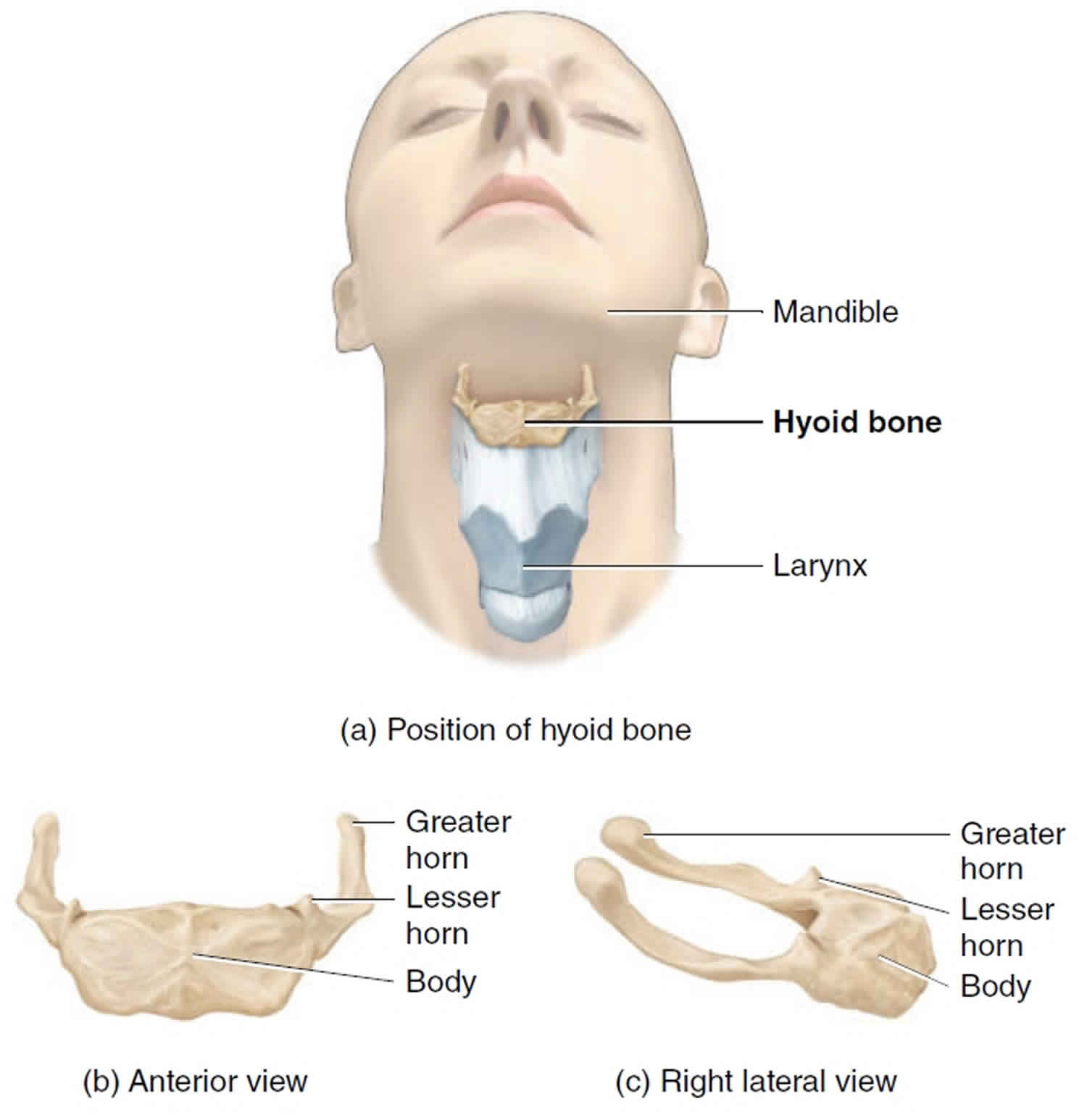
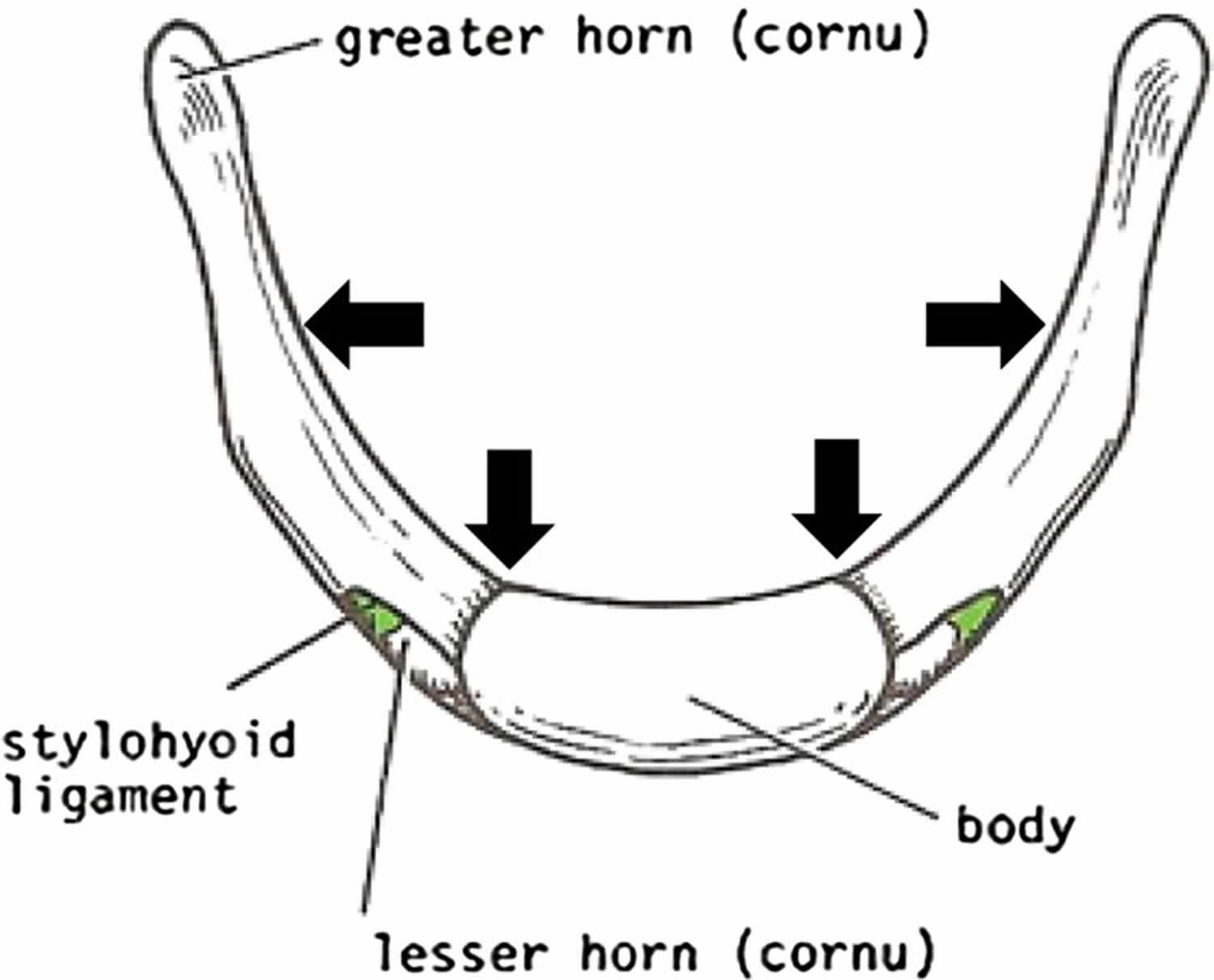
The hyoid bone is a small U-shaped mobile bone (Figure 1) oriented in the horizontal plane just superior to the larynx, where it can be palpated and moved from side to side. The hyoid bone resembles an archer’s bow. The hyoid bone has a body and two pairs of horns, each of which is also called a cornu, the Latin word for “horn.” The greater and lesser horns (cornua) fuse to body of hyoid bone between 40 and 60 years of age although non-fusion has been found even after the age of 60 years 1. The body of the hyoid bone is anterior and forms the base of the U. The two arms of the U (greater horns) project posteriorly from the lateral ends of the body. The hyoid is the only bone in the skeleton that does not articulate directly with any other bone in the head and neck. Instead, the hyoid bone lesser horns are tethered by thin stylohyoid ligaments to the styloid processes of the temporal bones. Other ligaments connect the hyoid to the larynx (voice box) inferior to it.
The hyoid bone and the cartilages of the larynx and trachea are often fractured during strangulation. As a result, they are carefully examined at autopsy when manual strangulation is a suspected cause of death.
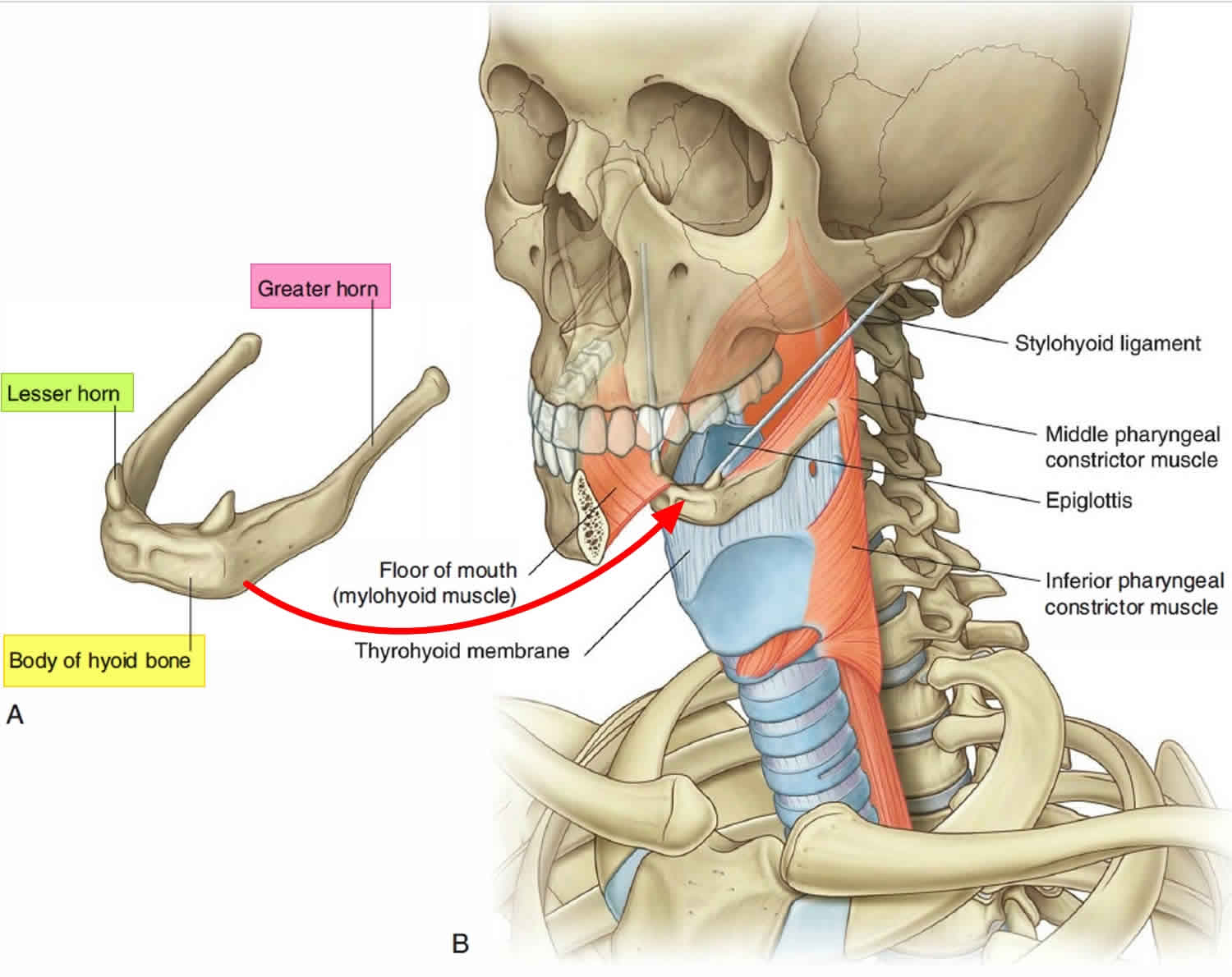
The hyoid bone is a highly movable and strong bony anchor for a number of muscles and soft tissue structures in the head and neck. Significantly, the hyoid bone is at the interface between three dynamic compartments:
- Superiorly, the hyoid bone is attached to the floor of the oral cavity.
- Inferiorly, the hyoid bone is attached to the larynx.
- Posteriorly, the hyoid bone is attached to the pharynx.
Figure 1. Hyoid bone anatomy
 Where is the hyoid bone located?
Where is the hyoid bone located?
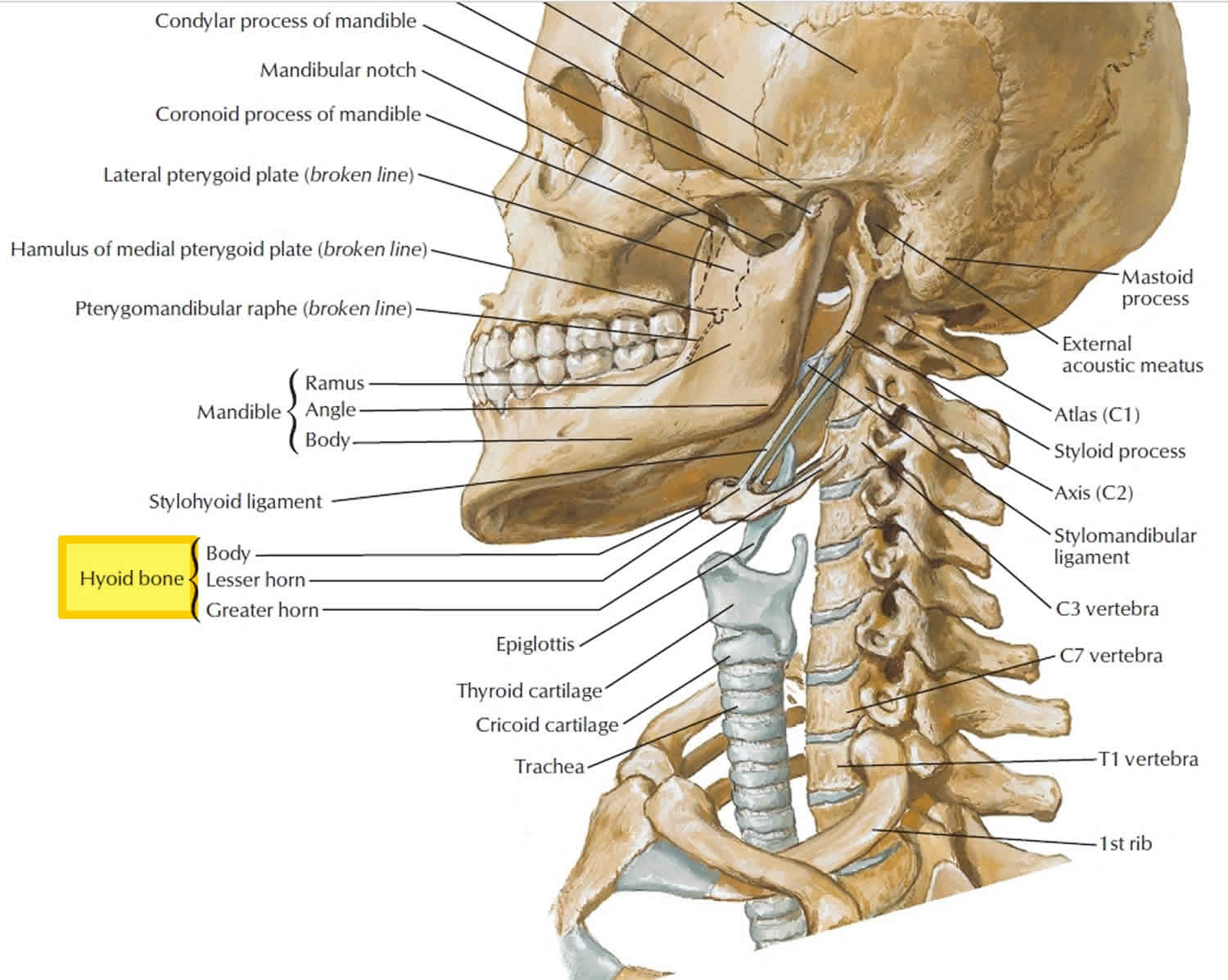
The hyoid bone (“U-shaped” bone) lies just inferior to the mandible (between the mandible and the thyroid cartilage) in the anterior portion of the neck at the level of the C3 vertebra. The single hyoid bone is a unique component of the axial skeleton because it does not articulate with any other bone. Rather, it is suspended from the styloid processes of the temporal bones by ligaments and muscles.
What does the hyoid bone do?
Functionally, the hyoid bone supports the tongue, providing attachment sites for some tongue muscles and for muscles of the neck and pharynx. The hyoid bone acts as a movable base for the tongue. Furthermore, the hyoid bone body and greater horns are points of attachment for neck muscles that raise and lower the larynx during swallowing. Because of hyoid bone morphology and its position amongst the other anatomical structures of the neck, it is associated not only with the sound production and the fully articulate human speech, but also with the smooth function of the airway and possibly with the normal swallowing.
Broken hyoid bone
Hyoid bone fractures resulting from trauma other than strangulation are very rare; hyoid bone fracture associated with panfacial trauma are even rarer 2. A fracture of hyoid bone secondary to trauma other than strangulation is a rare incident with only 31 cases being reported so far in the world literature 3. Hyoid bone fracture accounts for 0.002 % of all fractures 2, but a higher incidence of 1.15 % was found by Stiebler and Maxeine 4. Hyoid bone fractures occur more frequently in young individuals, and in men more than in women 5.
Suspended from the styloid process, the hyoid bone is not susceptible to fractures owing to it’s inherent protection which is secured by its safe position and reinforced by its mobility. The hyoid bone is encircled, in normal anatomic position, by bones: anteriorly and laterally by the mandible and posteriorly by the cervical spine. Therefore, the hyoid bone is a well protected bone in the neck. However, when the neck is hyperextended, the protection is diminished, which allows the trauma to cause an isolated fracture of the hyoid bone 2. Fractures are seen frequently in fusion of greater horn and body and mid-portion of greater horn (Figure 3). Patient’s age ranges between 15 and 55 years [7]. Most patients are under 35 years old, which may refer to the elastic cartilage-structure of the hyoid bone. They affect more frequently young individuals with a greater prevalence in the male gender.
Injuries to the hyoid bone are rare. The most commonly reported injury is fracture, yet this is often a post-mortem finding, with an incidence of between 17–76 percent, in victims of strangulation and hanging 2. In survivors it is more often associated with a trauma other than manual strangulation.
Figure 2. Hyoid bone fracture
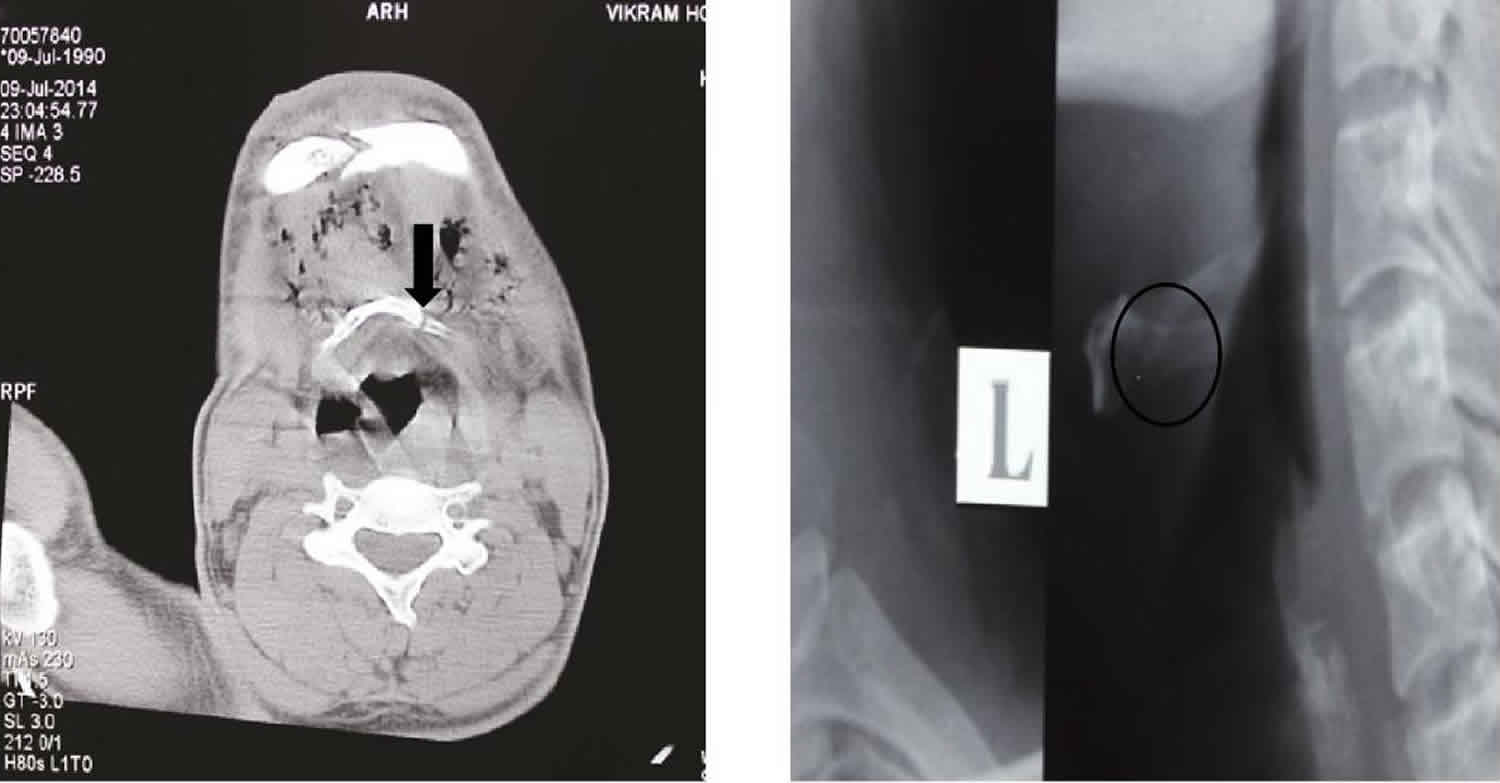
Footnote: A 24 year old man presented to the emergency room with a complaint of pain over the face and neck region following a road traffic accident. His symptoms on presentation were a constant and severe neck pain, localized on the left side, with marked odynophagia (painful swallowing) when opening his mouth, swallowing or speaking. The patient had no dyspnea or signs of airway compromise. Physical examination revealed tenderness over right chin and malar region, entire right side of maxilla was mobile with a midline split of maxilla, avulsion of mandibular incisors, tenderness on palpation of left side of hyoid bone with no external wounds noticed on neck except for some blunt traumatic injuries. Occlusion was deranged with maximal mouth opening of 30 mm; opening the mouth over this limit was painful. Diagnosis was achieved by a CT scan, orthopantomographic radiograph, lateral and antero-posterior view of cervical radiographs, which showed a fracture of the hyoid bone with panfacial fractures. Open reduction and internal fixation with mini plates was done for panfacial fractures, and the hyoid bone fracture was treated conservatively under general anesthesia without any complications while intubation.
[ Source 2 ]Figure 3. Weak areas of hyoid bone leading to fracture (arrow marks)
Hyoid bone fracture causes
In general hyoid bone fractures are reported to occur in 50 % of cases of manual strangulation or of ligature strangulation and in 27 % of hanging 6. It can be classified into 6:
- Inward compression fractures with outside periosteal tears.
- Antero-posterior compression fractures with inside periosteal tears.
- Avulsion fractures.
Most cases of hyoid bone fractures are presented due to road traffic accidents, gunshot and knife wounds, others have happened during basketball, karate, martial arts or ice hockey as a result of falling assault, iatrogenically created following cervical spine surgery, or during attempts of resuscitation. Vomiting was also reported to be a causative factor 7.
Hyoid bone fracture complications
Complications of hyoid bone fracture are divided into early and late. Early complications include subcutaneous emphysema, dyspnoea, pharyngeal tears and thyroid cartilage injury. Late complications are dysphagia, stridor, pseudoaneurysm of the external carotid artery, and crepitus by neck flexion 5. Dysphagia, dysphonia, and dyspnoea with stridor, may develop quickly. Therefore, close observation of the patient for a minimal of 48–72 hour is strongly recommended 8.
Hyoid bone fracture diagnosis
Diagnosis is difficult and is usually made with a strong degree of suspicion. Patients may suffer from severe pain in the area of throat, which is exaggerated by swallowing, nose blowing, or coughing. The most frequently presenting signs include anterior neck tenderness, swelling, ecchymosis, subcutaneous emphysema and crepitus, on palpation. Related symptoms such as dysphagia, severe pain especially by swallowing, or even dyspnoea may occur. Patient may suffer suffocation by tongue protrusion. Profuse bleeding may result from penetration of the bone fragments into the soft tissue and the pharynx.
Physical examination may reveal swelling in the area of trauma, crepitus in the neck, tenderness on palpation, and pain on moving the head. If a hyoid bone fracture is clinically strongly suspected in a patient with neck injury, diagnosis is made by radiographs, computed tomography, laryngoscopy, and surgical inspection (penetrating trauma) 9. Certain criteria are made for radiographic diagnosis including: radiolucent line, interruption of the cortical continuity, or displacement of the fragments. Laryngoscopy and CT scan are recommended for dyspnoea, haemoptysis, or bleeding from laryngeal lacerations, in order to assess the extent of injury.
Hyoid bone fracture treatment
Treatment depends on the severity of affliction, symptoms and signs. However, it has been suggested to achieve the laryngoscopic examination in all suspected cases of hyoid bone fracture 10, unless cervical spine injury is present.
Hyoid bone fracture treatment can be divided clinically into 11:
- Asymptomatic: usually needs no treatment.
- Symptomatic: treatment is organized according to the presence of:
- Mild or severe pain on turning head and swallowing: analgesics for few days, limitation of the movement of head and a soft diet may be useful.
- Pharyngeal laceration: Suturing the deep wounds, removing the fragments of hyoid bone fracture if present, and smoothing the ends are suggested. Fixation of fractured fragments by means of wiring is recommended especially when the fracture line runs through the curved greater cornua, at its junction with the body. Patients with dysphagia may need gastric tube feeding.
- External laceration of the neck: primary wound care and excision of the fragments of hyoid bone fracture if present have been suggested.
- Respiratory distress: may develop rapidly and without warning and can end with a cardiovascular collapse. For airway obstruction, endotracheal intubation or tracheostomy must be applied. However, in massive subcutaneous emphysema, surgical exposure and drainage of retro-pharyngeal space is mandatory. The associated injuries must be taken to consideration in the treatment plan.
Hyoid bone fracture prognosis
Even in cases of non-union, the prognosis for hyoid bone fractures is good. Prognosis in cases involving laryngeal laceration may be less favorable due to underlying complications such as increased edema, hemoptysis, dyspnoea and risk of infection. While osseous healing in any fracture typically occurs in 6 weeks, symptom resolution for a hyoid fracture has been reported at 2–8 weeks 1.
Hyoid bone dislocation
There are currently no reports of hyoid bone dislocation secondary to sport-related trauma 12. Only 1 other reported case of hyoid dislocation currently exists in the literature, and it involves a 45-year-old man who presented with 1 year of odynophagia and dysphonia after an argument triggered the acute onset of right-sided neck pain 13. Laryngoscopy revealed a mass in the right hypopharynx, and treatment with partial resection of the lateral hyoid was performed. The authors reported full resolution of symptoms, and repeat laryngoscopy demonstrated disappearance of mucosal indentation.
In this case report, Knapik et al. 12 reported a high school football player presenting with an acute hyoid dislocation in the setting of a subacute fracture sustained 6 weeks prior. The patient was a 15-year-old high school sophomore who sustained a direct blow to the anterior neck by the helmet of a teammate during contact drills at practice. At the time of injury, the patient was in full pads, with his appropriately fitted helmet in place and secured with a hard-shell chinstrap. Following the collision, he was able to stand and walk off the field with no loss of consciousness. He presented to the athletic trainer complaining of headache, throat pain, and amnesia to the event. During physical examination, the athletic trainer noted confusion, slowed speech, and right upper extremity weakness to the deltoid, infraspinatus, and subscapularis graded as 4 out of 5 strength on examination. The patient complained of odynophagia; however, no dysphonia or stridor were detected. Intense pain was elicited with palpation of the anterior aspect of the neck at the level of the thyroid cartilage, but no pain was elicited with cervical range of motion testing in all planes. Out of concern for concussion, throat pain, and weakness, he was advised to go to an emergency room for further examination.
Following arrival to the emergency department 2 hours after injury, the patient continued to complain of throat pain, dizziness, and confusion. Vital signs were normal, and on physical examination, the neck was symmetric in appearance with no ecchymosis or cervical edema. On palpation, point tenderness was noted over the right upper midline of the neck at the level of the thyroid cartilage, although no crepitus, masses, or lymphadenopathy was present. The hyoid was mobile during swallowing, even though the player continued to report odynophagia. He also continued to demonstrate right upper extremity weakness to the shoulder, scored as 3 out of 5 strength by the emergency department physician.
During examination, the player reported a similar injury 6 weeks prior, during a game in which he was tackled and the opponent’s helmet was driven into his upper chest, causing his hard-shell chinstrap to hit his throat. He reported having had minor difficulty breathing and odynophagia following the injury but was able to complete the game. He also reported having minor neck pain on palpation and odynophagia following the injury, which gradually resolved after 4 weeks. He did not cite this injury or symptoms to the athletic trainer, coach, or team physician, and he missed no games or practices. The athlete denied having any preceding neck trauma or possessing symptoms of odynophagia or difficulty breathing prior to this initial injury.
For comfort, a soft cervical collar was placed in the emergency department. Computed tomography (CT) of the head and magnetic resonance imaging of the brain were performed out of concern for concussive symptoms (i.e., confusion and slowed speech), and results revealed no abnormalities. Of note, following return from imaging, the player had complete resolution of right upper extremity weakness, graded as 5 out of 5 strength. Cervical CT of the neck demonstrated medial displacement of the posterior portion of the right aspect of the hyoid bone, impressing on the right epiglottis and causing an asymmetric appearance of the pharyngeal mucosa (Figure 1, A–C). No acute fracture was noted, but acute angulation to the right side of the hyoid was noted, with well-corticated edges and minimal callus formation, suggestive of a prior-healed fracture approximately 4 to 6 weeks old, based on consultation with 3 musculoskeletal radiologists (Figure 4, D–F). No free air within the neck was appreciated. No malalignment of the cervical spine or stenosis of the spinal canal or foramina was present, and no additional injuries to the laryngeal skeleton were noted. CT arteriogram of the neck revealed no vascular abnormalities.
Figure 4. Hyoid bone dislocation
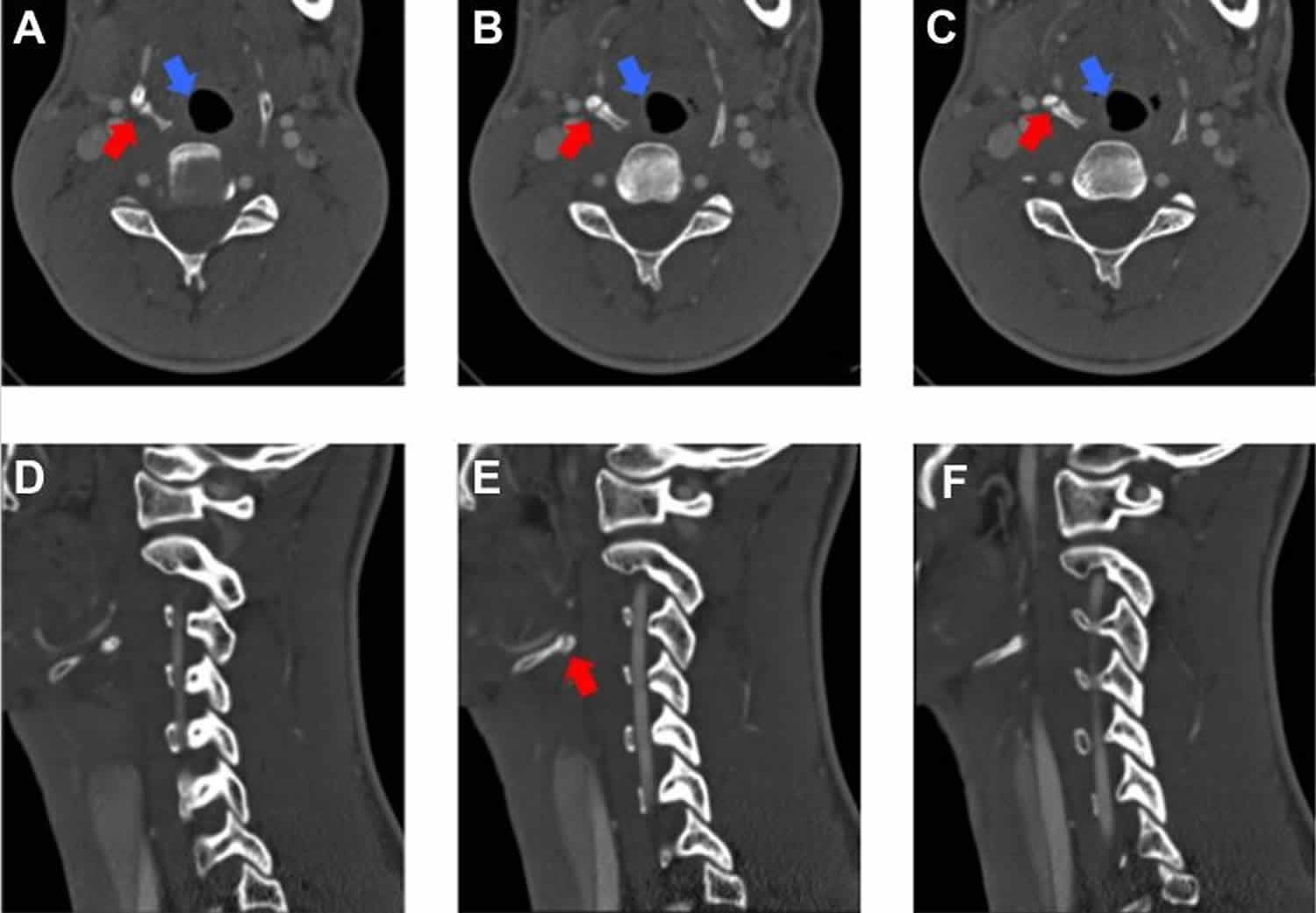
Footnote: (A-C) Noncontrast computed tomography scans (axial views) of cervical region showing medial displacement of the right aspect of the hyoid (red arrows) causing mild compression of the epiglottis and pharyngeal mucosal space (blue arrows). (D-F) Noncontrast computed tomography scans (sagittal views) showing angulation and displacement of the hyoid with well-corticated edges (red arrow), indicative of prior fracture.
[Source 12 ]Owing to continued point tenderness and odynophagia, the player underwent flexible nasopharyngoscopy that demonstrated slight effacement of the right hypopharynx mucosa, more easily seen during phonation. No mucosal injury, masses, or lesions to the pharyngeal walls were present. True vocal movement was intact bilaterally and the airway widely patent with no evidence of obstruction.
The player was admitted for 24 hours of observation to detect for possible worsening edema or decline in swallowing function. He remained stable and was discharged the following day with instructions to remain on a soft diet for 48 hours and progress as tolerated while remaining in the collar. At his 2-week follow-up with the otolaryngologist, he was still in the collar because of the mild neck pain that he experienced when turning his head; however, his odynophagia had resolved, and he was tolerating a regular diet. His otolaryngologist did recommend retirement from football for fear of additional, more severe injury to the hyoid and neck from direct-impact trauma leading to potential complications involving the airway28 or external carotid artery.2 Three weeks following injury, he reported being asymptomatic with no neck pain throughout range of motion, and the collar was discontinued. Despite the absence of neck pain, he remained sidelined and restricted from all contact through the conclusion of the football season secondary to persistent concussive symptoms. His pediatric neurologist cleared him 37 days following injury for full-contact participation in time for the start of basketball. During the basketball season, he remained asymptomatic, playing in every game and having no recurrent symptoms or additional injuries to the neck.
No consensus exists for the treatment of hyoid fractures or dislocations, thereby necessitating that treatment be tailored per individual presentation and symptom severity 14. Asymptomatic patients or those with mild symptoms and no airway compromise or progressively worsening dysphonia or dysphagia are generally treated conservatively. Analgesics, soft collar immobilization for comfort, and a brief period of a soft/liquid diet with close observation allow for symptomatic resolution 15. A period of in-hospital observation between 48 and 72 hours following injury is also recommended to watch for the potential development of late complications, such as dysphagia, dysphonia, or dyspnea secondary to airway obstruction 16. One patient in the literature developed acute airway obstruction as far out as 51 hours following injury 17. In the setting of pharyngeal lacerations following hyoid fracture, surgeons may elect to smooth the sharped ends of bone 18, perform wire reduction and internal fixation 19, or undergo partial or total hyoid bone removal 18. In patients with acute respiratory distress, endotracheal intubation or surgical tracheotomy may be required to ensure an adequate airway 20.
Overall, the prognosis for patients suffering hyoid fracture or dislocation is good in the absence of acute airway compromise, pharyngeal laceration, or late complications secondary to swelling or infection 16. In uncomplicated cases, symptoms generally resolve between 2 and 8 weeks, with athletes successfully returning to sports following resolution of neck pain 21. For patients with fractures that progress to nonunion based on repeat cervical radiographs, no significant lasting effects on swallow function or neck pain have been documented, with most patients reporting satisfactory results 22.
Despite properly fitted helmets and chinstraps, injury to the hyoid may be encountered when contact from the helmet of another player is directed to the upper chest and neck. Because of the potential life-threatening consequences associated with fracture or dislocation, a high index of suspicion must be maintained for hyoid injury in athletes presenting with generalized neck pain, point tenderness, or odynophagia following neck trauma in any sport.
Hyoid bone syndrome
In 1954 Brown described a so-called hyoid bone syndrome 23, that is tenderness at the site of the greater horn of the hyoid bone. His paper, however, did not offer any definitive treatment. In 1968 Steinmann reported the hyoid bone syndrome as a form of “insertion tendinois,” for which he recommended the use of procaine hydrochloride injection with corticosteroid at the tip of the greater hyoid horn for relief of pain. The relief, however, was temporary 23. Saito et al. 24 describe hyoid bone syndrome as a disease caused by an abnormality in the apparatus hyoid, indicated by a variety of symptoms such as a feeling of discomfort in the pharyngolarynx, neck pain, a clicking sound when twisting the neck, etc. They report on two cases of hyoid bone syndrome accompanying an excessively long greater cornu of the hyoid bone. Case 1 consulted the hospital with the excessively long of discomfort when swallowing along with a clicking sound when swallowing from several years prior 24. The greater horn of the hyoid bone on both sides was found to be long upon neck CT scan, in addition to approaching the transverse process of the fourth cervical vertebra. Case 2 became aware of neck pain from 1 year prior and consulted the hospital due to exacerbation of the symptoms. The excessively long greater horn of the hyoid bone was observed on both sides of neck on CT imaging, with the greater horn of the hyoid bone approaching the transverse process of the third cervical vertebra. From the above, the patient was diagnosed with hyoid bone syndrome accompanying an excessively long greater cornu of the hyoid bone on both sides, with prominent improvement in symptoms observed when partial resection of the bilateral greater cornu of the hyoid bone was carried out, yielding good results 24.
Although such cases may be diagnosed as pharyngolaryngeal paresthesia, when symptoms are observed over a long period of time and the complaint is strong and clear, an in-depth examination including imaging testing is required. Moreover, it was believed that resection of the greater cornu of the hyoid bone is a useful treatment for hyoid bone syndrome.
Nir and colleagues 25 treated their patients with suspected hyoid bone syndrome (38) with oral nonsteroidal anti-inflammatory drugs (NSAIDs) and/or with an NSAID ointment for topical application. Symptomatic relief was obtained in 66% of their patients and in 71% of the patients treated by nonsteroidal anti-inflammatory drug (NSAID) tablets 25. Symptomatic relief was obtained in 91% of their patients with symptom durations of less than 6 weeks 25. Nir et al. 25 recommended a course of NSAID therapy as the first method of treatment for hyoid bone syndrome before treatment with invasive procedures, especially for patients with symptom durations of less than 6 weeks. Better recognition of the hyoid bone syndrome will result in a more effective treatment and will avoid an unnecessary investigation.
Stern et al. 26 presented a case study involving eighty-four patients who presented with throat pain and had tenderness of one (63%) or both (38%) greater horn of the hyoid bone. Stern and colleagues 26 treated their patients with injections of triamcinolone acetonide (40 mg/mL). Seventy-four percent of the patients had complete resolution of their symptoms with injection of the affected side(s), 15% had a partial response, and 10% had no response 26. One patient had a recurrence at 3 months and chose not to receive another treatment. Forty-five of the 62 patients with a complete response required only 1 injection. Forty-three patients (51%) also complained of dysphonia, only 5 of whom had additional laryngeal disorders that accounted for the dysphonia. The authors concluded that hyoid bone syndrome should be considered in patients who present with throat pain. Injection of triamcinolone into the affected greater horn can confirm the diagnosis and resolve symptoms 26. A positive response to triamcinolone injection may obviate the need for additional testing and procedures.
References- Angoules AG, Boutsikari EC. Traumatic hyoid bone fractures: rare but potentially life threatening injuries. Emerg Med. 2013;3:e128. doi: 10.4172/2165-7548.1000e128.
- Keerthi R, Quadri A. Hyoid Bone Fracture: Associated With Head and Neck Trauma-A Rare Case Report. J Maxillofac Oral Surg. 2015;15(Suppl 2):249-52. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4925585/
- Ml Bangnoli, Leban SG, Williams FA. Isolated fracture of the hyoid bone: report of a case. J Oral Maxillofac Surg. 1998;46:326–328
- Stiebler A, Maxeiner H. Nicht strangulations bedingte Kehlkopf- und Zungenbeinverletzungen. Beitr Gerichtl Med. 1990;48:309.
- Dalati T. Isolated hyoid bone fracture. Review of an unusual entity. Int J Oral Maxillofac Surg. 2005;34:449–452. doi: 10.1016/j.ijom.2004.09.004.
- Weintraub CM. Fractures of the hyoid bone. Med Leg J. 1961;29:209–216.
- Iacovou E, Nayar M, Fleming JC, Lew-Gor S. A pain in the neck: a rare case of isolated hyoid bone trauma. JSCR. 2011;7:3.
- Padgham ND. Hyperextension fracture of the hyoid bone. J Laryngol Otol. 1988;102:1062–1063. doi: 10.1017/S0022215100107285.
- Carroll B, Boulanger B, Gens D. Hyoid bone fracture secondary to gunshot. Am J Emerg Med. 1992;10:177–179. doi: 10.1016/0735-6757(92)90062-3.
- Eliachar I, Goldsher M, Gotz A, Joachimas HZ. Hyoid bone fracture with pharyngeal lacerations. J Laryngol Otol. 1980;94:331–335. doi: 10.1017/S0022215100088861
- Dalati T. Isolated hyoid bone fracture. Review of an unusual entity. Int J Oral Maxillofac Surg. 2005;34:449–452. doi: 10.1016/j.ijom.2004.09.004
- Knapik DM, Royan SJ, Salata MJ, Voos JE. Hyoid Dislocation Following Subacute Fracture in an American High School Football Athlete. Orthop J Sports Med. 2018;6(2):2325967117753594. Published 2018 Feb 12. doi:10.1177/2325967117753594 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5813857/
- Hyoid bone dislocation: a new clinical condition. White JB, Kim SW, Bielamowicz S. Otolaryngol Head Neck Surg. 2008 Aug; 139(2):318-9.
- Porr J, Laframboise M, Kazemi M. Traumatic hyoid bone fracture—a case report and review of the literature. J Can Chiropr Assoc. 2012;56(4):269–274.
- Cutuk A, Bissell B, Schmidt P, et al. Isolated hyoid bone fractures in collegiate football players: a case series and review of the literature. Sports Health. 2012;4(1):51–56.
- Ramchand T, Choudhry OJ, Shukla PA, Tomovic S, Kuperan AB, Eloy JA. Management of hyoid bone fractures: a systematic review. Otolaryngol Head Neck Surg. 2012;147(2):204–208.
- Szeremeta W, Morovati SS. Isolated hyoid bone fracture: a case report and review of the literature. J Trauma. 1991;31(2):268–271.
- David S, Corrigan AM. Fracture of the hyoid bone presenting as a dislocated mandible. Dentomaxillofac Radiol. 1989;18(2):89–90.
- Lakhia TS, Shah RB, Kapoor L. Fracture of the hyoid bone. J Laryngol Otol. 1991;105(3):232–234.
- Kaufman HJ, Ciraulo DL, Burns RP. Traumatic fracture of the hyoid bone: three case presentations of cardiorespiratory compromise secondary to missed diagnosis. Am Surg. 1999;65(9):877–880.
- Porr J, Laframboise M, Kazemi M. Traumatic hyoid bone fracture—a case report and review of the literature. J Can Chiropr Assoc. 2012;56(4):269–274
- Dickenson AJ. Fracture of the hyoid bone following minimal trauma. Injury. 1991;22(5):420–421.
- Lim, R. Y. (1982). The Hyoid Bone Syndrome. Otolaryngology–Head and Neck Surgery, 90(2), 198–200. https://doi.org/10.1177/019459988209000211
- Yoshimitsu Saito, Yasuhiro Miyamoto, Aibi Akashi, Masatoshi Akutsu, Satoko Fujita, Koushi Mikami, Shigeru Kasugai, Manabu Nakamura, Yoshihiro Akazawa, Yuichiro Yaguchi, Shoji Watanabe, Izumi Koizuka, Two Cases of Hyoid Bone Syndrome, Practica oto-rhino-laryngologica. Suppl., 2016, Volume 147, Pages 50-51, Released November 25, 2016, https://www.jstage.jst.go.jp/article/jibirinsuppl/147/0/147_50/_article
- Hyoid bone syndrome and its treatment with nonsteroidal anti-inflammatory drugs. Hyoid bone syndrome and its treatment with nonsteroidal anti-inflammatory drugs. https://www.ncbi.nlm.nih.gov/pubmed/9758176
- Stern, N., Jackson-Menaldi, C., & Rubin, A. D. (2013). Hyoid Bone Syndrome: A Retrospective Review of 84 Patients Treated with Triamcinolone Acetonide Injections. Annals of Otology, Rhinology & Laryngology, 122(3), 159–162. https://doi.org/10.1177/000348941312200303





{kind=link}