
What is LEOPARD syndrome
LEOPARD syndrome is now called Noonan syndrome with multiple lentigines, is a rare inherited disorder characterized by abnormalities of the skin, the structure and function of the heart, the inner ears, the head and facial (craniofacial) area, and/or the genitalia 1. In individuals with LEOPARD syndrome, the range and severity of symptoms and physical characteristics may vary from person to person.
LEOPARD syndrome (Noonan syndrome with multiple lentigines) is thought to be a rare condition; approximately 200 cases have been reported worldwide.
The acronym LEOPARD describes the features of the LEOPARD syndrome:
- (L)entigines – multiple black or dark brown spots on the skin
- (E)lectrocardiographic conduction defects – abnormalities of the electrical activity and the coordination of proper contractions of the heart
- (O)cular hypertelorism – widely spaced eyes
- (P)ulmonary stenosis – obstruction of the normal outflow of blood from the right ventricle of the heart
- (A)bnormalities of the genitals
- (R)etarded (slowed) growth resulting in short stature
- (D)eafness or hearing loss due to malfunction of the inner ear (sensorineural deafness)
- Some affected individuals may also exhibit mild intellectual disability, speech difficulties, and/or, in some cases, additional physical abnormalities.
LEOPARD syndrome (Noonan syndrome with multiple lentigines) is one of a group of related conditions collectively known as RASopathies. These conditions all have similar signs and symptoms and are caused by changes in the same cell signaling pathway. In addition to LEOPARD syndrome (Noonan syndrome with multiple lentigines), the RASopathies include Noonan syndrome, cardiofaciocutaneous syndrome, Costello syndrome, neurofibromatosis type 1, and Legius syndrome.
The term RASopathies includes disorders with mutations in the genes that code for the proteins of the RAS/MAPK pathway, such as neurofibromatosis type 1, Noonan syndrome, Legius syndrome, LEOPARD syndrome, Costello syndrome, and cardiofaciocutaneous syndrome 2. Molecular studies have proven that LEOPARD syndrome and Noonan syndrome are allelic disorders caused by different missense mutations in PTPN11, a gene encoding the protein tyrosine phosphatase SHP-2 located at band 12q24.1 3. SHP2 mutations seem to facilitate melanin synthesis in melanocytes 4. Variation in SHP2 catalytic activity may have important clinical implications 5.
As the condition name suggests, LEOPARD syndrome or Noonan syndrome with multiple lentigines is very similar to a condition called Noonan syndrome, and it can be difficult to tell the two disorders apart in early childhood 6. However, the features of these two conditions differ later in life. The characteristic features of LEOPARD syndrome (Noonan syndrome with multiple lentigines) include brown skin spots called lentigines that are similar to freckles, heart defects, widely spaced eyes (ocular hypertelorism), a sunken chest (pectus excavatum) or protruding chest (pectus carinatum), and short stature. These features vary, however, even among affected individuals in the same family. Not all individuals with LEOPARD syndrome (Noonan syndrome with multiple lentigines) have all the characteristic features of this condition.
The lentigines seen in LEOPARD syndrome (Noonan syndrome with multiple lentigines) typically first appear in mid-childhood, mostly on the face, neck, and upper body. Affected individuals may have thousands of small dark brown skin spots by the time they reach puberty. Unlike freckles, the appearance of lentigines has nothing to do with sun exposure. In addition to lentigines, people with this condition may have lighter brown skin spots called café-au-lait spots. Café-au-lait spots tend to develop before the lentigines, appearing within the first year of life in most affected people.
Of the people with LEOPARD syndrome (Noonan syndrome with multiple lentigines) who have heart defects, about 80 percent have hypertrophic cardiomyopathy, which is a thickening of the heart muscle that forces the heart to work harder to pump blood. The hypertrophic cardiomyopathy most often affects the lower left chamber of the heart (the left ventricle). Up to 20 percent of people with LEOPARD syndrome (Noonan syndrome with multiple lentigines) who have heart problems have a narrowing of the artery from the heart to the lungs (pulmonary stenosis).
People with LEOPARD syndrome (Noonan syndrome with multiple lentigines) can have a distinctive facial appearance. In addition to ocular hypertelorism, affected individuals may have droopy eyelids (ptosis), thick lips, and low-set ears. Affected individuals also usually have an abnormal appearance of the chest; they either have pectus excavatum or pectus carinatum.
At birth, people with LEOPARD syndrome (Noonan syndrome with multiple lentigines) are typically of normal weight and height, but in some, growth slows over time. This slow growth results in affected individuals being shorter than average, although less than half of people with LEOPARD syndrome (Noonan syndrome with multiple lentigines) have significantly short stature.
Other signs and symptoms of LEOPARD syndrome (Noonan syndrome with multiple lentigines) include hearing loss caused by abnormalities in the inner ear (sensorineural deafness), mild intellectual disability, and extra folds of skin on the back of the neck. Affected males often have genital abnormalities, which can include undescended testes (cryptorchidism) and a urethra that opens on the underside of the penis (hypospadias). These abnormalities may reduce the ability to have biological children (decreased fertility). Females with LEOPARD syndrome (Noonan syndrome with multiple lentigines) may have poorly developed ovaries and delayed puberty.
LEOPARD syndrome is inherited in an autosomal dominant genetic disorder. LEOPARD syndrome can be inherited from an affected parent, or it can be due to a new mutation in a person with no family history of the condition. LEOPARD syndrome and Noonan syndrome are both caused by mutations in the PTPN11 and RAF1 genes.
There are 3 types of LEOPARD syndrome, which are distinguished by their genetic cause. Type 1 is caused by mutations in the PTPN11 gene; type 2 is caused by mutations in the RAF1 gene; and type 3 is caused by mutations in the BRAF gene. Other cases are caused by mutations in the MAP2K1 gene, and in some cases the cause is unknown.
Figure 1. LEOPARD syndrome

Footnote: Skin features of LEOPARD syndrome individual at different ages. (A) Numerous lentigines in the upper part of the trunk in a 2 year old child with a PTPN11 gene mutation. (B) Lentigines and a large cafè-au-lait spot (28 year-old female patient). (C) A 28 year old female patient with thousands of lentigines scattered all over the neck and back. Note the pterigium colli. (D) Multiple lentigines on the lower leg (37 year-old male patient).
[Source 7 ]LEOPARD syndrome causes
Mutations in one of several genes can cause LEOPARD syndrome (Noonan syndrome with multiple lentigines). Approximately 85 percent of individuals with LEOPARD syndrome have mutations in the PTPN11 gene. Another 10 percent have mutations in the RAF1 gene. In rare cases, mutations in the BRAF or MAP2K1 gene have been found to cause LEOPARD syndrome. Mutations in these genes also cause a different genetic condition called Noonan syndrome. The remaining individuals with LEOPARD syndrome (Noonan syndrome with multiple lentigines) do not have an identified mutation in any of these four genes. In these individuals, the cause of the condition is unknown.
The PTPN11, RAF1, BRAF, and MAP2K1 genes all provide instructions for making proteins that are involved in important signaling pathways needed for the proper formation of several types of tissue during development. These proteins also play roles in the regulation of cell division, cell movement (migration), and cell differentiation (the process by which cells mature to carry out specific functions).
A mutation in the PTPN11, RAF1, BRAF, or MAP2K1 gene leads to the production of a protein that functions abnormally, which impairs the protein’s ability to respond to cell signals. A disruption in the regulation of systems that control cell growth and division leads to the characteristic features of LEOPARD syndrome (Noonan syndrome with multiple lentigines).
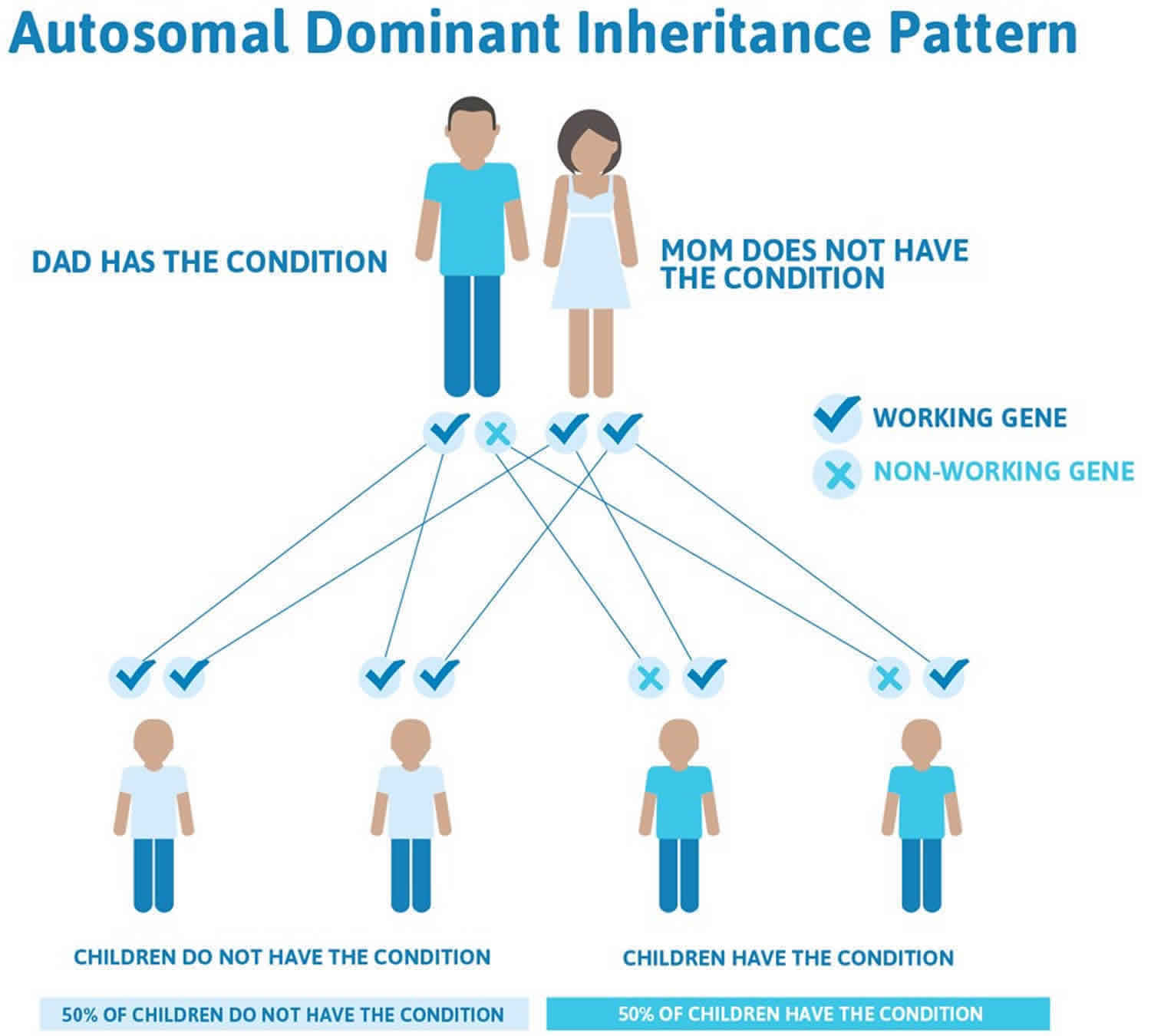
LEOPARD syndrome inheritance pattern
LEOPARD syndrome (Noonan syndrome with multiple lentigines) is inherited in an autosomal dominant pattern, which means one copy of the altered gene in each cell is sufficient to cause the disorder.
Often autosomal dominant conditions can be seen in multiple generations within the family. If one looks back through their family history they notice their mother, grandfather, aunt/uncle, etc., all had the same condition. In cases where the autosomal dominant condition does run in the family, the chance for an affected person to have a child with the same condition is 50% regardless of whether it is a boy or a girl. These possible outcomes occur randomly. The chance remains the same in every pregnancy and is the same for boys and girls.
- When one parent has the abnormal gene, they will pass on either their normal gene or their abnormal gene to their child. Each of their children therefore has a 50% (1 in 2) chance of inheriting the changed gene and being affected by the condition.
- There is also a 50% (1 in 2) chance that a child will inherit the normal copy of the gene. If this happens the child will not be affected by the disorder and cannot pass it on to any of his or her children.
There are cases of autosomal dominant gene changes, or mutations, where no one in the family has it before and it appears to be a new thing in the family. This is called a de novo mutation. For the individual with the condition, the chance of their children inheriting it will be 50%. However, other family members are generally not likely to be at increased risk.
Figure 1 illustrates autosomal dominant inheritance. The example below shows what happens when dad has the condition, but the chances of having a child with the condition would be the same if mom had the condition.
Figure 2. LEOPARD syndrome autosomal dominant inheritance pattern
People with specific questions about genetic risks or genetic testing for themselves or family members should speak with a genetics professional.
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://www.findageneticcounselor.com/) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://www.abgc.net/about-genetic-counseling/find-a-certified-counselor/) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counselors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (http://www.acmg.net/ACMG/Genetic_Services_Directory_Search.aspx) has a searchable database of medical genetics clinic services in the United States.
LEOPARD syndrome symptoms
The symptoms and physical characteristics associated with LEOPARD syndrome (Noonan syndrome with multiple lentigines) are highly variable. However, most affected individuals tend to exhibit characteristic abnormalities of the skin, the structure and function of the heart, the head and facial (craniofacial) area, and/or the genitals.
The clinical features of LEOPARD syndrome (Noonan syndrome with multiple lentigines) vary considerably between patients, with most only manifesting 3–5 abnormalities. Lentigines are the most common feature of the syndrome and occur in more than 90% of patients. However, they do not have to be present to diagnose the syndrome.
The lentigines are small, dark pigmented flat or slightly raised lesions with well defined borders.
- Often 2–5 mm in diameter, some lentigines may grow to 1–1.5 cm in size.
- They are an irregular round or oval shape.
- Unlike freckles, these spots are not affected by sun exposure.
- They are often found on the face, neck, and upper part of the trunk but also on the palms, soles, and the sclerae (whites) of the eyes.
Other skin abnormalities include:
- Freckling around the armpit region
- Café au lait macules (coffee-coloured flat macules)
- Localised hypopigmentation (lightening of skin colour)
- Onychodystrophy (malformation of the nails)
- Interdigital webs (webbing between the fingers)
- Hyperelastic skin (stretchy skin)
Non-cutaneous features of LEOPARD syndrome (Noonan syndrome with multiple lentigines) include:
- Hearing loss in about 25% of patients
- Short stature in about 1/3 of patients
- Mild degree of mental retardation in about 30% of patients
- Craniofacial abnormalities (eg, low set ears, abnormal shaped skull, dental abnormalities)
- Abnormalities of the genitals in about 26% of patients, mainly in men
- Heart abnormalities, often without symptoms
Children with LEOPARD syndrome (Noonan syndrome with multiple lentigines) may exhibit numerous black or dark brown “freckle-like” spots on the skin (multiple lentigines). However, most individuals with LEOPARD syndrome (Noonan syndrome with multiple lentigines) do not exhibit lentigines during the first few years of life. Lentigines increase in number with age, usually until puberty. Many affected individuals may exhibit thousands of such lentigines. Although these small, flat discolorations (macules) resemble freckles, they tend to be darker, range from approximately one to five millimeters (mm) in size, and do not darken upon exposure to sunlight. The lentigines tend to be most numerous on the neck and upper chest area (trunk), be less concentrated below the knees, and involve only the skin, not the mucous membranes. However, they may appear anywhere on the skin of the body including the scalp, face, upper arms and/or upper legs, palms of the hands, soles of the feet, and/or genitals. In approximately 20 percent of affected individuals, larger, dark brown discolorations (café-au-lait spots) may also appear on the skin.
Many individuals with LEOPARD syndrome (Noonan syndrome with multiple lentigines) also have cardiac anomalies. Such heart defects, which are often apparent during infancy or early childhood, may include the abnormal transmission of electrical impulses that coordinate contractions of the heart (electrocardiographic conduction defects). In many cases of LEOPARD syndrome (Noonan syndrome with multiple lentigines), there may be an interruption of the normal passage of electrical impulses (heart block) through the heart’s conducting system. As a result, although the two upper chambers of the heart (atria) may beat normally, the two lower chambers (ventricles) may contract less often or “fall behind” the atria.
The effects of such electrocardiographic conduction defects in individuals with LEOPARD syndrome (Noonan syndrome with multiple lentigines) may be highly variable, ranging from no apparent symptoms (asymptomatic) in some affected individuals to potentially serious complications in others. For example, those who exhibit prolonged P-R intervals may not exhibit any associated symptoms. Observable symptoms may also not occur in affected individuals who experience dropped beats. In more severe cases of heart block, however, if there is inadequate blood output from the ventricles, affected individuals may experience breathlessness due to the heart’s inability to pump blood effectively (heart failure), fatigue, or experience fainting episodes. If the ventricular beat slows dramatically or stops, affected individuals may black out, experience seizures, or exhibit life-threatening symptoms.
In addition, individuals with LEOPARD syndrome (Noonan syndrome with multiple lentigines) may also have structural (anatomical) malformations of the heart. The most common cardiac malformation appears to be overgrowth (hypertrophy) of the cardiac muscle in the ventricular wall(s) (hypertrophic obstructive cardiomyopathy), particularly the left ventricle. This condition may cause reduced cardiac output, potentially resulting in fatigue; fainting episodes (syncope), particularly during physical activity; and/or, in some cases, potentially life-threatening symptoms (e.g., arrhythmias, etc.)
The second most common abnormality is the obstruction of the normal outflow of blood from the lower right chamber (ventricle) of the heart to the lungs (isolated valvar pulmonary stenosis). Such obstruction may be due to abnormal narrowing (stenosis) of the pulmonary artery, which carries blood from the right ventricle to the lungs; stenosis of the pulmonary valve, the valve that controls the regular flow of deoxygenated blood through the pulmonary artery and on to the lungs; abnormal narrowing of the upper portion of the right ventricle; and/or other causes. In individuals with pulmonary stenosis, the heart must work harder to send blood to the lungs for oxygenation.
In most individuals with LEOPARD syndrome (Noonan syndrome with multiple lentigines), pulmonary stenosis tends to be mild and symptoms may not occur (asymptomatic). In those cases when symptoms do occur, they often may not appear until later in childhood.
In some people, hypertrophic cardiomyopathy and pulmonary stenosis may be associated.
Some affected individuals with pulmonary stenosis may also exhibit abnormal narrowing (stenosis) of the aorta, the main artery of the body. Aortic stenosis may result in obstruction of blood flow from the left ventricle to the aorta and abnormal thickening of cardiac muscle in the wall of the left ventricle. As a result, aortic stenosis may contribute to such symptoms as fatigue, chest pain (angina pectoris) during exertion, breathlessness, and/or fainting episodes.
Many individuals with LEOPARD syndrome (Noonan syndrome with multiple lentigines) exhibit widely spaced eyes (ocular hypertelorism), with or without additional malformations of the head and facial (craniofacial) area. These may include a triangular-shaped face, drooping of the upper eyelids (ptosis), the presence of abnormal folds of skin over the inner corners of the eye (epicanthal folds), abnormal protrusion of the lower jaw (mandibular prognathism), and/or low-set, unusually prominent ears. Some affected individuals may also exhibit additional abnormalities including crossing of the eyes (strabismus) and/or mild webbing of the neck (pterygium colli).
Many individuals with LEOPARD syndrome (Noonan syndrome with multiple lentigines) also have genital abnormalities. Affected males may exhibit abnormal placement of the urinary opening (meatus) on the underside of the penis (hypospadias), unusual smallness of the penis (micropenis), and/or failure of one or both testes to descend into the scrotum (unilateral or bilateral cryptorchidism). Affected females may exhibit underdevelopment (hypoplasia) or absence (agenesis) of an ovary. Abnormally decreased function of the gonads (i.e., testes in males, ovaries in females) may result in delayed development of secondary sexual characteristics (puberty) in some affected males and females.
Individuals with LEOPARD syndrome (Noonan syndrome with multiple lentigines) may also exhibit growth retardation that results in short stature. Affected individuals may also have additional skeletal abnormalities. These may include malformations of the chest (thoracic deformity) such as abnormal depression of the bone forming the center of the chest (sternum), known as “funnel chest” or pectus excavatum, or abnormal protrusion of the sternum, known as “keeled chest” or pectus carinatum. Some individuals with LEOPARD syndrome (Noonan syndrome with multiple lentigines) may exhibit additional skeletal abnormalities such as unusually prominent shoulder blades (winged scapula), abnormal sideways curvature of the spine (scoliosis), and/or the development of abnormal front-to-back spinal curvature (kyphosis) during later life.
Some individuals with LEOPARD syndrome (Noonan syndrome with multiple lentigines) may also exhibit mild to severe hearing loss due to malfunction of the inner ears (sensorineural deafness). In some people, such hearing loss may be apparent at birth or during early childhood. However, other affected individuals may have normal hearing in early childhood yet eventually exhibit hearing loss at a later age. Hearing impairment may contribute to speech difficulties in many people. Although most affected individuals have normal intelligence, others may exhibit mild intellectual disability.
LEOPARD syndrome diagnosis
LEOPARD syndrome (Noonan syndrome with multiple lentigines) diagnosis based on clinical features. LEOPARD syndrome (Noonan syndrome with multiple lentigines) should be suspected in patients who demonstrate one or more of the following cardinal features:
- Lentigines
- Cardiac abnormalities
- Short stature
- Pectus deformity
- Facial dysmorphia.
Proposed minimum criteria are:
- The presence of multiple lentigines, plus 2 other cardinal features
- If lentigines are absent, a first degree relative with a diagnosis of LEOPARD syndrome (Noonan syndrome with multiple lentigines) plus 3 of the cardinal features.
Diagnosis may be based on molecular genetic testing. Single gene or multi-gene panels can be used to identify mutations.
In some children, the diagnosis of LEOPARD syndrome (Noonan syndrome with multiple lentigines) may be suspected soon after birth due to the presence of pale tan or light brown discolorations on the skin (café-au-lait spots), characteristic facial features and hypertrophic cardiomyopathy. Multiple lentigines are usually not apparent before the age of five years. When they are seen in combination with two other related features in the LEOPARD acronym or when an individual has three related features plus a parent or sibling with multiple lentigines, the diagnosis of LEOPARD syndrome (Noonan syndrome with multiple lentigines) can be made.
Molecular genetic testing for the PTPN11 gene and the RAF1 gene is available to confirm the diagnosis and for prenatal diagnosis.
The diagnosis of certain specific abnormalities that may occur in association with LEOPARD syndrome (Noonan syndrome with multiple lentigines) may be confirmed by specialized imaging studies and/or additional tests. Examination of skin samples (biopsies) under a microscope that uses light (light microscopy) or an electron beam (electron microscopy) may confirm that pigmented areas of skin represent multiple lentigines as opposed to freckles.
Children who exhibit multiple lentigines should receive prompt, thorough cardiac evaluation. If no cardiac abnormalities are revealed during such evaluation, individuals should receive periodic reassessments to detect any heart abnormalities that may develop later.
A variety of tests may be conducted to perform such a cardiac assessment. For example, the electrocardiographic conduction defects (e.g., varying degrees of heart block) and/or structural (anatomical) malformations of the heart (e.g., pulmonary and/or aortic stenosis, hypertrophic obstructive cardiomyopathy) may be confirmed by a thorough clinical examination and several specialized tests that allow physicians to evaluate the structure and function of the heart.
Clinical examination may include a physician’s evaluation of heart and lung sounds through use of a stethoscope. For example, in mild asymptomatic cases of pulmonary stenosis, the condition may initially be suspected through the detection of an abnormal heart murmur during such stethoscopic evaluation. Heart block may initially be identified by detection of a slow, regular heartbeat that fails to increase during exercise.
Specialized cardiac tests may include electrocardiography (EKG), echocardiography, cardiac MRI and/or cardiac catheterization. An EKG, which records the electrical activities of the heart muscle, may confirm the presence of abnormal electrical patterns such as those associated with varying degrees of heart block (e.g., prolonged P-R interval, left anterior hemiblock, widening of the QRS complex, complete heart block). During an echocardiogram, sound waves are directed toward the heart, enabling physicians to study cardiac function and motion. Echocardiography may play an essential role in helping to confirm hypertrophic obstructive cardiomyopathy. EKG, echocardiograms, cardiac catheterization, and/or other tests may help to clarify the underlying anatomical cause and/or severity of narrowing associated with pulmonary stenosis.
Sonographic and radiological techniques may be conducted to detect and/or confirm certain genital abnormalities in many individuals with LEOPARD syndrome (Noonan syndrome with multiple lentigines) (e.g., unilateral or bilateral cryptorchidism in affected males, hypoplastic ovaries in affected females). In addition, because deficiencies of certain hormones (gonadotrophin) may contribute to abnormally decreased function of the gonads (hypogonadism) and delayed puberty in some affected males and females, individuals with LEOPARD syndrome (Noonan syndrome with multiple lentigines) may be monitored closely to promptly detect such delays and laboratory tests may be conducted to screen for deficient levels of certain gonadotrophins in the blood.
In many individuals with LEOPARD syndrome (Noonan syndrome with multiple lentigines), X-ray studies may also be used to confirm the presence of certain skeletal abnormalities suspected during clinical observation. Growth retardation may not become obvious until early childhood, when there may be an observable decline in the normal growth rate.
Thorough, regular hearing (audiological) evaluation should also be conducted in individuals with LEOPARD syndrome (Noonan syndrome with multiple lentigines) to promptly detect potential hearing impairment and help ensure early implementation of appropriate supportive measures. If hearing impairment is detected, a scanning procedure, such as computerized tomography or CT scan, may be performed to confirm the underlying cause (e.g., inner ear malformation) and characterize the type of hearing loss (e.g., sensorineural hearing impairment). During a CT scan, a computer and x-rays are used to create a film showing cross-sectional images of the structures of the inner ear.
LEOPARD syndrome treatment
A team of specialist doctors including a cardiologist, endocrinologist, orthopedist and dermatologist should manage LEOPARD syndrome (Noonan syndrome with multiple lentigines). The treatment of LEOPARD syndrome (Noonan syndrome with multiple lentigines) is directed toward the specific symptoms that are apparent in each individual. Pediatricians, surgeons, physicians who diagnose and treat disorders of the skin (dermatologists), cardiologists, specialists who diagnose and treat skeletal disorders (orthopedists), physicians who specialize in diagnosing and treating disorders of the glands (endocrinologists), specialists who assess and treat hearing problems (audiologists), speech pathologists, and/or other health care professionals may need to systematically and comprehensively plan an affected child’s treatment.
Specific therapies for LEOPARD syndrome (Noonan syndrome with multiple lentigines) are symptomatic and supportive. Isolated lentigines can be removed through the use of chemical peels, cryotherapy, laser treatments or surgical excision. For some patients, treatment with topical retinoids and hydroquinone cream may be helpful. In affected individuals who exhibit mild forms of cardiac conduction abnormalities, treatment may not be required. However, in more severe cases when associated symptoms occur (e.g., fainting episodes) and in some cases of pulmonary stenosis, hypertrophic obstructive cardiomyopathy, and/or other structural heart abnormalities potentially associated with LEOPARD syndrome (Noonan syndrome with multiple lentigines), treatment with certain medications, surgical intervention, and/or other techniques may be necessary. The surgical procedures performed will depend upon the location and severity of the anatomical abnormalities and their associated symptoms.
Other abnormalities potentially associated with LEOPARD syndrome (Noonan syndrome with multiple lentigines) may also be corrected surgically. These may include certain craniofacial, skeletal, genital, and/or other malformations. For example, in some affected males with cryptorchidism, hormone treatment may be administered; however, if this treatment is not successful, surgery may be performed to move the undescended testes into the scrotum and attach them in a fixed position to prevent retraction (orchiopexy).
In addition, if laboratory and additional tests demonstrate that deficient levels of gonadotrophin (hypogonadotropism) have contributed to abnormally decreased gonadal function (hypogonadism) and delayed puberty in affected males or females, sex hormone replacement therapy may be considered in some cases.
If individuals with LEOPARD syndrome (Noonan syndrome with multiple lentigines) demonstrate hearing impairment, hearing aids may be beneficial. Appropriate use of hearing aids, other supportive techniques, and speech therapy may help to prevent, improve, and/or correct some speech problems that may result from such hearing impairment.
Early intervention is important to ensure that children with LEOPARD syndrome (Noonan syndrome with multiple lentigines) reach their potential. Special services that may be beneficial to affected children include special remedial education, special social support, physical therapy, and/or other medical, social, and/or vocational services.
Genetic counseling is recommended for individuals with LEOPARD syndrome (Noonan syndrome with multiple lentigines) and their families.
LEOPARD syndrome prognosis
Prognosis is determined mainly by cardiac complications. Most patients with LEOPARD syndrome lead a normal life. Cardiac pathologic findings (eg, obstructive cardiomyopathy, cardiac dysrhythmias) may be a cause of death in selected patients. A 19-year-old woman who died as a result of respiratory insufficiency secondary to thoracic deformities and a congenital heart defect has been reported.
References- Noonan Syndrome with Multiple Lentigines. https://rarediseases.org/rare-diseases/leopard-syndrome
- Duat-Rodriguez A, Hernandez-Martin A. [Update on the treatment of RASopathies]. Rev Neurol. 2017 May 17. 64 (s03):S13-S17.
- Kim J, Kim MR, Kim HJ, Lee KA, Lee MG. LEOPARD Syndrome with PTPN11 Gene Mutation Showing Six Cardinal Symptoms of LEOPARD. Ann Dermatol. 2011 May. 23(2):232-5.
- Motegi SI, Yokoyama Y, Ogino S, Yamada K, Uchiyama A, Takeuchi Y, et al. Pathogenesis of Multiple Lentigines in LEOPARD Syndrome with PTPN11 Gene Mutation. Acta Derm Venereol. 2015 Apr 28.
- Noda S, Takahashi A, Hayashi T, Tanuma S, Hatakeyama M. Determination of the catalytic activity of LEOPARD syndrome-associated SHP2 mutants toward parafibromin, a bona fide SHP2 substrate involved in Wnt signaling. Biochem Biophys Res Commun. 2016 Jan 22. 469 (4):1133-9.
- Noonan syndrome with multiple lentigines. https://ghr.nlm.nih.gov/condition/noonan-syndrome-with-multiple-lentigines
- Leopard syndrome. Orphanet Journal of Rare Diseasesvolume 3, Article number: 13 (2008) https://ojrd.biomedcentral.com/track/pdf/10.1186/1750-1172-3-13





{kind=link}