
What is liposuction
Liposuction also known as lipectomy or lipoplasty, is a cosmetic surgery procedure which involves the removal of excess body fat from under your skin from various parts of your body using a cannula and a suction device. Liposuction is a type of cosmetic surgery that some people consider to improve how they feel about the way they look. Liposuction is not a weight loss method. Liposuction is the most popular cosmetic surgery performed worldwide and is usually done to improve the appearance of distorted body shapes and remove pockets of fat that are difficult to eliminate with diet and exercise, in order to slim and reshape specific areas of your body. Liposuction is also known as body contouring as it can be used to contour the chin, neck, cheeks, ankles, calves, and breasts. Liposuction is most commonly used for the thighs, buttocks, abdomen, arms, neck and under the chin, but it is also used for the back, inner knee, chest, cheek, calves and ankles.
Liposuction is an invasive surgery that aims to improve your body’s contours and proportion by removing localized and disproportional deposits of fat. Liposuction can remove up to 5 liters of fat with relative safety during one session. Depending on the number of areas that require treatment, repeated treatments may be necessary.
In some cases, liposuction is performed alone, in other cases it is used with plastic surgery procedures such as a facelift, breast reduction or a tummy tuck.
There are a number of liposuction techniques that may be used depending on the site and how much fat is to be removed. Specific techniques of liposuction include:
- Tumescent liposuction: Tumescent liposuction is the most common type of liposuction. It involves injecting a large amount of fluid (3-4 times the volume of the fat being removed) made up of a salt solution (saline) containing a mix of local anesthetic and epinephrine (adrenaline) into the areas before the fat is removed. The anesthetic numbs the area and the purpose of the epinephrine is to minimize bruising, swelling and blood loss. Injection of the fluid creates space between the muscle and fatty tissue for the cannula. This form of liposuction usually takes longer than others as the fluid must be injected slowly. However it has the fastest recovery time and least amount of complications.
- Superwet liposuction: The super-wet technique is similar to tumescent liposuction except that not as much fluid is used, the amount of fluid injected is about equal to the amount of fat to be removed. This technique takes less time however it usually requires sedation with general anesthesia.
- Suction Assisted Lipectomy where fat is removed from the body using a vacuum suction. Suction Assisted Lipectomy may be dry, wet or tumescent depending on the volume of saline (salt solution) which is injected into the operation site before the procedure begins
- Ultrasonic Assisted Lipoplastry: Ultrasound or ultrasonic-assisted liposuction is a fairly recent technique introduced in 1996. Ultrasonic Assisted Lipoplastry uses ultrasound or ultrasonic energy to liquefy the fat cells before Suction Assisted Lipectomy is used to remove the liquefied fat and to smooth the edges of the treated areas. Ultrasonic Assisted Lipoplastry can be done internally through the cannula which transmits ultrasound vibrations under the skin, or by external exposure. This technique may be useful in the removal of fat from dense or fibrous areas of the body such as the upper back or male breast tissue. Ultrasonic Assisted Lipoplastry is often used in conjunction with the tumescent technique or in follow-up procedures. Little benefit is achieved from this procedure and it has been associated with cutaneous burns and higher risk of seroma formation.
- Mechanical Assisted Lipoplasty uses an oscillating shaver driven by a motor to shave the fat which is vacuumed away as used in the Suction Assisted Lipectomy and Ultrasonic Assisted Lipoplastry methods.
- Power assisted liposuction: Power-assisted liposuction is a new technology which utilizes a motor-driven, reciprocating cannula attached to a standard aspirator. This reduces the workload on the surgeon as it limits the physical movements that must be made. In addition, it allows the surgeon to remove fat more completely in tight areas where forceful cannula movements are difficult because of physical space constraints. This new technology has been shown to have significant benefits over traditional cannulas.
- Laser assisted liposuction: The newest liposuction technique is Laser-assisted liposuction which works by focusing low energy waves from a laser onto the parts of the body that require treatment. This causes the fat cells to weaken and burst. Like Ultrasonic Assisted Lipoplastry this technique can be used in conjunction to other liposuction procedures. This technique has the advantage of producing much less swelling and bruising and hence a faster recovery time.
Liposuction techniques may be used to reduce localized fat deposits of the:
- Thighs
- Hips and buttocks
- Abdomen and waist
- Upper arms
- Back
- Inner knee
- Chest area
- Cheeks, chin and neck
- Calves and ankles
Some people choose only to have liposuction, whereas other people have it at the same time as other cosmetic surgery procedures such as a facelift, a breast augmentation or a tummy tuck (an abdominoplasty).
You can find Board Certified Plastic Surgeons here:
- American Society for Aesthetic Plastic Surgeon (https://www.surgery.org/consumers/find-a-plastic-surgeon)
- American Society of Plastic Surgeons (https://find.plasticsurgery.org/)
Current liposuction devices
Traditional suction-assisted lipectomy
During the late 1970s and early 1980s, a number of surgeons were concurrently contributing to the technique and technology that later became traditional liposuction. Until that time, surgeons were using sharp curettes, which led to several unwanted complications, including excess bleeding, contour irregularities, lack of overlying skin contraction, seroma formation, and even frank skin necrosis. In 1977, brothers Arpad and George Fisher were the first surgeons to describe adding suction to assist the process of fat extraction 1. The Fisher brothers utilized a sharp instrument connected to a suction device, which led to increased efficiency of fat removal; however, the complication rate remained high. Therefore, the technique was not widely adopted.
Similar to Teimourian, the contributions of Ulrich Kesselring were rooted more in technical refinements, which clearly led to the appreciation for the need for better technology. Kesselring used sharp instruments attached to a suction-generating device; however, he introduced the instruments in the deep fat layer immediately superficial to muscle fascia. Furthermore, his selection of young, healthy women with minimal to no loss of skin elasticity contributed significantly to improved surgical outcomes, helping renew interest in liposuction benefits 2.
Yves-Gerard Illouz (Paris, France) is often credited with the major technological advances to liposuction instruments. A known collaborator/colleague of Kesselring, Illouz’s modification of the sharp curette to a blunt-tip cannula was spawned from the observation of a high complication rate due to collateral tissue laceration and damage. The blunt cannula was increasingly easy to navigate through tissue and remove fat while still maintaining the integrity of adjacent soft tissue structures 3. Not only did adopting the blunt cannula technology lead to an overall decrease in complication rate, but further allowed a standardized safer technique for surgeons with varying levels of experience to adopt. Small access incisions were made in the skin, and the blunt cannula was introduced through these incisions to aspirate fat in the deep subcutaneous layer. Cannulas with different curves, lengths, and diameters were manufactured. The cannulas had two basic design features consisting of a blunt end with a round tip and a lateral opening that one was to always direct away from the skin surface in order to avoid the creation of irregular skin contour. There was a notched area on the cannula to help the surgeon orient positioning of the opening. A 10 mm cannula was used for large fatty deposits, and an 8 mm cannula was used for the knees, ankles, abdomen, and arms. Finally, a 5 mm cannula was used for the face. The cannula was connected to a suction pump by a semirigid transparent tube, which allowed for the isolated fat to be visualized as it was suctioned. The endpoint of liposuction occurred when aspirated fat changed in color from a pure yellow to bloody appearance. It was at this point, the cannula was to be inserted in a different tunnel as described by Kesselring 4. This technique continued to become refined, and the potential of liposuction as a staple of aesthetic plastic surgery was validated. Two additional French surgeons, Fournier and Otteni, introduced the utilization of syringes in place of the suction machine as the source of negative pressure connected to a non–cutting edge cannulae 5. Over the years, the cannula length changed, and inner diameters were made smaller. It is therefore rare to use a cannula greater than 5 mm (diameter) on the body and 2.4 mm (diameter) on the face. In addition, cannula design has changed to have several openings to optimize fat extraction.
Ultrasound-assisted liposuction
Ultrasound-assisted liposuction is a form of liposculpting, which employs ultrasonic energy to allow for a more selective tissue lipolysis. Zocchi10 initially described the technique, where he utilized a two-stage process of selective tissue lipolysis using an ultrasonic probe followed by traditional suction-assisted lipectomy to evacuate the fat. The selective adipose lipolysis seen in ultrasound-assisted liposuction can be attributed to the transformation of electrical into mechanical energy via an ultrasonic probe that vibrates at frequencies in excess of 16 kHz. This oscillating sound wave produces a negative pressure vector that overcomes molecular forces selectively within adipose tissue leading to cavitation and cellular fragmentation 6. The large-scale cellular disruption is later aspirated in a second stage liposuction. Rohrich et al 7 confirmed that ultrasound-assisted liposuction generates significantly higher levels of several intracellular adipocyte enzymes than suction-assisted lipectomy, confirming the notion that adipocytes are mechanically lysed in larger amounts. One of the reported benefits of ultrasound-assisted liposuction over other forms of energy- and thermal-assisted suction-assisted lipoplasty is caviation formation of the air bubbled in the tumescent fluid. This process results in a “crow bar” effect of streaming intact fat cells and adipocyte-derived stem cells so that these can then be used for successful fat grafting.
Supporters of ultrasound-assisted liposuction claim that adipocyte cavitation prior to suction-assisted lipectomy decreases blood loss and operative time while providing for less ecchymosis and discomfort as well as improved contouring in areas with an abundance of fibrous tissue, such as the back and chest 8. While the evidence to substantiate claims of decreased operative time and ecchymosis are mixed, several studies have confirmed that ultrasound-assisted liposuction is effective in cases of secondary liposuction as well as liposuction in fibrotic areas such as the male flank or chest area 9. Beckenstein and Grotting demonstrated that ultrasound-assisted liposuction was effective in 70% of secondary liposculpting cases 9. Additionally, Fodor and Watson 10 directly compared ultrasound-assisted liposuction with suction-assisted lipectomy and supported ultrasound-assisted liposuction’s superiority in sculpting fibrotic areas when compared with suction-assisted lipectomy. Finally, contemporary, third-generation ultrasound-assisted liposuction devices such as VASER™ (Solta Medical, Hayward, CA, USA), allow for greater fragmentation of adipocytes at a lower energy setting, using pulsed rather than continuous energy 11.
Critics of ultrasound-assisted liposuction claim that the technology is expensive, requires larger incisions, and carries the risk of thermal burns 12. While ultrasound-assisted liposuction remains promoted by some authors, the reported use and market share appears to be in decline 13, likely due to a combination of the aforementioned factors and the advent of newer technologies with safer side-effect profiles and decreased learning curves 14.
Power-assisted liposuction
Further advances in technology led to a device that allowed less overall decrease in operator fatigue. The emergence of power-assisted liposuction, a rapidly vibrating cannula, quickly became a mainstay in the armamentarium of plastic surgeons 15. The first such device (1998) receiving US Food and Drug Administration (FDA) approval was from MicroAire Surgical Instruments (Charlottesville, VA, USA). The indication was “for removal of tissue or fluid … including suction lipoplasty for the purpose of aesthetic body contouring.” The first-generation device was powered by medical-grade nitrogen (N2) or by compressed air tanks attached to the MicroAire handle and suction tubing. The vibrating cannula reciprocated at 2,000–4,000 cpm with a 2 mm stroke. The speed of cannula movement could be adjusted according to the surgeon’s preference. Subsequent generations became powered by a quieter electric source instead of medical-grade compressed air 16.
Advocates of power-assisted liposuction (power-assisted liposuction) find the cannula breaks up fibrous fat much more readily than does traditional suction-assisted lipectomy. Furthermore, there is less plugging/congestion of the cannula due to constant motion and vibration of the suction cannula. Many surgeons have noted the process of power-assisted liposuction to be less labor-intensive than traditional suction-assisted lipectomy. Furthermore, operative times can be decreased 17. One author (SMS) noted in the Journal of American Medical Association improved ease of using power-assisted liposuction in fibrotic fat seen in HIV (human immunodeficiency virus) retroviral medication-induced cervical lipodystrophy/buffalo hump 18.
The disadvantages of power-assisted liposuction technology routinely expressed are additional cost, learning curve, vibration transmitted to the surgeon’s upper extremity, and noise associated with the device 16.
Laser-assisted liposuction
Laser-assisted liposuction (laser-assisted liposuction) was first described in 1994 by Apfelberg et al 19. This group from California performed a preliminary investigation that used a neodymium-doped, yttrium aluminum garnet (Nd-YAG) laser within the liposuction cannula. Although initial trials sought to demonstrate superiority over conventional suction-assisted lipectomy, the FDA did not approve the technique 20. Since this initial study, several investigators have sought to utilize laser energy of different wavelengths to induce adipocyte lysis in an effort to decrease intraoperative blood loss and postoperative ecchymosis while improving cutaneous tightening.
Several laser companies are utilizing laser technology as an adjunct to liposuction. The largest market share in the United States for laser-assisted liposuction belongs to SmartLipo™ (Cynosure Inc., Westford, MA, USA). Another company with a laser platform that has expanded the technology to liposuction is Sciton (Palo Alto, CA, USA) with its ProLipo PLUS™ product. In its current fashion, laser-assisted liposuction is performed either simultaneously while performing suction-assisted lipectomy or in a two-stage procedure using laser-assisted liposuction prior to performing suction-assisted lipectomy.
Laser-assisted liposuction utilizes the principles of selective photothermolysis to preferentially lyse adipocytes while leaving surrounding structures unaffected 21. Different laser wavelengths may vary in their relative effectiveness in targeting substances present in the subcutaneous environment, including collagen, fat, vascular structures, hemoglobin, and water. Thus, lasers achieve their desired effect in laser-assisted liposuction via photolysis of adipose cells, photocoagulation of small vessels, liberation of adipocyte lipases, and contraction of dermal collagen 22.
The most commonly utilized lasers in cosmetic dermatology are the Nd:YAG 1,064 nm, 1,320 nm, 2,010 nm, 980 nm diode laser, 924 nm, and the 975 nm; however, the three major lasers evaluated for laser-assisted liposuction are the 1,064 nm Nd:YAG, the 980 nm diode, and the 1,064/1,320 nm Nd:YAG lasers 23. The 1,064 nm Nd:YAG is the most studied and has the greatest evidence for safety and tolerability. The 980 nm diode laser utilizes high power settings that provide for greater utility in dense areas containing large fat deposits, such as the thigh and abdomen. The 1,064/1,320 nm Nd:YAG demonstrates a greater selectivity for dermal collagen, with the added potential to induce skin tightening and neocollagenesis. Additionally, the 1,320 nm laser converts hemoglobin to methemoglobin, which may enhance hemostasis, making this laser ideal for highly vascular areas 23. The 1,440 nm pulsed laser has 60 times greater selective absorption of water when compared with the 1,064 nm laser, therefore leading to more efficient fat coagulation.51 Increased wavelength for larger surface areas with laser-assisted liposuction has also shown in randomized, blinded studies to result in up to 17% skin contraction and 25% improvement in skin elasticity 24. Furthermore, a superficial version of laser-assisted liposuction, using a side-light firing laser (Cellulaze; Cynosure, Westford, MA, USA) has shown significant reduction in cellulite long-term, with 25% thicker dermis on B-mode ultrasound and 29% improvement in skin elasticity 25.
The disadvantages of laser-assisted liposuction include the potential of thermal injury, high costs of equipment, and prolonged procedural time. Initial studies evaluating first-generation laser devices showed, in randomized trials, no increased cosmetic benefits of laser-assisted liposuction when compared with traditional suction-assisted lipectomy 26. The emerging laser technology utilizes varying wavelengths with different effects of the surrounding environment, leading to promising dermal physiologic changes with decreased complications 27.
Water-assisted liposuction
The concept behind Water-assisted liposuction (water-assisted liposuction) utilizes a thin, targeted, fan-shaped jet, called Body-Jet™ (Human Med, Schwerin, Germany), to inject fluid during liposuction which loosens fat cells while minimizing surrounding soft tissue collateral damage. A piston pump powers the system and forces pressurized fluid through a closed tubing system. Subsequently, the infiltration fluid is forced through a thin application cannula in a pulsatile manner. This cannula is surrounded by an external cannula that varies in diameter and arrangement of openings. The rate of flow for the infiltrative fluid and applied pressure are controlled/selected by the surgeon via a software guidance system. After the infiltration is performed, traditional liposuction is used to evacuate the subcutaneous fat. Like ultrasound-assisted liposuction, water-assisted liposuction is a gentle, less traumatic form of suction lipoplasty and has advantages in large volume fat grafting; however, water-assisted liposuction does not provide inherent skin contraction following adipose aspiration. Although theoretical advantages have been touted, there is limited adoption of this technology in the United States 28. In one study, approximately 3% of patients developed nodularity in the subcutaneous space within 6 weeks after surgery. Irregularities were successfully managed by a series of external ultrasound treatments and resolved by 3 months 29.
Aspirator devices
There have been few refinements or technological advances to the equipment responsible for generating one atmosphere of negative pressure necessary to adequately perform liposuction. Most devices generate vacuum suction through high-powered dual-cylinder piston pumps or modular pumps (vapor pressure vacuum) 30. Certain devices house a cooling fan to allow for pumps to run continuously as certain cases can last several hours. High-pressure tolerance tubing facilitates aspiration of the adipose tissue through the cannulas. Most devices contain a pressure gauge and generate up to 29+ inches Hg, which roughly translates to a negative pressure of 736 mmHg or greater to safely aspirate the subcutaneous fat. Several companies offer varying lines of aspirator devices. Wells Johnson Co, (Tucson, AZ, USA) and Mentor Worldwide LLC (Santa Barbara, CA, USA) are two examples of manufacturers of vacuum suction generating aspiration equipment.58 Generally, these aspirator generators can be used with any of the other technology devices listed in the previous sections.
Emerging medical technology
Radiofrequency-assisted liposuction
As surgeons and scientists continued to explore combining surgical suction of subcutaneous adipose with technology to tighten skin/provide soft tissue contraction, increased interest has grown in utilizing radiofrequency as an adjunct to suction-assisted lipectomy 31. Radiofrequency energy is high frequency oscillating electrical current (one million cycles per second) applied to the tissue to create a thermal effect. Radiofrequency-assisted liposuction is responsible for dissolving fat cells, which leads to the creation of small channels in the fatty tissue. Furthermore, radiofrequency-assisted liposuction causes dermal physiologic responses including immediate contraction of the collagen fibers, subdermal remodeling, and neocollagen formation 32.
Radiofrequency-assisted liposuction is a computer controlled, bipolar radiofrequency device that simultaneously coagulates fat, aspirates the liquefied fat, and contracts the fibroseptal network (FSN) 33. The first such technological advancement to employ radiofrequency for lipolysis is the BodyTite™ system (Invasix Ltd, Yokneam Ilit, Israel). The internal electrode of the BodyTite™ is a hollow Mercedes-tip suction cannula/electrode and is silicone coated, except for the tip. The tip delivers radiofrequency, which flows to an external circular electrode that slides along the surface of the skin, in tandem with the internal electrode. This contact surface creates lower power density in the upper dermal layer and closes the radiofrequency current loop by receiving the energy through the skin. Furthermore, the external electrode has an imbedded thermal sensor that measures real-time skin temperature ten times per second, leading to uniform heating of the subreticular dermis, which aids in the denaturation and remodeling of collagen 34. This is an important concept and ensures patient safety by avoiding thermal injury which can result in deep burns and pathologic scarring. In addition, the pericanalicular temperature, high and low dermal impedance, and the external electrode contact are measured. There are safety radiofrequency cutoffs for each of these measured parameters, which greatly reduce the risk of a thermal injury. The two Bodytite™ electrodes are connected to a handpiece that controls the depth of the internal electrode. Power settings, from 25 to 75 W, result in radiofrequency being emitted from the tip which creates a thermal coagulative necrosis zone (approximately 90°C for 1.0 cm above the cannula), leading to adipose tissue coagulation and contraction of the fibroseptal network.62 The radiofrequency-assisted liposuction hand piece and the hollow internal cannula/probe are attached to suction, so there is simultaneous aspiration of the coagulated and liquefied fat. When the internal pericanalicular temperature reaches an average of 60°C, the fat is liquefied, and the fibroseptal network has been stimulated and contracted. The Bodytite™ safety features include computer-monitored external skin thermal sensors, high and low dermal impedance, and internal thermal sensors, as well as contact sensors. When the internal temperature or skin temperature is reached, the radiofrequency energy is cut off, alerting the physician when to proceed or stop. The radiofrequency-assisted liposuction generally never approaches more superficial than 2 cm from the skin surface. When the epidermis reaches 38°C–42°C, the thermal heating and aspiration in the respective zone is complete. During the radiofrequency-assisted liposuction thermal procedure, approximately 30% of the desired aspiration occurs, and completion suction-assisted lipectomy or power-assisted liposuction contouring is performed.
One of the reported advantages of Bodytite™ and radiofrequency-assisted liposuction is the significant contraction of the skin and soft tissue, which has been reported to be ≥35% at 12 months compared with <8% for standard suction-assisted lipectomy 35. Surgeons proficient in the Bodytite™ technique can get very strong soft tissue contraction in zones with prominent fibroseptal network, without the need for aggressive subdermal liposuction or skin excision. While a theoretical disadvantage of the radiofrequency-assisted liposuction system is thermal injury to the surrounding dermal structures, there have been no reports of this within the peer-reviewed literature. Reported complications have been minimal, and include bruising, surface irregularities, and pain 36. The radiofrequency-assisted liposuction system shows promise and has a significant amount of international experience and data. FDA approval is pending.
Non surgical liposuction
The “holy grail” for body-sculpting technology is noninvasive technologies that minimize tissue morbidity, decrease downtime, and increase skin contraction/tightening, which lessens the need for skin excision by way of surgical intervention. This has led to a new industry: noninvasive body contouring. The technology and products are beyond the scope of this liposuction technology update report; however, these nonsurgical adipose reducing techniques are on the horizon and available. The indications and outcomes are completely different than liposuction, and therefore, are not comparable.
Cryolipolysis is being routinely employed to decrease small target adipose deposits. Coolsculpt™ (Zeltiq, Pleasanton, CA, USA) employs this technology. Cryolipolysis refers to using cold exposure to selectively induce subcutaneous fat necrosis by stimulating the inflammatory reaction/cascade within adipose tissue due to a response to the exposure to cold 37. A systematic review of 662 patients performed by the authors demonstrated a 22% reduction in subcutaneous fat deposits as measured by caliper thickness. Additionally, there was a minimal (4%) reported complication rate, which included pain and contour irregularities. These complications resolved without intervention.
High-intensity focused ultrasound (HIFU) delivers focused, high-intensity ultrasonic energy to deep subcutaneous tissue. This effectively produces heat capable of ablating adipose tissue and thermally modifying collagen. The optimal high-intensity focused ultrasound frequency and intensity for body sculpting, which is capable of disrupting adipocytes and contracting collage fibers to tighten skin, is 2 MHz and >1,000 W/cm2, respectively 38. One such product available is the Liposonix™ system from Solta Medical (Hayward, CA, USA). Complications of using the device were minimal and included pain, surface irregularities, and subcutaneous nodules. All complications resolved without intervention 39.
Radiofrequency devices utilize optical energies delivered to the dermis/hypodermis. Optical infrared energy targets primarily the dermal water, whereas the radiofrequency energy targets the hypodermis by controlled thermal stress. The application of thermal energy to the dermis leads to dermal tightening and contraction. Furthermore, there is activation of physiologic responses inside the dermal fibroblasts to stimulate collagen formation. The vacuum adjunct potentiates collagen formation by inducing mechanical stress factors on the dermal fibroblasts. The application of bipolar radiofrequency energy to the hypodermis increases fat cell metabolism and quickens triglyceride egress 40. Certain devices (BodyFX™; Invasix Ltd, Yokneam Ilit, Israel) use radiofrequency to preheat the dermis and first 15–20 mm of fat and use a precise thermistor built inside the suction cavity to monitor the skin temperature and suction distribution. When the epidermal temperature reaches the desired level, a high-voltage, electroporation pulse is generated through the adipose tissue within the treatment field. Randomized, human tissue studies have shown a high voltage electroporation apoptotic effect on up to 30% of the adipocytes in the field of treatment, leading to a permanent radiofrequency induced fat reduction 41.
The emerging technologies are unified in the goal to decrease subcutaneous fat deposits while providing dermal tightening. Additionally, these instruments aim to provide this result in a single use, minimally invasive application. While all of these emerging technologies fall short in achieving superiority over one another, they seemingly all have the same side-effect profile, which includes pain and surface irregularities. There is continued interest in modifying the technique by adding technologies with energy to optimize skin tightening and fat emulsification. Furthermore, recognizing the existence of adipose-derived stem cells and the capability of autologous fat grafting has led to the desire to study harvesting/liposuction techniques to optimize graft survival 42.
Who is a suitable candidate for liposuction?
Liposuction is a cosmetic surgery used to remove localized accumulations of fat that are resistant to diet and exercise. Liposuction is not a weight loss strategy, substitute for exercise or cure for obesity. It also does not have any effect on cellulite or stretch marks.
Generally anyone with good health physically and mentally can have the procedure done however a patient must go through extensive counseling prior to undergoing surgery to ensure they are suitable.
An ideal candidate for liposuction would have:
- normal-weight or slightly-overweight with localized pockets of excess fat in certain areas
- generally healthy and does not have significant medical problems
- elastic skin
- realistic expectations
- is over 18
- age is not a major factor, although older persons with diminished skin elasticity may not have the same results as persons with tighter skin
- has tried diet and exercise
- has a stable weight and has a regular exercise routine
- does not suffer from diabetes, coagulation disorders, cardiovascular disease or any infectious disease
- is not pregnant
These are only a guide; however patients that fill these criteria will have a more optimal result.
Liposuction is also suitable for the treatment of other conditions such as breast reduction in men, gynecomastia, removal of lipomas and angiolipoma, hematoma evacuation and improving hyperhidrosis of axillae (excessive armpit sweating).
If you are thinking about liposuction
There is a great deal of pressure on people to have a certain look and body shape. But liposuction might not be the solution.
Liposuction might be right for you if you have realistic expectations about the procedure, have tried to change your body shape with a healthy diet and regular exercise, and are in good health going into the procedure.
You should speak to your doctor before undergoing liposuction since your doctor is best placed to help you manage your overall health.
You should also be aware:
- Liposuction is probably not right for you if you are looking for a way to lose weight.
Is liposuction right for me?
Liposuction is an individualized procedure and may not be suitable for everyone. Always talk to your Board Certified Plastic Surgeon before making a decision. Your Board Certified Plastic Surgeon will assess your condition and general health, and plan the treatment that is best suited to you.
Liposuction may be suitable for you if:
- You are physically healthy and at a stable weight
- You have realistic expectations
- You are a non-smoker or have stopped smoking
- You have bulges that persist despite a healthy diet and exercise
Liposuction is most likely to be successful for healthy weight people with firm, elastic skin who have pockets of excess fat in certain areas. Although age is not a significant concern, older people may have less skin elasticity and may not achieve the same results as a younger person with tighter skin.
Before opting for liposuction, you must keep in mind that:
- Liposuction is not a substitute for weight loss
- If your skin is dimpled before the liposuction, it will probably still be dimpled afterward the procedure has been done
- If the ‘extra’ skin doesn’t contract (tighten) after liposuction, you may need a further procedure to remove excess skin
- You may not be able to undergo the procedure if you are unable to have an anesthetic, if you are prone to bleeding tendencies or have poor healing ability or are too high risk of having surgical complications
What are the costs associated with liposuction procedure?
Cost is always a consideration in elective surgery. Prices for individual procedures can vary widely between Board Certified Plastic Surgeon. Some factors that may influence the cost include the surgeon’s experience, the type of procedure used and the geographic location of the office.
Costs associated with the procedure may include:
- Surgeon’s fee
- Hospital or surgical facility costs
- Anesthesia fees
- Prescriptions for medication
- Post-surgery garments
- Medical tests
Your surgeon should welcome any questions you may have regarding fees.
You can find Board Certified Plastic Surgeons here:
- American Society for Aesthetic Plastic Surgeon (https://www.surgery.org/consumers/find-a-plastic-surgeon)
- American Society of Plastic Surgeons (https://find.plasticsurgery.org/)
Liposuction preparation
Before undergoing liposuction surgery, it is important that you:
- Be as fit as possible to help the recovery process
- Reach your optimal weight
- Check with your surgeon about your medications as some may need to be stopped
- Stop smoking
You will also be asked to provide a complete medical history for your Board Certified Plastic Surgeon including any health problems you have had, any medication you are taking or have taken, and any allergies you may have.
Physical evaluation
An assessment of your general physical health is necessary to determine whether you are a suitable candidate for surgery. The specific sites that are being considered for liposuction are examined for potential problems. Your skin tone and elasticity is assessed as well as the presence of hernias, scarring, cellulite and stretch marks. If you have poor skin elasticity you are informed that following liposuction surgery you may have skin draping which may need further surgical correction.
Psychological assessment
Inquires are made about your diet and exercise habits and any history of weight gain and loss as this can affect the long term success of the liposuction procedure. Patients are counseled on the limitations and risks associated liposuction. Their expectations are determined to ensure they are realistic and are aware that full results may take up to 12 weeks to be seen. Liposuction does not result in any significant weight loss and patients should also be aware that fat removed may return if excess weight is put on.
Blood tests
Some general blood tests are carried out to ensure you are in good health. Selection blood tests to be performed depends on the type and extent of the liposuction procedure and the conditions revealed in your medical history and physical examination. Usually a complete blood cell count with quantitative platelet assessment, prothrombin time, partial thromboplastintime, liver function tests, pregnancy test for women of child bearing age are performed.
Patients with any history of the following conditions must receive medical clearance before undergoing liposuction:
- Bleeding disorders
- Blood clotting disorders
- Thrombophlebitis (inflammation of the vein)
- Infectious diseases
- Poor wound healing
- Diabetes mellitus
- Heart problems
- High blood pressure
- Allergic reactions to medications
- Lung problems
- Smoking, alcohol, or drug use
You may be advised to stop taking certain medicines such as non-steroidal anti-inflammatory drugs (NSAIDs), aspirin, and medicines that contain aspirin. You may also be asked to stop taking naturopathic substances such as garlic, ginko, ginseng and St John’s Wort as they may affect clotting and anesthesia. Always tell your surgeon EVERYTHING you are taking.
You may be given medicines to take before the surgery, such as antibiotics.
Your surgeon will also advise you if any other tests are required, such as blood tests, X-ray examinations or an Electrocardiograph (ECG) to assess your heart.
Prepare a “recovery area” in your home. This may include pillows, ice packs, a thermometer and a telephone within easy reach. Make sure you arrange for a relative or friend to drive you to and from the hospital or clinic. Someone should also stay with you for at least 24 hours after you return home.
Your surgeon should give detailed preoperative instructions. Follow them carefully.
What happens during a liposuction procedure?
Liposuction Procedural Steps
- Step 1 – Anesthesia
Medications are administered for your comfort during the surgical procedures. The choices include intravenous sedation and general anesthesia. Your doctor will recommend the best choice for you.
- Step 2 – The incision
Liposuction is performed through small, inconspicuous incisions.
First, sterile liquid solution is infused to reduce bleeding and trauma. Then a thin hollow tube, or cannula, is inserted through these incisions to loosen excess fat using a controlled back and forth motion.
The dislodged fat is then suctioned out of the body using a surgical vacuum or syringe attached to the cannula.
- Step 3 – The recovery
Your improved body contour will be apparent when the swelling and fluid retention commonly experienced following liposuction subside.
With continued practices of healthy diet and fitness, the loss of excess fatty tissue should be permanently maintained. However, substantial weight gain can alter an otherwise permanent result.
Anesthesia
Liposuction can be performed in either in an office, an accredited day surgery or a hospital, depending on your general health and the extent of the procedure. A short hospital stay may be required in some instances. Your Board Certified Plastic Surgeon will advise on the best option for you. Usually liposuction of smaller volumes are done as an outpatient while larger volumes require a stay in hospital to monitor fluid levels and if you’re suffering from any other medical conditions. Depending on how many sites will be treated, the surgery time may range from 1-4 hours.
Depending on your procedure and the amount of fat removed, liposuction can take place under either local or general anesthesia. If only a small amount of fat and a limited number of body sites are involved, liposuction can be performed under local anesthesia, which numbs only the affected areas. For large volumes of fat, general anesthesia is commonly used.
Modern anesthesia is safe and effective, but does have some risks. Ask your Board Certified Plastic Surgeon and anesthetist for more information. Your surgeon and/or anesthetist will ask you about all the medications you are taking or have taken, and any allergies you may have. Make sure you have an up to date list before the surgery.
The incision
Markings are made on your skin as a guide to where fat is to be removed. Depending on which procedure is used a general anesthetic is administered, or for the tumescent technique, a fluid consisting of a salt solution or local anesthetic and epinephrine is injected into the area being liposuctioned. Very small cuts are made in your skin through which a cannula is inserted. The cannula is attached to vacuum pump which can suction out the fat cells as the surgeon moves it back and forth. After the fat is removed, small drainage tubes may be inserted which remove any blood and fluid which has accumulated. If a lot of fluid is lost then a blood transfusion or IV fluid replacement may be needed.
Volumes of fat removed should not exceed five liters especially in patients with other medical problems. Generally, removal of larger volumes is associated with a higher risk of complications mainly due to the fact that this requires general anesthesia as opposed to local anesthesia.
Following your liposuction surgery, bandages are applied to stop any bleeding and keep pressure on the area. These usually are left on for about two weeks. Depending on the extent of the liposuction surgery and how much fat was removed you may be required to stay overnight in hospital.
It must also be determined whether any previous abdominal surgery has been performed and any problems from past surgical procedures that may influence complications.
Medications that affect blood clotting such as aspirin, anti-coagulants, non-steroidal anti-inflammatory agents and vitamin E, as well as other vitamins and herbs must be ceased two weeks prior to your liposuction surgery. Depending on the extent of the liposuction to be done, the contraceptive pill may have to be ceased as well.
Liposuction recovery
How you recover after a liposuction will vary depending on how much surgery you have and which part of your body is involved. You might wake up with a small tube draining fluid from the site of the surgery.
Some people need a short hospital stay after liposuction. You will also need a few days rest at home. You should expect to have pain for several days and will probably be prescribed some form of pain relief medicine (as well as antibiotics to prevent infection).
Following your surgery, dressings or bandages may be applied to your incisions. You may be wrapped in an elastic bandage or a compression garment to reduce swelling and support the skin as it readjusts to the new contour and to support your operation site as it heals. These usually need to be left on for 2-3 weeks. A small, thin tube may also be temporarily placed under the skin to drain any excess blood or fluid that may collect.
Depending on the extent of your procedure, you may need to take a few days off work to rest, however walking soon after surgery is advised to prevent blood clots. Avoid heavy lifting, strenuous exercise, swimming and strenuous sports until advised by your surgeon.
It may take up to 3-6 months to see the final result of the liposuction surgery as swelling subsides and skin contraction occurs. The final outcome generally depends on your age, skin elasticity, volume of fat removed and the area it is removed from, with the best results are generally seen in younger patients of normal weight and who have had a small volume of fat removed. Maintaining a healthy lifestyle with regular exercise all aid in improving the final outcome.
If you experience any of the following symptoms, notify your surgeon immediate:
- Temperature higher than 100.4 °F (38°C) or chills
- Heavy bleeding from the incisions
- Worsening redness around the incision sites
- Increasing pain or tenderness, or other problems that appear to be worsening
Your surgeon will give you specific instructions on post-operative care. These instructions may include:
- How to care for your surgical site(s) following surgery
- Medications to apply or take orally to aid healing and reduce the risk of infection
- Specific concerns to look for at the surgical site(s) or in your general health
- When to follow-up with your surgeon
Be sure to ask your surgeon specific questions about what you can expect during your individual recovery period, such as:
- Where will I be taken after my surgery is complete?
- What medication will I be given or prescribed after surgery?
- Will I have dressings/bandages after surgery? If so, when will they be removed?
- Are stitches removed? When will they be removed?
- When can I resume normal activity and exercise?
- When do I return for follow-up care?
Recovery time frame after liposuction
It is vitally important that you follow all patient care instructions provided by your surgeon. This will include information about wearing compression garments, taking an antibiotic, if prescribed, and the level of activity that is safe. Your surgeon will also provide detailed instructions about the normal symptoms you will experience and any potential signs of complications. It is important to realize that the amount of time it takes for recovery varies greatly among individuals.
The first two weeks
- The first few days after surgery, you should rest quietly. Elevate the affected body part if possible. Remember, you must not take aspirin or certain anti-inflammatory medications. You will most likely wear a postsurgical garment; if it is too tight, notify your surgeon.
- The first 48 hours after surgery, you will experience varying degrees of swelling and bruising. The swelling is maximal at 48 hours after surgery and mostly disappears within two to three weeks, but there may be slight residual swelling for up to four months. Bruising is normal and typically disappears within seven to ten days.
- Sutures, if placed, are usually removed seven to ten days after liposuction.
- Do not smoke after your liposuction surgery to prevent coughing and bleeding. Do not drink alcohol for five days after surgery or while you are taking pain medication.
- Avoid straining, bending over and lifting during the early postoperative period. In many cases, you will be able to resume most of your normal activities within ten days or less.
- Discomfort after liposuction is generally limited to soreness rather than pain. Pain medications are prescribed to lessen any discomfort during the first few days.
- Patients usually return to work within a few days following a liposuction procedure.
Weeks two to six
- It is important to ambulate (walk) as soon as possible after liposuction to discourage swelling and prevent blood clots in the legs. However, avoid strenuous exercise for four to six weeks because it can trigger unnecessary fluid retention in the treated areas.
- You should wait a minimum of six weeks before exposure to sun and heat, including sunbathing, because of the possibility of swelling.
- You will wear a compression garment over the treated areas for four to six weeks to control swelling and promote skin contraction.
Long-term recovery
Since the healing process is gradual, you should expect to wait at least several months to get an accurate picture of the results of your surgery. The small incisions used for access will fade over a number of months, usually becoming barely visible. For six to nine months, you may experience a fluctuating return of ten to 15 percent swelling with exercise or excessive activity. It is important to see your doctor as scheduled. Follow-up visits will continue for several weeks and then after several months at prescribed intervals.
Liposuction scars
Scars are an inevitable part of any invasive surgery. Your Board Certified Plastic Surgeon will endeavor to minimize scarring and to keep your scars as inconspicuous as possible by locating the incisions in easily hidden sites. That way, scars will be along natural skin lines and creases. Scars may fade with time and become barely noticeable over time.
- The amount or degree of scarring depends on the surgeon’s technique and your genetic tendencies.
- Most liposuction scars fade and are barely perceptible over time. Visible scars are more likely when large liposuction cannulas are used and in patients who have darkly pigmented skin.
- There are two types of marks that can remain on the skin after liposuction. One is a true scar and the other is known as dyschromia, which is a dark (hyperpigmented) or light (hypopigmented) spot on the skin.
- Generally, the incisions are very small and placed in hidden areas. Sometimes, depending on the area, the incisions cannot be hidden.
Liposuction results (before and after)
Liposuction for women
Figure 1. Stomach liposuction

Figure 2. Thigh liposuction
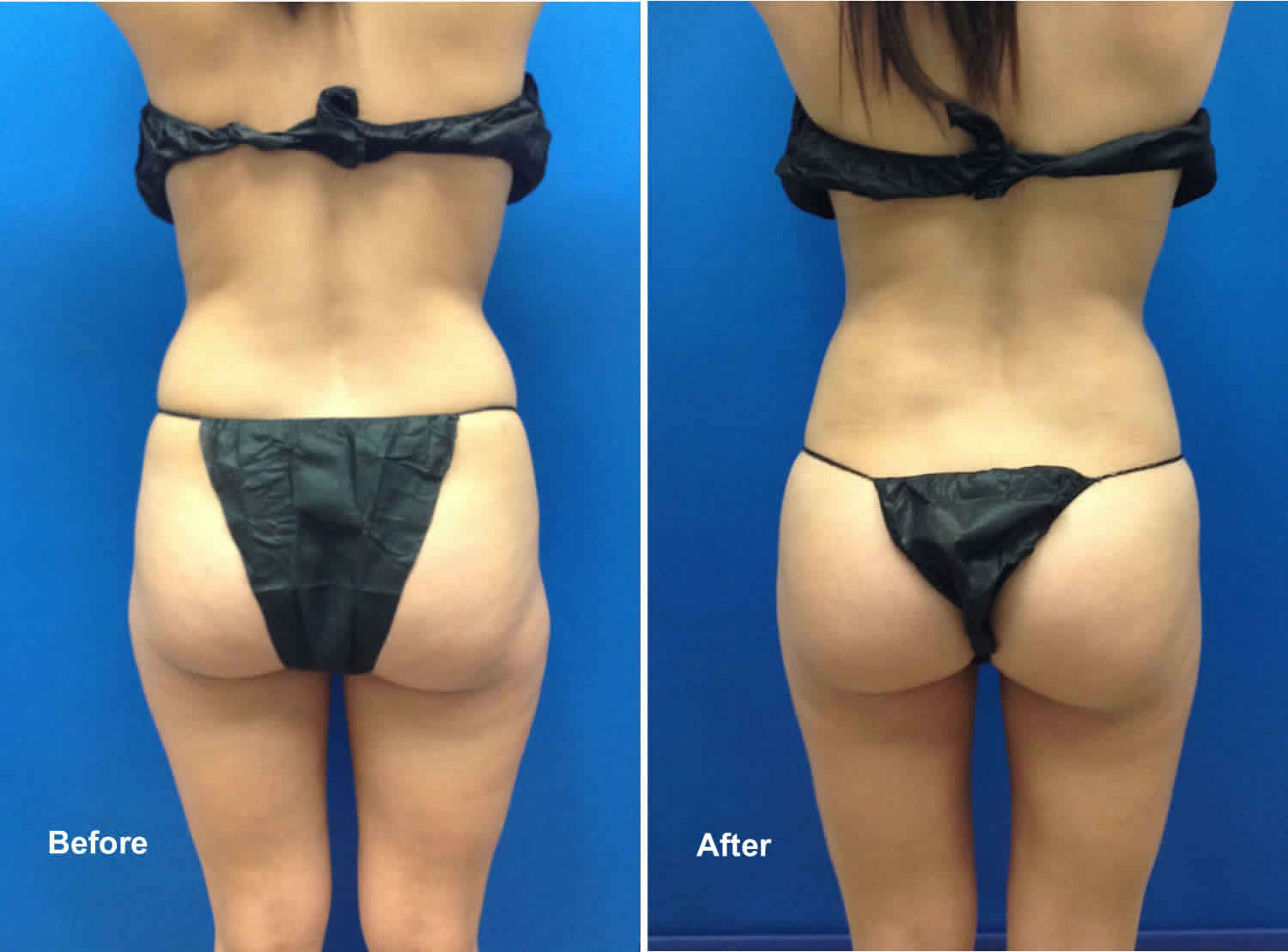
Figure 3. Face liposuction

Figure 4. Chin liposuction

Figure 5. Neck liposuction

Figure 6. Arm liposuction with arm-lift

Liposuction for men
Figure 7. Breast liposuction

Footnote: 48 year old male had extra breast tissue that he wished to have reduced. He was treated for Gynecomastia with Liposuction of the chest. His Post Op photos were taken 1 month after surgery.
Figure 8. Stomach liposuction

Will I need revisional surgery?
In most circumstances, liposuction does not need to be repeated. Usually, the ‘extra’ skin will contract (tighten) after the procedure. However, as with all surgical procedures, revisional surgery may be necessary to correct minor irregularities. In some cases, a procedure to remove excess skin may also be needed.
How long will the results last?
The results of liposuction surgery are technically permanent because fat cells have been removed. However, your body shape and contours might be affected by weight gain, aging, pregnancy, family genes and lifestyle factors.
It is crucial to maintain healthy habits and a stable weight to maintain liposuction results. Following liposuction, if you continue to eat excess calories, fat will no longer be stored in the cells that have been removed, but will be stored in other body areas.
There is no way to predict where your body will store new fat. What’s more, your surgeon will not remove all of the fat cells from your target area, so you could still increase the size of remaining fat cells in that area.
- The basic message: keep your weight stable for a long lasting result.
Maintain a relationship with your aesthetic plastic surgeon. For safety, as well as the most beautiful and healthy outcome, it’s important to return to your plastic surgeon’s office for follow-up evaluation at prescribed times and whenever you notice any changes in the treated area. Do not hesitate to contact your surgeon when you have any questions or concerns.
Liposuction vs Tummy tuck
A tummy tuck is also called abdominoplasty surgery. Tummy tuck surgery can range from a simple mini-abdominoplasty to more extensive surgery. Tummy tuck is able to eliminate excess skin and stubborn excess deposits of fat in the midsection. Tummy tuck surgery can also repair abdominal muscle separation, known as diastasis recti. Tummy tuck surgery can help you achieve a tighter, flatter, more fit appearance of the abdomen and flanks (love handles).
The tummy tuck is one of the most commonly performed aesthetic surgical procedures across the world. It is estimated that more than 800,000 people undergo tummy tuck each year, making tummy tuck the sixth most common cosmetic procedure 43. The main objective of an tummy tuck is to reshape your body contour by means of excising redundant skin and fat tissue to remodel the abdominal wall. Since its initial conception more than a century ago, various surgical alternatives have been proposed 44. However, it was during the 1960s and 1970s that the contributions of Vernon 45, Pitanguy 46 and Grazer 47 established the founding pillars of modern tummy tuck. Tummy tuck is also the second most popular body cosmetic surgery nationwide and is performed over 100,000 times per year in the United States.
Tummy tuck surgery is not the same as liposuction, which is another way to remove fat. But, tummy tuck is sometimes combined with liposuction. Tummy tuck in combination with liposuction of the abdomen and flanks can remove stubborn pads of fat that may be resistant to diet and exercise.
An tummy tuck is not a substitute for weight loss and patients should reach their goal weight prior to undergoing tummy tuck surgery. However, if you have subcutaneous fat around your abdomen that persists despite your best weight loss efforts, your American Board of Plastic Surgery certified plastic surgeon can include liposuction in your tummy tuck procedure to better contour the midsection.
The best candidates for a tummy tuck have loose skin around their abdomen, as well as loose abdominal muscles (diastasis recti) or excess fatty deposits. Most frequently, tummy tuck patients are women who have been pregnant, but the procedure can also benefit men or women who have lost a significant amount of weight that left them with baggy skin and an unflattering midsection. A consultation with a board certified plastic surgeon (American Board of Plastic Surgery) will help you better understand the results you can expect to see from an tummy tuck surgery and whether you might be a good candidate
During an tummy tuck surgery, the surgeon will make a cut in the fold under the belly. This is the “bikini line.” Skin is also cut around the belly button. A large area of fat and skin are then pulled away from the muscle.
Tummy tuck can be helpful when:
- Diet and exercise have not helped improve muscle tone, such as in women who have had more than one pregnancy.
- Skin and muscle cannot regain its normal tone. This can be a problem for very overweight people who lost a lot of weight.
You might consider a tummy tuck if:
- You have excess skin that’s accumulated around the area of your bellybutton
- You have a weak lower abdominal wall
- Liposuction didn’t adequately improve the appearance of your abdomen
- You previously had a C-section and have retracted scarring
If you’ve previously had a Caesarean section, your plastic surgeon might be able to incorporate your existing C-section scar into your tummy tuck scar.
A tummy tuck can also be done in combination with other body contouring cosmetic procedures, such as breast surgery.
A tummy tuck isn’t for everyone. Your doctor might caution against an tummy tuck if you:
- Plan to lose a significant amount of weight
- Might consider future pregnancy
- Have a severe chronic condition, such as heart disease, diabetes or irritable bowel syndrome
- Have a body mass index (BMI) that’s greater than 30
Tummy tuck procedure is a major surgery. Be sure you understand the risks and benefits before having it.
Tummy tuck is not used as an alternative to weight loss.
Tummy tuck risks
Risks for anesthesia and surgery in general are:
- Reactions to medicines
- Breathing problems
- Bleeding, blood clots, or infection
Risks for tummy tuck surgery are:
- Loss of skin
- Nerve damage that can cause pain or numbness in part of your belly
- Poor healing
- Fluid accumulation beneath the skin (seroma). Drainage tubes left in place after surgery can help reduce the risk of seroma. Your doctor might also remove fluid after surgery using a needle and syringe.
- Poor wound healing. Sometimes areas along the incision line heal poorly or begin to separate. You might be given antibiotics during and after surgery to prevent a resulting infection.
- Excessive scarring. The incision scar from a tummy tuck is permanent, but is placed along the easily hidden bikini line. The length and visibility of the scar will vary from person to person.
- Tissue necrosis. During a tummy tuck, fatty tissue deep within your skin in the abdominal area might get damaged or die. Smoking increases the risk of tissue necrosis. Depending on the size of the area, tissue might heal on its own within weeks or require a surgical touch-up procedure.
- Changes in skin sensation. During a tummy tuck, the repositioning of your abdominal tissues can affect superficial sensory nerves in the abdominal area, and infrequently, in the upper thighs. You’ll likely feel some reduced sensation or numbness. This usually diminishes in the months after the procedure.
Like any other type of major surgery, a tummy tuck poses a risk of bleeding, infection and an adverse reaction to anesthesia.
According to the published case series, local complications are considerably more common than complications with systemic repercussions 48. Approximately 10% to 20% of patients suffer a local complication following tummy tuck, while fewer than 1% suffer a systemic complication. Complications including seroma, hematoma, infection, skin necrosis, suture extrusions, hypertrophic scars, neurological symptoms, umbilical anomalies, deep venous thrombosis and pulmonary thromboembolism, respiratory distress, and death 48.
The combination of tummy tuck with abdominal liposuction remains a controversial subject. This controversy reached its zenith in February of 2004 when, after several patient deaths, the state of Florida placed a temporary moratorium preventing the simultaneous combination of tummy tuck with liposuction in the office setting, mandating a minimum 14-day interval between the two operations 49. This has led to the evolution of a different operation entirely, sometimes called lipotummy tuck 50. Lipotummy tuck differs from the combination of tummy tuck and liposuction in that the liposuction is performed first in lipotummy tuck, and there is limited undermining of the abdominal flap in the area above the umbilicus, thus sparing multiple perforator vessels. This new operation slowly evolved out of many surgeons’ efforts. This operation differs from traditional tummy tuck in several ways. First, the liposuction is performed first and the flap is elevated with hydrodissection and liposuction. Second, there is typically limited undermining of the flap above the umbilicus. Third, there is usually no closure, or only segmental closure of the rectus diastasis 51. The results shown in the article by Brauman and Capocci are impressive, and this is a useful technique for body contouring 51. Avelar’s technique involves even less undermining of the superior abdominal flap, and the umbilicus is not transposed 52. His technique does involve the addition of skin excision in the inframammary area in selected cases.
Despite all the complications mentioned, tummy tucks and lipotummy tucks are reproducible and very gratifying operations for both patients and surgeons.
Liposuction risks
Modern surgery is generally safe but does have the potential for risks and complications to occur. Liposuction is associated with several risks and complications, many of which are rare and are dependant on the extent and type of procedure. The risks of liposuction increase if a large number of body areas are treated at the same time or if the areas operated on are large in size. As there is no central registry for reporting of these it is difficult to ascertain the likelihoood or frequency of them. It appears that prolonged procedures and aspirate volumes greater than five liters seem to be associated with higher complication rates. Limiting the volume of aspirate and using local rather than general anesthesia can reduce the risk of some of the major complications such as embolism and death.
A national survey of plastic surgeons found that the most common complications were:
- contour irregularities
- unplanned hospital admissions
- prolonged swelling
Other complications include:
- Patient dissatisfaction
- Unfavorable aesthetic results- irregularities in the skin surface following excessive or subdermal liposuction asymmetry, dimpling, lumpiness and waviness and skin laxity
- Hyperpigmentation
- scarring- incisions usually heal however patient can develop hypertrophic scarring following inadvertent injury to overlying skin through superficial liposuction or ultrasound assisted liposuction
- Hematomas
- Seromas
- Infections
- Skin burns, particularly in the use of ultrasound assisted liposuction devices
- Skin necrosis- superficial liposuction, overzealous subdermal fat thinning, liposuction in areas of prior incision scars, and UAL can result in partial-thickness and full-thickness skin necrosis
- Necrotizing fasciitis
- Cerebrovascular accident (stroke) or transient ischemic attack
- Pulmonary thromboembolism (blood clots in lungs)
- Pulmonary fat embolism (fat clots in lungs)
- Bleeding, especially if large amounts of fat are removed
- Shock if not enough fluid is replaced during the surgery
- Fluid overload
- Transfusion complication
- Deep vein thrombosis (DVT or blood clots in legs)
- Drug toxicity, the patient can react to the anesthetic or epinephrine
- toxic shock syndrome
- Nerve damage
- Thoracic and abdominal cavity perforation
- Aortic perforation
- Acute renal failure (kidney failure)
Rates of serious or fatal complications are in the range of 0.02% to 0.3% and are predominantly attributed to pulmonary embolus, fat embolus, abdominal perforation and anesthesia.
Some of the possible complications and risks associated with liposuction may include:
- Thermal burn or other heat injury to the skin or deeper tissues from the ultrasound device that is used to liquefy fat cells. This can occur in ultrasound-assisted liposuction
- Complications caused by the injection of anesthetic fluid can include lignocaine toxicity (if the solution’s lignocaine content is too high) or collection of fluid in the lungs (if too much fluid is given). This can occur in tumescent and super-wet liposuction
- Excessive fluid loss, which can lead to shock
- Fluid accumulation
- Infection that develop in fatty tissues. This can be a serious complication and can be difficult to treat
- Delayed healing
- Friction burns or other damage to the skin or nerves
- Irregular skin surface, uneven contours or rippling
- Asymmetric or ‘baggy’ skin surface
- Change in skin sensation or numbness
- Skin pigmentation changes, skin discoloration or swelling
- Unacceptable scarring
- Damage to deeper structures such as nerves, blood vessels, muscles, lungs and abdominal organs
- Pain, which may be ongoing
- Allergic drug reactions
- Formation of blood clots or fat clots, which may migrate to the lungs
- Persistent swelling in the legs
- Deep vein thrombosis, cardiac and pulmonary complications
- Further surgery may be necessary to address complications
Some common minor side effects that can occur which are usually not permanent or life threatening and are a normal consequence of the liposuction surgery include:
- Bruising which should fade after a few weeks
- Swelling which should subside gradually over a month or two
- Scars varying in size depending on the particular procedure but should fade over the weeks. Scarring depends on the individual as it is partly dependent on heredity. In some people it may take up to a year to heal.
- Pain which should be temporary and can be controlled by either over-the-counter medication
- Numbness which may persists for a few weeks
- Limited mobility
Liposuction risks that are reasonably common include:
- uneven skin with ripples or dimples
- baggy skin
- numbness or reduced sensation in the skin
- scarring
- changes to skin color
- slow healing.
Serious complications, which are less common, include:
- blood clots in the legs, which can travel to the lungs and cause serious illness
- excessive fluid loss, which can lead to shock
- burns to the skin or deeper tissue due to the ultrasound used to liquefy fat
- infection in the fatty tissues, which can be hard to treat.
Some people feel they may need to have more cosmetic surgery to remove or tighten any loose skin that may remain after the fatty tissue has been removed. Overall revision or re-operative rates range from 5-15%.
References- Georgiade NG. Essentials of plastic, maxillofacial, and reconstructive surgery. Baltimore: Williams & Wilkins; 1987.
- Kesselring UK. Body contouring with suction lipectomy. Clin Plast Surg. 1984;11:393–408.
- Illouz YG. Body Sculpting by Lipoplasty. New York: Churchill Livingstone; 1989.
- Kesselring UK. Regional fat aspiration for body contouring. Plast Reconstr Surg. 1983;72:610–619.
- Fournier PF, Otteni FM. Lipodissection in body sculpturing: the dry procedure. Plast Reconstr Surg. 1983;72:598–609.
- Zocchi ML. Ultrasonic assisted lipoplasty. Technical refinements and clinical evaluations. Clin Plast Surg. 1996;23:575–598.
- Rohrich RJ, Morales DE, Krueger JE, et al. Comparative lipoplasty analysis of in vivo-treated adipose tissue. Plast Reconstr Surg. 2000;105:2152–2158. discussion 2159.
- Maxwell GP, Gingrass MK. Ultrasound-assisted lipoplasty: a clinical study of 250 consecutive patients. Plast Reconstr Surg. 1998;101:189–202. discussion 203.
- Beckenstein MS, Grotting JC. Ultrasound-assisted lipectomy using the solid probe: a retrospective review of 100 consecutive cases. Plast Reconstr Surg. 2000;105:2161–2174. discussion 2175
- Personal experience with ultrasound-assisted lipoplasty: a pilot study comparing ultrasound-assisted lipoplasty with traditional lipoplasty. Fodor PB, Watson J. Plast Reconstr Surg. 1998 Apr; 101(4):1103-16; discussion 1117-9.
- Clinical application of VASER–assisted lipoplasty: a pilot clinical study. Jewell ML, Fodor PB, de Souza Pinto EB, Al Shammari MA. Aesthet Surg J. 2002 Mar; 22(2):131-46.
- Ultrasound-assisted lipoplasty learning curve. Zukowski ML, Ash K. Aesthet Surg J. 1998 Mar-Apr; 18(2):104-10.
- The American Society for Aesthetic Plastic Surgery (ASAPS) survey: current trends in liposuction. Ahmad J, Eaves FF 3rd, Rohrich RJ, Kenkel JM. Aesthet Surg J. 2011 Feb; 31(2):214-24.
- Complications of liposuction. Illouz YG. Clin Plast Surg. 2006 Jan; 33(1):129-63, viii.
- Fodor PB, Vogt PA. Power-assisted lipoplasty (PAL): a clinical pilot study comparing PAL to traditional lipoplasty (TL) Aesthet Plast Surg. 1999;23:379–385.
- Fodor P. Power-assisted lipoplasty. Aesthet Surg J. 2001;21:90–92.
- Fodor PB. Power-assisted lipoplasty versus traditional suction-assisted lipoplasty: comparative evaluation and analysis of output. Aesthet Plast Surg. 2005;29(2):127.
- Shridharani SM, Mohan R. A 51-year-old man with HIV and cervicodorsal lipodystrophy (buffalo hump) JAMA. 2013;309:1289–1290.
- Apfelberg DB, Rosenthal S, Hunstad JP, Achauer B, Fodor PB. Progress report on multicenter study of laser-assisted liposuction. Aesthet Plast Surg. 1994;18:259–264.
- Apfelberg DB. Results of multicenter study of laser-assisted liposuction. Clin Plast Surg. 1996;23:713–719.
- Anderson RR, Parrish JA. Selective photothermolysis: precise microsurgery by selective absorption of pulsed radiation. Science. 1983;220:524–527.
- Khoury JG, Saluja R, Keel D, Detwiler S, Goldman MP. Histologic evaluation of interstitial lipolysis comparing a 1064, 1320 and 2100 nm laser in an ex vivo model. Lasers Surg Med. 2008;40:402–406.
- Zelickson BD, Dressel TD. Discussion of laser-assisted liposuction. Lasers Surg Med. 2009;41:709–713.
- DiBernardo BE. Treatment of cellulite using a 1440-nm pulsed laser with one-year follow-up. Aesthet Surg J. 2011;31:328–341.
- DiBernardo BE, Reyes J. Evaluation of skin tightening after laser-assisted liposuction. Aesthet Surg J. 2009;29:400–407.
- Progress report on multicenter study of laser-assisted liposuction. Apfelberg DB, Rosenthal S, Hunstad JP, Achauer B, Fodor PB. Aesthetic Plast Surg. 1994 Summer; 18(3):259-64.
- 1,000 consecutive cases of laser-assisted liposuction and suction-assisted lipectomy managed with local anesthesia. Chia CT, Theodorou SJ. Aesthetic Plast Surg. 2012 Aug; 36(4):795-802.
- Araco A, Gravante G, Araco F, Delogu D, Cervelli V. Comparison of power water–assisted and traditional liposuction: a prospective randomized trial of postoperative pain. Aesthet Plast Surg. 2007;31:259–265.
- Sasaki GH. Water-assisted liposuction for body contouring and lipoharvesting: safety and efficacy in 41 consecutive patients. Aesthet Surg J. 2011;31:76–88.
- Grams Medical . Grams Aspirator (Model S-300): An Efficient, Exceptionally Quiet, Portable, Deep Vacuum Aspirator for Surgery. Costa Mesa, CA: Grams Medical
- Shridharani SM, Broyles JM, Matarasso A. Liposuction devices: technology update. Med Devices (Auckl). 2014;7:241-51. Published 2014 Jul 21. doi:10.2147/MDER.S47322 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4114741/
- Hantash BM, Ubeid AA, Chang H, Kafi R, Renton B. Bipolar fractional radiofrequency treatment induces neoelastogenesis and neocollagenesis. Lasers Surg Med. 2009;41:1–9.
- Paul M, Mulholland RS. A new approach for adipose tissue treatment and body contouring using radiofrequency-assisted liposuction. Aesthet Plast Surg. 2009;33:687–694.
- Theodorou SJ, Paresi RJ, Chia CT. Radiofrequency-assisted liposuction device for body contouring: 97 patients under local anesthesia. Aesthet Plast Surg. 2012;36:767–779.
- Duncan DI. Nonexcisional tissue tightening: creating skin surface area reduction during abdominal liposuction by adding radiofrequency heating. Aesthet Surg J. 2013;33:1154–1166.
- Ion L, Raveendran SS, Fu B. Body-contouring with radiofrequency-assisted liposuction. J Plast Surg Hand Surg. 2011;45:286–293.
- Mulholland RS, Paul MD, Chalfoun C. Noninvasive body contouring with radiofrequency, ultrasound, cryolipolysis, and low-level laser therapy. Clin Plast Surg. 2011;38:503–520. vii–viii
- Jewell ML, Baxter RA, Cox SE, et al. Randomized sham-controlled trial to evaluate the safety and effectiveness of a high-intensity focused ultrasound device for noninvasive body sculpting. Plast Reconstr Surg. 2011;128:253–262.
- Broyles JM, Shridharani SM. The safety and efficacy of cryolipolysis: a systematic review of available literature. American Society for Aesthetic Plastic Surgery; Annual Meeting; 2014; San Francisco.
- Anolik R, Chapas AM, Brightman LA, Geronemus RG. Radiofrequency devices for body shaping: a review and study of 12 patients. Semin Cutan Med Surg. 2009;28:236–243.
- Mulholland RS, Kreindel M. Non-surgical body contouring: introduction of a new non-invasive device for long-term localized fat reduction and cellulite improvement using controlled, suction coupled, radiofrequency heat and high voltage ultra-short electrical pulses. J Clin Exp Dermatol Res. 2012;3:1–9.
- Magarakis M, Shridharani SM, Singh NK, Redett RJ. Adipose stem cells and regenerative medicine. New York: Springer; 2011.
- International Society of Aesthetic Plastic Surgery . International study on aesthetic/cosmetic procedures performed in 2013. Hanover: International Society of Aesthetic Plastic Surgery; 2014.
- Kelly HA. Excision of the fat of the abdominal wall lipectomy. Surg Gynecol Obstet. 1910;10:229–31.
- Umbilical transplantation upward and abdominal contouring in lipectomy. VERNON S. Am J Surg. 1957 Sep; 94(3):490-2. https://www.ncbi.nlm.nih.gov/pubmed/13458618/
- Pitanguy I. Abdominal lipectomy: an approach to it through an analysis of 300 consecutive cases. Plast Reconstr Surg. 1967;40:384–91.
- Abdominoplasty. Grazer FM. Plast Reconstr Surg. 1973 Jun; 51(6):617-23. https://www.ncbi.nlm.nih.gov/pubmed/4705318/
- Vidal P, Berner JE, Will PA. Managing Complications in tummy tuck: A Literature Review. Archives of Plastic Surgery. 2017;44(5):457-468. doi:10.5999/aps.2017.44.5.457. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5621815/
- Florida Board of Medicine. Emergency Rule 64b8er04-2: Moratorium on combined liposuction/tummy tuck procedures in office surgery settings Florida Administrative Weekly. 2004;30:808.
- Samra S, Sawh-Martinez R, Barry O, Persing JA. Complication rates of lipotummy tuck versus traditional tummy tuck in high-risk patients. Plast Reconstr Surg. 2010;125:683–690. https://www.ncbi.nlm.nih.gov/pubmed/20124853
- Brauman D, Capocci J. Liposuction tummy tuck: An advanced body contouring technique. Plast Reconstr Surg. 2009;124:1685–1695. https://www.ncbi.nlm.nih.gov/pubmed/20009857
- Avelar JM. tummy tuck without panniculus undermining and resection: Analysis and 3-year follow-up of 97 consecutive cases. Aesthet Surg J. 2002;22:16–25. https://www.ncbi.nlm.nih.gov/pubmed/19331948





{kind=link}