What is a lobectomy
Lobectomy is a surgery to remove a whole lobe (section) of an organ (such as the lungs, liver, brain, or thyroid gland).
Lobectomy lung
A lobectomy is the surgical removal of one lobe of the lungs, usually to remove a lung cancer. A bilobectomy is the removal of two lobes, and a pneumonectomy is the removal of an entire lung. Lobectomy is usually used for the treatment of non-small cell lung cancers, especially if caught early enough that they have not spread very far. Because lung cancer most often develops in the right upper lobe, right upper lobectomy is the most performed resection.
Lobectomy is a major operative procedure, and there are risks involved. These, along with the benefits and the method of the procedure, should be discussed in detail with a surgeon before the operation takes place.
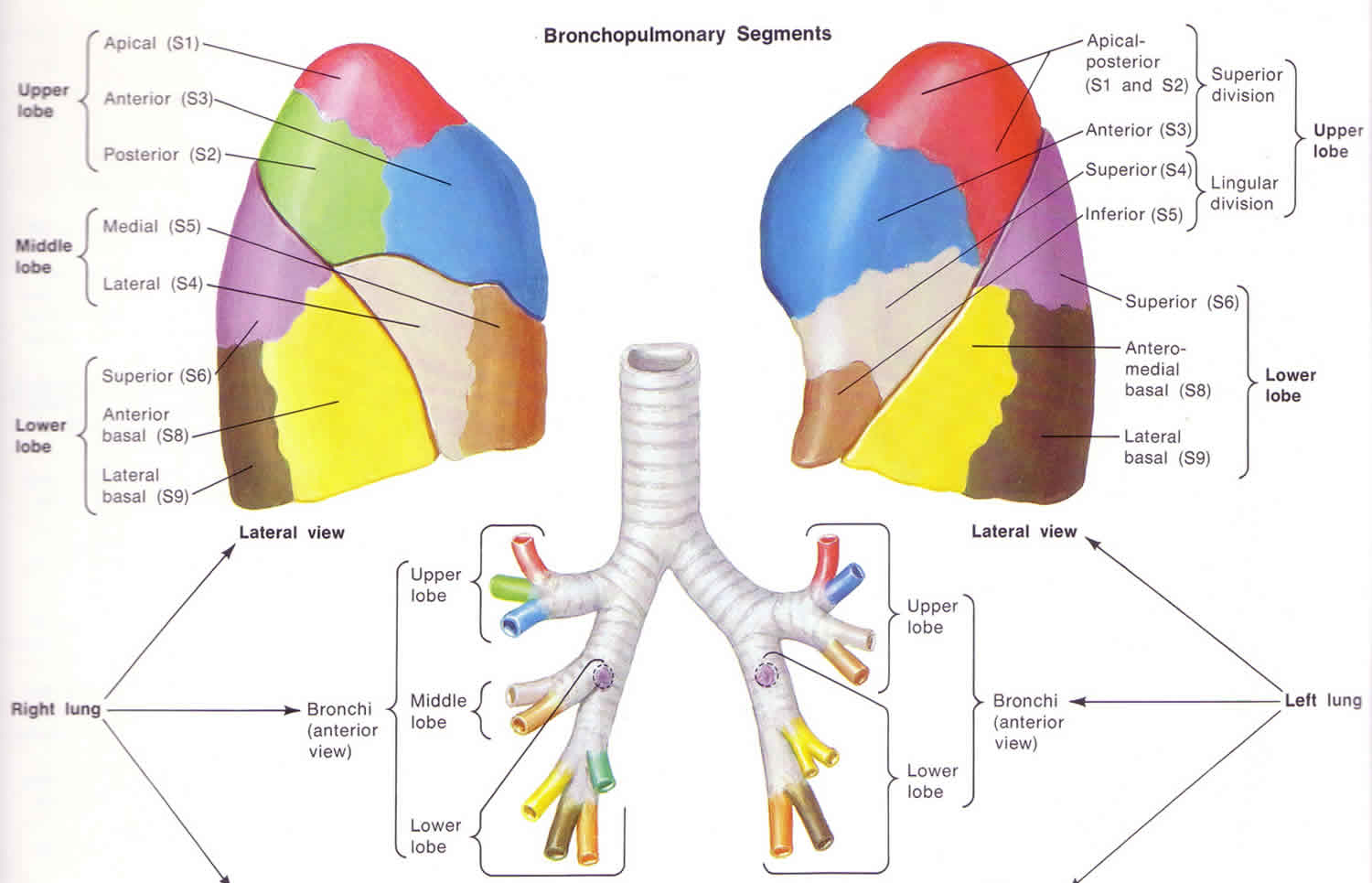
As shown in the Figure 1 below, the lungs are actually made up of several sub-sections known as ‘lobes’. Lobes are big areas of lung tissue divided by lines or ‘fissures’. The right lung has three lobes, called the superior (meaning top), middle and inferior (meaning bottom) lobes. The left lung only has two lobes, the superior and inferior lobes, partially because there is less room due to the presence of the heart in the left side of the chest. In a lobectomy, the surgeon will try and remove only one of these lobes, allowing the rest to remain functional. Removal of two lobes of the lung is called a ‘bilobectomy’ and removal of an entire lung is called a pneumonectomy.
Figure 1. Lung lobes
When is a pulmonary lobectomy used as treatment?
A lung lobectomy is usually used for treatment of non-small cell lung cancers (NSCLC), especially those that are caught early. The amount of lung that needs to be removed to prevent the spread of these tumors is affected by the location of the tumor as well as whether or not there are any ‘hilar lymph nodes‘ (that lie between the lobes) involved. Whether the surgeon decides to remove one lobe, two lobes or an entire lung will depend on the site of the tumor, the size of the tumor as well as the presence of any lymph nodes that appear to have tumor cells in them. If there are hilar nodes involved then a pneumonectomy may be necessary. Decisions may also depend on the general state of a person’s health, as a healthier patient may be able to cope with surgery better than someone who is very unwell.
When is a pulmonary lobectomy not used as treatment?
Pulmonary lobectomy is not suitable therapy for all lung cancers. For example if the cancer was caught very, early when it is small and has not spread, and if the patient is too weak to get through a lobectomy, then removal of an even smaller section of lung called a ‘segment’ may be used. The type of cancer is also important in deciding whether lobectomy is a suitable treatment or not. Lobectomy may not be as appropriate for the treatment of small-cell cancers, as they require far more aggressive treatment. Advanced lung cancers that have spread to other parts of the body may not be suitable candidates for lobectomy either, as there may not be sufficient benefit from it. However for some patients, especially those with isolated metastases (areas of spread) in their brain or adrenal glands, surgery may still have some benefit.
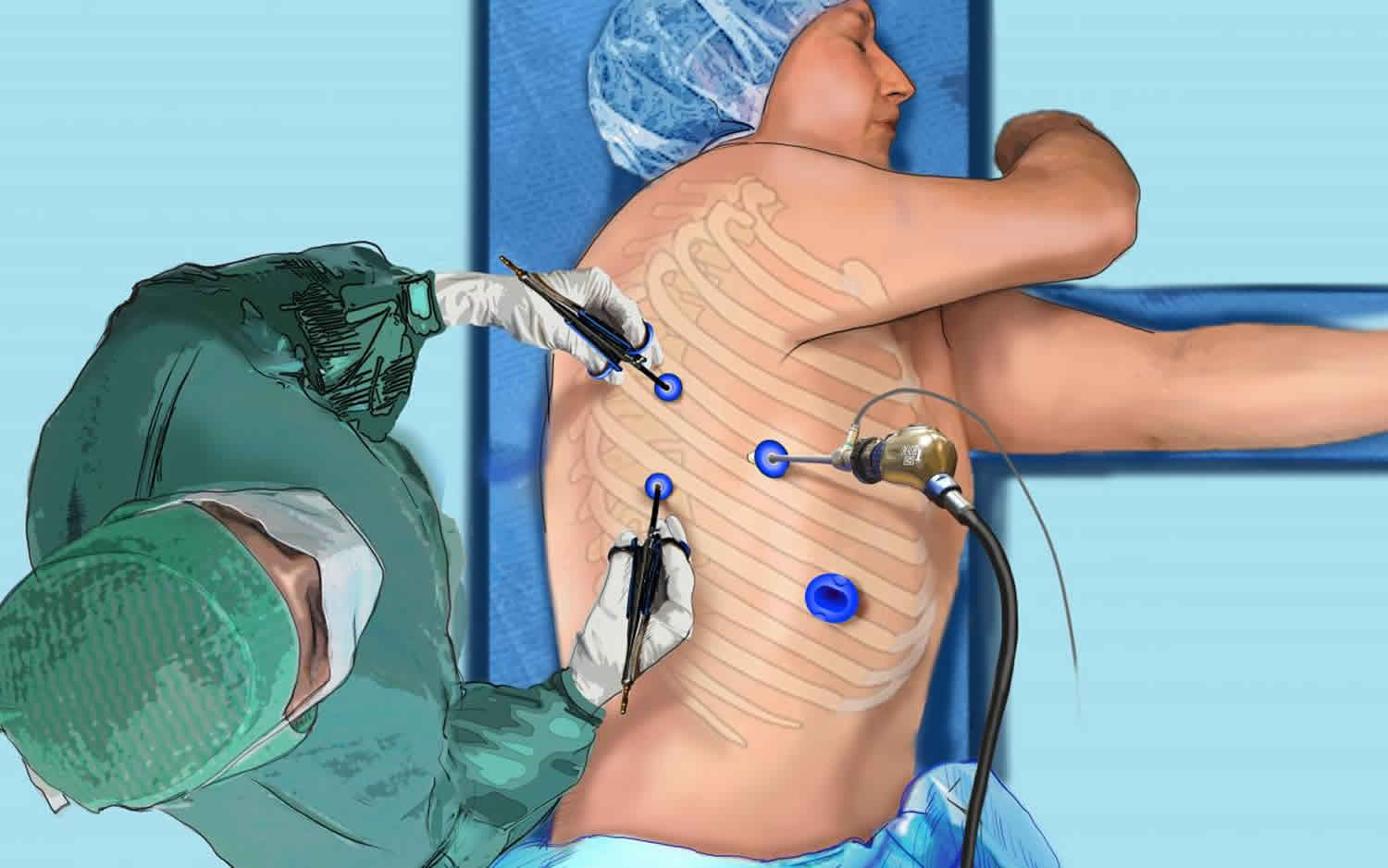
What is involved in a pulmonary lobectomy?
A pulmonary lobectomy will be done under general anesthesia. The exact details of where a surgeon will make an incision will depend on the location and size of the tumor. The surgeon will have to isolate the lobe of the lung by removing its blood supply as well as the bronchi (the airways that feed into the lobe) before the lobe itself is able to be removed. During the procedure, the surgeon may want to take what is known as a ‘frozen section’ from a lymph node, or an area surrounding the tumor. A frozen section is basically a relatively quick sample of tissue that can be examined by the pathologists on the spot so that they can assess whether or not the tumor has spread to the tissue that the surgeon has sampled. This can also be done to make sure that there is a good margin of healthy tissue that has been removed from the area around the tumor, ensuring all the tumor has been taken out.
What to expect before and after a pulmonary lobectomy
Before a lung lobectomy details about the procedure, the benefits, and the risks should all have been explained to you by your surgeon. If you have any questions regarding the operation you should feel free to ask them, as the more you know then the less worried you will be regarding the surgery. To decide whether lobectomy is the correct procedure, several investigations will have to be done to examine both the lesion itself as well as your general health. An X-ray and CT of the chest will help to assess the size, location and operability of the lesion. An ECG to assess the function of your heart will give the doctor a good idea of how your heart will cope with the strain of the operation and the suitability of a lobectomy. Lung Function Tests will give the doctor an idea about how well the rest of the lung is working. They need to know that they rest of the lungs are strong enough to take over the function of the removed lobe.
After the pulmonary lobectomy there will usually be a ‘drain’ attached to the site of the operation. This drain is a tube that sits in the operative site and will remove any blood or other fluid that may otherwise cause breathing problems. This will be removed once fluid has stopped draining. The doctors, nurses and physiotherapists on the ward will probably try and get you moving as soon as possible. This is because it not only helps your lungs to get better, but also stops the blood from pooling in your leg veins and helps prevent deep vein thrombosis. X-rays of your chest should be taken regularly while in hospital to make sure that they are inflating correctly, and there are no abnormalities. After the surgery you will be kept in hospital for observation until the doctors are satisfied that you are ready to leave. The length of stay in hospital varies from person to person, but should not be rushed.
Pulmonary lobectomy complications
A lung lobectomy is a major operation and while everything is done to try and prevent complications, it is inevitable that they will occasionally occur. The mortality rate for a pulmonary lobectomy is between 3 and 4%, which is significantly lower than for a pneumonectomy which is between 6 and 8%. Possible complications following a pulmonary lobectomy include:
- Cardiac arrhythmias: the heart beats irregularly and stops pumping blood as efficiently
- Bleeding
- Infection
- Bronchopleural fistulae: a connection forms between the lung and the surrounding area leading to air leakage
- Respiratory Insufficiency: if the rest of the lung cannot compensate for the loss of the lobe
- Pulmonary Embolism: a blood clot can lodge in the vessels of the lung, causing an area to lose blood supply
- Deep Vein Thrombosis: lying in bed for long periods after surgery can cause blood to pool in the veins of the legs and clot, causing a DVT
Thyroid lobectomy
Thyroid lobectomy also called hemi-thyroidectomy, is a surgery to remove one lobe (one half) of the thyroid.
The most common reason for thyroid lobectomy is to remove a thyroid nodule, which has been found to be suspicious through a thyroid biopsy (fine needle aspiration biopsy). Thyroid lobectomy may be recommended for the following biopsy results:
- Cancer (papillary cancer);
- Possible cancer (follicular neoplasm or atypical findings); or
- Inconclusive biopsy;
- Molecular marker testing of biopsy specimen which indicates a risk for malignancy.
Thyroid lobectomy may be also recommended for nodules with benign biopsy results if the nodule is large, if it continues to increase in size or if it is causing symptoms (discomfort, difficulty swallowing, etc.). Thyroid lobectomy is also an option for the treatment of hyperthyroidism (Grave’s disease or a “toxic nodule”, for large and multinodular goiters and for any goiter that may be causing symptoms.
For patients with papillary or follicular thyroid cancer, many, but not all, surgeons recommend total or near total thyroidectomy when they believe that subsequent treatment with radioactive iodine might be necessary. For patients with larger (>1.5 cm) or more invasive cancers and for patients with medullary thyroid cancer, local lymph node dissection may be necessary to remove possibly involved lymph node metastases.
A thyroid lobectomy (hemi-thyroidectomy) may be recommended for overactive solitary nodules or for benign one sided nodules that are causing local symptoms such as compression, hoarseness, shortness of breath or difficulty swallowing. A total or near – total thyroidectomy may be recommended for patients with Graves’ Disease or for patients with large multinodular goiters.
What to expect before a thyroid lobectomy
As for other operations, all patients considering thyroid surgery should be evaluated preoperatively with a thorough and detailed medical history and physical exam including cardiopulmonary (heart and lungs) evaluation. An electrocardiogram and a chest x-ray prior to surgery are often recommended for patients who are over 45 years of age or who are symptomatic from heart disease. Blood tests may be performed to determine if a bleeding disorder is present.
Importantly, any patient who has had a change in voice or who has had a previous neck operation (thyroid surgery, parathyroid surgery, spine surgery, carotid artery surgery, etc.) and/or who has had a suspected invasive thyroid cancer should have their vocal cord function evaluated routinely before surgery. This is necessary to determine whether the recurrent laryngeal nerves that control the vocal cord muscles are functioning normally.
Finally, in rare cases, if medullary thyroid cancer is suspected, patients should be evaluated for endocrine tumors that occur as part of familial syndromes including adrenal tumors (pheochromocytomas) and enlarged parathyroid glands that produce excess parathyroid hormone (hyperparathyroidism).
Thyroid lobectomy surgery
Once you have met with the surgeon and decided to proceed with surgery, you will be scheduled for your pre-operative evaluation. You should have nothing to eat or drink after midnight on the day before surgery and should leave valuables and jewelry at home.
The surgery usually takes 2-2½ hours, after which time you will slowly wake up in the recovery room. Surgery may be performed through a standard incision in the neck or may be done through a smaller incision with the aid of a video camera (minimally invasive video assisted thyroidectomy). Under special circumstances, thyroid surgery can be performed with the assistance of a robot through a distant incision in either the axilla or the back of the neck. There may be a surgical drain in the incision in your neck (which will be removed after the surgery) and your throat may be sore because of the breathing tube placed during the operation. Once you are fully awake, you will be allowed to have something light to eat and drink. Many patients having thyroid operations, especially after thyroid lobectomy, are able to go home the same day after a period of observation in the hospital. Some patients will be admitted to the hospital overnight and discharged the next morning.
Thyroid lobectomy recovery
Most surgeons prefer that patients limit extreme physical activities following surgery for a few days or weeks. This is primarily to reduce the risk of a postoperative neck hematoma (blood clot) and breaking of stitches in the wound closure. These limitations are brief, usually followed by a quick transition back to unrestricted activity. Normal activity can begin on the first postoperative day. Vigorous sports, such as swimming, and activities that include heavy lifting should be delayed for at least ten days to 2 weeks.
Once you have recovered from the effects of thyroid surgery, you will usually be able to do anything that you could do prior to surgery. Some patients become hypothyroid following thyroid surgery, requiring treatment with thyroid hormone. This is especially true if you had your whole thyroid gland removed. Generally, you will be started on thyroid hormone the day after surgery, even if there are plans for treatment with radioactive iodine.
Will I need to take a thyroid pill after my thyroid lobectomy?
The answer to this depends on how much of the thyroid gland is removed. If half (hemi) thyroidectomy or lobectomy is performed, there is an 80% chance you will not require a thyroid pill UNLESS you are already on thyroid medication for low thyroid hormone levels (e.g. Hashimoto’s thyroiditis) or have evidence that your thyroid function is on the lower side in your thyroid blood tests. If you have your entire gland removed (total thyroidectomy) or if you have had prior thyroid surgery and now are facing removal of the remaining thyroid (completion thyroidectomy) then you have no internal source of thyroid hormone remaining and you will definitely need lifelong thyroid hormone replacement.
Thyroid lobectomy complications
In experienced hands, thyroid surgery is generally very safe. Complications are uncommon, but the most serious possible risks of thyroid surgery include:
- bleeding in the hours right after surgery that could lead to acute respiratory distress;
- injury to a recurrent laryngeal nerve that can cause temporary or permanent hoarseness, and possibly even acute respiratory distress in the very rare event that both nerves are injured;
- damage to the parathyroid glands that control calcium levels in the blood, leading to temporary, or more rarely, permanent hypoparathyroidism and hypocalcemia.
These complications occur more frequently in patients with invasive tumors or extensive lymph node involvement, in patients undergoing a second thyroid surgery, and in patients with large goiters that go below the collarbone into the top of the chest (substernal goiter). Overall the risk of any serious complication should be less than 2%. However, the risk of complications discussed with the patient should be the particular surgeon’s risks rather than that quoted in the literature. Prior to surgery, patients should understand the reasons for the operation, the alternative methods of treatment, and the potential risks and benefits of the operation (informed consent).
Lobectomy brain
Brain lobectomy also called lesionectomy is a surgical removal of a lobe of the brain. Brain lobectomy is a surgery to remove a seizure focus involves removing the defined area of the brain where seizures originate. Brain lobectomy is the most common type of surgery for epilepsy and is appropriate only for focal seizures that originate in just one area of the brain. In general, people have a better chance of becoming seizure-free after surgery if they have a small, well-defined seizure focus. The most common type of lobectomy is a temporal lobe resection, which is performed for people with medial temporal lobe epilepsy. In such individuals one hippocampus (there are two, one on each side of the brain) is seen to be shrunken and scarred on an MRI scan.





{kind=link}