What is a pelvic exam
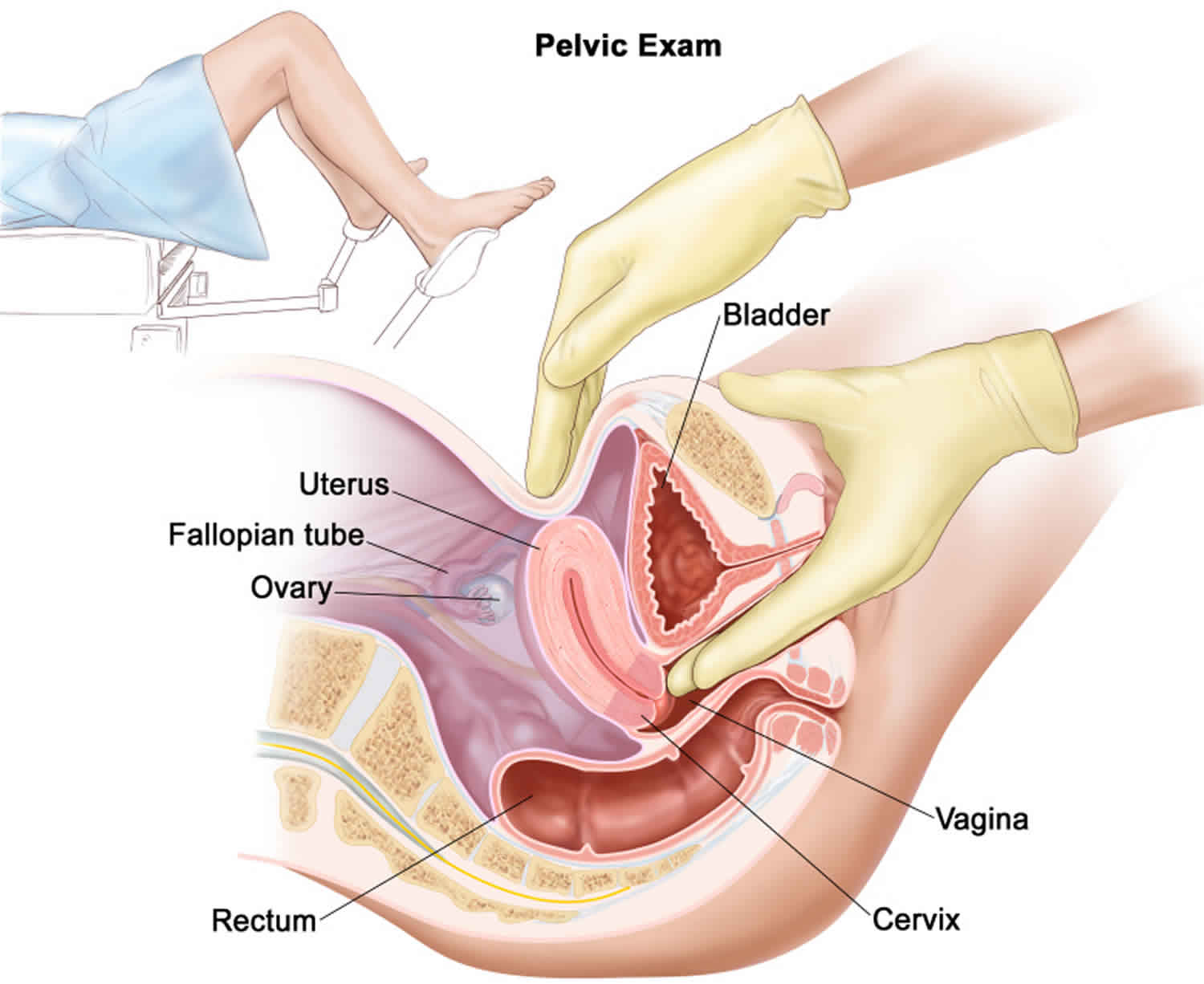
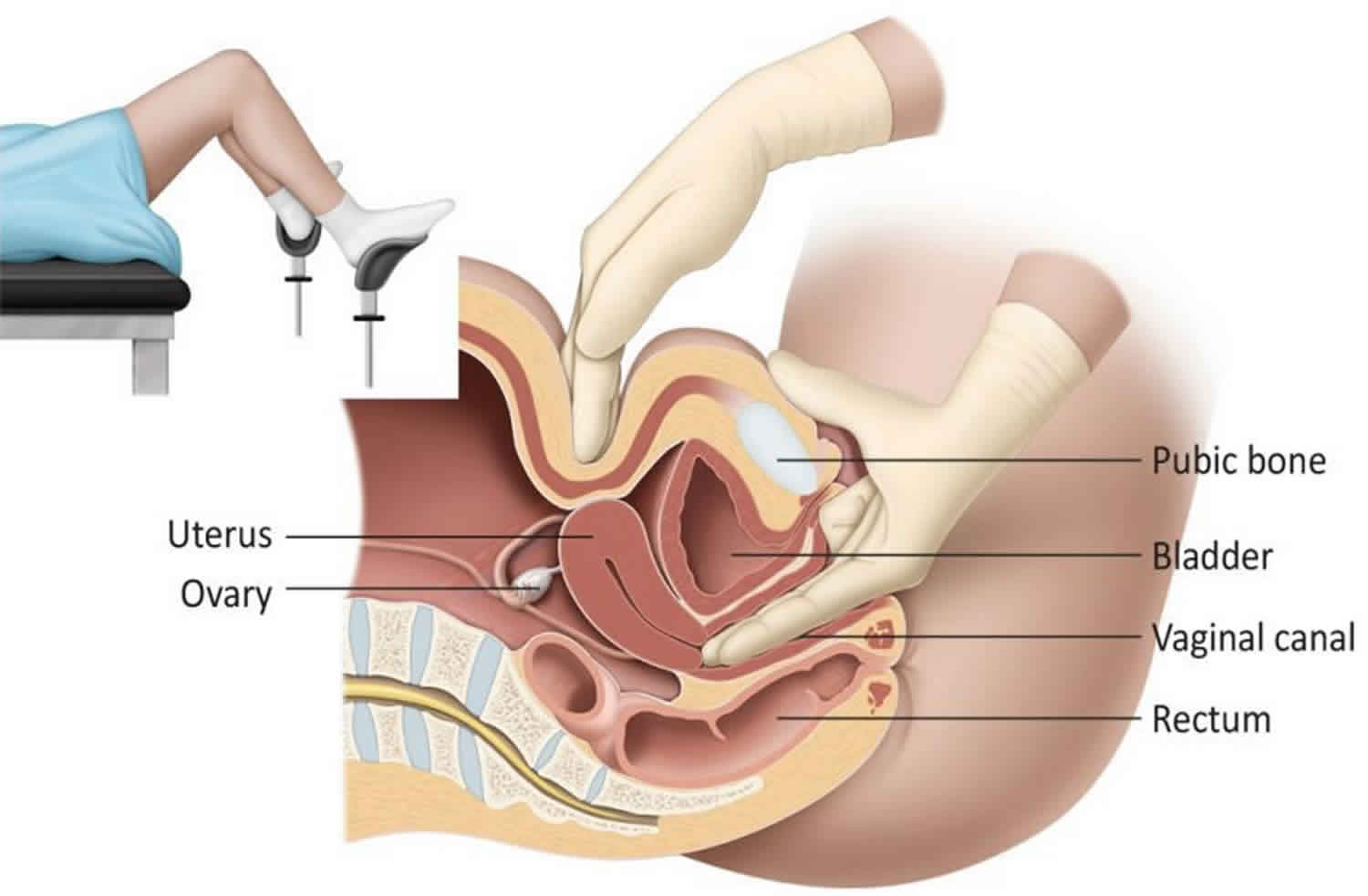
Pelvic exam also called gynecological exam is typically needed for females with gynecological complaints or for screening for cervical cytology at 21 years of age 1. During a pelvic exam, your doctor or nurse inserts one or two lubricated, gloved fingers of one hand into your vagina and presses on the lower abdomen with the other hand. This is done to feel the size, shape, and position of the uterus and ovaries. The vagina, cervix, fallopian tubes, and rectum are also checked.
You might have a pelvic exam as part of your regular checkup. Or your doctor might recommend a pelvic exam if you have symptoms such as unusual vaginal discharge or pelvic pain.
A pelvic exam usually lasts only a few minutes. Your doctor checks your vulva, vagina, cervix, ovaries, uterus, rectum and pelvis for any abnormalities. A Pap test, which screens for cervical cancer, is often performed during a pelvic exam.
Pelvic exam technique
The pelvic exam should start with an evaluation of the external vulva first. The clinician should look at the basic development of vulvar anatomy, symmetry, hair distribution, any swelling, bruising, erythema, rashes, lesions, discharge, growths and assessment of tenderness of any abnormalities. The labia should be palpated for tenderness or growths. This is done by placing the thumb on the perineal area with the index finger in the vaginal opening. The fingers are then moved along both labia feeling for nodules, abscesses, cysts, and tenderness 2.
Next is the internal speculum examination. First, the tips of the speculum should be lubricated with petroleum jelly or water. The speculum is held with the right hand with the index and middle fingers at the base of either blade holding them closed. The examiner should spread the labia slightly with the left hand to allow for easier insertion of the speculum. The speculum should then be inserted at an angle that guides insertion typically from 0 to 90 degrees and then immediately after insertion, rotating the speculum as necessary so that handle is pointing downward. Typically, women can accommodate a downward-angled handle right away but some narrower vaginas will require a slanted insertion. The inferior blade should be placed in the posterior fornix before opening. This can require a significantly posterior pathway to the speculum, especially in nulliparous women. Once the inferior blade is in the posterior fornix, the cervix should pop into view once the blades are opened like a duckbill. At this point, the cervix should be examined for color, lesions, discharge, blood and whether the external os looks open or closed. If the cervix is not visible right away, a bimanual exam may be necessary next to ascertain its location. A retroverted uterus may have anterior positioning of the cervix. Samples are taken at this time. To take out the speculum, the clinician should release the blades loosely while starting to slowly withdraw to avoid pinching the cervix and vaginal walls. At this time, the clinician should examine the vaginal wall for any irregularities.
The bimanual examination is next. Typically, if the examiner is right-handed, they will use their right hand internally and their opposite hand externally and vice versa. The examiner will use lubrication on their dominant hand on their two first fingers. The fingers are inserted into the vagina slowly. With either finger, locate the cervix. It may be necessary to push down and inferiorly with the non-dominant hand on the abdomen to push the cervix closer to the fingers. The external os and, as needed, the internal os are evaluated. The examiner will see if either the external or internal os are open with one finger. Cervical motion tenderness is elicited now as well. The non-dominant hand should help push the uterus between the hands to palpate its size and position. Next, both hands evaluate either adnexa by evaluating for masses and tenderness. This concludes the bimanual exam and the fingers are withdrawn.
Sometimes, clinicians will feel a rectovaginal examination is necessary to examine the rectovaginal septum and posterior cul-de-sac. The presence of hemorrhoids, polyps, and growths should be noted. The lubricated third digit is slowly inserted into the rectum to allow for relaxation of the sphincter to minimize discomfort. At the same time, the index finger is inserted into the vagina and both fingers are used to feel the rectovaginal septum and tenderness.
Pelvic exam during pregnancy
This is an exam of the pelvic organs, like the vagina, cervix, uterus and ovaries, to make sure they’re healthy. The cervix is the opening to your uterus that sits at the top of the vagina. If you have any problems in these organs, getting treatment before pregnancy may help prevent problems during pregnancy. Treatment also can help if you have fertility problems (problems getting pregnant).
Figure 1. Female pelvic exam
Why is a pelvic exam done?
You might need a pelvic exam:
- To assess your gynecological health. A pelvic exam often is part of a routine physical exam to find possible signs of ovarian cysts, sexually transmitted infections, uterine fibroids or early-stage cancer. Pelvic exams are also commonly performed during pregnancy. There is a lot of debate among experts regarding the recommended frequency of pelvic exams. Ask your doctor what he or she recommends.
- To diagnose a medical condition. Your doctor might suggest a pelvic exam if you’re experiencing gynecological symptoms such as pelvic pain, unusual vaginal bleeding, skin changes, abnormal vaginal discharge or urinary problems. A pelvic exam can help your doctor diagnose the causes of these symptoms. Your doctor might suggest additional diagnostic testing or treatment.
The following are complaints that would warrant a pelvic exam:
- Sexually transmitted infection testing or screening
- Screening exams by primary care physicians and gynecologists in females above the age of 21
- Pain
- Discharge
- Pregnancy or postpartum
- Infection
- Itching
- Swelling
- Bleeding
- Menstrual abnormalities
- Sexual development abnormalities
- Sexual or physical trauma
- Neurological conditions
- Incontinence
- Pelvic floor disorders
Pelvic exam vs Pap smear
A Pap smear, also called a Pap test, is a procedure to test for cervical cancer in women. A Pap smear involves collecting cells from your cervix — the lower, narrow end of your uterus that’s at the top of your vagina. Detecting cervical cancer early with a Pap smear gives you a greater chance at a cure. A Pap smear can also detect changes in your cervical cells that suggest cancer may develop in the future. Detecting these abnormal cells early with a Pap smear is your first step in halting the possible development of cervical cancer.
A Pap smear is a safe way to screen for cervical cancer. However, a Pap smear isn’t foolproof. It’s possible to receive false-negative results — meaning that the test indicates no abnormality, even though you do have abnormal cells.
A false-negative result doesn’t mean that a mistake was made. Factors that can cause a false-negative result include:
- An inadequate collection of cells
- A small number of abnormal cells
- Blood or inflammatory cells obscuring the abnormal cells
Although it’s possible for abnormal cells to go undetected, time is on your side. Cervical cancer takes several years to develop. And if one test doesn’t detect the abnormal cells, the next test most likely will.
Why is PAP smear done?
A Pap smear is used to screen for cervical cancer.
The Pap smear is usually done in conjunction with a pelvic exam. In women older than age 30, the Pap test may be combined with a test for human papillomavirus (HPV) — a common sexually transmitted infection that can cause cervical cancer. In some cases, the HPV test may be done instead of a Pap smear.
Who should have a Pap smear?
You and your doctor can decide when it’s time for you to begin Pap testing and how often you should have the test.
In general, doctors recommend beginning Pap testing at age 21.
How often should a Pap smear be repeated?
Doctors generally recommend repeating Pap testing every three years for women ages 21 to 65.
Women age 30 and older can consider Pap testing every five years if the procedure is combined with testing for HPV. Or they might consider HPV testing instead of the Pap test.
If you have certain risk factors, your doctor may recommend more-frequent Pap smears, regardless of your age. These risk factors include:
- A diagnosis of cervical cancer or a Pap smear that showed precancerous cells
- Exposure to diethylstilbestrol (DES) before birth
- HIV infection
- Weakened immune system due to organ transplant, chemotherapy or chronic corticosteroid use
- A history of smoking
You and your doctor can discuss the benefits and risks of Pap smears and decide what’s best for you based on your risk factors.
Who can consider stopping Pap smears?
In certain situations a woman and her doctor may decide to end Pap testing, such as:
- After a total hysterectomy. After a total hysterectomy — surgical removal of the uterus including the cervix — ask your doctor if you need to continue having Pap smears. If your hysterectomy was performed for a noncancerous condition, such as uterine fibroids, you may be able to discontinue routine Pap smears. But if your hysterectomy was for a precancerous or cancerous condition of the cervix, your doctor may recommend continuing routine Pap testing.
- Older age. Doctors generally agree that women can consider stopping routine Pap testing at age 65 if their previous tests for cervical cancer have been negative.
Discuss your options with your doctor and together you can decide what’s best for you based on your risk factors. If you’re sexually active with multiple partners, your doctor may recommend continuing Pap testing.
How you prepare for a Pap smear
To ensure that your Pap smear is most effective, follow these tips prior to your test:
- Avoid intercourse, douching, or using any vaginal medicines or spermicidal foams, creams or jellies for two days before having a Pap smear, as these may wash away or obscure abnormal cells.
- Try not to schedule a Pap smear during your menstrual period. It’s best to avoid this time of your cycle, if possible.
During the Pap smear
A Pap smear is performed in your doctor’s office and takes only a few minutes. You may be asked to undress completely or only from the waist down.
You’ll lie down on your back on an exam table with your knees bent. Your heels rest in supports called stirrups.
Your doctor will gently insert an instrument called a speculum into your vagina. The speculum holds the walls of your vagina apart so that your doctor can easily see your cervix. Inserting the speculum may cause a sensation of pressure in your pelvic area.
Then your doctor will take samples of your cervical cells using a soft brush and a flat scraping device called a spatula. This usually doesn’t hurt.
After the Pap smear
After your Pap smear, you can go about your day without restrictions.
Depending on the type of Pap testing you’re undergoing, your doctor transfers the cell sample collected from your cervix into a container holding a special liquid to preserve the sample (liquid-based Pap test) or onto a glass slide (conventional Pap smear).
The samples are transferred to a laboratory where they’re examined under a microscope to look for characteristics in the cells that indicate cancer or a precancerous condition.
Ask your doctor about when you can expect the results of your test.
Pap Smear Results
A Pap smear can alert your doctor to the presence of suspicious cells that need further testing.
Normal results
If only normal cervical cells were discovered during your Pap smear, you’re said to have a negative result. You won’t need any further treatment or testing until you’re due for your next Pap smear and pelvic exam.
Abnormal results
If abnormal or unusual cells were discovered during your Pap smear, you’re said to have a positive result. A positive result doesn’t mean you have cervical cancer. What a positive result means depends on the type of cells discovered in your test.
Here are some terms your doctor might use and what your next course of action might be:
- Atypical squamous cells of undetermined significance (ASCUS). Squamous cells are thin and flat and grow on the surface of a healthy cervix. In the case of ASCUS, the Pap smear reveals slightly abnormal squamous cells, but the changes don’t clearly suggest that precancerous cells are present. With the liquid-based test, your doctor can reanalyze the sample to check for the presence of viruses known to promote the development of cancer, such as some types of human papillomavirus (HPV). If no high-risk viruses are present, the abnormal cells found as a result of the test aren’t of great concern. If worrisome viruses are present, you’ll need further testing.
- Squamous intraepithelial lesion (SIL). This term is used to indicate that the cells collected from the Pap smear may be precancerous. If the changes are low grade, it means the size, shape and other characteristics of the cells suggest that if a precancerous lesion is present, it’s likely to be years away from becoming a cancer. If the changes are high grade, there’s a greater chance that the lesion may develop into cancer much sooner. Additional diagnostic testing is necessary.
- Atypical glandular cells. Glandular cells produce mucus and grow in the opening of your cervix and within your uterus. Atypical glandular cells may appear to be slightly abnormal, but it’s unclear whether they’re cancerous. Further testing is needed to determine the source of the abnormal cells and their significance.
- Squamous cell cancer or adenocarcinoma cells. This result means the cells collected for the Pap smear appear so abnormal that the pathologist is almost certain a cancer is present. “Squamous cell cancer” refers to cancers arising in the flat surface cells of the vagina or cervix. “Adenocarcinoma” refers to cancers arising in glandular cells. If such cells are found, your doctor will recommend prompt evaluation.
If your Pap smear is abnormal, your doctor may perform a procedure called colposcopy using a special magnifying instrument (colposcope) to examine the tissues of the cervix, vagina and vulva.
Your doctor also may take a tissue sample (biopsy) from any areas that appear abnormal. The tissue sample is then sent to a laboratory for analysis and a definitive diagnosis.
How you prepare for a pelvic exam
You don’t need to do anything special to prepare for a pelvic exam. For your own comfort, you might want to schedule your pelvic exam on a day when you don’t have your period. Also, you might be more comfortable if you empty your bladder before the exam.
If you have questions about the exam or its possible results, consider writing down your questions and taking them with you to the appointment so that you don’t forget to ask them.
Pelvic exam procedure
A pelvic exam is done in your doctor’s office and takes only a few minutes. You’ll be asked to change out of your clothes and into a gown. You might be given a sheet to wrap around your waist for added privacy. Before performing the pelvic exam, your doctor might listen to your heart and lungs and perform an abdominal, back and breast exam.
You’ll lie on your back on an exam table with your knees bent and your feet placed on the corners of the table or in supports (stirrups). You’ll be asked to slide your body toward the end of the table and let your knees fall open.
A pelvic exam generally includes:
- External visual exam. First, your doctor looks at your vulva, checking for irritation, redness, sores, swelling or other abnormalities.
- Internal visual exam. Next, your doctor uses a speculum — a plastic or metal-hinged instrument shaped like a duck’s bill — to spread open your vaginal walls and see your vagina and cervix. The speculum might be warmed before it’s inserted to make it more comfortable for you. Inserting and opening the speculum causes pressure that can be uncomfortable for some women. Relax as much as possible to ease discomfort, but tell your doctor if you’re in pain.
- The speculum comes in a variety of sizes and types. Metal specula are not disposable and need sterilization between each use. Plastic specula are disposable and individually used. The Graves speculum is the most commonly used speculum; it has 2 handles and a fixed base. The handles can either be opened like a duckbill or spread further apart with the mechanism on the handle. The Pederson speculum is similar to a Graves speculum but with narrower blades for pediatric patients or to accommodate a narrower vagina. Many speculums are designed with a light source. If the speculum is not designed with a light source, ensure proper lighting with an adjustable lamp. Simple room lighting will not be adequate for the examination.
- Pap test. If your pelvic exam includes a Pap test (Pap smear), your doctor will swipe a small wand to collect a sample of your cervical cells before removing the speculum.
- Physical exam. Because your pelvic organs, including your uterus and ovaries, can’t be seen from outside your body, your doctor needs to feel (palpate) your abdomen and pelvis for this part of the exam. Your doctor will insert two lubricated, gloved fingers into your vagina with one hand, while the other hand presses gently on the outside of your lower abdomen. During this part of the exam, your doctor will check the size and shape of your uterus and ovaries, noting any tender areas or unusual growths. After the vaginal exam, your doctor will insert a gloved finger into your rectum to check for tenderness, growths or other irregularities.
Your doctor should tell you exactly what he or she is doing at each step so that nothing comes as a surprise to you.
After the pelvic exam
After the pelvic exam is over, you can get dressed. Then, your doctor will discuss the results of your exam.
Results of the pelvic exam
Your doctor can usually tell you immediately if the exam revealed anything unusual. Pap test results might take a few days. Your doctor will discuss with you any next steps, additional tests, follow-up or treatment that you need.
Your pelvic exam is a good time to talk to your doctor about your sexual or reproductive health. If you have questions, be sure to discuss them during your visit.
Pelvic exam possible complications
Pelvic exam complications can be encountered in a number of special circumstances. In women with atrophic vaginitis, the speculum exam may be very painful and liberal lubrication, and a narrow speculum is recommended for these patients.
There may be challenges when encountering a patient with a history of sexual trauma; a pelvic examination may trigger anxiety or post-traumatic stress disorder. Consent must be acquired. Especially during these examinations, thorough explanations of the procedure should be emphasized. Mental health counseling, anxiolytics, and various alternatives to the exam can be suggested such as only removing the underwear, having a chaperone present, self-insertion of the speculum, offering the option to have a female provider present or having a friend or family member in the room for comfort. It should be stressed that the examiner can stop the exam at any time when requested by the patient 3.
References- Qaseem A, Humphrey LL, Harris R, Starkey M, Denberg TD., Clinical Guidelines Committee of the American College of Physicians. Screening pelvic examination in adult women: a clinical practice guideline from the American College of Physicians. Ann. Intern. Med. 2014 Jul 01;161(1):67-72.
- Bates CK, Carroll N, Potter J. The challenging pelvic examination. J Gen Intern Med. 2011 Jun;26(6):651-7
- Bates CK, Carroll N, Potter J. The challenging pelvic examination. J Gen Intern Med. 2011 Jun;26(6):651-7.





{kind=link}