What is ring avulsion
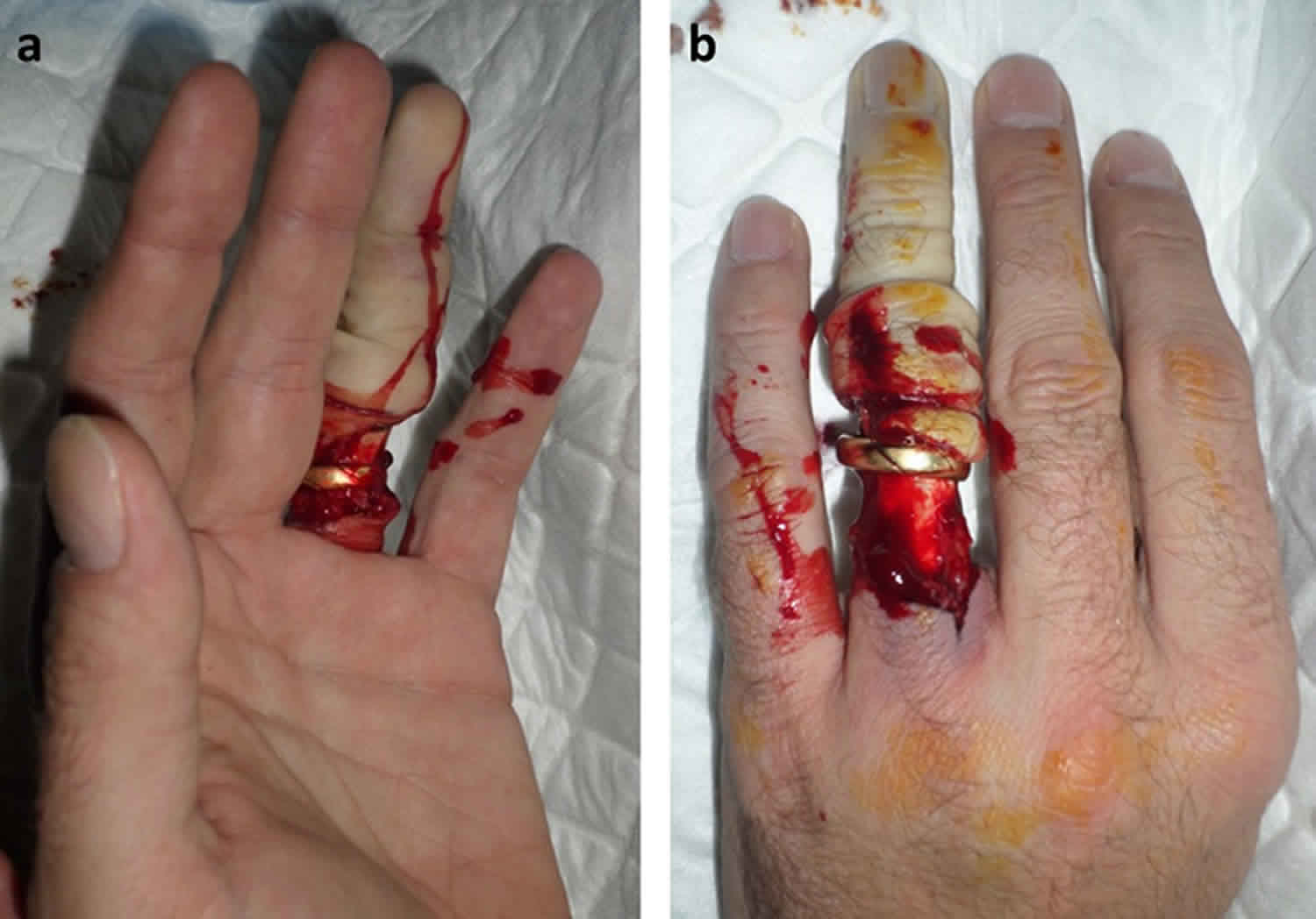
Ring avulsion injury is sustained by a sudden force pulling a ring from a finger, usually worn on the 4th or ring finger, is caught on machinery or a protruding immobile object 1. Ring avulsion represents a spectrum of soft tissue, neurovascular, tendon, and bone injury. Ring avulsion injury result in severe injury ranging from circumferential soft-tissue laceration to complete amputation. Ring avulsion injury may involve crushing, shearing and avulsion of neurovascular structures along with additional flexor tendon, and bony injuries 2.
Urbaniak et al. 3 classified ring avulsion injuries into 3 classes based on the circulatory status:
- Ring avulsion Class I—circulation adequate;
- Ring avulsion Class II—circulation inadequate; and
- Ring avulsion Class III—complete degloving or complete amputation.
Nissenbaum 4 subsequently modified class II (circulation inadequate) adding class IIA for isolated arterial injuries. Kay et al. 5 described an alternative classification emphasizing the presence of skeletal injury, reflecting the difference in treatment required and predicted functional outcome. In cases where there was inadequate circulation, they were divided into the absence of (class II) or presence of (class III) fracture or joint injury with only inadequate arterial (a) or venous (v) circulation. Circulation adequate injuries were still considered class I and complete amputations or gloving as class IV. Classification systems are useful to stratify an approach to recommended treatment and to predict possible outcomes, which is of value when counseling patients preoperatively.
Ring finger avulsion classifications
Urbaniak classification 3:
- Class I: Avulsion injury with adequate circulation
- Class II: Avulsion injury with inadequate circulation
- Class III: Complete degloving or complete amputation
Nissenbaum modification of Urbaniak classification 4:
- Class IIa: Avulsion injury with inadequate circulation (only arteries injured)
Kay classification 5:
- Class I: Adequate circulation, with or without skeletal injury
- Class II: Inadequate circulation (arterial and venous), no skeletal injury
- Class III: Inadequate circulation (arterial and venous), fracture of joint injury present
- Class IV: Complete amputation
- a. Arterial circulation inadequate only
- b. Venous circulation inadequate only
The most severe forms of ring avulsion injury involve vascular compromise or complete amputation, associated with tendon injury and/or fracture. Optimal management will vary depending on the pattern of injury, status of the amputated part, and functional requirements and expectation of individual patients.
Advances in microsurgery have made salvage of amputated fingers a commonly performed procedure. Survival of replanted digits has become fairly reliable, with survival rates estimated to be 80 – 90 percent in the literature 6. Avulsion amputations are a particularly difficult problem to treat due to the extent of damage sustained by skin, nerves, and vessels. As surgeons continued to push the boundaries of microsurgery, novel techniques were proposed to manage the difficulties of salvaging avulsed digits. Reconstruction of vessels with long vein grafts 7, venous flow-through flaps 8, or transfer of vessels from adjacent fingers 9 enhanced survival of the avulsed digit.
Ring avulsion prevention
Ring avulsion isn’t possible if you don’t wear any rings. Avoid wearing your ring in situations where the ring can get caught on something, such as heavy machinery. You should take your rings off before you play sports or use any exercise equipment, too.
Ring avulsion treatment
As for any hand injury, appropriate first aid is given, and the patient is stabilized and given adequate analgesia. The amputated part, if completely avulsed, is preserved appropriately and the wounds assessed. Radiographs should be taken of the injured digit and the amputated part. Admission for elevation, analgesia, and intravenous antibiotics should be initiated, and the patient counseled for appropriate urgent surgical management. Urbaniak 3 suggested management of injuries based on their class. Class I injuries require repair of soft tissues and fixation of any bone injury. Class II injuries (inadequate circulation) require urgent operative assessment and possible revascularization. Urbaniak et al. 3 supported revision amputation for class III injury (complete degloving/amputation) due to poor functional outcome. Avulsion amputation poses particular problems due to long-segment neurovascular bundle injury involving crush and shearing forces. Microsurgery has allowed for revascularization and replantation, along with local flap, pedicle flap, and graft coverage for further reconstruction. More recent literature also recommends attempting replantation in complete finger avulsion injuries with a preserved proximal interphalangeal (PIP) joint and flexor digitorum superficialis tendon insertion 10.
Urbaniak class I avulsion injuries (ie, adequate circulation) have good reported functional outcomes, with only slight reduction in proximal interphalangeal (PIP) joint motion; one study quoting an average of 94.4° (normal = 100°) 1. Outcomes for Urbaniak class II injuries (ie, avulsion with inadequate circulation) depend on the structures involved. Average proximal interphalangeal (PIP) joint motion of 88.3° has been reported. Proximal interphalangeal (PIP) joint motion is worse if the flexor tendon is concomitantly injured and more so if there is a fracture. Patients with class II injuries have been shown to preserve or regain protective sensation: 7- to 10-mm static 2-point discrimination 1. In Urbaniak class III injury (complete avulsion), mean survival for reimplantation is 78% compared with 80% to 90% in finger reimplantation following amputation in general. An average total active motion, following replantation for class III injury, has been found to be 177° versus 199° in class II injuries. A normal range is 260° to 270°. For comparison, average recovered total active motion after isolated zone II flexor tendon repair is reported as 229°. The mean 2-point discrimination in patients after class III injury is 10 mm 10.
References- Crosby N, Hood J, Baker G, Lubahn J. Ring injuries of the finger: long-term follow-up. Hand (N Y). 2014;9(3):274–281. doi:10.1007/s11552-014-9651-9 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4152427
- Jones M, Gujral S. Ring Avulsion Injuries. Eplasty. 2016;16:ic5. Published 2016 Feb 10. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4753839
- Urbaniak JR, Evan JP, Bright DS. Microvascular management of ring avulsion injuries. J Hand Surg. 1981;5A:25–30
- Nissenbaum M. Class IIA ring avulsion injuries: an absolute indication for microvascular repair. J Hand Surg. 1984;9A:810–5
- Kay S, Werntz J, Walf TW. Ring avulsion injuries: classification and prognosis. J Hand Surg. 1989;12A:204–13
- Medling BD, Bueno RA, Jr, Russell RC, Neumeister MW. Replantation outcomes. Clin Plast Surg. 2007;34:177–185
- Hyza P, Vesely J, Drazan L, Stupka I, Ranno R, Castagnetti F. Primary vein grafting in treatment of ring avulsion injuries: a 5-year prospective study. Ann Plast Surg. 2007;59:163–167
- Brooks D, Buntic RF, Taylor C. Use of the venous flap for salvage of difficult ring avulsion injuries. Microsurg. 2008;28:397–402
- Adani R, Castagnetti C, Busa R, Caroli A. Transfer of vessels in the management of thumb and ring avulsion injuries. Ann Acad Med Singap. 1995;24:51–57
- Sears ED, Chung KC. Replantation of finger avulsion injuries: a systematic review of survival and functional outcomes. J Hand Surg Am. 2011;36(4):686–94





{kind=link}