Sebaceous carcinoma
Sebaceous carcinoma also called sebaceous gland carcinoma, sebaceous gland adenocarcinoma, or meibomian gland carcinoma, is a rare aggressive skin cancer that begins in an oil gland (sebaceous gland) in your skin. Sebaceous carcinoma is considered an aggressive skin cancer because it can spread. Sebaceous carcinoma most often affects the eyelids and may cause a lump or skin thickening.
Sebaceous carcinoma may begin as a painless lump or thickening of skin on the eyelid. As it grows, the cancer may bleed or ooze. Sebaceous carcinoma that occurs on other parts of the body usually appears as a yellowish lump that may bleed.
Sebaceous carcinoma may begin elsewhere. It can develop in any sebaceous gland. You have sebaceous glands on most areas of your skin. Sebaceous carcinoma tends to develop in and around the eyes because you have the greatest number of sebaceous glands in that area.
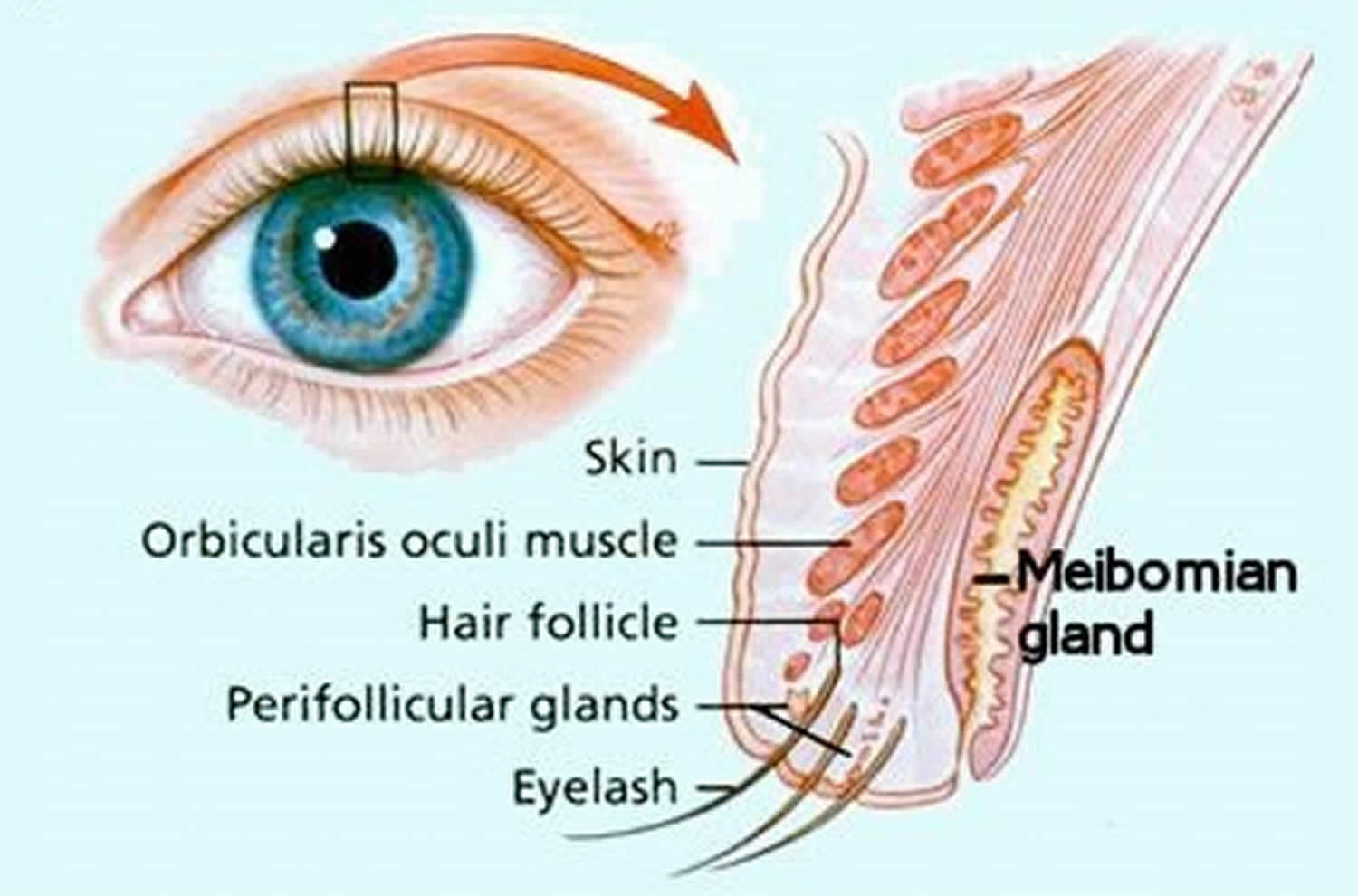
When this cancer begins in an eyelid, a dermatologist may refer to it as a meibomian gland carcinoma. This is a unique type of sebaceous gland found in the eyelids.
Ocular sebaceous carcinomas affect adults. It occurs more frequently in Asian populations than Caucasians and is more common in women than in men, particularly those around 60 to 80 years of age. In patients with a predisposing genetic syndrome, it may be diagnosed at a younger age.
Extraocular sebaceous carcinomas occur mainly in older adults and without predilection for male or female. Sebaceous carcinoma can begin earlier or later. According to research studies, sebaceous carcinoma has been diagnosed in a 3-year-old child and people in their 90s.
Sebaceous carcinoma can spread to other areas of the body and may be difficult to treat.
Sebaceous carcinoma treatment usually involves surgery to remove the cancer. Radical surgical excision with frozen section control by either a standard method or Mohs micrographic surgery is the most common and effective method of treatment. Approximately, 30% of sebaceous carcinomas recur after resection.
Radiation therapy should only be used in patients unable or willing to undergo surgery.
Found early and treated, treatment is often successful. It is helpful to know that:
- Most sebaceous carcinomas begin on an eyelid.
- You may notice a painless, round, firmly implanted tumor on your upper or lower eyelid.
- Sometimes you have to pull gently on your eyelid to see the tumor.
Other growths can develop on and around the eyelids. Most growths are benign (not cancer). If you notice a growth on your eyelid that remains despite treatment, you should make an appointment to see a dermatologist. The sooner this cancer is diagnosed and treated the better the outcome. If sebaceous carcinoma spreads, it can be deadly.
Figure 1. Sebaceous carcinoma (ocular sebaceous carcinoma)

Figure 2. Extraocular sebaceous carcinoma

What is a sebaceous gland?
Sebaceous glands are small glands connected to hair follicles in the skin. They are located in any hair-bearing region of the body but are most numerous on the skin of the scalp and face. The glands are responsible for producing sebum which is an oily substance that keeps hair and skin moisturized.
Figure 3. Sebaceous glands
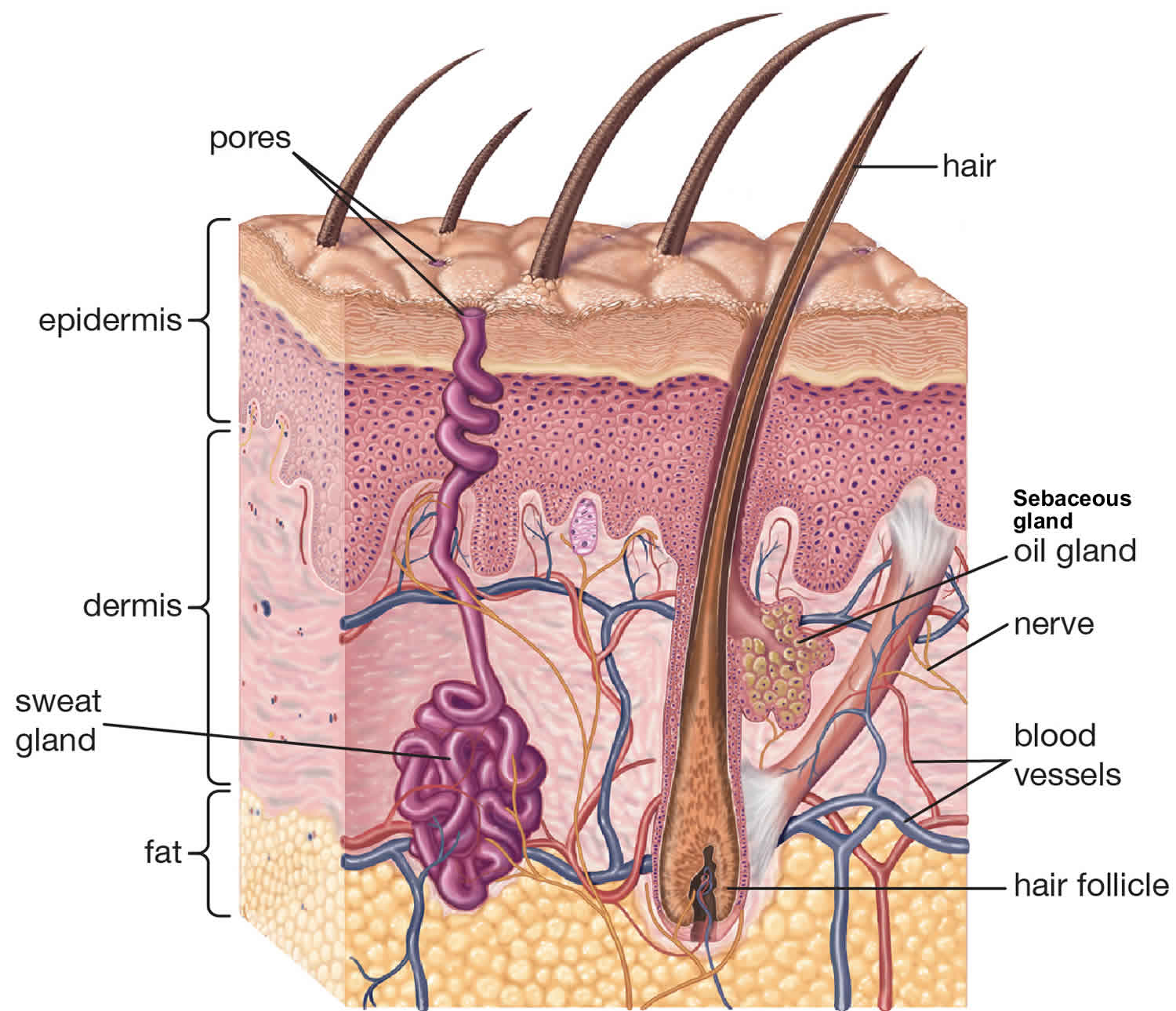
Figure 4. Meibomian gland
Sebaceous carcinoma causes
The exact cause of sebaceous carcinoma is unclear. Because most sebaceous carcinomas develop on the head and neck, the sun may play a role in causing this rare skin cancer.
If you notice a growth on your eyelid, it is important that you see a dermatologist for a diagnosis.
The following have been reported to possibly increase the risk of sebaceous carcinomas:
- Underlying Muir-Torre or Lynch syndrome
- Previous radiation therapy to the area for a variety of benign and malignant conditions, such as retinoblastoma
- History of oral thiazide diuretic use
- Mutations to the tumour suppressor gene p53
- Immunosuppression.
Risk factors for sebaceous carcinoma
Anything that increases your risk of getting a disease is a risk factor. For sebaceous carcinoma, age is a common risk factor. Other risk factors for sebaceous carcinoma are:
- Weakened immune system: A weakened immune system greatly increases the risk for sebaceous carcinoma. The immune system may be weakened by:
- Medicine taken to prevent the body from rejecting a transplanted organ.
- Certain medical conditions, such as human immunodeficiency virus (HIV) or cancer.
- Some medications used to treat psoriasis or arthritis.
- Radiation treatments to the head or neck: People who received these radiation treatments as a child have been diagnosed with this rare skin cancer in their 60s and 70s. sebaceous carcinoma also develops in children who receive radiation treatments for retinoblastoma, a cancer that develops in the eye.
- Asian heritage: sebaceous carcinoma on the eyelid may be more common in Asians. Some studies suggest this. Others studies have not found this to be true.
- Muir-Torre syndrome: This is a rare medical condition. Many people do not know they have this condition until they are diagnosed with sebaceous carcinoma. People who have Muir-Torre syndrome have a higher risk of developing some cancers. The risk is greatest for developing a type of colon cancer. Your doctor can talk with you about testing to find colon cancer in its earliest stage.
Sebaceous carcinoma symptoms
Sebaceous carcinoma most commonly develops from the meibomian glands which are located mostly in the upper but also in the lower eyelids. Clinical features of ocular sebaceous carcinoma include:
- Small, erythematous or yellowish, firm, deep-seated, slowly enlarging nodule on the upper eyelid.
- Lesions occur on the upper eyelid 2–3 times more commonly than on the lower eyelid.
- The lesion is often mistaken for chalazion (a benign inflammation of the meibomian gland).
- As the carcinoma grows it may spread onto the conjunctiva, where it can be mistaken for keratoconjunctivitis or blepharoconjunctivitis.
- In advanced cases, the spread of the lesion may lead to both upper and lower lid lesions and cause loss of eyelashes (madarosis), ulceration and distorted vision.
- Undiagnosed or late diagnoses can lead to metastases (spread) to lymph nodes and parotid glands.
The diagnosis of ocular sebaceous carcinoma is often delayed by months to years (mean delay from disease onset to diagnosis ranges from 1–3 years) because numerous other inflammatory conditions, autoimmune diseases, infectious processes and other tumours mimic the condition.
Extraocular sebaceous carcinoma accounts for about 25% of sebaceous carcinomas. These tumors mostly occur around the head and the neck. Other sites where these tumors have been found include the genitals, ear canal, breasts, trunk and oral cavity.
The clinical presentation of extraocular lesions is non-specific; they typically appear as a pink to a yellow-red nodule of varying sizes.
Sebaceous carcinoma complications
Sebaceous carcinoma, although rare, is an aggressive and potentially dangerous tumor that can lead to significant morbidity and mortality. The overall mortality rate is 5–10% because of inherent tumor factors, or delayed diagnosis and treatment.
Factors for a poorer prognosis include delay in diagnosis of greater than 6 months, tumor diameter greater than 1 cm, and both upper and lower eyelid involvement.
Sebaceous carcinoma diagnosis
Tests and procedures used to diagnose sebaceous carcinoma include:
- Skin examination. Your doctor will carefully inspect your skin to understand your condition.
- Eye examination. An eye doctor (ophthalmologist) will carefully examine your eyelid and your eye to look for signs that cancer has spread to the tissue (conjunctiva) that covers the inside of your eyelid and the white of your eye (sclera).
- Skin biopsy. Your doctor will remove a small amount of tissue for testing. Specialized laboratory tests can determine if cancer cells are present.
Sebaceous carcinoma may be suspected clinically. Dermoscopy may reveal typical irregular yellowish lobules and irregular linear blood vessels.
Definitive diagnosis is based upon patient history, adequate surgical biopsy and the combined knowledge of a pathologist, ophthalmologist and dermatologist.
Immunohistochemistry stains may be used to determine the likelihood of an underlying genetic syndrome.
How do doctors know if the sebaceous skin cancer has spread?
Before creating a treatment plan for sebaceous carcinoma, your dermatologist or ophthalmologist wants to answer these questions:
- Has the cancer spread to the lymph nodes?
- Has the cancer spread to other parts of the body?
To find out whether the cancer has spread, you may need more medical tests, such as:
- Fine needle aspiration biopsy: This test is used to obtain a sample from an internal organ, lymph node, or tissue beneath the skin. To perform this test, a surgeon (or other specially trained doctor) inserts a small, hollow needle. Once in the right place, the doctor uses the needle to remove a small sample. The sample will be checked for cancer cells.
- Lymph node biopsy: The results from this procedure can tell doctors if the cancer has spread to a patient’s lymph nodes. During this surgery, one or more lymph node is removed. The removed lymph node(s) is checked for cancer cells.
- Other medical tests: Other tests that can check for cancer include a colonoscopy, blood tests, and chest x-ray.
Sebaceous carcinoma treatment
Sebaceous carcinoma treatment typically involves surgery to remove the cancer. Radiation therapy and experimental treatments may be options if you can’t undergo surgery.
Treatment is typically led by a doctor who treats skin diseases (dermatologist) who may consult with other experts, such as eye doctors (ophthalmologists) and doctors who use radiation to treat cancer (radiation oncologists). Other experts may be included, depending on your situation.
Treatment options may include:
- Surgery to remove the cancer. Your doctor may recommend a procedure to remove the cancer and some of the healthy tissue that surrounds it (excisional surgery with a normal margin of tissue). A specialist will examine the edges of the tissue to make sure no cancer cells are present. This makes it more likely that all of the cancer cells are removed during surgery.
- Mohs surgery. Mohs surgery is a specialized type of surgery that involves progressively removing thin layers of cancer-containing skin until only cancer-free tissue remains. After each layer of skin is removed, it’s examined for signs of cancer. The process continues until there are no signs of cancer along the edge of the removed tissue. Your Mohs surgeon may refer to this edge as the “margin.” When the Mohs surgeon no longer sees cancer cells along the edges, the surgeon may tell you that the “margins look clear.” This technique may be helpful if your cancer is located in a spot that makes taking a wide margin of healthy tissue difficult, such as on your eyelid or on your face. After the cancer surgery, some patients need reconstructive surgery. This surgery is often performed immediately after the cancer surgery. One study followed 18 patients who had sebaceous carcinoma on an eyelid. All patients had Mohs surgery. Most (16 out of 18) patients were cancer-free after an average follow-up of 37 months.
- Surgery to remove lymph nodes: When the cancer spreads to the lymph nodes, the patient may have surgery to remove the affected lymph nodes. Reports of patients surviving for many years after such surgery have been made.
- Radiation therapy. Radiation therapy uses powerful energy beams, such as X-rays and protons, to kill cancer cells. For sebaceous carcinoma, radiation therapy may be used alone, or it can be used after surgery to kill any cancer cells that might remain. Radiation therapy is usually not the first choice for treating sebaceous carcinoma. This treatment may be an option for:
- Easing a patient’s pain if the cancer has spread.
- Treating patients who refuse or cannot withstand surgery.
- Treating patients who have had surgery but may still have some cancer.
- Clinical trials. Some patients are encouraged to join a clinical trial. A clinical trial is a type of research study. The purpose of a clinical trial is to study how well a new treatment or a new way of treating a disease works. For some patients, joining a clinical trial may be the best treatment option. Ask your doctor whether you’re eligible to participate in a clinical trial.
Sebaceous carcinoma prognosis
When found early and treated, the prognosis is good. It is important to keep in mind that sebaceous carcinoma is an aggressive cancer. This cancer can return after treatment. For these reasons, it is essential to keep all follow-up appointments with your doctors.
When found early and treated, sebaceous carcinoma has a high survival rate. The best way to find this cancer early is to return for check-ups. Your dermatologist will tell you how often you should return for check-ups. It is essential to keep all appointments.





{kind=link}