
Sensitive tooth
Sensitive tooth is also known as “dentin hypersensitivity”, is defined as “short, sharp pain arising from exposed dentin in response to stimuli typically thermal, chemical, tactile, osmotic, or even related to evaporation (air jet) and which cannot be ascribed to any other form of dental defect or disease” 1. When you have sensitive teeth, certain activities, such as brushing, eating and drinking, can cause sharp, temporary pain in your teeth. A layer of enamel, the strongest substance in your body, protects the crowns of healthy teeth (see Figure 1). A layer called cementum protects the tooth root under the gum line. Underneath the enamel and the cementum is dentin (dentine), a part of the tooth that is less dense than enamel or cementum. The dentin contains microscopic tubules (small hollow tubes or canals). When the dentin loses its protective covering, the tubules allow heat and cold or acidic or sticky foods to stimulate the nerves and cells inside your tooth. This may cause teeth hypersensitivity and occasional discomfort when you chew, drink cold or hot liquids, or when you breathe through your mouth. By definition, sensitive teeth or dentin hypersensitivity is a diagnosis of exclusion 2. Before proceeding to management and treatment for sensitive teeth, conditions that present with symptoms mimicking dentin hypersensitivity must be ruled out (see Figure 2 below) 3. Therefore, whether you have one sensitive tooth or several, it’s wise to see your dentist right away. Because early diagnosis and treatment can ensure that small problems won’t progress into more serious dental complications or the loss of a tooth.
Data available from available studies concluded that the incidence of tooth hypersensitivity ranges from 10% to 30% of the general population with higher female incidence than male, commonly affecting premolar and incisor teeth 4. A recent study demonstrated 42% of 18–35-year-old individuals present with teeth sensitivity 5. The incidence of teeth sensitivity reportedly peaks during the third and fourth decades of life 6.
Sensitive teeth are typically the result of worn tooth enamel or exposed tooth roots (see Figure 1). Sometimes, however, tooth discomfort is caused by other factors, such as a cavity, a tooth decay, a cracked or chipped tooth, a worn filling or gum disease. If you’re bothered by sensitive teeth, visit your dentist. Your dentist can identify or rule out any underlying causes of your tooth pain. Depending on the circumstances, your dentist might recommend:
- Desensitizing toothpaste. After several applications, desensitizing toothpaste can sometimes help block pain associated with sensitive teeth. There are a variety of products available over-the-counter. Ask your dentist which product might work best for you.
- Fluoride gel. Your dentist might apply fluoride to the sensitive areas of your teeth to strengthen tooth enamel and reduce pain. He or she might also suggest the use of prescription fluoride at home, applied via a custom tray.
- Desensitizing or bonding. Occasionally, exposed root surfaces can be treated by applying bonding resin to the sensitive root surfaces. A local anesthetic might be needed.
- Surgical gum graft. If your tooth root has lost gum tissue, a small amount of gum tissue can be taken from elsewhere in your mouth and attached to the affected site. This can protect exposed roots and reduce sensitivity.
- Root canal. If your sensitive teeth cause severe pain and other treatments aren’t effective, your dentist might recommend a root canal — a procedure used to treat problems in the tooth’s soft core (dental pulp). While this might seem like a significant treatment, it’s considered the most successful technique for eliminating tooth sensitivity.
Proper oral hygiene is an important step in preventing tooth decay, periodontal disease and pain from sensitive teeth. If you brush your teethincorrectly or brush too aggressively, you mayinjure your gums and expose tooth roots.
To prevent sensitive teeth from recurring, brush your teeth twice a day with a soft-bristled toothbrush and fluoride toothpaste and floss daily. Use gentle strokes, rather than vigorous or harsh scrubbing and avoid using an abrasive toothpaste. If you grind your teeth (also known as bruxism), ask your dentist about a mouth guard. Tooth grinding can fracture teeth and cause sensitivity.
You might also consider taking care when eating or drinking acidic foods and drinks, such as carbonated drinks, citrus fruits and wine — all of which can remove small amounts of tooth enamel over time. When you drink acidic liquids, use a straw to limit contact with your teeth. After eating or drinking an acidic substance, drink water to balance the acid levels in your mouth.
Figure 1. Tooth anatomy
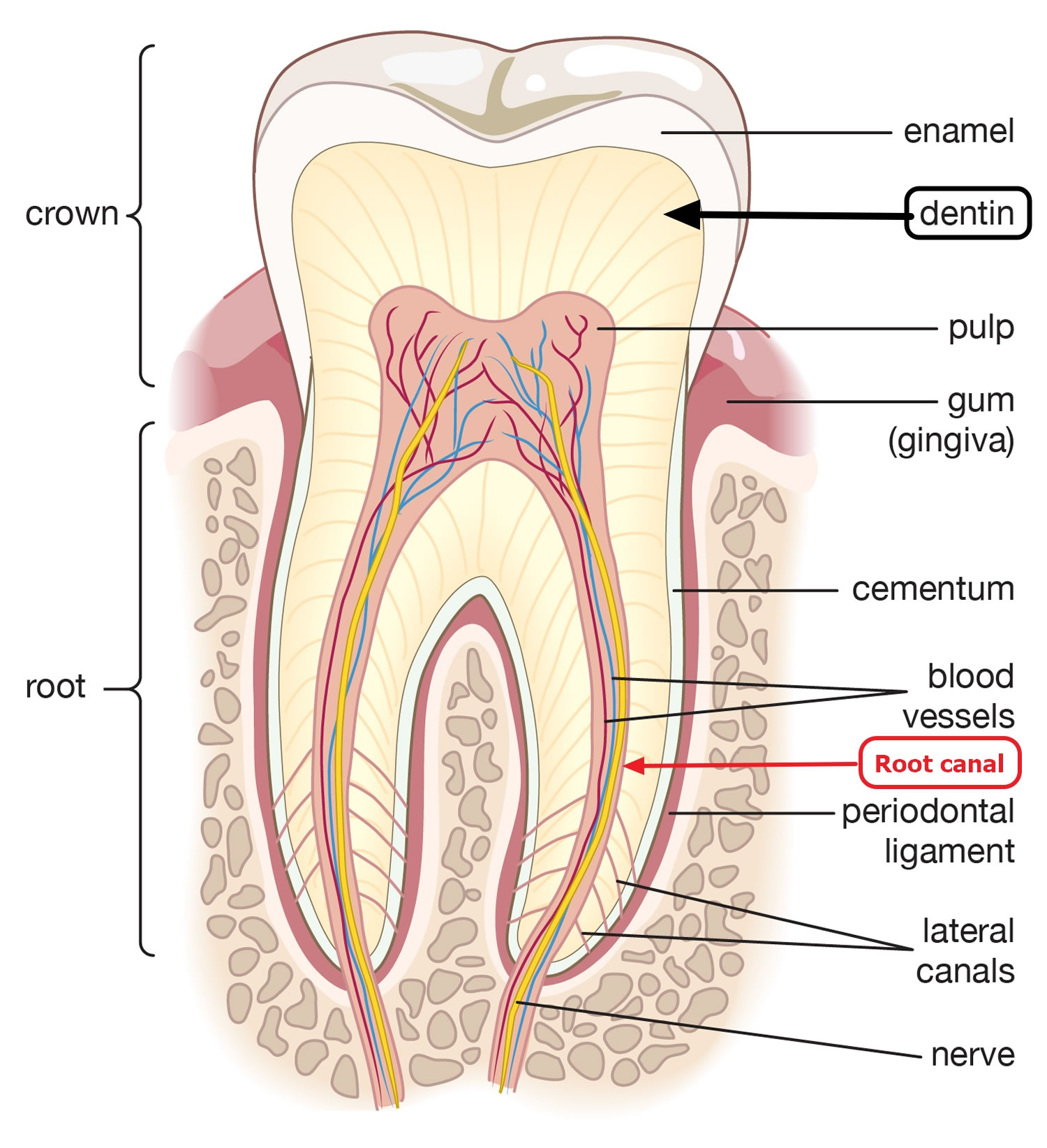
Footnote: The inside of your tooth is mostly made of a material called dentine (dentin), which surrounds the pulp of the tooth at the very center. The pulp is a soft tissue containing nerve fibers. The dentin contains microscopic tubules which communicate with the pulp of the tooth and hence, the nerve fibers. A hard outer layer of enamel protects the dentin on the crown portion of your tooth, and a layer of cementum protects the dentine on the root of your tooth. Dental erosion causes dentin hypersensitivity or nerve irritation. The dentine loses its protective covering of enamel or cementum, exposing the nerve endings in the pulp to hot, cold, acidic or sweet foods.
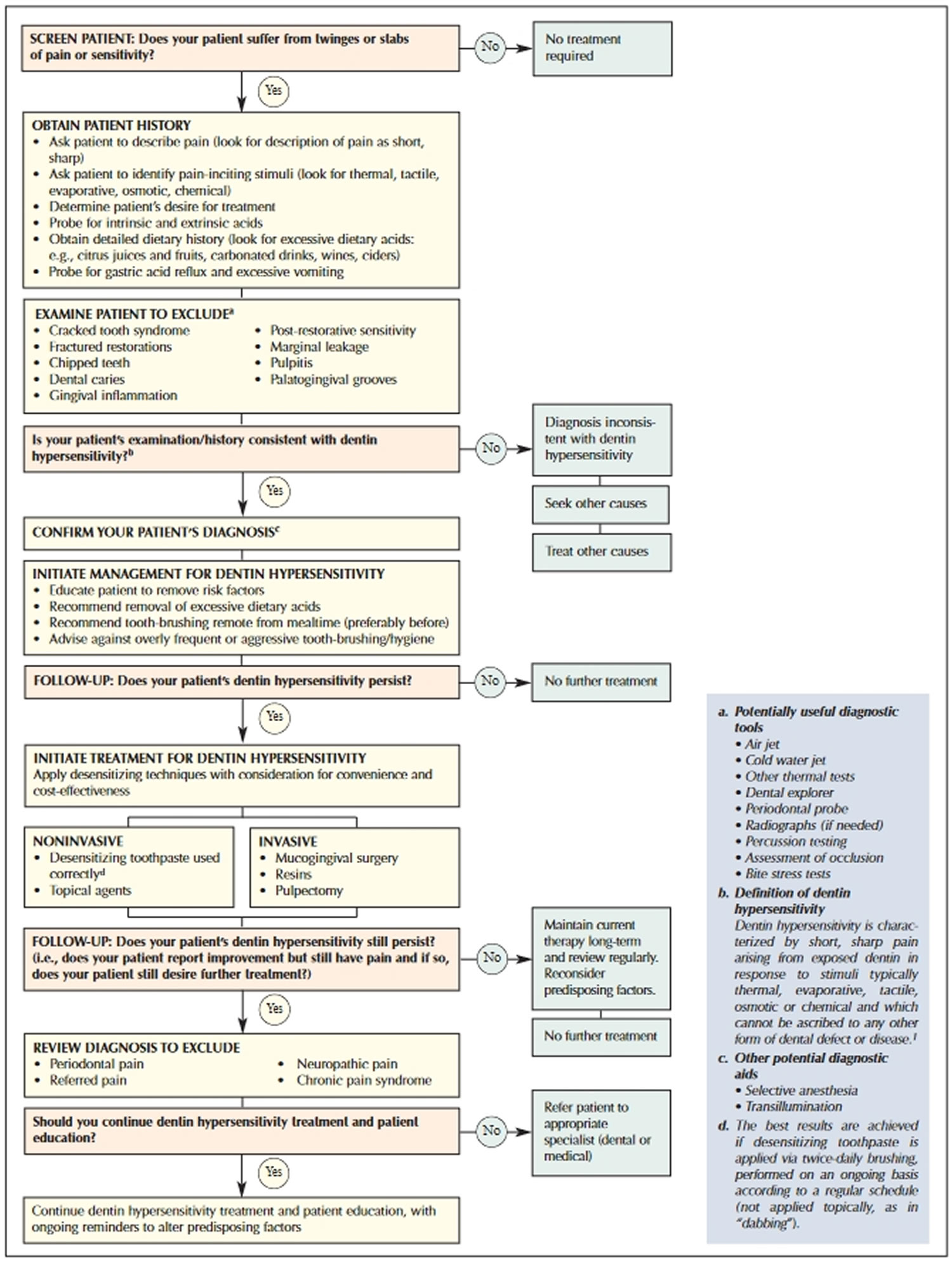
Figure 2. Algorithm for diagnosis and management of tooth sensitivity or dentin hypersensitivity
When are teeth more likely to be sensitive?
You are more likely to feel the sensitivity when drinking or eating something cold, from cold air catching your teeth, and sometimes with hot foods or drinks. Some people have sensitivity when they have sweet or acidic food and drinks. The pain can come and go, with some times being worse than others.
Do I need to go and see my dentist?
Yes, if you have tried treating your sensitive teeth for a few weeks and have had no improvement.
How can I prevent sensitive teeth?
- Brush your teeth last thing at night and at least one other time during the day, with fluoride toothpaste containing at least 1350ppm (parts per million) of fluoride. Consider using toothpaste specially designed for sensitive teeth. Use small, circular movements with a soft-to medium-bristled brush. Try to avoid brushing your teeth from side to side.
- Change your toothbrush every two to three months, or sooner if it becomes worn.
- Don’t brush straight after eating – some foods and drinks can soften the enamel of your teeth, so leave it for at least an hour before you brush.
- Have sugary foods, and fizzy and acidic drinks, less often. Try to have them just at mealtimes.
- If you grind your teeth, talk to your dental team about whether you should have a mouthguard made, to wear at night.
- If you are thinking about having your teeth bleached or whitened, discuss sensitivity with your dentist before starting treatment.
- Visit your dentist regularly, as often as they recommend.
Is there anything I should avoid if I have sensitive teeth?
You may find that hot, cold, sweet or acidic drinks, or foods like ice cream, can bring on sensitivity, so you may want to avoid these. If you have sensitivity when brushing your teeth with cold water from the tap, you may need to use warm water instead. It is important to keep brushing your teeth regularly – if you don’t, this could make the problem worse.
Sensitive teeth cause
Two processes are essential for the development of teeth sensitivity or dentin hypersensitivity: the dentin must become exposed (lesion localization), through either loss of enamel or gingival (gum) recession, and the dentin tubules must be open to both the oral cavity and the pulp (lesion initiation).
- Worn tooth enamel from using a hard toothbrush and using a hard grip while brushing aggressively. Brushing your teeth too hard will not make them cleaner, but it may wear away the protective enamel layer and make them sensitive, so when you brush remember to brush gently and with a ‘soft’ toothbrush.
- Gum disease can cause your gums to recede, exposing the root surfaces which can trigger sensitivity.
- Periodontal disease is an infection of the gums and bone that support your teeth—also may be responsible. If periodontal disease is left untreated, gum tissues can separate from the teeth and form spaces called pockets that provide a home for bacteria. Periodontal disease can progress until the bone and other tooth-supporting tissues are destroyed, leaving the root surfaces of teeth exposed. Regular dental checkups are important so that tooth decay, periodontal disease and other problems may be detected and treated in the early stages.
- Grinding or clenching your teeth can wear away your tooth enamel and usually occurs at night while you are asleep.
- Erosion of the tooth enamel by acidic drinks and foods, or stomach acid from reflux or vomiting. Pregnancy, eating disorders and conditions such as gastro-esophageal reflux disease (GERD) can increase your risk of erosion, so you should take extra care with your teeth in these situations.
- Chipped or broken tooth can cause the nerve in the tooth to become irritated and sensitive.
- Cracked or fractured tooth. A cracked tooth may not be visible to the naked eye. It may not even show on X-rays, making a diagnosis difficult. A common symptom of a cracked tooth is a sharp pain when biting down, but one that disappears after releasing that bite. Cracks involving a break around a filling can be repaired with a new filling or crown, but when a crack extends into the pulp of your tooth, you may need root canal treatment before a crown can be placed. Ultimately, a crack that extends below the gumline and into the root of the tooth will need to be removed.
- Tooth decay. If one tooth in particular bothers you, your dentist will examine the tooth in question and ask you to describe your symptoms. Most likely, he or she will take an X-ray to determine if a few common conditions could be the problem – one of which is tooth decay. In this case, acids produced by the bacteria built up against the tooth can eventually dissolve its enamel, exposing the dentin layer. And because dentin is filled with tiny nerve endings, you may experience temperature sensitivity and pain when biting down. Once your dentist removes the decay and fills the tooth with either an amalgam or tooth-colored filling, you should be pain free. A full-coverage crown might be needed for more stability and longevity.
- Abscess. An abscessed tooth occurs when the pulp of your tooth – which is made up of nerve and blood vessels – becomes infected. An abscessed tooth symptoms can include fever, persistent pain and facial swelling. Usually, there’s pus-filled swelling at the root tip, which drains periodically and gives you a bad taste in your mouth. You will need root canal treatment to save any tooth that has abscessed.
- Recent dental work such as restorations, crowns, fillings and even a routine scale and clean can inflame the nerves within the pulp tissue and may result in sensitive teeth. This can cause a temporary sensitivity to hot and cold, but it usually dissipates after a week or two. Your dentist will normally advise you if the treatment you are undertaking may cause sensitivity and will suggest a range of available options to minimize discomfort.
- Loose or broken filling. Unfortunately fillings don’t last forever, and when they break or become loose, you may experience sensitivity due to bacteria getting underneath, causing the tooth to decay further. Luckily, this problem is easily remedied with a new filling or crown.
Enamel is resistant to abrasion by tooth-brushing, with or without toothpaste, but is particularly sensitive to the effects of acid; thus, brushing of acid-softened (eroded) enamel has a marked abrasive effect 7. While it is possible that toothpaste may erode dentin to some extent, the abrasivity might also produce a smear layer, thereby reducing sensitivity 8. Interestingly, toothpaste abrasives in combination with detergents may remove the smear layer and open the tubules. Indeed, if predisposing factors are not eradicated, brushing with nearly any toothpaste may openthe tubules 9. Occasionally, some deposits of the abrasive from toothpastes do adhere to the tubules, but they detache asily later.
Gingival recession, another factor in exposure of dentin, has recently been described as an enigma 10 and its causes are not well understood. However, overzealous brushing, acute necrotizing ulcerative gingivitis, self-inflicted injury and periodontal procedures are the major predisposing factors.
The most widely accepted mechanism of dentin hypersensitivity is the hydrodynamic theory proposed by Braennstroem and Astroem in 1964 11, whereby fluid flow within dentinal tubules is altered (increased or changed directionally), absent of a smear layer, is subject to thermal, chemical, tactile or evaporative stimuli 12. The movement of the fluid within the dentinal tubules stimulates the mechanical receptors which are sensitive to fluid pressure, resulting in the transmission of the stimuli to the pulpal nerves, ultimately causing pain response 13. Absi and others 14 reported that nonsensitive teeth were unresponsive to any stimuli and had very few exposed tubules. In contrast, sensitive teeth had much greater numbers of open tubules per unit area (8 times as many tubules at the root surface than nonsensitive teeth). Similarly, the average diameter of tubules in sensitive teeth was almost 2 times greater than that of tubules in nonsensitive teeth (0.83 μm vs. 0.4 μm). Dentin hypersensitivity is caused by the exposure of the dentinal tubule, and with the increasing diameter of the tubule, dentin is demineralized by micro-organisms within the oral cavity or by acidic food 15. Thus, the key point of sensitive tooth treatment is to desensitize dentin through the remineralization of exposed dentin-occluding dentinal tubules 16.
Tooth sensitivity treatment
Sensitive teeth can be treated. Your dentist can identify the underlying cause of your teeth sensitivity and recommend the best oral hygiene practices to help reduce your discomfort and maintain the health of your teeth. It’s important to remember that some tooth sensitivity is caused by more serious problems, including tooth decay, a fractured filling, a cracked tooth or even a root canal problem. So don’t overlook the importance of a professional diagnosis by your dentist.
In the meantime, there are some simple things you can do every day to help minimize the discomfort of sensitive teeth. Brush and floss regularly and make sure you are brushing your teeth correctly. It’s not hard to learn how to brush properly – ask your dentist to teach you. Always use a soft toothbrush and consider using toothpaste for sensitive teeth which contains compounds that help block sensation traveling from the tooth surface to the nerve as a part of your daily routine. Desensitizing toothpaste usually requires several applications before the sensitivity is reduced. Of course brushing is good for your teeth, but when you eat or drink something acidic, it’s best to rinse your mouth with water and chew sugar-free gum afterwards and wait at least 60 minutes before brushing.
If the desensitizing toothpaste does not ease your discomfort, your dentist may suggest in-office treatments. A fluoride gel or special desensitizing agents may be applied to the sensitive areas of the affected teeth. When these measures do not correct the problem, your dentist may recommend other treatments, such as a filling, a crown, an inlay or bonding to correct a flaw or decay that results in sensitivity. The type of treatment will depend on what is causing your teeth sensitivity.
If gum tissue has been lost from the root (gum recession), your dentist may recommend a surgical gum graft to cover the root, protect the tooth and reduce the sensitivity. In cases in which teeth hypersensitivity is severe and persistent and cannot be treated by other means, your dentist may recommend endodontic (root canal) treatment to eliminate the problem.
Sensitive teeth pain relief
The key point of the teeth sensitivity treatment is to desensitize dentin through the remineralization of exposed dentin-occluding dentinal tubules 17. Currently, two treatment approaches are widely applied for teeth sensitivity, namely tubular occlusion and blockage of nerve activity 18. Tubular occlusion incorporates the use of a physical or chemical agent that occludes the dentinal tubules. These occluding agents include stannous, strontium or oxalate salts; arginine; silicas; and bioactive glasses 19. Treatment strategies such as lasers and periodontal soft-tissue grafting also work on the same principle. In the second approach, depolarizing agents, such as potassium ions, are directly diffused to reduce intradental nerve activity 20.
Many kinds of studies have been done to identify dentin-desensitizing materials, and it has been found that sodium fluoride solution 21, calcium hydroxide, stannous hydroxide, calcium oxalate, ferric phosphate 22 and potassium nitrate solution 23 are effective for dentine hypersensitivity treatment. Also, dental products like fluoride varnishes 24 and resin adhesives 25 are proven to be helpful in decreasing teeth sensitivity, by occluding dentinal tubules. Low-level laser treatment, such as the neodymium:yttrium-aluminum-garnet (Nd:YAG) laser 26, has potential for teeth sensitivity treatment.
Recently, a particulate bioactive glass (calcium sodium phosphosilicate [NovaMin]) has been proposed as a good option for teeth sensitivity treatment, due to its excellent remineralization ability and bioactivity 27. Bioactive glass is a material that is composed of SiO2–CaO–Na2O–P2O5 (calcium sodium phosphosilicate), which has been proven to be effective in occluding dentinal tubules by binding preferentially to exposed tubules and for dental remineralization 28 and has been incorporated into dental products to provide relief from teeth sensitivity 29. On exposure to the aqueous oral environment, calcium sodium phosphosilicate provides calcium and phosphate ions to form a hydroxycarbonate apatite-like layer on the dentine surface and within the tubules 30. Recently, fluoro calcium phosphosilicate, a fluoride-containing bioglass is designed and optimized for desensitizing toothpaste 31. This formulation differentiates from previous bioglass toothpastes by its higher phosphate content, the presence of calcium fluoride (CaF2) in the glass and the smaller average particle size 31. It forms fluorapatite, rather than hydroxyapatite, on teeth which is much more resistant to acids produced by bacteria and promotes remineralization, particularly in combination with the calcium and phosphate released from the glass. The fluoro calcium phosphosilicate containing toothpaste was launched in 2016 in the UK (online only) and pharmacies in Germany and India.
Poly(amidoamine) (PAMAM), is a highly developed polymer with reactive end-parts in various forms and sizes inside the sphere 32. Polyamidoamine (PAMAM) is a notable dendrimer in biomineralization fields, because it can perform in a similar manner to non-collagenous proteins that play an important role in dentin mineralization 33. Also, with its relatively lower toxicity, better biocompatibility, and wider surface area, it is considered as potentially providing an ideal platform for hydroxyapatite reformation 34. According to Tao S. et al. 35, PAMAM–NH2 reacts with calcium and phosphorus ions to form hydroxyapatite, and it has been experimentally verified that it could be effective in dentin remineralization. In particular, in terms of intrafibrillar remineralization within the dentinal tubule, studies on the remineralization effect of PAMAM showed quite an interesting result. Furthermore, intrafibrillar remineralization using nanostructures has significance in teeth sensitivity treatment 36.
Studies on dentinal remineralization have shown that bioactive glass and polyamidoamine (PAMAM) could be effective in teeth sensitivity treatment, with their distinctive properties. If these two materials are synthesized into new materials to yield a higher reactivity for PAMAM and the ion-releasing effects of bioactive glass, a better nanostructured biomaterial can be expected in the dentin remineralization field. However, such studies have not yet been conducted 12.
References- Canadian Advisory Board on Dentin Hypersensitivity. Consensus-based recommendations for the diagnosis and management of dentin hypersensitivity. J Can Dent Assoc. 2003 Apr;69(4):221-6. http://www.cda-adc.ca/jcda/vol-69/issue-4/221.pdf
- Holland GR, Narhi MN, Addy M, Gangarosa L, Orchardson R.Guidelines for the design and conduct of clinical trials on dentine hyper-sensitivity. J Clin Periodontol 1997; 24(11):808–13.
- Dowell P, Addy M, Dummer P. Dentine hypersensitivity: aetiology,differential diagnosis and management. Br Dent J 1985; 158(3):92–6.
- Shiau HJ. Dentin hypersensitivity. J Evid Based Dent Pract. 2012 Sep;12(3 Suppl):220-8. doi: 10.1016/S1532-3382(12)70043-X
- West NX, Seong J, Davies M. Management of dentine hypersensitivity: efficacy of professionally and self-administered agents. J Clin Periodontol. 2015 Apr;42 Suppl 16:S256-302. doi: 10.1111/jcpe.12336
- Rees JS, Addy M. A cross-sectional study of buccal cervical sensitivity in UK general dental practice and a summary review of prevalence studies. Int J Dent Hyg. 2004 May;2(2):64-9. doi: 10.1111/j.1601-5029.2004.00068.x
- Davis WB, Winter PJ. The effect of abrasion on enamel and dentineand exposure to dietary acid. Br Dent J1980; 148(11-12):253–6.
- Adams D, Addy M, Absi EG. Abrasive and chemical effects of denti-frices. In: Embery G, Rolla G, editors. Clinical and biological aspects ofdentifrices. Oxford: Oxford University Press; 1992. p. 345–55.
- Addy M. Dentine hypersensitivity: definition, prevalence, distributionand aetiology. In: Addy M, Embery G, Edgar WM, Orchardson R,editors. Tooth wear and sensitivity. Clinical advances in restorative dentistry. London: Martin Dunitz; 2000. p. 239–48.
- Smith RG. Gingival recession. Reappraisal of an enigmatic conditionand new index for monitoring. J Clin Periodontol 1997; 24(3):201–5.
- Braennstroem M, Astroem A. A study on the mechanism of pain elicited from the dentin. J Dent Res. 1964;43:619–25. doi: 10.1177/00220345640430041601
- Bae, J., Son, W. S., Yoo, K. H., Yoon, S. Y., Bae, M. K., Lee, D. J., Ko, C. C., Choi, Y. K., & Kim, Y. I. (2019). Effects of Poly(Amidoamine) Dendrimer-Coated Mesoporous Bioactive Glass Nanoparticles on Dentin Remineralization. Nanomaterials (Basel, Switzerland), 9(4), 591. https://doi.org/10.3390/nano9040591
- Brannstrom M., Linden L.A., Johnson G. Movement of dentinal and pulpal fluid caused by clinical procedures. J. Dent. Res. 1968;47:679–682. doi: 10.1177/00220345680470050201
- Absi EG, Addy M, Adams D. Dentine hypersensitivity. A study of thepatency of dentinal tubules in sensitive and non-sensitive cervical dentine.J Clin Periodontol 1987; 14(5):280–4.
- Yoshiyama M., Noiri Y., Ozaki K., Uchida A., Ishikawa Y., Ishida H. Transmission electron microscopic characterization of hypersensitive human radicular dentin. J. Dent. Res. 1990;69:1293–1297. doi: 10.1177/00220345900690061401
- Cummins D. Dentin hypersensitivity: from diagnosis to a breakthrough therapy for everyday sensitivity relief. J Clin Dent. 2009;20(1):1-9.
- Bartold, P. (2006), Dentinal hypersensitivity: a review. Australian Dental Journal, 51: 212-218. https://doi.org/10.1111/j.1834-7819.2006.tb00431.x
- Ashwini, S., Swatika, K., & Kamala, D. N. (2018). Comparative Evaluation of Desensitizing Efficacy of Dentifrice Containing 5% Fluoro Calcium Phosphosilicate versus 5% Calcium Sodium Phosphosilicate: A Randomized Controlled Clinical Trial. Contemporary clinical dentistry, 9(3), 330–336. https://doi.org/10.4103/ccd.ccd_735_17
- Ganss C, Lussi A. Diagnosis of erosive tooth wear. Monogr Oral Sci. 2014;25:22-31. doi: 10.1159/000359935
- Markowitz K, Pashley DH. Discovering new treatments for sensitive teeth: the long path from biology to therapy. J Oral Rehabil. 2008 Apr;35(4):300-15. doi: 10.1111/j.1365-2842.2007.01798.x
- Kishore A., Mehrotra K.K., Saimbi C.S. Effectiveness of desensitizing agents. J. Endod. 2002;28:34–35. doi: 10.1097/00004770-200201000-00008
- Jain P, Vargas MA, Denehy GE, Boyer DB. Dentin desensitizing agents: SEM and X-ray microanalysis assessment. Am J Dent. 1997 Feb;10(1):21-6.
- Frechoso C.S., Menendez M., Guisasola C., Arregui I., Tejerina J.M., Sicilia A. Evaluation of the efficacy of two potassium nitrate bioadhesive gels (5% and 10%) in the treatment of dentine hypersensitivity. A randomized clinical trial. J. Clin. Periodontol. 2003;30:315–320. doi: 10.1034/j.1600-051X.2003.20077.x
- Lutins N.D., Greco G.W., McFall W.T., Jr. Effectiveness of sodium fluoride on tooth hypersensitivity with and without iontophoresis. J. Periodontol. 1984;55:285–288. doi: 10.1902/jop.1984.55.5.285
- Orucoglu H, Belli S. Evaluation of the effect of four self-etching adhesives on dentin permeability. J Biomed Mater Res B Appl Biomater. 2009 Jul;90(1):110-5. doi: 10.1002/jbm.b.31259
- Ciaramicoli M.T., Carvalho R.C., Eduardo C.P. Treatment of cervical dentin hypersensitivity using neodymium:yttrium-aluminum-garnet laser. Clinical evaluation. Lasers Surg. Med. 2003;33:358–362. doi: 10.1002/lsm.10232
- Du Min Q, Bian Z, Jiang H, Greenspan DC, Burwell AK, Zhong J, Tai BJ. Clinical evaluation of a dentifrice containing calcium sodium phosphosilicate (novamin) for the treatment of dentin hypersensitivity. Am J Dent. 2008 Aug;21(4):210-4.
- Chen W.C., Kung J.C., Chen C.H., Hsiao Y.C., Shih C.J., Chien C.S. Effects of bioactive glass with and without mesoporous structures on desensitization in dentinal tubule occlusion. Appl. Surf. Sci. 2013;283:833–842. doi: 10.1016/j.apsusc.2013.07.027
- Gendreau L, Barlow AP, Mason SC. Overview of the clinical evidence for the use of NovaMin in providing relief from the pain of dentin hypersensitivity. J Clin Dent. 2011;22(3):90-5.
- Hall C, Mason S, Cooke J. Exploratory randomised controlled clinical study to evaluate the comparative efficacy of two occluding toothpastes – a 5% calcium sodium phosphosilicate toothpaste and an 8% arginine/calcium carbonate toothpaste – for the longer-term relief of dentine hypersensitivity. J Dent. 2017 May;60:36-43. doi: 10.1016/j.jdent.2017.02.009
- Jones JR, Brauer DS, Hupa L, Greenspan DC. Bioglass and bioactive glasses and their impact on healthcare. Int J Appl Glass Sci. 2016;7:423–34.
- Svenson S., Tomalia D.A. Dendrimers in biomedical applications-reflections on the field. Adv. Drug Deliv. Rev. 2005;57:2106–2129. doi: 10.1016/j.addr.2005.09.018
- Tsiourvas D., Tsetsekou A., Kammenou M.I., Boukos N. Controlling the formation of hydroxyapatite nanorods with dendrimers. J. Am. Ceram. Soc. 2011;94:2023–2029. doi: 10.1111/j.1551-2916.2010.04342.x
- Tsortos A., Nancollas G.H. The Adsorption of Polyelectrolytes on Hydroxyapatite Crystals. J. Colloid Interface Sci. 1999;209:109–115. doi: 10.1006/jcis.1998.5881
- Tao S., Fan M., Xu H.H.K., Li J., He L., Zhou X., Liang K., Li J. The remineralization effectiveness of PAMAM dendrimer with different terminal groups on demineralized dentin in vitro. RSC Adv. 2017;7:54947–54955. doi: 10.1039/C7RA11844A
- Liang K., Yuan H., Li J., Yang J., Zhou X., He L., Cheng L., Gao Y., Xu X., Zhou X., Li J. Remineralization of Demineralized Dentin Induced by Amine-Terminated PAMAM Dendrimer. Macromol. Mater. Eng. 2015;300:107–117. doi: 10.1002/mame.201400207





{kind=link}