Septal hematoma
Septal hematoma is when blood collects (hematoma) in the area of your nose between your nostrils, called the septal cartilage and the overlying mucoperichondrium. A septal hematoma can block one or both nostrils. Usually some kind of injury disrupts the blood vessels and pulls the lining away from the cartilage, allowing blood to collect between the two 1. Nasal trauma is extremely common, with the nasal bones being the third most commonly fractured bone in the human body 2. In about 90% of nasal fractures the nasal septum is also injured 2. Although septal hematomas are rare, early diagnosis and treatment is important to prevent abscess formation, septal perforation, saddle-nose deformity, and potentially permanent complications 3.
The anterior portion of the nasal septum is composed of a thin cartilaginous plate with a closely adherent perichondrium and mucosa. Submucosal blood vessels are torn as buckling forces pull the perichondrium from the cartilage. Subsequently, blood may collect between the perichondrium and the septal cartilage. Bacterial proliferation and abscess formation may then result from the presence of stagnant blood. A septal hematoma may become infected within 3 days of the trauma.
The nasal septum derives its blood supply from the sphenopalatine and the anterior and posterior ethmoid arteries with the added contribution of the superior labial artery (anteriorly) and the greater palatine artery (posteriorly). The Kiesselbach plexus, or the Little area, represents a region in the anteroinferior third of the nasal septum, where all 3 of the chief blood supplies to the internal nose converge (see Figures 1 and 2).
A broken nose, also called a nasal fracture, is a break or crack in a bone in your nose — often the bone over the bridge of your nose.
Common causes of a broken nose include contact sports, physical fights, falls and motor vehicle accidents that result in facial trauma. A broken nose can cause pain, along with swelling and bruising around your nose and under your eyes. Your nose may look crooked, and you may have trouble breathing.
A careful examination is important for anyone who sustains nasal trauma. Signs of external trauma, such as nasal deformity, epistaxis, or significant pain, are associated with a septal hematoma. However, a septal hematoma may be present without any signs of external trauma 1.
Treatment for a broken nose may include procedures that realign your nose. Surgery usually isn’t necessary for a broken nose.
Nasal septal hematoma key points 2:
- Clinicians should have a high clinical suspicion for nasal septal hematoma in patients who have sustained nasal trauma 4
- Septal hematomas should be drained as soon as possible to prevent long-term complications.
- Inspect the nasal septum after any nasal trauma, no matter how trivial, to assess for a septal hematoma
- Common presenting features include nasal obstruction, pain, rhinorrhea, and fever
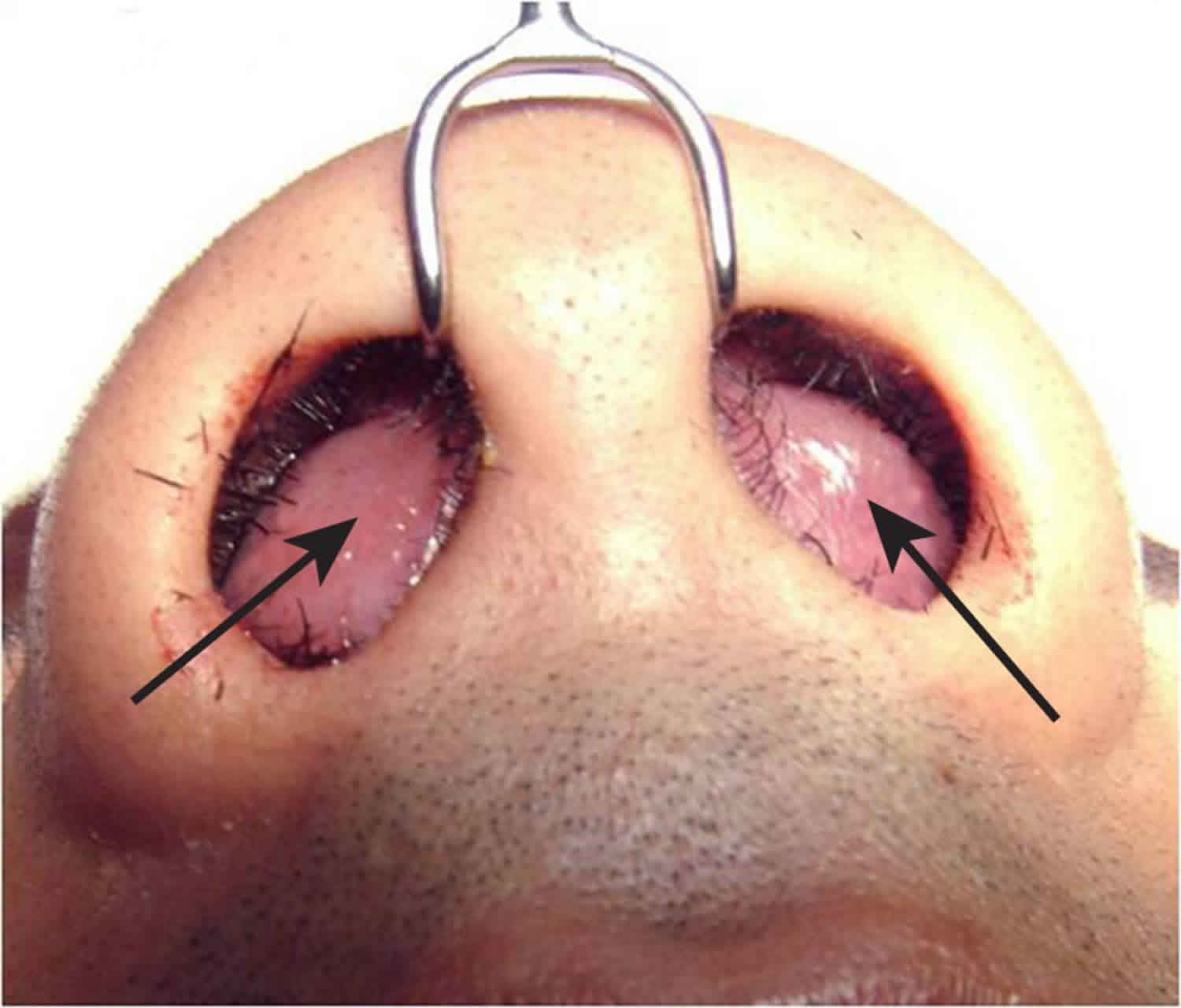
- It may be visible as a fluctuant swelling arising from the nasal septum, more commonly (but not always) bilateral
- Refer all patients suspected of having a septal hematoma as an emergency to the ear, nose, and throat specialist (otolaryngologist)
- Close follow-up with an otolaryngologist must be arranged to avoid potentially delayed complications 5. Children should follow-up periodically for 12-18 months after initial treatment.
- Septal hematomas can cause severe cosmetic nasal deformities as well as serious life threatening infective complications
- Prophylactic broad-spectrum antibiotics should be administered to cover Staphylococcus aureus, Haemophilus influenzae, and Streptococcus pneumoniae.
Figure 1. Arteries involve in nasal septal hematoma
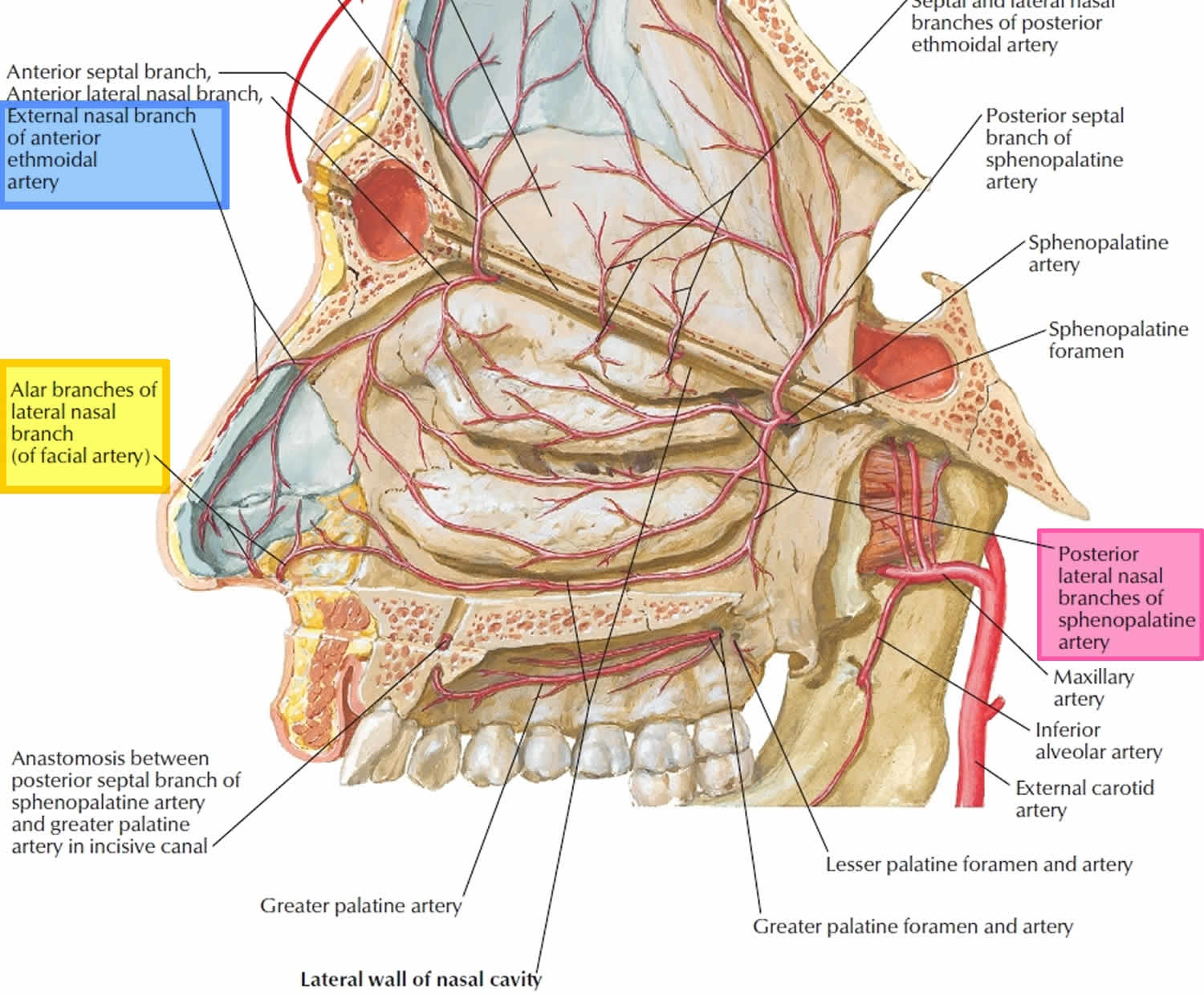
Figure 2. Arterial supply of the nasal cavity
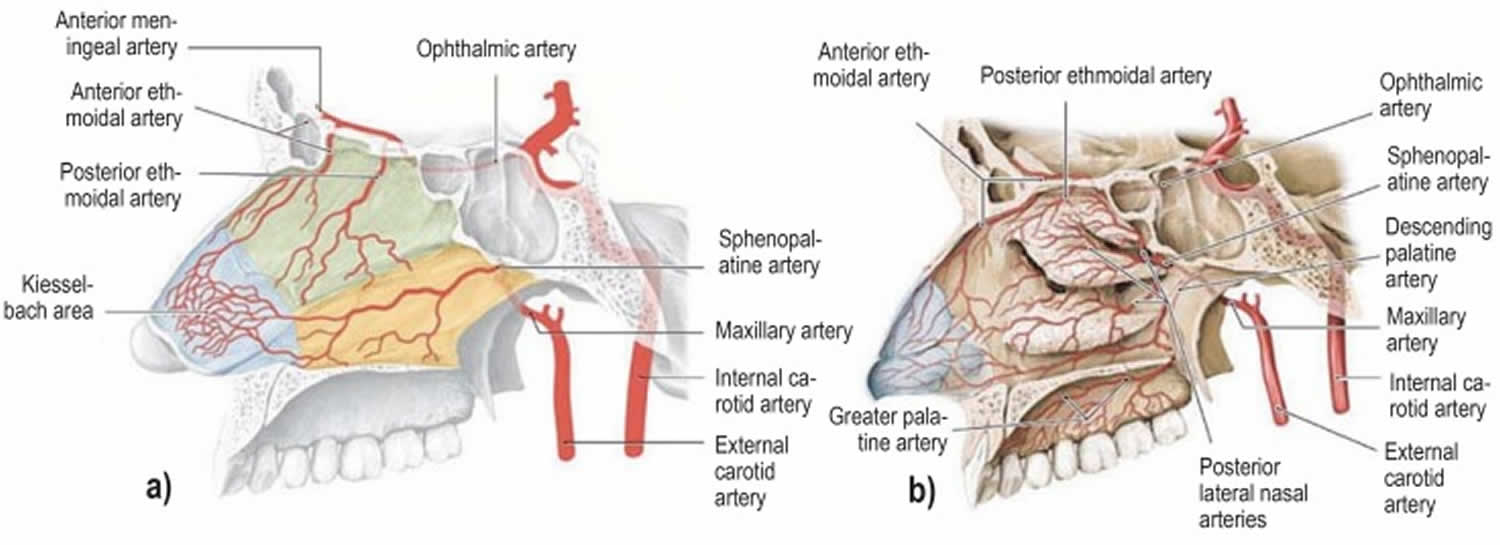
Footnote: The different territories supplied by the internal carotid artery (green) and the external carotid artery (yellow) are indicated in a). The Kiesselbach area (blue) is supplied by branches of both the main arteries (red).
a) Arteries supplying the nasal septum and b) the lateral walls of the nasal cavity.
[Source 6 ]Septal hematoma causes
Nasal septal hematoma in adults typically occurs with significant facial trauma and nasal fracture. However, in children, nasal septal hematoma may be found with minor nasal trauma such as simple falls, collisions with stationary objects, or minor altercations with siblings 7. Additionally, the presence of nasal septal hematoma with or without concomitant injuries should raise suspicion for child abuse, especially in infants and toddlers.
Septal hematoma symptoms
The nasal septum is normally 2-4 mm thick. If the cartilage is fractured, blood can dissect through the fracture line and form bilateral hematomas; therefore, both sides should be examined. According to a study by Canty et al 8, the most common symptoms noted in children were nasal obstruction (95%), pain (50%), rhinorrhea (25%), and fever (25%). Symptoms usually appear within the first 24-72 hours.
Septal hematoma complications
Though nasal septal abscesses are rare, they are the most common acute complications of septal hematomas 9. Abscesses can result in the spread of bacteria into the paranasal and intracranial structures 10. Further complications, including meningitis, intracranial abscesses, orbital cellulitis, and cavernous sinus thrombosis, may ensue 11.
An expanding hematoma can cause pressure-induced avascular necrosis of the cartilage. Collapse of the nasal septum and loss of dorsal support can lead to depression of the nasal bridge and a subsequent saddle-nose deformity 12. Early drainage of the hematoma improves blood flow to the septal cartilage but may not reverse antecedent cartilage destruction. Therefore, the clinician must have a high index of suspicion of a nasal septal hematoma after any nasal trauma in order to initiate proper early surgical treatment.
Septal hematoma diagnosis
A septal hematoma can usually be diagnosed by inspecting the septum with a nasal speculum or an otoscope. Asymmetry of the septum with a bluish or reddish fluctuance may suggest a hematoma. Direct palpation may also be necessary, as newly formed hematomas may not be ecchymotic. The best way to palpate is to insert a gloved small finger into the patient’s nose and palpate along the entire septum, feeling for swelling, fluctuance, or widening of the septum. Blood clots should be suctioned to allow better visualization.
Septal hematoma treatment
Septal hematoma requires prompt surgical drainage to prevent cartilage damage 13. Topical lidocaine or Pontocaine or injectable lidocaine without epinephrine can be used, not to exceed a dose of 5 mg/kg or a total of 300 mg.
Septal hematoma surgical drainage technique
If a septal abscess is suspected, needle aspiration under topical anesthesia can be performed using an 18- to 20-ga needle.
Except in patients who present immediately after hematoma formation, specimens should be sent for gram stain and aerobic and anaerobic cultures. Systemic antibiotics should then be administered.
- To drain the hematoma, incise the mucosa over the area of greatest fluctuance without incising cartilage. Bilateral staggered incisions should be made for bilateral hematomas to avoid a through-and-through perforation.
- Suction out the clot; then irrigate with sterile normal saline.
- A small section of the mucoperichondrium should be excised to prevent premature closure of the incision.
- Place a small Penrose drain and suture it in place.
- Finally, pack both nostrils, as in anterior epistaxis, to reapproximate the perichondrium to the cartilage. The drain and packing remain in place until the drainage stops for 24 hours; this usually takes 2-3 days 14.
Broad spectrum antibiotics should be administered. If infection is suspected, the patient should be admitted for parenteral antibiotics.
The patient should follow up with an otolaryngologist without delay. Children should also be evaluated periodically for 12-18 months to avoid cosmetic deformities.
Prophylactic treatment with an antibiotic is recommended to cover Streptococcus pneumoniae and beta-lactamase–producing organisms. Although no clear consensus exists on the choice of antibiotic or duration of treatment, most case reports have used amoxicillin/clavulanate (Augmentin). If an abscess is suspected, clindamycin is recommended as initial therapy until culture results are available.
References- Matsuba HM, Thawley SE. Nasal septal abscess: unusual causes, complications, treatment, and sequelae. Ann Plast Surg. 1986 Feb. 16(2):161-6.
- Nasal septal haematoma. BMJ 2014; 349 doi: https://doi.org/10.1136/bmj.g6075
- Junnila J. Swollen masses in the nose. Am Fam Physician. 2006 May 1. 73(9):1617-8.
- Agrawal N, Brayley N. Audit of nasal fracture management in accident and emergency in a district general hospital. J Eval Clin Pract. 2007 Apr. 13(2):295-7.
- Menger DJ, Tabink I, Nolst Trenité GJ. Treatment of septal hematomas and abscesses in children. Facial Plast Surg. 2007 Nov. 23(4):239-43.
- Beck R, Sorge M, Schneider A, Dietz A. Current Approaches to Epistaxis Treatment in Primary and Secondary Care. Dtsch Arztebl Int. 2018;115(1-02):12–22. doi:10.3238/arztebl.2018.0012 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5778404
- Sayn I, Yazc ZM, Bozkurt E, Kayhan FT. Nasal septal hematoma and abscess in children. J Craniofac Surg. 2011 Nov. 22(6):e17-9.
- Canty PA, Berkowitz RG. Hematoma and abscess of the nasal septum in children. Arch Otolaryngol Head Neck Surg. 1996 Dec. 122(12):1373-6.
- Ginsburg CM, Leach JL. Infected nasal septal hematoma. Pediatr Infect Dis J. 1995 Nov. 14(11):1012-3.
- Ambrus PS, Eavey RD, Baker AS, et al. Management of nasal septal abscess. Laryngoscope. 1981 Apr. 91(4):575-82.
- Huang PH, Chiang YC, Yang TH, Chao PZ, Lee FP. Nasal septal abscess. Otolaryngol Head Neck Surg. 2006 Aug. 135(2):335-6.
- Savage RR, Valvich C. Hematoma of the nasal septum. Pediatr Rev. 2006 Dec. 27(12):478-9.
- Chukuezi AB. Nasal septal haematoma in Nigeria. J Laryngol Otol. 1992 May. 106(5):396-8.
- Günaydin RÖ, Aygenc E, Karakullukcu S, Fidan F, Celikkanat S. Nasal packing and transseptal suturing techniques: surgical and anaesthetic perspectives. Eur Arch Otorhinolaryngol. 2011 Aug. 268(8):1151-6.





{kind=link}